Introduction to Trauma-Focused
Cognitive-Behavioral Therapy for
Children and Adolescents
By
Adam H. Benton, PhD
TF-CBT
•
•
•
•
•
Traumatic Stress in Children
Assessment of Trauma Symptoms
Development and Research On TF-CBT
Treatment Using TF-CBT Components
The AR BEST Program
What is Child Traumatic Stress (CTS) ?
• Child Maltreatment
• Medical Trauma
• Domestic Violence
• Traumatic Loss
• Natural Disasters
• Terrorism
• Community and School
Violence
• War-Zone Trauma
How Big is the Problem?
The Epidemiology of Child Traumatic Stress
General population
studies
Disaster studies
• Terrorism
• Natural disasters
Child maltreatment
studies
General Population Studies of Child
Traumatic Stress
National Survey of Adolescents (Kilpatrick & Saunders, 1997)
•
Representative US sample: 12-17 yrs
•
Serious physical assault: 5 million
•
Sexual assault: 1.8 million
Youths in Urban America study (Breslau et al., 2004)
•
Mid-Atlantic US city
– Baseline 6 yrs; follow-up 20-22 yrs
•
82.5% one or more lifetime traumatic events: 87.2% males, 78.4% females
•
Exposure to violent assault
– Increase after 15 years, peaked @ 16-17 yrs
– Major decrease by age 21
General Population Studies of Child
Traumatic Stress
Developmental Victimization Study (Finklehor et al., 2005)
• Representative US sample: 2-17 yrs
• 1 in 8 experienced a form of child maltreatment
• 1 in 3 witnessed violence
The Great Smoky Mountains Study (Copeland, et al., 2007)
• A majority of children (67.8%) were exposed to one or
more traumatic events by age 16.
• Children exposed to trauma had almost double the
rates of psychiatric disorders of those not exposed.
Disaster Studies
New York City, NY Department of Education Study (Hoven et al., 2005)
• At 6 months post World Trade Center attack, the prevalence of:
–
–
–
–
–
•
PTSD was 10.6%
agoraphobia was 14.8%
conduct disorder was 12.8%
separation anxiety was 12.3%
alcohol problems was 4.5%
Over 60% experienced at least one major traumatic event prior to the attacks.
Gulf Coast Child & Family Health Study (Abramson et al., 2007)
• At 2 years after Hurricane Katrina.
–
–
46,000 children were displaced
51% of displaced children had at least 1 risk factor for poor long term outcomes
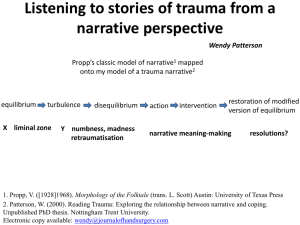
National Estimated Child Maltreatment Reports
3.5
3
Million
2.5
2
1.5
1
0.5
0
1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Year
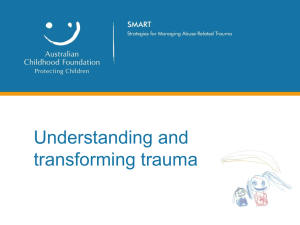
Victimization Rates by Age Group, 2000
age 16-17
5.8
age 12-15
10.4
age 8-11
11.8
age 4-7
13.3
age 0-3
15.7
0
5
10
15
Rate per 1,000 children of same age group
20
Child Maltreatment Prevalence
2007
Nationally
Arkansas
6 million Child maltreatment
investigations
58,000 child maltreatment investigations
794,517 confirmed cases of abuse /
neglect (1 out of every 94 children)
9,847 confirmed cases of abuse / neglect
(1 out of every 71 children)
• 59% Neglect (436,944 children)
• 55% Neglect (5,439 children)
• 8% Sexual Abuse (56,460 children)
• 20% Sexual Abuse (1,961 children)
• 11% Physical Abuse (79,886 children)
• 12% Physical Abuse (1,135 children)
• 13% Multiple types (97,123 children)
• 7% Multiple types (711 children)
• 4% Psychological Abuse (31,366
• 1% Psychological Abuse (31,366
children)
children)
Comparisons
1 out of every 71 children in Arkansas were victims of abuse or
neglect
• 1 out of every 6250 children were diagnosed with cancer (U.S. Department of
Health and Human Services, 2009)
•
1 out of every 4032 individuals under 24 had a confirmed case of H1N1
(Centers for Disease Control and Prevention, 2009)
•
•
•
1 out of every 30,303 individuals under 24 had a confirmed case on H1N1
that required hospitalization (Centers for Disease Control and Prevention, 2009)
1 out of every 1,514,175 individuals under 24 died from a confirmed case
on H1N1 (Centers for Disease Control and Prevention, 2009)
1 out of every 150 eight-year-old children were diagnosed with an
Autism Spectrum Disorder (Centers for Disease Control and Prevention, 2002)
Posttraumatic Stress Disorder
A.
