Assessment and Treatment of High Risk
Sexual Offenders: Practical Guidelines for
Clinicians
Jan Looman, Ph.D., C.Psych.
Kingston, Ontario
Jan1looman2@yahoo.ca
1
Assessment and Treatment of High Risk
Sexual Offenders: Practical Guidelines for
Clinicians
Note: The views expressed here are the
views of the author and do not reflect the
views of the Correctional Service of Canada
2
Outline
1. Models of Treatment - RNR vs. GLM
2. Describe triage process for sex
offenders in Ontario/Canada
3. What do I mean by “high
risk/needs”?
4. Describe treatment process for High
Risk/Needs Sex Offenders
5. Link to community treatment –
continuity of care
3
Models of Treatment
What really is RNR?
RNR vs. GLM
Is the Good Lives model different?
4
Models of Treatment
RNR model is not a theory of intervention in
itself – it represents principles of effective
correctional intervention (Andrews & Bonta,
2010)
derived from Andrews and Bonta’s general
personality and cognitive social learning
(GPCSL; Andrews & Bonta, 2010) theory of
criminal behavior.
5
Models of Treatment
GPCSL posits that crime results when the
personal, interpersonal, and community
supports for behavior are favorable to crime
Strong influences - antisocial attitudes,
antisocial associates, a history of offending,
antisocial personality traits.
Weaker influences - familial difficulties, poor
adjustment to work and school.
6
Models of Treatment
RNR Principles – guide us in designing
intervention within the GPCSL theory
The Risk Principle - that higher levels of
intervention should be reserved for higher
risk cases - low risk offenders should
receive no, or very little intervention.
Risk is to be determined through validated
actuarial assessment of static and dynamic
risk
7
Models of Treatment
The Need Principle - interventions should target
criminogenic needs (dynamic risk factors).
Central Eight risk/need factors (Andrews & Bonta, 2010):
–
–
–
–
–
–
–
antisocial associates,
antisocial cognitions,
antisocial personality pattern,
history of antisocial behavior,
substance abuse,
family–marital,
school–work,
– leisure–recreation.
8
Models of Treatment
Sex offender specific criminogenic needs
identified by Mann, Hanson & Thornton
(2010)
– Sexual preoccupation
– Sexual deviance – esp. deviant arousal to
children; multiple paraphilias
– Offense-supportive attitudes
– Emotional congruence with children
9
Models of Treatment
Sex offender specific criminogenic needs
(con’t)
– Lack of emotionally intimate relationships
with adults
– Lifestyle impulsiveness
– Poor problem solving
– Resistance to rules/supervision
– Hostility
– Negative social influences
10
Models of Treatment
Other factors identified as “Promising”
criminogenic needs:
– Hostility toward women
– Machiavellianism
– Lack of concern for others
– Dysfunctional coping
– Sexualized coping
– Externalized coping
11
Models of Treatment
Non –Criminogenic Needs Hanson & MortonBourgon (2005)
Force/violence in sex offending
Neglect or abuse during childhood
Sexual abuse during childhood
Loneliness*
Low self-esteem
Lack of victim empathy
Denial of sexual crime *
Low motivation for treatment at intake
Poor progress in treatment (post)
12
Models of Treatment
Within the Need Principle non-criminogenic
needs not relevant targets for intervention
A caveat to this: dealing with a
noncriminogenic need may be an important
strategy in the context of addressing a
specific responsivity factor.
Treatment providers must build on strengths
and remove barriers to effective participation
enhancing responsivity (Andrews, Bonta &
Wormith (2011)
13
Models of Treatment
The Responsivity Principle
1. general - the most effective interventions
tend to be those based on cognitive,
behavioral, and social learning theories
1. the relationship principle (Andrews, 1980) (establishing
a warm, respectful and collaborative working alliance
with the client) and,
2. the structuring principle (influence the direction of
change towards the prosocial through appropriate
modeling, reinforcement, problem-solving, etc.)
14
Models of Treatment
The Responsivity Principle
2. specific responsivity - the treatment offered
is matched not only to criminogenic need
but to those attributes and circumstances
of cases that render them likely to profit
from that treatment
15
Models of Treatment
Responsivity Factors (Looman, Dickie & Abracen,
2005; Olver, Stockdale & Wormith, 2011)
psychopathy
Low motivation/ denial/minimization
low intellectual functioning/lack of education
hostile interpersonal style/disruptive
Mental health difficulties
personality profile
16
Models of Treatment
Summary RNR
Treatment directed toward higher risk clients
Addresses known criminogenic needs
Cognitive behavioural/social learning
approaches
Emphasis on effective therapist
characteristics and role modeling delivered
in a manner appropriate for the client group
17
Evidence for RNR
Dowden and Andrews (1999) - meta-analysis of 25
studies of treatment for female offenders
effect sizes larger when criminogenic needs were
targeted.
treatment services which adhered to all of the RNR
principles found to be related to the greatest
reductions in recidivism, while treatment rated as
inappropriate had the weakest effects.
targeting vague personal/emotional targets, family
interventions not addressing criminogenic needs, and
other non-criminogenic personal treatment targets
were associated with no reduction in recidivism.
18
Evidence for RNR
Dowden and Andrews (2000) - meta-analysis 35
studies of treatments for violent offenders
criminal sanctions alone no effect on recidivism
any human service delivery significant positive
effect.
programs which adhered to RNR principles were
more effective than those which did not
Programs targeting criminogenic needs associated
with a moderate effect size - those which did not
produced no significant reduction in recidivism.
19
Evidence for RNR
Dowden and Andrews (2000) (con’t)
Programs that adhered to all three RNR principles
produced the largest effect sizes.
correlation between effect size and number of
criminogenic needs targeted was .69 (p <.001)
correlation between effect size and number of
non-criminogenic needs was -.30 (p <.05).
20
Evidence for RNR
Hanson, et al. (2009) - 23 studies of sexual
offender treatment
adherence to the RNR principles greater
reductions in recidivism
effect was linearly related to the number of RNR
principles adhered to.
programs which adhered to none of the principles
a negative treatment effect.
21
Evidence for RNR
Dowden, Antonowitz and Andrews (2003) - metaanalysis of 24 studies of treatment programs
which employed an RP approach in the delivery of
treatment.- (7 addressed sex off).
moderate overall effect size for RP programs
Coded presence of various aspects of the RP
approach (i.e., offence chain, relapse rehearsal,
advanced relapse rehearsal, identification of high
risk situations, training significant others, Booster
sessions, coping with failure situations)
22
Evidence for RNR
Dowden et al (2003)
Overall, the greater the number of RP components
employed in treatment, the stronger the treatment
effect (r = .38, p < .01).
found that RP programs which adhered to all three
RNR principles had the greatest impact, while
those that adhered to none of the principles had
no impact on recidivism.
