A Perspective on Developmental Trauma
advertisement

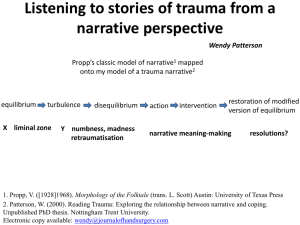
The Complexities of Developmental Trauma: A Clinician’s View Larry M. Rosenberg, Ph.D. Our Agenda My clinical experience with Developmental Trauma Some preliminary research on the subject ADD, ODD, CDD, and Adjudicated Teens The early interpersonal nature of Developmental Trauma: A synthesis of theory Discussion of Developmental Trauma as a diagnostic category? Benefits Problems Implications for treatment My Clinical Experience Rape victims The kids that I was seeing The problem with diagnosis based on observable behaviors alone What do you see when you include intrapsychic factors into the diagnostic discussion? Pilot studies Findings 1987 1987: A subgroup of these children emerges…”These are…children who have been chronically traumatized; children from backgrounds that are chaotic, destructive, overwhelming and may involve exposure to violence, abuse and/or neglect; children whose development reveals little protection from intrusive and disruptive impingement on a state of going on being…that is the basis of the development of ego strength…and the unfolding of a sense of self and other. 2 More Pilot Studies Children with ODD Children who have experienced abuse and neglect 2 distinct subgroups of kids with ODD 1 higher functioning group of oppositional children looking liked you would expect ‘spoiled’, ‘neurotic’ children having difficulty with authority figures 1 much more impulsive, angry, primitive in the functioning and appearing to have an Axis II, rather than an Axis I appearance Over and Under Stimulation Comparing Borderline Traits with Developmental Trauma BPD From a neurobiological perspective Key dimensions of BPD Affect modulation/self regulation Impaired interpersonal relationships Identity diffusion Impulsivity Self injurious behaviors and suicidality Developmental Trauma From Criteria Proposed for DSM V Affective and Physiological Dysregulation Attentional and Behavioral Dysregulation including habitual or reactive self harm Self and Relational Dysregulation What About the Comparison? Developmental Trauma is not the equivalent of Borderline Personality Disorder, ADHD, or ODD But there is considerable overlap between the diagnostic categories and To the degree that there is overlap is not just in the area of behavior, but in the root causes and the resulting neuro-biological and intrapsychic affects At the Outset: Mirroring What is the mirroring function of the “mother” figure? A paradigm for the way manner in which the child comes to understand who he/she is The only way for the infant child has to see himself at the outset is through his mother’s eyes “In human development the precursor of the mirror is the mother’s face” Consequences of the Mother’s Gaze If she is unattuned to the child and blank by way of her own depression or emptiness: The child may come to feel that he himself is empty or that the world is devoid of supplies If she projects her own self onto him He winds up seeing her face and not his own He is left unable to differentiate himself from the other He comes to believe that he has to be her in order to engage her What are we Saying About the Mirroring Function Critical to the development of the sense of self Critical to the ability to differentiate oneself from another A forerunner of empathy and mindfulness Involved in the formation of identity Critical beginning to the experience of how one views others Protecting the Young Child The primary caregiver initially has to protect the child from becoming overly distressed The notion of a stimulus barrier Stress can come from within or outside of the infant The infant has no ability to protect herself, except by way of withdrawal Clearly relates to the issue of attachment, establishment of basic trust, and the capacity to postpone gratification Empathic Attunement This refers to the ability of the mothering figure to understand, empathize with, and respond in keeping with the affective state of the child Being in rhythm or in tune with the child Stern, Beebe, Brazelton, Kestenberg Feeding Rhythm What Results from Empathic Attunement? Helps the child to regulate themselves Helps restore a child’s emotional equilibrium once the child has become dysregulated Kestenberg’s work with rhythm and choreographic notation Beebe and Stern What Results When the Mothering Figure is not Attuned to the Child? The mother does recognize the impact that the environment is having on the child’s affective state The child becomes over-stimulated; unable to emotionally contend with the level of stimulation that the environment is presenting him with The child becomes disorganized internally; unable to organize his experience of the world Overwhelmed by his own affect; a definition of traumatic experience Mother (cont) If the mother’s own range of emotions is limited and she reacts only in this limited way, the child’s own affective range will be similarly limited 0-60 and back again Blunted constricted affect A Brief Summary Said another way, if the environment surrounding the child fails to provide a protective function in the form of