Exposure
– Experienced or witnessed…actual
or threatened injury or death
– Responded with intense fear,
helplessness, or horror
B. Reexperiencing
• Intrusive recollections
• Recurrent dreams
• Acting or feeling as if the event
were recurring
• Intense distress triggered by
internal or external cues
• Physiological reactivity
C. Persistent Avoidance (3+)
– Avoiding thoughts, feelings
etc
– Places, activities, or people
– Inability to recall events
– Diminished interests in
significant activities
– Detachment or
estrangement from others
– Restricted affect
– Foreshortened future
Posttraumatic Stress Disorder
D. Persistent Increased
Arousal (2+)
• Difficulty sleeping
• Irritability
• Difficulty concentrating
• Hypervigilance
• Exaggerated startle
response
E. Duration of 1 month or
more
F. Clinical impairment
What is the impact of Child Traumatic
Stress?
•
•
•
•
•
•
•
•
•
Capacity to regulate emotion and attention
Social development
Cognitive development: IQ and language
Academic performance
Substance use/abuse
Numbness, desensitization to threat
Re-victimization
Recklessness and reenacting behavior
Posttraumatic stress and other disorders
(depression, anxiety, phobia, panic)
• Developmental Trauma Disorder
• Health effects
Traumatic Stress in Children
• Physical consequences can include impaired brain
development and/or poor physical health
•
(Kaufman & Charney, 2001; Perry, 2002; Shore, 1997; Springer, Sheridan, Kuo, & Carnes, 2007)
• Psychological consequences can include
internalizing disorders, externalizing disorders,
cognitive difficulties, and/or social difficulties
•
(Kaufman & Charney, 2001; Morrison, Frank, Holland, & Kates, 1999; Silverman, Reinherz, & Giaconia, 1996; Springer, Sheridan, Kuo, & Carnes, 2007; Teicher, 2000; U.S.
Department of Health and Human Services, 2003; Watts-English, Fortson, Gibler, Hooper, & DeBellis, 2006)
• Behavioral consequences can include juvenile
delinquency, adult criminality, substance abuse,
and/or abusive behavior
•
(National Institute on Drug Abuse, 1998; Prevent Child Abuse America, 2001; Widom & Maxfield, 200; Widom, White, Czaja, & Marmorstein, 2007)
Traumatic Stress Symptoms in Children
Compared to adults…
• Less numbing and difficulty recognizing
avoidance
• More overt aggression, destructiveness,
and reenactment (also in play and
drawings)
• Older children – foreshortened future
• Over the age of 10 – react more like adults
Dyregrov & Yule, 2005
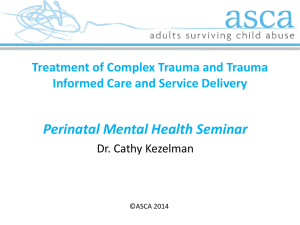
Effect of increasing trauma exposures on cumulative rates of
psychiatric diagnoses by age 16 years (Copeland et al., 2007)
70
60
Percent
50
40
30
20
10
0
None
(32.2% )
1
(30.8% )
2
(22.4% )
3
(7.1% )
4 or more
(7.5% )
Number of Events
Any Diagnosis
Any Anxiety Dx
Any Depression Dx
Any Behavioral Dx
Incidence of PTSD in Children
• 6% life-time prevalence in older
adolescents
• Exposure to war
• Natural Disasters
• Diseases or hospitalization
– 30-50% moderate symptoms
– 5-10% full criteria
•
•
• Traffic Accidents
–
–
–
–
29% at 4 wks
36% at 6 wks
6 – 25% at 12-15 wks
14% at 9 months
• X < 15%
Sexual and Physical Abuse
•
•
25 – 70%
11 – 20%
Symptoms often remain for years
without treatment (15-29% still
meet criteria 5- 33 years later)
Dyregrov & Yule, 2005
Predictors of PTSD Reactions in
Children
•
•
•
•
Level of Exposure
Lack of social support
Female gender
Previous trauma
exposure
• Prior psychiatric
problems
• Strong acute response
• Family history of