23
Evidence for RNR
Summary
Treatment approaches which adhere to RNR
principles effective in reducing recidivism for
violent offending, female offenders, sexual
offenders
RP approaches which adhere to RNR principles
also effective
Approaches which focus on noncriminogenic
needs (for SOs internalizing psychological
problems denial, low victim empathy, and social
skills deficits) non-effective or even harmful
24
Models of Treatment
Good Lives Model
25
Good Lives Model
Assumptions about Human
Nature
Assumes all human being are practical
decision-makers and have similar
aspirations and needs
one of the primary responsibilities of
parents/teachers to equip people with the
skills/tools to make their own way in the
world
26
Good Lives Model
Assumptions about Human
Nature (con’t)
People formulate plans and
intentionally modify themselves and
their environment in order to achieve
goals
In order for people to function
effectively their basic needs must be
met
27
Good Lives Model
Assumptions about Human
Nature (con’t)
Primary human goods – have their origins in
human nature and have evolved in order to help
people establish strong social networks, survive
and reproduce
People derive a sense of who they are and what
matters from what they do (Practical identity)
Therefore in rehab need to provide offenders with
an opportunity to acquire a more adaptive practical
identity
28
GLM on RNR
Criticize RNR approaches
focus on risk reduction/management unlikely
to motivate offenders – need to have
approach goals
pay attention to offender as a whole - RNR
sees offender as “disembodied bearer of
risk”
Lack of focus on non-criminogenic needs –
therapeutic relationship
RNR approaches “one-size fits-all”
29
What Does the GLM Say
Nine* Primary Human Goods (Ward &
Marshall (2004):
1. life (including healthy living and optimal
physical functioning, sexual satisfaction);
2. knowledge;
3. excellence in play and work (including
mastery experiences);
4. excellence in agency (i.e., autonomy and
self-directedness);
30
GLM
Nine Primary Human Goods (con’t)
5. inner peace (i.e., freedom from emotional
turmoil and stress);
6. relatedness (including intimate, romantic
and family relationships) and community;
7. spirituality (in the broad sense of finding
meaning and purpose in life);
8. happiness; and
9. creativity.
31
GLM & Offending
Criminogenic needs = internal or external
obstacles that frustrate and block the
acquisition of primary human goods
Individual lacks the ability to obtain the good
in a prosocial manner and is unable to think
about his life in a reflective manner
i.e. criminogenic needs =deficiency in
agency and conditions that that support
agency
32
GLM & Offending
4 major difficulties with offender’s life
plans that lead to offending
1. Means he uses to secure goods
a) Inappropriate strategies Violation of norms
2. Lack of scope – important good missing
e.g., lack if connectedness feelings of
loneliness/inadequacy
33
GLM & Offending
4 major difficulties with offender’s life
plans that lead to offending (con’t)
3. Conflict among goods sought – e.g. attempt to
pursue good of autonomy leads to relationship
issues
4. Lack of capability – knowledge/skills deficits
34
GLM & Offending
Two routes to the onset of offending
1. Direct – offending is the primary focus – e.g.,
offender may lack the relevant competencies
and understanding to obtain the good of
intimacy with an adult – offending = striving for
fundamental goods – intentionally seeks
goods through criminal activity.
2. Indirect – pursuit of a good increases the
pressure to re-offend – e.g. conflict between
good of relatedness and autonomy leads to
break-up of relationship
loneliness/distress alcohol use offending
35
GLM & Offending
Offenders search for primary goods in their
environments under the guidance and
constraint of their practical identity
– Act in ways that they think will satisfy them
– Sex offending arises because people make
faulty judgements
– Lack of forethought or knowledge concerning
relevant facts
36
GLM & Intervention
Should be a direct relationship between
goods promotion and risk management
Rehabilitation = holistic reconstruction of the
self new practical identity
Focus on promotion of goods is likely to
automatically eliminate or modify risk factors
Attitude of therapist – offender viewed as
someone attempting to live a meaningful,
worthwhile life in the best way he can in the
specific circumstances confronting him
37
GLM & Intervention
Tailoring of therapy to match the individual
client’s life plan and their risk factors
Therapeutic task shaped to suit the person
in question
Focus on approach goals rather than
avoidance of risk factors
38
GLM & Intervention
Assumptions/Considerations (Laws &
Ward, 2011)
Offenders lack many of the essential
skill/capabilities to achieve a fulfilling life
Criminal behaviour = attempt to achieve
desired goods but the skills/abilities absent
– alternatively:
Criminal behaviour arises from an attempt to
relieve a sense of incompetence, conflict, or
dissatisfaction that arises from not achieving
39
valued human goods.
GLM & Intervention
Assumptions/Considerations (con’t)
Laws & Ward (2011)
The absence of certain goods more strongly
related to offending**:
1.
2.
3.
4.
Self-efficacy/sense of agency
Inner peace
Personal dignity/social esteem
Generative roles and relationships (work,
leisure)
5. Social relatedness (associates).
40
GLM & Intervention
Assumptions/Considerations (con’t)
Risk of offending reduced by assisting
individuals to develop the skills/abilities to
achieve the full range of human goods
Intervention = activity that adds to an
individual’s repertoire of personal
functioning rather than simply removing a
problem or managing a problem
41
Evidence for the GLM
Laws & Ward (2011) indicate (p. 202) that
the GLM has empirical support – however
they fail to offer any citations
The area of positive psychology generally is
empirically based however this cannot be
taken as evidence that such approaches are
effective with offenders
E.g. Deci & Ryan (2000) - self-determination
is positively correlated with personal wellbeing
42
Evidence for the GLM
Specific to Offenders?
Case studies – which do not tell us whether or
not effective in reducing recidivism or more
effective in addressing criminogenic needs
E.g. White, Ward & Collie, 2007 – Mr. C. gang
member with long criminal history of violence
including sexual violence
– Noted that he had engaged in RNR based
interventions on previous sentences
– Remained in pre-contemplation and rigid
antisocial attitudes, continued drug use
43
Evidence for GLM
Mr. C. (con’t)
Treatment according to GLM
Outcome – 14 months following release
Disclosed two violent incidents
“The first involved a retaliatory action after
being pushed to the ground at a party. … The
second relapse occurred in response to his
partner being insulted and offended. Mr. C’s
reaction included “smashing” the victim and
entering an emotional state synonymous with
the abstinence violation effect
44
Evidence for the GLM
Specific to Offenders?