empathic attunement the result is either inadequate or excessive stimulation of the child It is this under or over-stimulation of the baby that leads to difficulties in the areas of development of self, self differentiation, and in the child’s capacity to self regulate We now potentially have a child who either doesn’t know who he is, and/or can’t manage to keep himself emotionally stable The Protective Function of the Child’s Environment (cont) Note that all that we have just described as emanating from a chronically deficient care giving environment mimics what we see being proposed as DTD and possesses similarities to BPD, ADHD and other existing diagnostic categories Aside from genetic and biological factors, the failure to adequately protect the child from the environment is the stuff that psychopathology is made of Synthesizing Theories that Underlie the Concept of Developmental Trauma What happens when a child experiences events reflective of poor attachment, lack of empathic attunement, failures to protect the child from the environment, failures to experience oneself as enjoyed by the parenting figures, and excessively stimulated by the environment on a consistent or chronic basis? We have strung together theories ranging from Freud, to object relations theory, self psychology, to attachment theory, to trauma An analog: Casson and Siegel DTD too produces actual affects on brain development, cortical mass, neuropeptides and the corpus collosum Developmental Trauma Symptom presentation is more complex than in PTSD Diffuse and tenacious It leads to personality changes including problems with relatedness and identity (Axis II) It leads to further harm; either self or other inflicted It involves the loss of the capacity to self soothe and to tolerate or regulate affect Developmental Trauma (cont) In CT 60-80% of out-pt kids screened positive for trauma as do 80% of kids in juvenile justice system They may be entirely overlapping populations Likely the same patient population I saw 25 years ago Though involvement in anti-social activities is only one of the bi-products of this kind of cumulative trauma. Substance abuse, academic performance, relational problems, health problems, etc. Trauma in Its Extreme Form Overwhelming affect leading to immobilization, withdrawal, somaticization, dissociation, and psychological disorganization At its worst we see breaks with reality, disturbances in ones ability to experience emotion, or regulate affect, a loss of ones sense of self, and cognitive impairment It is not an all or none phenomenon, but occurs on a spectrum of severity What Trauma is not Trauma should not be defined or determined by an aversive event Trauma should be defined by the nature of ones reaction to an aversive event Mitigating Factors What we don’t know is the portion of the variance in trauma that relates to where the aversive event took place, who was responsible for the exposure, or how it was responded to by caregivers All of the above may relate to influence whether a trauma occurs and the severity with which it does occur Will DTD Become a Diagnosis? Why yes? More accurately diagnosis kids and provide more appropriately focused treatment Co-morbid possibilities at present include CD, BPD, Major affective disorder, ADHD, phobias, dissociative disorders, OCD, panic disorders’ PTSD is inadequate and fails to capture the essence of the problem, omitting the attachment, relational, and early and pervasive level of impairment Children may be more appropriately medicated or not medicated as often DTD Diagnosis? Why not? It is not viewed as having sufficient specificity as to causality The definitions of maltreatment are too broad, as are the definitions of trauma itself Some researchers remain unconvinced by the evidence Some say that “the science around it is not serious” There might be consequences to the pharmacological industry and the insurance industry It may shift too much focus to parenting to be politically unviable Many of those who will be voting are not people who work with children, or people who are clinicians Treatment Implications TF CBT, DBT or psychodynamic treatment or group seem indicated Any treatment for DTD should have an interpersonal component Where areas to address would be basic trust, building a clear sense of self, and affect regulation through the use of empathic attunement, consistency, and support The ability of the clinician to tolerate the affect of the child in association with the mistreatment they have suffered Significant caring for the parent figure who must likewise be able to do all of the above for the child Implications (cont) The need for longer term treatment The benefits of having families deal with one clinician from start to finish The benefit of spending time, at the outset of treatment, in establishing helpful alliances with primary caregivers This, rather than an emphasis on data collection or quick diagnosis An alteration in the way we view the caregivers of our patients The ability to see them as we would any patient so that empathy becomes more easily attainable and so that the focus is not solely on the experience of the child