Schizophrenia II - Psychiatry Training
advertisement

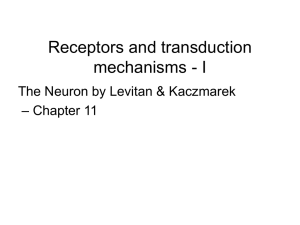
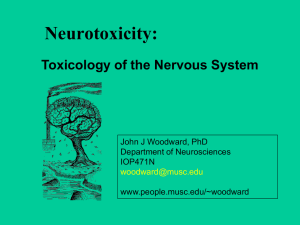
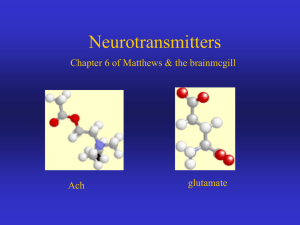
Amino Acid Neurotransmitters Paul Glue Objectives • Review: – Relative abundance of AAs vs monoamines – Pharmacology of glutamate, GABA – Postulated role of glutamate, GABA dysfunction in neuropsych disorders Relative abundance of neurotransmitters • Glutamate ~60% of synapses • GABA ~30% of synapses • Monoamines, peptides, other AAs (e.g. glycine) <5% COOH Glutamate Pharmacology COOH H2N • Glutamate is one of the most common transmitters in the CNS – Fast, excitatory transmitter; receptors on almost all neurons. Transmitter in ~60% of neurons, esp cortex, limbic structures. • Glutamate binds to 4 classes of receptor – three "ionotropic" receptor classes - ligand-gated ion channels which are characterized by the different ligands that bind to them: • AMPA • kainic acid • N-methyl-D-aspartate or NMDA – one G-protein coupled or "metabotropic" receptor class. The Glutamate Synapse Interconversion of glutamate to glutamine Note – significant Glu uptake (mainly astrocytes) COOH Glutamate Function COOH H2N • Under physiological conditions, activation of ionotropic receptors in neurons initiates transient depolarization and excitation. • AMPA-Rs mediate the fast component of excitatory postsynaptic currents • NMDA-Rs underlie a slower component. • AMPA-Rs modulate Ca++ influx thru NMDA-Rs. – Depolarization of the postsynaptic neuronal membrane via AMPA-Rs relieves the Mg++ block of the NMDA-R ion channel (this occurs in NMDA-R under resting conditions). This allows controlled Ca++ influx through the NMDA-R. This voltage-dependent modulation of the NMDA-R results in activity-driven synaptic modulation. • Glutamate overactivity can lead to neuronal death due to Ca++ toxicity, other associated mechanisms. NMDA-Receptors Structure - tetramers of two NR1 subunits and two NR2 subunits (some brain areas have NR3 subunits). Binding sites on the extracellular domain: NR1: coagonist glycine; NR2: glutamate. For efficient ion channel opening, the NMDA receptor requires both glutamate and the co-agonist glycine. Binding sites in the ion channel: Mg2+; PCP/ketamine site NMDA antagonists: Synthetic antagonists include: MK-801 (dizocilpine) Phencyclidine Ketamine Dextromethorphan Memantine, Amantadine Procyclidine Ketamine and NMDA modulators: Mg2+ blocks the NMDA channel in a voltage-dependent manner. - Na+, K+ and Ca2+ not only pass through the NMDA receptor channel but also modulate the activity of NMDA receptors. - Zn2+ blocks the NMDA current in a non-competitive and voltage-independent manner. - The activity of NMDA receptors is also sensitive to the changes in H+ concentration, and is partially inhibited by the ambient concentration of H+ under physiological conditions. Metabotropic glutamate receptors • Metabotropic receptors are coupled to their associated ion channel through a second messenger pathway. – May be located pre-, post- or extra-synaptically • Glutamate binding activates a G-protein and initiates an intracellular cascade • There are 8 cloned mGluRs (mGluR1-mGluR8) – classified into three groups (I, II, and III) based on structural homology, agonist selectivity, and associated second messenger cascade • Group I mGluRs (mGluR1 and mGluR5) are coupled to the hydrolysis of fatty acids and the release of calcium from internal stores. Quisqualate and trans-ACPD are Group I agonists. • Group II (mGluR2 and mGluR3) and Group III (mGluRs 4, 6, 7, and 8) receptors are considered inhibitory because they are coupled to the downregulation of cyclic nucleotide synthesis – Appear to have neuroprotective effects in animal models mGluR1 mGluR2 mGluR3 mGluR4 mGluR5 mGluR subtype mRNA distribution in rat brain Glutamate hypothesis of schizophrenia (1) • Is DA antagonism alone enough for an effective antipsychotic agent? – DA antagonism has limited effects on negative symptoms – DA antagonists take several weeks to show clinical antipsychotic activity; other pharmacological effects (PRL, EPSE) much more rapid. • NMDA receptor antagonists (ketamine, PCP) are psychotogenic in normal individuals and schizophrenic patients; positive in animal models indicative of psychotogenic potential. • Potency of antagonism correlates with ability to produce behavioral/ psychotogenic effects Glutamate hypothesis of schizophrenia (2) • Glutamate may have a significant role in the control of dopamine transmission in the striatum. – Dopamine transmission occurs in two different temporal modes, phasic and tonic. • Phasic DA release is transient and rapidly terminated, and selectively affects only receptors within or near the synapse. Phasic transmission is primarily dopamine dependent. • Tonic release of dopamine results in a constant level of dopamine