Harkins, Flak, Beech & Woodhams (2012)
– 76 men who participated in GLM based
community SO treatment
– 701 who participated in an RP oriented
treatment
45
Evidence for GLM
Harkins et al.(2012) (con’t)
1. pre-post treatment psychometric
assessment – measures which previous
research demonstrated associated with
recidivism
2. Attrition rates
3. Facilitators perception of the program and
offender’s motivation
4. Offender’s perception of the program
46
Evidence for GLM
Harkins et al.(2012) (con’t)
Attrition rates did not differ significantly
No difference in rates of change on
psychometric measures
Facilitators liked the GLM-based module
63.7% did not think it would be appropriate
for high-risk/unmotivated clients
47
Evidence for GLM
Harkins et al.(2012) (con’t)
Clients rating of improved understanding of
their offending - 80% of RP group compared
to 46% GLM
better understanding of the positive aspects
of themselves 61% for GLM compared to
20% for RP
48
Evidence for GLM
Harkins et al.(2012) (con’t)
Rating re: changing thoughts and attitudes
in a way that they were better able to
manage themselves or their reoffending
80% for RP, vs. 27% for the GLM module
thoughts and attitudes about themselves or
the future were more positive - 47% for GLM
vs. 20% for the RP module.
49
Evidence for GLM
Harkins et al.(2012) (con’t)
Summary
GLM module led to offenders who feel better
about themselves and their future, however
did not improve their awareness of risk
factors and self-management strategies
Opposite was true for RP/RNR based
program
no differences overall in terms of attrition or
change on risk factors
50
GLM vs. RNR
Does GLM say anything that RNR does not?
GLM: Criminal behaviour arises from an
attempt to relieve a sense of incompetence,
conflict, or dissatisfaction that arises from
not achieving valued human goods
RNR approach: crime results when the
personal, interpersonal, and community
supports for behavior are favorable to crime
51
GLM vs. RNR
RNR focuses on the Central Eight addressing such needs as lack of education
and employment and lack of supportive,
rewarding, and prosocial familial and marital
relationships
GLM identifies 9 “goods” with a great deal of
overlap with the Central eight
52
GLM vs. RNR
GLM goods
RNR Central Eight
1. Knowledge
1. Schooling/Employment
2. Excellence in Play and 2. Employment/leisure
Work
3. Autonomy
3. Employment/cognitions/
attitudes
4. Inner peace
4. Antisocial cognitions;
antisocial personality pattern
5. Relatedness/
5. Associations/Family marital
Community
6. Spirituality
6. Antisocial attitudes
7. Happiness/Creativity
7. Leisure/work/family/
53
associates
GLM vs. RNR
Both models discuss the importance of
acquiring skills
Ward et al. claim that the GLM addresses
criminogenic needs by building strengths and
being positively oriented
Andrews & Bonta(2010) discuss the
importance of prosocial skills building and rolemodeling by treatment providers
54
GLM vs. RNR
Wormith, Gendreau & Bonta (2012) - some
of the professed shortcomings of RNR and
alleged differences between RNR and GLM
are illusory.
– E.g., the difference between addressing deficits
and building strengths. From a practical fieldlevel perspective, the difference is mostly
semantic
55
GLM vs. RNR
The need to use approach goals and
positive language is a contribution – field too
often focused on negative
No evidence this leads to greater benefit
from treatment
56
RTC Sex Offender Program
1. Triage Process
2. What do I mean by High Risk/Needs
3. RTC program
57
Triage Process in
Ontario
RTCSOTP in operation from 1972 to
2011
Only institutional sex offender program
in Ontario until 1989
WSBC initiated at that time
1992 Sex Offender Assessment Team
established at the Millhaven
Assessment Unit
58
MAU Assessment
MAU Sex Offender Assessment team
assesses all sex offenders entering the
Federal prison system in Ontario
In Canada sentence 2+ years served Federally
Assessment addresses level of risk
(actuarial) and treatment needs
59
MAU Assessment (con’t)
Initially used PCL-R, SORAG, LSI-R,
RRASOR and case history
added Static-99/STABLE when
available
Dropped PCL-R/SORAG in 2002
60
MAU Assessment (con’t)
1995 - developed first National
Standards for sex offender
treatment
established Low, Moderate and High
Intensity designations
61
Intensity Levels
With Standards we (i.e., regional sex
offender program directors) adopted
these levels of intensity
RTCSOTP=high
WSBC=moderate
Bath (est. ~ 1992) low-moderate
late 1995 RTCSOTP focus on high
risk, high treatment needs offenders
62
Intensity Levels
Risk/Needs defined according to
RNR principles:
Risk assessed actuarially
Need defined in terms of
established criminogenic needs
(intimacy deficits, attitudes,
deviant arousal, problem solving,
social competence, etc.)