mental illness
• Cognitive variables
–
–
–
–
–
Negative appraisal
Unfairness
Rumination
Thought suppression
Confusion during the
event
Assessment of Trauma Symptoms
• “The development of the abused or neglected
child seldom follows a predictable course, because
child maltreatment is characterized by many other
negative socialization forces,
such as family instability,
parental inconsistency, and
socioeconomic disadvantage.”
Wolf & McEachran, In Mash & Terdal, 1997)
Assessment Process
• Assess existing risk and safety
• Identify general strengths and problems areas
for family (marital problems, Family Stressors,
etc.)
• Identify parental needs (support, child rearing,
etc)
• Identify child needs (behavior, cognitive,
social, mental health symptoms, etc)
• Reporting issues
Assessment Process
• Cognitive problems: Maladaptive patterns of thinking about
self, others and situations, including distortions and unhelpful
thoughts, like self-blame or rumination about the trauma
• Relationship problems: Difficulties getting along with peers,
poor problem-solving or social skills, hypersensitivity in
interpersonal interactions, maladaptive strategies for making
friends, impaired ability to trust.
• Affective problems: Sadness, anxiety, fear, anger, poor ability
to tolerate or regulate negative affective states, inability to
self-soothe.
Assessment Process
• Family problems: Parenting skills deficits, poor parent-child
communication, disturbances in parent-child attachment,
disruption in family relationships or functioning due to abuse.
• Traumatic behavior problems: Avoidance of trauma
reminders; trauma-related, sexualized, aggressive, or
oppositional behaviors; unsafe behaviors
• Somatic problems: Sleep difficulties, physiological
hyperarousal and hypervigilance toward possible trauma
cues, physical tension, somatic symptoms.
Cohen, Mannarino, & Deblinger, 2006
Assessment Instruments
• Family Adjustment
– Family Adaptability , Cohesion and
Expression Scale
– Family Environment Scale
• Cognitive / Learning Ability
– WISC, WPPSI, Stanford Binet, KBIT,
WASI
– WIAT, Woodcock-Johnson, WRAT,
• Social Functioning
– Harter Self-Perception Profile for
Children
– Harter Social Support Scale for Children
– Adolescent Interpersonal Competency
Questionnaire
– Children’s Attributional Style
Questionnaire
• Emotional /Behavioral
–
–
–
–
–
–
Child Behavior Checklist
Behavior Assessment Scale for Children
Roberts Apperception Test – 2
Child Depression Inventory
Manifest Anxiety Scale for Children
Strengths & Difficulties Questionnaire
• Traumatic Stress Symptoms
–
–
–
–
UCLA Posttraumatic Stress Index
Trauma Symptom Checklist for Children
Child PTSD Screen
Child Report of Posttraumatic
Symptoms
– Children’s Impact of Traumatic Events
Scale
– Child Dissociative Checklist
– Traumatic Events Screening Inventory
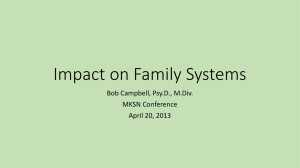
Tracking Outcomes
Strengths & Difficulties Questionnaire – Symptom Subscale Severity
10
Emotional Distress
(clinical cut =3)
10
9
8
8
6
6
9
Behavioral Difficulties
(clinical cut =2)
5
4
4
4
3
2
2
4
3
2
2
2
0
Baseline
3 Months
6 Months
9 Months
Attentional
Difficulties (clinical
cut =5)
*Getting along with
Children
(clinical cut =2)
*Kind / helpful
Behavior (clinical cut
=6)
Tracking Outcomes
UCLA PTSD Index Subscale Severity
30
25
Intrusion
20
Avoidance
15
Arousal
10
5
0
Baseline
3 Month Follow-up
6 Month Follow-up
9 Month Follow-up
Development of TF-CBT
Judith A. Cohen, M.D.