in the extracellular, extrasynaptic space and is regulated mainly by glutamate. • Not all GluRs are realistic targets – – Ionotropic GluRs mediate most fast synaptic transmission in the CNS - too ubiquitous – Excess Glu is neurotoxic; NMDA antagonism is psychotogenic • Metabotropic glutamate receptors may be better targets – These modulate synaptic neurotransmission – mGluR2 and 3 are primarily distributed in forebrain regions. – Stimulation of these mediates presynaptic depression and decreases evoked release of glutamate. – PCP and other NMDA antagonists increase glutamate efflux; this may increase DA activity (amongst others) – Reduction of presynaptic glutamatergic activity by targeting group II mGluRs may be a novel approach to treating schizophrenia Clinical Trial: LY2140023: (mGluR 2/3 agonist in acute SCZ) (Nat Med 2007) LY=OLZ, >pbo for: PANSS, CGI LY=pbo, >OLZ for: Weight, PRL Dopamine Glutamate Antagonists in Major Depression • Rationale: – NMDA-antagonists are effective in animal models of depression – Elevated glutamate levels in occipital cortex of depressed patients – Chronic antidepressants may work indirectly on NMDA systems (altered subunit transcription, binding density) – Inhibitors of glutamate release (lamotrigine, riluzole) have antidepressant properties • Clinical studies using single dose ketamine infusions – Placebo-controlled, crossover, double-blind – May work through effects on mTOR (promotes synapse development) (Science 2010) 40 Single Dose Ketamine Infusion Studies (1) MADRS score •Diazgranados; Arch Gen Psych 2010 30 20 10 •Treatment refractory bipolar depression, unmedicated Ketamine Placebo 0 40 •Randomized, double blind, 2 period crossover •Assessments to 14 days 110 230 1 Minutes 2 3 7 10 14 Days Time after infusion 80 MADRS Responders (%) •Ketamine (0.5mg/kg) or placebo via 40 minute IV infusions 80 60 Ketamine Placebo 40 20 0 40 80 110 Minutes 230 1 2 3 7 Days Time after infusion 10 14 Single Dose Ketamine Infusion Studies (2) • Zarate, Arch Gen Psych 2006 • Treatment resistant MDD, unmedicated • Single 0.5mg/kg IV infusion; placebo controlled, crossover design 100 90 100 Percent of responders (>50% ↓HAMD) 90 80 80 70 70 Percent in remission (HAMD <7) Ketamine Placebo 60 60 (%) (%) 50 50 40 40 30 30 20 20 10 10 0 0 40 80 110 230 24 48 72 168 - - - - -mins- - - - - - - - - - - - - -hours- - - - - (time) 40 80 110 230 24 48 72 168 - - - - -mins- - - - - - - - - - - - - -hours- - - - - - (time) •Main side effects of ketamine: Perceptual disturbances and dizziness; confusion; elevated blood pressure; euphoria; increased libido •Generally occurred in 1st 20min of infusion. Glutamate and other disorders • All effective mood stabilizers influence glutamate signalling (generally ) – Li Glu transport; LTG Glu release, etc • Excess Glu signalling in alcohol withdrawal, epilepsy, ? anxiety GABA • Inhibitory amino acid neurotransmitter; both pre- and postsynaptic receptors • 2 receptors – GABA-A – ion channel • GABA-B – G-protein coupled receptor (heterodimer) Besides CNS, GABA also found in liver, GI tract, uterus, ovary, testis, lung, etc BDZs bind to the GABA-A Receptor -Ligand-gated receptor complex -Made up of 5 helical columns surrounding a chloride channel -Separate binding sites for •GABA, GABA agonists/ antagonists •benzodiazepines •barbiturates •ethanol •neurosteroids (pregnanolone) •convulsants (picrotoxin, PTZ) Resting state outside video plus GABA GABA plus GABA and BDZ GABA BDZ Cell membrane inside ClCl- Cl- Cl- Cl- ClCl- Cl- Cl- Cl- Cl- Benzodiazepine pharmacology Agonists Partial Agonists Anxiolytic Anticonvulsant Amnestic Sedating Diazepam Lorazepam Antagonists Neutral/ no effect Abecarnil Bretazenil Flumazenil Partial Inverse Agonists Inverse Agonists Anxiogenic Convulsant Promnestic Arousing FG7142 DMCM Clonazepam (all BDZs and Z-drugs in clinical use) Pharmacological theories of Anxiety (1) - GABA theories • Observations: • positive modulators of GABA-A receptor are anxiolytic (BDZs; barbiturates; ethanol) • negative modulators are anxiogenic (FG7142; metrazol) in normals • flumazenil (BDZ antagonist) is anxiogenic in panic disorder but not in healthy controls; BDZs are less sedating/impairing in anxious patients than in controls Agonists -anxiolytic -diazepam, etc Antagonists -neutral/no effect -flumazenil Inverse Agonists -anxiogenic Normal Panic Disorder Agonists are less sedating Antagonists are anxiogenic Pharmacological theories of Anxiety (1) - GABA theories • Observations (cont’d): • Altered GABA-A PET binding in panic disorder •15-BDZ naïve, drug free patients with panic disorder and 18 controls •Statistical parametric map illustrating an area where benzodiazepine receptor binding (11C-flumazenil) was decreased in subjects with panic disorder vs control subjects (R dorsal anterolateral prefrontal cortex). Arch Gen Psych 2008:1166