63
Moderate
WSBC
Low-Mod
Bath
MAU
HISOP
RTC**
**Low
Pittsburgh
64
RTC Sexual Offender
Treatment Program
65
RTCSOTP
Description of the Clientele
Program Components
Outcome data
66
Actuarial Risk
Instrument
RTC sample (sd, n)
WSBC sample (sd,n)
VRAG
11.7 (10.9, 233; risk bin 6)
3.15 (8.70, 468; risk bin 5)
SRAG
18.3 (11.8, 215; risk bin 6)
7.77 (11.59, 468; risk bin 4)
PCL-R
22.8(7.8, 248)
16.50 (7.11, 442)
LSI-R
29.7 (9.1, 147)
------
RRASOR
2.23 (1.4, 276)
1.72 (1.35, 468)
Static-99/
Static-99R
5.5 (2.0, 308) / 5.3 (2.2, 308)
3.44 (2.11, 468)
67
Changes over Time
Static99R %
high
risk
Sample
1993- 40.0
1995
Sample 66.0
1998 to
present
SRAG VRAG LSI-R
%
% high %
High
risk
high
risk
risk
PCLR%
high
risk
RRASOR VRS% high
SO %
risk
high
risk
44.6
29.9
29.4
17.5
28.0
46.6
65.0
72.1
53.3
31.3
40.0
73.7
68
Program Differences
Hi
Mod
Lo-Mod
Lo
LSI-R b
25.1
21.9
17.3
10.3
Static-99a
5.9
4.1
2.9
1.6
STABLEa
9.5
7.0
4.8
3.5
Note: aHi intensity differs from Moderate
bHi intensity same as moderate but different
from other groups
69
Diagnosis
Finally, use DSM diagnoses to
determine the presence of increased
responsivity needs
looked at 48 consecutive admissions to
the SOTP (in 2005)
37 (77.1%) meet criteria for a personality
disorder
15/37 (40.5%) have personality orders described
as “severe” by the diagnostician (e.g., BPD,
Narcissistic, psychopathy)
70
Diagnosis (con’t)
Behaviours resulting from these PD’s
lead to management difficulties in their
parent institution, including long-term
segregation (15, or 31%)
16/48 (31.3%) suffer from mood
disorder (Depression, Bipolar
Disorder)
10 (28%) suffer from psychosis
71
Diagnosis (con’t)
22 (45.9%) met the criteria for a
paraphilia, most often sexual sadism
or pedophilia
Nine of these 22 (41%) also meet
criteria for severe personality
disorder – typically psychopathy or
borderline
72
Deviant Arousal
Every admission to our program assessed
via PPG
Men with child victim audio child sexual
violence assessment (Quinsey & Chaplin,
1988)
Men with adult victims adult sexual violence
assessment (Quinsey, Chaplin & Varney,
1981)
73
Deviant Arousal
40% of adult rapists deviance on adult
sexual violence assessment
92% of child molesters deviant on child
sexual violence assessment
24% of sample (n=657) non-responders
74
RTC Sex Offender Treatment
Program
Designed to be delivered over ~7 months
13-session intro module then
Two primary components
1. Self Management – Disclosure; Cognitive
Distortions; Emotions Management;
Development of Behavioural Progression;
Development of Self Management Plan
2. Social Skills – Communication Skills; Goal
Setting; Problem Solving; Empathy;
Assertiveness; Relationships
75
RTC Sex Offender Treatment
Program
4-5 group sessions per week (ideally 4) and
one individual therapy session
Either alternate between Self Management
and Social skills sessions (if two different
delivery teams) or alternate modules
In addition milieu therapy – program staff
interacting with offenders in unstructured
manner on living unit
76
Program Delivery Schedule
Monday
Tuesday
Wednesday
Thursday
Friday
SelfAM
Management
B Group
Self-
Self-Management
Social Skills A&B Social Skills
PM
Management
A
groups
A&B groups
Group/Social
A Group
Skills B Group
77
Program Structure Related to
Criminogenic Needs
Criminogenic Need
Treatment components
Antisocial Associates/Negative
Social Skills/ Milieu
Social Influences
Antisocial cognitions/Offence
Cognitive Distortions/
Supportive Attitudes/emotional
Individual Therapy/Social
congruence with Children
Skills/Milieu
/Resistance to Rule/Supervision
Antisocial Personality Pattern
Cognitive Distortions/
/Lifestyle Impulsiveness
Emotions Management
/Individual Therapy
78
Program Structure Related to
Criminogenic Needs
Criminogenic Need
Treatment components
Substance Abuse
Emotions Management
/Individual therapy
Family/Marital problems/Lack
Social Skills / Milieu
of emotionally intimate
relationships with adults
School-work
Leisure/recreation
Social Skills/
Self-Management /Milieu
79
Program Structure Related to
Criminogenic Needs
Criminogenic Need
Treatment components
Sexual Preoccupation
Emotions Management
/Relationships/ Individual
Therapy
Sexual Deviance
Arousal Management/
Emotions management/
Individual
Poor Problem solving
Problem Solving
Hostility/dysfunctional
Emotions management /
emotions
Individual therapy
80
Treatment Components
Wong & Hare (2005) identify as treatment
targets for psychopathic offenders
1. Dysfunctional attitudes and behaviors
2. Dysfunctional emotions and lack of emotional
control
3. Failure to accept responsibility for their own
actions
4. Substance abuse
5. Lack of work ethic, employable skills and
appropriate leisure activities
6. Antisocial peers, networks and subculture
81
Introductory Module
Introduces offender to the program
Group rules (arrived at through group
discussion)
Treatment concepts/Jargon (CBT, Offence
Chain etc.)
CBT – the idea that thoughts and
behavior are related new to clients
– Examples to illustrate
82
Introductory Module
“goof”
need to fight
“I need to retaliate otherwise people
will think they can push me around”
“I don’t think – I just react”
83
Introductory Module
“I need to retaliate otherwise people
will think they can push me around”
84
Introductory Module
Motivational Issues
Psychopathic clients often poorly motivated
to change
Motivation to change typically self-focus (get
out of prison – “good report”)
Work with what you’ve got
First sessions focused on motivation/goal
setting – finding reason for change
85
Introductory Module
Process of change
– How we begin the change process
– Cost-benefit analysis of changing
– Possible selves – how do you see yourself after
you’ve completed the program
– Realistic expectations for the future
86
Change Process
Have offender identify a role model
“Can you name anybody from your life who is
not a criminal that you might use as a role
model?”
Old me /New me homework
87
Old Me New Me
Old Me
What would you like to change about your
personality and how you act?
What strengths do you have that will help you to
make these changes?
New Me
Based on these changes what do you think the
new me will be like?
What goals do you have for yourself in this
program?
88
Treatment Motivation/Goal
Setting
Importance of setting goals
SMART principle
– S = SPECIFIC
– M= MEASURABLE
– A= ACHIEVABLE
– R= REALISTIC
– T= TIME LIMITED
Require them to set some goals for the
program and monitor progress
89
Introductory Module- Consent
Discussion early on in program to start
offenders thinking about issues of consent
– What is consent
– Conditions necessary for consent
– have to be willing to have sex
– have to be able to understand possible
consequences of consenting
– e.g. STDs, pregnancy
– need to be sober
– Must be of age
90
Introductory Module- Consent
Consent negotiated
Reasons for age of consent
Legal age vs. age appropriate
Consent scenarios
91
Consent Scenarios
1. You are in a bar and you are getting along well
with a woman who seems quite interested in you.
However, you realize that she looks quite young although it is certainly possible that she is 19
years old. What do you do?
2. Your 13 year old step-daughter comes into the
room in a see-through night gown and cuddles up
to you on the couch. No one else is home. Is she
indicating that she is sexually interested in you?
92
Consent Scenarios
3. You have met the same woman at the bar you
like to go to several times before. Tonight things
have become very friendly and you think that she
really likes you. At closing time you ask her back
to your place for a drink. She accepts. What would
you do from here?
4. Same situation as above except that you have
been “fooling around” (i.e., kissing and caressing
each other) while at the bar. At closing you ask her
if she would like to “continue this at your place” she accepts. Do you have consent? Consent for
93
what?