Anthony P. Mannarino, Ph.D.
Allegheny General Hospital, Pittsburgh, PA
Center for Traumatic Stress in Children and Adolescents
Esther Deblinger Ph.D.
New Jersey Child Abuse Research Education and Services
Institute
Research On TF-CBT
• TF-CBT is the most rigorously tested treatment for
traumatized children
– 6 randomized trials
• Improved PTSD, depression, anxiety, shame and
behavior problems compared to supportive treatments
• Improved parental distress, parental support, and
parental depression compared to supportive treatment
• Successful with diverse ethnic and racial populations
Reviews of Research
• “Well supported” by the CEBC (2009)
• “Best practice” by the Kauffman Best
Practices Project (2004)
• “Well-supported and efficacious” by Saunders,
Berliner, & Hanson (2004)
• “Well-established” by Silverman et al. (2008)
Statewide Dissemination
• 18 states including Arkansas
Evidence Based Treatments
• What it is not…
What is TF-CBT?
A hybrid treatment model that integrates:
• Trauma sensitive interventions
• Cognitive-behavioral principles
• Attachment theory
• Developmental neurobiology
• Family therapy
• Empowerment therapy
• Humanistic therapy
Core Values
• CRAFTS
– Components-based
– Respectful to Cultural
Values
– Adaptable and Flexible
– Family Focused
– Therapeutic Relationship
is Central
– Self-efficacy is
Emphasized
TF-CBT Treatment Structure
• Average 12 – 18 sessions
• 1 to 1 ½ hour weekly sessions
• Each session is divided into individual child and
parent sessions
• The length of the child and parent portions may vary
by topic
• Similar topics in most parent and child sessions
• Same therapist for both child and parent(s)
• Combined parent-child time in some to many
sessions
Treatment Using TF-CBT Components
•
•
•
•
•
•
•
•
Psychoeducation and Parenting Skills
Relaxation
Affect Modulation
Cognitive Coping
Trauma Narrative and Processing
In Vivo Mastery of Trauma Reminders
Conjoint Child-Parent Sessions
Enhancing Future Safety and Development
TF-CBT Components
CHILD’S TREATMENT
Education
Skill Building
Exposure/Processing
PARENT’S TREATMENT
Education
Skill Building
Exposure/Processing
Behavior Management
JOINT
FAMILY SESSIONS
1996 Deblinger & Heflin
Psychoeducation
• Begins during first session and continues
throughout treatment
• Provide information about the specific
trauma, common psychosocial reactions to
trauma, etc.
• Review benefits of early, effective tx
• Explain treatment plan and theoretical
rationale for skills, exposure and processing
Education and Hope
Parenting Skills
• TF-CBT views parents as central therapeutic agent for
change
• Establish parent as the person the child turns to for
help in times of trouble
• Explain the rationale for parent inclusion in treatment
– Not because parent is part of the problem but because
parent can be the child’s strongest source of healing
• Emphasize positive parenting skills, enhance enjoyable
child-parent interactions, maximize perception/reality
effective parenting
Parenting Skills (Praise)
• Focus on actively praising the child
– Praise a specific behavior
– Provide praise ASAP after behavior occurs
– Be consistent
– Do not qualify your praise
– Provide praise with same level of intensity as
criticism
• “Catch your child being good!”