Sex and the Media
Discussion of the effects of media on sexual
attitudes and behavior
foster skills necessary to exercise
responsible and healthy personal choices in
using media
pornography = any media that promotes
unhealthy beliefs about sexuality, exploits
sexuality for commercial purposes, or is
sexually degrading.
degrading towards both women and men
94
Sex and the Media
media that is legal can be used for
unhealthy purposes.
use legal pornography to prime deviant
fantasies.
possible to use material that is not usually
thought of as pornography to prime deviant
fantasies. E.g. TV shows, movies,
commercials or magazine ads
95
Autobiography
and
Disclosure
96
AB & Disclosure
AB outline handed out during the second
intro session
Given specific deadline (i.e., first disclosure
will occur…)
Meet with therapist a couple of times to
discuss and track progress
Less than 10 pages too short, more than 30
too long
97
AB & Disclosure
includes information regarding times in their
lives where they have engaged in criminal
behaviour
also periods where they have managed to
remain crime free.
What was going on when things were going
well vs. when things were going poorly
98
AB & Disclosure
Disclosure – one session per offender
30-45 minutes presentation, break then
questions ~ 30 minutes
Content of disclosure
– brief personal background
– Relationship history
– Offences – but no specific detail
99
AB & Disclosure
Questioning – by all group members
Clarification
Supportive challenging of
minimization/denial
Not confrontational – Marshall, Marshall,
Serran & O’Brien (2011) – therapists who
present as warm, empathic, rewarding and
directive, but not confrontational most
effective
100
AB & Disclosure
Goal of these exercises/sessions to
increase accountability/openness about
offending/sexual deviance
NOT looking for the “truth”
Official version not the true version of events
– Trauma effects recall
– Reconstructive nature of memory
101
AB & Disclosure
DO NOT expect offender’s account to match
the official version
plausible explanation of offence that does
not include victim blaming and that
acknowledges impact
Is this approach effective in terms of
increasing accountability?
102
103
AB & Disclosure
104
AB & Disclosure
Slight nonsignficant tendency for men
discharged from treatment to deny
– E.g. 36% of discharged deny facts
pretreatment compared to 26% of
completers
105
AB & Disclosure
Who gets discharged?
attrition table.rtf
only disruptive behavior predicts discharge
106
107
Static-99R
B
SE
Wald
df
p
Exp B
.100
.043
6.65
1
.036
1.09
8.14
2
.017
Denial of Impact – full
acknowledgement
Denial Of Impact –
some
acknowledgement
-.87
.307
7.99
1
.005
.420
Denial of impact – no
acknowledgement
-.27
.203
1.72
1
.190
.767
10.84
2
.004
Denial of sexual
motivation –
acknowledgment
Denial of sexual
motivation – some
acknowledgement
.77
.274
7.62
1
.006
2.128
Denial of sexual
motivation – no
acknowledgment
.69
.292
5.564
1
.018
1.993
108
Cognitive Distortions
Cognitive distortions component
Focus on becoming aware of
distorted thinking
Both generally criminal and
associated with sexual offending
Challenging cognitive distortions
without being confrontational.
Use the group process
109
Cognitive Distortions
What information has the client previously
provided which is contradictory to the
distortion?
What is the evidence for the thought?
Remain neutral.
110
Cognitive Distortions
Use of ACT model to challenge
distortions
1)Awareness of distorted thinking.
2)Choose to think rationally (what is true,
what is not).
3)Take action - Replace with appropriate
thoughts.
111
Cognitive Distortions
Important notion re: cognitive distortions is
the idea of excuse making
Mann & Maruna (2006; Mann & Ware, 2012)
– normal human tendency toward excuse
making
– excuse making is “the process of shifting
causal attributions for negative personal
outcomes from sources that are relatively more
central to the person’s sense of self to sources
that are relatively less central” p. 156
112
Cognitive Distortions
‘fundamental attribution error’ … many of
the rationalizations and minimizations
offered by offenders may be situational
rather than dispositional.
“When challenged about having done
something wrong, all of us reasonably
account for our own actions as being
influenced by multiple, external and internal
factors. Yet, we pathologize [offenders] for
doing the same thing.” p. 158
113
Cognitive Distortions
No win situation:
“If they make excuses for what they did,
they are deemed to be criminal types who
engage in criminal thinking. If, however, they
were to take full responsibility for their
offences – claiming they committed some
awful offence purely ‘because they wanted
to’ and because that is the ‘type of person’
they are – then they are, by definition,
criminal types as well.” p. 158
114
Cognitive Distortions
Zuckerman (1979) – people make
predominantly external attributions for our
failures and predominantly internal
attributions for our successes.
Argue that we need to be more
sophisticated in our approach to cog.
Distortions
115
Cognitive Distortions
excuse making is a highly adaptive
mechanism for coping with stress, relieving
anxiety and maintaining self-esteem.
Those who assume full responsibility for
their failings put themselves at risk of
suffering depression.
116
Cognitive Distortions
‘revised helplessness theory’ (Abramson,
Seligman, and Teasdale,1978) individuals
who have an explanatory style that invokes
internal, stable and global attributions for
negative life events (and external, unstable
and specific attributions for positive events)
will be most at risk when faced with
unfortunate circumstances, such as the loss
of a job or a relationship breakup.
117
Cognitive Distortions
Hanson & Morton-Bourgon (2004) no
relationship between denial of sex crime or
minimizing responsibility and recidivism
However more recent research has shown
that there is a relationship between denial
and recidivism for some offenders
118
Cognitive Distortions
Also note that there is no evidence to
support the notion that cognitive distortions
(as distinct from offence supportive
attitudes) predict recidivism
119
120
Static-99R
B
SE
Wald
df
p
Exp B
.100
.043
6.65
1
.036
1.09
8.14
2
.017
Denial of Impact – full
acknowledgement
Denial Of Impact –
some
acknowledgement
-.87
.307
7.99
1
.005
.420
Denial of impact – no
acknowledgement
-.27
.203
1.72
1
.190
.767
10.84
2
.004
Denial of sexual
motivation –
acknowledgment
Denial of sexual
motivation – some
acknowledgement
.77
.274
7.62
1
.006
2.128
Denial of sexual
motivation – no
acknowledgment
.69
.292
5.564
1
.018
1.993
121
Cognitive Distortions
it could be that offenders attempting to
rationalise their deviant behaviour may
exhibit other low-risk characteristics and feel
a need to justify their atypical behaviour,
whereas offenders admitting their deviant
actions may see no need to justify behaviour
that is consistent with their internal
representations of self.
122
Cognitive Distortions
Cognitive Distortions that
Impede Empathy
Do not have victim empathy/empathy
training component
Mann et al. (2011) – victim empathy
not associated with recidivism
123
Cognitive Distortions
Instead discuss cognitive distortions
that impede empathy
View videos to illustrate victim impact
Discuss specific distortions used to
shut down empathy
124
Attitudes
Discussion of helpful vs. harmful
attitudes
– How do we know?
How do positive attitudes affect our
behaviour?
125
Attitudes
Mr. Brown was released from prison two weeks ago
and has been looking for a job. He has circled yet
another ad and is on his way to another interview. He
has been rejected four times even though he feels that
he is well qualified to do each job. Here is an example
of what he is saying to himself,
"I don't know why I'm even bothering to see the boss.
I've never been able to get a good job before. I'm just
a fucking failure, an ex-con. I have no money left and I
won't lower myself to get welfare. I won't be able to
pay the rent and I'll be kicked out of my apartment. If I
don't get this job, I might as well just go back to jail. I
knew I'd never make it. I might as well use the rest of
my money and get drunk."
126
Attitudes
"Why will he never be able to get a good job?"
"What does Mr. Brown define as a failure?" "Is
getting a job the only way to define success
and failure?"
"If there is no money left, are there other
sources of money?"
"Why is getting welfare more problematic than
going back to jail?"
"Is getting drunk a good coping strategy?"
"What can it lead to?"
127
Attitudes
Identify the negative attitudes expressed
which positive attitudes could be substituted
How can these attitudes affect reintegration
and relapse.
Identify attitudes related to areas such as
self worth, success, using support, attitudes
towards change, etc. and how these relate
to thoughts, feelings and behaviours
128
Emotions Management
Emotions Management
Component
– Addresses coping with difficult
emotional states – loneliness, jealousy,
depression etc.
– Cognitive strategies – self-talk,
challenging distortions
– Behavioural strategies – relaxation
– Acceptance of negative emotions
129
Emotions Management
Awareness of emotions – how do we
know what we are feeling?
– Bodily signals
– Self talk
Self monitoring homework
Discussion of various “high risk” emotions
– Sadness, anxiety, anger, hostility, loneliness,
shame/guilt, self pity
130
Emotions Management
Also discuss positive emotions which
may place someone at risk
– Distorted cognitions which accompany
feelings of happiness related to
success/accomplishment
Link these emotions to behavioural
progression
131
Emotions Management
Anger
Discussion of role of anger
– It is a “normal” emotion
– can be helpful
Cognitive and physical signals related to
anger
Addressing cognitive distortions that lead
to anger
132
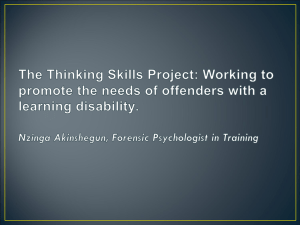
Emotions Management
Anger
Rating anger on a scale of 1-10 rather
than using emotionally based language.
What does “anger 7” look like? Why is this
important?
Anger funnel discussion.
133
Anger Funnel
Disappointment
Sadness
jealousy
Loneliness
Boredom
ANGER
134
Emotions Management
When Is Anger A Problem?
– When it is too frequent.
– When it is too intense.
– When it lasts too long.
– When it leads to aggression.
– When it disturbs work or relationships.
– When it is unresolved.
– When it hurts others.
– When it is sexualized.
135
Emotions Management
Strategies for managing emotions
– Assertion vs. aggression
– Self-talk
– Relaxation/mediation/mindfulness
– Effective communication
136
Emotions Management
Sexual arousal
Discussion the notion that sexual arousal is
a feeling
– Can be managed like other feeling
– Don’t need to act on it
– Same strategies apply
Discussion of arousal management
strategies
137
Arousal Management
Individual therapy sessions
Every offender discussion of fantasy and
how it relates to offences
Sexual fantasy monitoring
discussion of specific role fantasy plays in
life/offending (e.g., sex as coping)
social skills training, strategies to deal with
negative emotionality (e.g., anger,
depression)
138
Arousal Management
Fantasy/arousal modification
Covert sensitization
– develop fantasy scripts – deviant and
appropriate
– Develop strategies for controlling arousal
– In lab – monitor arousal while reciting script
– Use strategies to diminish arousal – then use
appropriate fantasy to generate arousal
– If not successful refer to psychiatrist
139
Behavioural Progression
Different ways of doing BP – e.g. Yates
Kingston & Ward (2010)
Prefer simple
Series of thoughts, feelings and behaviours
which culminate in sexual offence
Clients to identify 7-10 such sequences
If multiple offences chose “typical” offence
140
Behavioural Progression
OFFENCE CHAIN EXAMPLE.docx
4 wife chain.docx
approach goal.docx
approach chain.docx
141
Behavioural Progression
Also ask for distal factors related to
offending
– Background factors
Abuse
Substance abuse
Relationship problems
Present to group
Constructive feedback
142
Social Skills
Component
143
Social Skills Component
Majority of high risk/needs clients lack in
basic social skills
Risk factors
– Antisocial peers, networks and subculture
– Loneliness, lack of prosocial relationships, poor
job prospects, intimacy
Focusing on enhancing skills to
develop/maintain prosocial relationships
Heavily focused on skill-building
144
Social Skills Component
Values identification
– Serves as basis for much of discussion in
coming components
– What are my values?
– making decisions, solving problems and
communicating with others.
– Decisions that support our values enhance our
ability to solve problems and help us live prosocial lives
145
Social Skills Component
Communication Skills – oriented
toward developing appropriate
relationships
– Replacing aggressive communication (which
has likely been reinforcing for the client in the
past) with listening skills and active listening
– Emphasis on costs and benefits of aggressive
communication (decision matrix)
146
Social Skills Component
Problem solving/Assertiveness
– Recognize when they are facing a problem and
develop appropriate strategies to cope (as
opposed to substance abuse, violence and sex)
– Skills allow them to maintain supportive
relationships and end inappropriate one
– Help them to keep jobs
147
Social Skills Component
Relationship Skills:
– Emotions matter even if they are difficult to
figure out. At least need to understand that
they matter to other people and be able to
differentiate basic emotions.
– Dealing with jealousy
– Negotiating consent
– How to chose a partner
– Avoiding impersonal sex
148
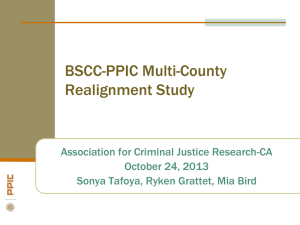
Relationship Skills
Disclosing criminal history to partner
Role play
Privacy circle discussion
Describes the development of
relationships
From stranger to intimate
relationships develop
3-date rule
149
Relationship Skills
150
Relationship Skills
Ideal Partner – asked to describe in terms
of: Appearance, Attitudes, Education, Career,
Personality traits, interests/hobbies,
Religion, Cultural background,
– Rank importance - 1 to 8
Is their ideal partner consistent with the
values they identified earlier?