Parenting Skills (Selective Attention)
• No reaction to certain negative behaviors
– Defiant or angry verbalizations to parent
– Nasty faces, rolling eyes, smirking
– Mocking, mimicking
• Walk away, busy oneself with an activity
• Remain calm, dispassionate
• Expect a reactions of more provocative
behavior
• Praise “the opposite”- wanted behavior
Parenting Skills (Time Out)
• Purpose: Interrupt child’s negative behaviors
and allow him/her to regain control
• Explain to child
• Location: quiet, least stimulating
• Once in time out, parent should refrain from
comments, and maintain calm demeanor.
• Be consistent!
Parenting Skills (Contingency
Reinforcement Program)
• Purpose: Decrease unwanted behaviors and
increase desired behaviors
• Select only one behavior to target
• Explain process to child
• Involve child in decisions about rewards
• Add stars and give rewards weekly, and
consistently
Parenting Skills (Behavior
Management)
• Reasonable developmental expectations
• Limit-setting
• Numerous other techniques (logical and
natural consequences, etc.)
• Behavioral interventions for:
– Anxieties
– Sleep problems
– Aggressive behaviors
– Sexually inappropriate behaviors
Relaxation/Affective Modulation
Feeling Identification
• Accurately identify and express a range of different feelings
– Board games
– Feeling brainstorm
– Color My Life or person
• Physiological responses to different feelings (spaghetti,
robot/ragdoll, etc.)
• Can ask directly about feelings experienced during traumatic
event.
• End on a positive note
Relaxation/Affective Modulation
•
•
•
•
•
•
•
•
Reduce physiologic manifestations of stress and PTSD
Explain body responses to stress
Shallow breath, muscle tension, headaches
Focused breathing/mindfulness/meditation
– Bubble breaths, diaphramatic breathing
Progressive Muscle Relaxation
Physical Activity
Positive Visual Imagery
Anything that helps relax (e.g., art, reading, etc.)
Relaxation/Affective Modulation
Thought Interruption and Positive Imagery
• Use when overwhelmed with trauma reminders
• Temporary measure early in treatment
• Teaches child control over their thoughts
• “Changing the channel”
• Saying “go away” or “snap out of it”
• Imagining a stop sign
• Replace unwanted thought with a positive one
Relaxation/Affective Modulation
Positive Self-talk
• Focus on child’s strengths
• Remind child to verbalize these
Enhancing Sense of Safety
• Ask about child’s sense of safety right now
• Develop a safety plan
Relaxation/Affective Modulation
Problem Solving / Impulse Control
• STOP Technique
• Turtle Technique
Cognitive Coping
• Help children and parents understand the cognitive triad:
connections between thoughts, feelings and behaviors, as
they relate to everyday events
• Help children distinguish between thoughts, feelings, and
behaviors
• Help children and parents view events in more accurate and
helpful ways
• Encourage parents to assist children in cognitive processing of
upsetting situations, and to use this in their own everyday
lives for affective modulation
Cognitive Coping
Cognitive Coping
Types of Inaccurate Thoughts
• Personal, Pervasive, Permanent
– All or Nothing Alan
– Again and Again Agnes
– Catastrophic Cassie
– Negative Ned
Trauma Narrative and Processing
• Reasons we avoid this with children:
– Child discomfort
– Parent discomfort
– Therapist discomfort
– Legal issues
Trauma Narrative and Processing
• Reasons to directly discuss traumatic events:
– Gain mastery over trauma reminders
– Resolve avoidance symptoms
– Correction of distorted cognitions
– Model adaptive coping
– Identify and prepare for trauma/loss reminders
– Contextualize traumatic experiences into life
– Gradual Exposure
Trauma Narrative and Processing
• Introduce the child to the rationale for the narrative
• Can introduce the idea by reading a book about a
child who told their trauma story and felt better
• Use analogies:
– Cleaning a wound
– Rollercoaster
• Help the child to identify how they would like to tell
their trauma story (e.g., book, poem, story, song,
drawing, painting, video, audiotape, typing on
computer, cartoon, talk show)
Trauma Narrative and Processing
• Chapter 1: Innocuous information about the
child (name, age, school, hobbies, etc)
• Chapter 2: “Before” (for example, what the
relationship was like with the person before
the trauma started or what life was like before
the traumatic event occurred)
Trauma Narrative and Processing
• Chapter 3: Encourage the child to “tell what
happened” during the trauma itself
– If multiple episodes, let the child choose one
(example: first, last, one most remembered)
– Typically, children proceed from first to last
episode
– Include disclosure, legal procedures, medical
exams, removal from home, etc.