151
Relationship Skills
What do they bring to the relationship –
what can they offer
Often expect more from a partner than
they themselves are able to give.
Lead to discussion of re-evaluating what
their expectations of a relationship are –
idea of compromise
152
Relationship Skills
Maintaining Relationships
– Relationships require work
– Face strain from change – children, job loss
– Other relationships – in-laws
Show respect
Be honest and truthful
Do little things to show you care
Treat your partner as an equal
Take equal responsibility
Make time (for family, for partner, for yourself)
Be open to change
Maintain individuality/respect individuality of
partner
153
Relationship Skills
Coping with loneliness, rejection and
jealousy
Being alone vs. loneliness
– What does it mean to “be alone”
– Advantages of not having a partner
Rejection – what does it mean when
someone rejects you?
– Possible reasons for rejection
– Ways to cope
154
Relationship Skills
Coping with loneliness, rejection and
jealousy
Jealousy – what is jealousy and why do
we feel it
– When you don't feel good about yourself
– When you are dependent on your partner for
your happiness
– When you don't enjoy spending time alone
– When you lack social skills
– When your expectations aren't being met
– When you've made the wrong partner choice
155
Relationship Skills
Coping with jealousy
Try to determine if the jealousy is based
on fact or fear
Communicate your feelings to your
partner in the very beginning
Don't allow negative self-talk to get out of
hand
Negotiate with your partner ways to avoid
situations that perpetuate the jealousy
Seek counselling
156
Self Management
Component
157
Self Management
Puts everything from program together
Remind themselves of goals/reasons for
change
Identify risk factors and main coping
strategies
Relapse Cues
Appropriate use of leisure time
Main sources of support
Present/discuss in group
158
Individual therapy
component
159
Individual therapy component
Address issues unique to the individual not
addressed in group
Follow-up on issues which come up in group
Assist with homework
Arousal work
160
Individual therapy component
Substance Abuse
– CSC has comprehensive substance abuse
programming therefore do not target directly in
SOTP
– Discuss role substance abuse plans in offence
progression
– Importance of avoiding substance abuse in risk
management/prosocial lifestyle
– Don’t mix substance use and sex
161
Individual Therapy
Importance of rapport.
Understanding that treatment with such
clients is a long term undertaking.
Prepare offender for dealing with the
lapses that WILL occur
Drug use
Fighting
Angry outbursts
162
Individual Therapy
Manipulative Behaviours
– Need to keep perspective in that these can be
expected with High PCL-R clients.
– Need for team communication.
– Meetings with the client and all those involved
in manipulative communications. That way
everyone hears the same thing
– Behavioral contracts .
– What is the client really after-Is it a reasonable
request?
163
Program Referrals
RTC
WSBC
Maintenance
Bath
SOP
164
Treatment Outcome
Table 4
Risk percentages for different Static-99R scores compared to published values
Static-99R Developmental Developmen Observed
Observed
score
Sample
tal
sexual
violent
Sexual
Sample
recidivism
recidivism
Recidivism
Violent
Recidivism
%
%
%(N)
95%CI
%(N)
LT 2
4.3
7.4
0.0 (6)
20.0(10)
2
9.1
15.7
0.0 (10)
0
3
11.9
20.3
12.5 (16)
3.5 to 36.0
17.6 (17)
4
15.4
25.8
8.1 (37)
2.8to 21.3
21.6 (37)
5
19.6
32.1
7.4(27)
2.0 to 25.8
25.9(27)
6
24.7
39.2
25.7(35)
13.1to 43.6
46.2(39)
7
30.6
46.8
25.0(20)
9.5to 49.4
40.9(22)
8
37.2
54.5
25.0(20)
9.5 to 49.4
35.0(20)
9
44.3
62.0
30.0(10) 10.7 to 60.3 66.7(12)
10+
51.6
69.0
25.0 (4)
4.5 to 69.9
25.0 (4)
Total
18.0
25.0
8.9(23)
5.4 to 12.4
31.8(63)
Recidivism
Mean score
3.15
5.4
(95%CI)
5.7 to 50.9
6.2 to 41.0
11.4 to 37.2
13.2 to 44.7
31.5 to 61.4
23.2 to 61.3
18.1 to 56.7
39.1 to 86.2
4.5 to 69.9
5.8 to 62.4
165
Treatment Outcome
Table 5
Risk percentages for different SORAG risk bins compared to published values
SORAG
Risk Bin
1
2
3
4
5
6
7
8
9
Total
Recidivism
Total
sample N
Developmental
Sample
Violent
Recidivism
%
7.0
15.0
23.0
39.0
45.0
58.0
58.0
75.0
100.0
Harris et
al.
(2003)a
Observed
violent
recidivism
%
19.0
18.0
29.0
50.0
55.0
63.0
63.0
71.0
76.0
%(N)
0
16.7(1)
10.5(2)
13.3(4)
31.7(13)
35.7(15)
33.3(11)
56.8(25)
57.1(16)
40.4
48.0
34.1
178
396
250
95%CI
-13.1 to 46.5
-3.4 to 24.4
10.9 to 25.7
17.5 to 45.9
21.2 to 50.2
17.2 to 49.4
42.2 to 71.4
38.8 to 75.4
166
Treatment Outcome
Sexual Recidivism for men with PCL-R
scores over 25 AND Static-99 over 5
n=70 follow-up 4.5 years
15.7% new sexual conviction
psychometric table.docx
167
Treatment Outcome
% Sexual
Recidivism
% Any Violent
recidivism
RTC only (n=152)
11.8
24.3
RTC + Mod (n=24)
8.3
12.5
RTC+ Mod +
Maintenance (n=11)
0
0
168
Community Treatment &
Supervision
169
Community Supervision
Community treatment of high risk sexual
offenders picks up where institutional
treatment ends.
The aim of community treatment is not to
discuss the same material as was covered
in institutional treatment programs.
The goal is to apply the knowledge which
offenders have gained in institutional tx. to
community settings.
170
Community Supervision
For example, institutional treatment
programs typically focus on intimacy deficits
as one aspect of dynamic criminogenic risk.
Institutional programs may teach the
offenders some of the communication skills,
skills related to dealing with jealousy,
knowledge of sexuality that will increase the
odds of these clients being able to establish
and maintain intimate relationships.