– For the first telling, allow the child to tell the story
with minimal interruption and little questioning.
Trauma Narrative and Processing
My uncle came into my room to kiss me
goodnight. He pulled down the covers and
touched me down there. I felt scared. I
pretended I was asleep. When he was done,
he left. The next morning I got up and my
uncle said, “Good morning, how are you?”
and I said, “Fine”. I went to school.
Trauma Narrative and Processing
• Identify “hot spots” or “worst moments”
• Rate distress (SUDS scale) before, during, and
after narrative
• Review the child’s description at subsequent
sessions
• Help the child to describe more details
• Encourage child to describe thoughts and
feelings related to trauma
Trauma Narrative and Processing
• Ask broad, open-ended questions
–
–
–
–
What were you thinking?
What were you saying to yourself?
How were you feeling?
What happened next?
• Make clarifying and reflective statements
–
–
–
–
–
Tell me more about it…
I wasn’t there, so tell me…
I want to know all about…
Repeat the part about…
So, your uncle began touching your vagina…
Trauma Narrative and Processing
My uncle came into my room to kiss me goodnight. I
felt good. He pulled down the covers and touched
me down there, on my vagina. I felt scared and dirty,
and thought why is he doing this, he’s my favorite
uncle. I pretended I was asleep. When he was done
touching my vagina, he left. The next morning I got
up and my uncle said, “Good morning, how are
you?” and I said, “Fine”. Inside I felt scared and I
didn’t know what to say or do. I went to school.
Trauma Narrative and Processing
• Common negative distortions
– Self-blame
– Overestimating danger
– Changed world view
Trauma Narrative and Processing
• Sexuality
– “Am I gay?” “I was abused because I dress sexy.”
• Body Concerns
– “I might die of AIDS.” “I might be pregnant.”
• Interpersonal Concerns
– Family
• “I tore apart my family.”
– Friends
• “My friends think I’m a slut.”
• Safety Concerns
– “I will never trust another man.” “I can’t go anywhere alone.”
• Self Image
– “I am so stupid.” “I am unlovable.”
Trauma Narrative and Processing
•
•
•
•
Examine contradictory evidence/facts
Test the accuracy of thoughts
Use the Socratic method
Use role plays (e.g. best friend)
Let’s Practice
Dear Dad,
I am writing because I have some things to tell you.
I’m glad you are in jail now. Now you can’t hurt me
or other kids anymore. Everyone knows what you did
to me. Some people think it was wrong, and some
people think it was OK. I think you ruined my life. I
keep asking why did I do that? I should have told you
to stop. I’m really mad that I told 2 years too late.
From,
The daughter you hate
Trauma Narrative and Processing
• Include the following in the final chapter:
– What have you learned?
– What would you tell other children who
experienced this?
– How are you different now from when it
happened/when you started treatment?
Trauma Narrative and Processing
• How caregivers talk to and behave towards
children can greatly influence developing
beliefs about self, others and the world.
• How might parents’ feelings and thoughts
about the trauma impact on their children’s
behaviors and developing beliefs?
• Provide parents with a forum to share their
feelings and thoughts related to the trauma
(even the socially undesirable ones)
Trauma Narrative and Processing
• Examine thoughts which are permanent, pervasive, or too
personalized
– Permanent: “ My child will never be happy again.”