171
Community Supervision
However, it is not until these clients enter
the community that the majority may have
the opportunity to use these skills in
developing a relationship.
Issues such as disclosure of offense history,
overnight visits and having the partner meet
with correctional staff all need to be
addressed.
172
Specific Challenges with High Risk Offenders
Manipulative behaviors
– Need for frequent contact with team members
involved in management of the case.
– Control of living environment.
– Checks with employers at worksite/via phone.
– Meeting with partners of offenders.
– Consequences of inappropriate behaviors
discussed.
– When possible, suspension is avoided.
173
Specific Challenges with High Risk Offenders
– Consequences of inappropriate behaviors
discussed.
Where possible these are discussed as
opportunities to learn (e.g., thinking that you
can put yourself in high risk situations).
– Aggressive Behaviors:
Fighting is clearly not permitted and almost
always results in suspension.
Threatening and aggressive communication
is discussed in sessions and contributing
factors addressed.
174
Community Supervision
Particularly with high risk offenders, there is the
need to watch for them falling into old patterns of
behavior (e.g., lying about their offence history to a
prospective partner, simply not informing
correctional staff about the fact that they are
dating someone).
We put few constraints on who sex offenders can
date with exception to child molesters being
involved in relationships with those who have
children.
175
General Guidelines
For high risk offenders it is best that they be
housed in a Community Correctional Centre
(CCC) or equivalent.
These settings offer offenders with few means of
support a place to live and provide enough money
for basic needs.
Offenders must sleep at the CCC unless
authorized in writing to stay elsewhere.
Team Supervision Unit (TSU) as another option.
176
General Guidelines
If possible, parole officers and psychology staff
should be housed within the same building.
In the Toronto area all sex offenders must be
assessed for treatment by staff in the psychology
department.
It is assumed that, except in rare circumstances,
all offenders with a recent sexual offence
conviction will attend one of several sex offender
specific treatment programs.
177
General Guidelines
Having psychology in the same building as
CCC/TSU makes it easier for those who are only
allowed limited access to the community to attend
treatment.
Meetings between parole officers, psychology
staff, parole supervisors occur on a regular basis.
STABLE 2007 is scored on offenders on a yearly
basis/STATIC-99/99R is scored if not available on
file
Individual therapy and/or group treatment are
available.
178
Sex Offender Maintenance
Treatment Program-Central District
Clients attend treatment until WED.
Groups begin with check in.
Issues of mutual concern typically arise.
Those issues related to criminogenic factors
(relationships, high risk situations) receive
more attention.
Clients are asked to present a synopsis of
their behavioral progressions, behavioral
management plans to group.
179
Specific Challenges with High Risk Offenders
The goal is to keep clients in the community
and when suspension is necessary, release
them at the earliest possible date.
There is a need to compromise with clients
on a variety of issues.
Context becomes very important in decision
making.
– How has the offender been doing in the
community to this point in time.
– Are we hearing about other difficulties with
client from residents at CCC.
180
Specific Challenges with High Risk Offenders
Substance Abuse
– Decision to suspend is client and context
dependent.
– More serious drugs (e.g., opiates) typically
result in suspension whereas there is more
flexibility with less serious drugs (e.g., THC
based drugs).
– Issues associated with lapses/relapse
addressed in detail.
181
Legal Issues and Impact on Treatment Decisions
In Canada legislation which is similar in
principle to sexually violent predator
legislation in the U.S. generally falls within
two categories:
– Dangerous Offender (DO) Legislation
– Long Term Offender (LTSO) Legislation.
182
Dangerous Offender Legislation
Criteria for DO designation:
– Demonstrated failure to control sexual impulses
– There is a likelihood of causing injury, pain, or
other evil to other persons in the future
– Because of the brutal nature of the offence.
Typically reserved for offenders with
extensive criminal histories.
Must be convicted of a serious personal
injury offense.
183
Dangerous Offender Legislation
Between 1977 and 1997 upon finding an offender
to be a DO a judge could sentence the offender to
either a determinate or indeterminate sentence.
In 1997, the law was amended and determinate
sentences were removed as a sentencing option.
90% of DOs are sex offenders.
88% have a previous record of incarceration
– (2001 data used).
As of 2001 there were 280 DOs in Canada.
– Fewer than 10% have been released under parole
supervision.
184
LTSO Legislation-Impact on the Community
To provide an alternative to indeterminate
incarceration for some sex offenders who, in
the opinion of the court, while exhibiting a
substantial risk, could be effectively
managed in the community after a period of
incarceration lasting two years or more
The court may impose a maximum of 10
years of supervision.
185
LTSO Legislation-Impact on the Community
The LTSO provisions came into force on
August 1, 1997.
To date, the 10-year term of supervision is
most common.
An LTSO does not begin until the offender
has completed serving the sentence
imposed by the court and any other
custodial sentence that may have been
imposed.
186
LTSO Legislation-Impact on the Community
LTSOs do not begin until after the Warrant
Expiry Date (WED) even if the offender is in
the community prior to the WED.
Some, due to “dead time” end up serving
sentences of days/weeks.
As a result some of these offenders are
released without any treatment having been
offered/received in provincial institutions.
187
LTSO Legislation-Impact on the Community
Many of these offenders impress as very
high needs/high risk.
It is very difficult to suspend these offenders
for any significant period of time unless
there are new charges laid.
It is difficult/impossible to offer a high
intensity sex offender treatment program in
the community.
188
LTSO Legislation-Impact on the Community
These offenders present with many
treatment needs.
In the community they tend to be housed at
our CCC or supervised through the Team
Supervision Unit (TSU).
Coordination with police
Frequent team discussions regarding these
cases.
189
LTSO Offenders
In Ontario as of 2011 there were 178 men
with LTSO
– 81 were in the community.
– 18 additional were suspended
Most of these are released to one of the
CCCs.
190
Community Treatment Outcome
Followed 25 sex offenders released to Keele
CCC in 2007
11/25 LTSO
19 were involved in treatment
Of those involved in treatment, none were
suspended over an average 3.1 year followup.
Of the 6 who did not participate in
community treatment, 3 were suspended
191
Community Treatment Outcome
None of these men were convicted of a new
sexual offence in the follow-up period
Two were convicted for violent non-sexual
offences
One of these received community treatment
192
LTSO Offenders
These data, which are only preliminary,
suggest that even very high risk offenders
can be managed effectively in the
community using a team based approach.
Inpatient housing, at least at first, is typically
recommended unless the individual has a
prosocial and well developed support
network available.
193