– Pervasive: “No one can be trusted with my child.” “The world is not a
safe place.”
– Personalized: “This happened because I am a terrible parent.” “I
should have known that man was a sex offender.”
• "If my best friend had a child who experienced a similar
traumatic experience, would I say to him or her what I am
saying to myself?“
• "Would I want my child to overhear me making this statement
out loud?"
In Vivo Desensitization
• Resolve generalized avoidant behaviors
– Gradually help the child get used to the
feared situation
• Identify the feared situation
• Design the in vivo desensitization plan
• Praise and reinforce in vivo work
• Therapist MUST have confidence that this will
work or it won’t
Conjoint Sessions
Format of sessions
• Meet individually with parent and child prior
to joint part of session
• Meet together after child and parent prepared
for session
Conjoint Sessions
Content of sessions
• Therapist models appropriate support of child
• Praise for progress made
• Caregiver models skillful coping
• Facilitates open communication
–
–
–
–
–
–
–
–
–
–
Trauma knowledge and education
Sharing the trauma narrative
Sex education
Personal Safety
Relaxation
Affective modulation
Psychoeducation
Cognitive Coping
In-vivo desensitization
Prepare for future reminders
Conjoint Sessions
When NOT to have joint sessions:
• Parent unable to provide appropriate support
• Child adamantly opposed (evaluate how realistic
objections are)
• Parent(s) continue to be disbelieving or unsupportive
• Parent(s) feel emotionally incapable of hearing
narrative
• Child is refusing to participate in joint parent child
sessions
Enhancing Safety and Future
Development
Sex Education
• Dependent on the age of the child
• Start young and continue through adolescence
• Model open communication beginning use of
accurate terms for private parts
• Broad or specific
– Puberty
– Sex vs. sexual abuse
– Relationship issues
• Talk with caregiver first
• Identify resources
Enhancing Safety and Future
Development
Enhancing Safety and Future
Development
Increasing Awareness
• Develop a safety plan which is responsive to the
child’s and family’s circumstances and the child’s
realistic abilities (No-Go-Tell, private part or sexual
behavior rules, etc.)
• Improve problem solving skills in stressful situations
• Increase awareness (Boundaries, Hula Space,
Personal Bubble, etc.)
• Counteract shame by enhancing confident body
language
• Increase assertive communication skills (mouse/lion)
Sexual Behavior Rules
• It is not ok to show your private parts to other
people.
• It is not ok to look at other people’s private parts.
• It is not ok to touch other people’s private parts.
• It is ok to touch your private parts as long as its in
private and does not take too much time.
• It is not ok to use sexual language or make other
people uncomfortable with your sexual behavior.
Terminating Therapy
•
•
•
•
Review skills and progress achieved
Fade out and/or plan booster sessions
Discuss and plan for natural setbacks
Encourage clients’ confidence in managing
setbacks
• Emphasize parents’ role as a continued
therapeutic resource for the child
• Celebrate clients’ therapy graduation
Applying TF-CBT in Real Life
• Match length and intensity to child
presentation
• Focus on what is most distressing for child
• Incorporate into interventions for other
concerns/problems
• Be flexible
Strategy for Less Affected Children
•
•
•
•
Psychoeducation
Identification of potential areas of problems
Review of coping strategies
Revictimization prevention
Children with History of Multiple
Traumas
• Integrate trauma treatment into broader
intervention
• Be prepared to offer longer term relationship
based therapy
• Provide assistance with managing every day
life
Family Complications
• Do not agree that child was victimized/ harmed
• Overwhelmed with own reactions to child
victimization
• Compromised relationship with child
• Inadequate parenting skills/child behavior out of
control
• Depressed, substance abusers, anti-social
• Unstable, in financial straights, homeless, facing legal
problems
Trauma-Focused Cognitive-Behavioral
Therapy Web Site
Arkansas BEST for Children
The mission of AR BEST is
to improve outcomes for
traumatized children and
their families in Arkansas
through excellence in clinical
care, training, advocacy and
research/evaluation.
Arkansas BEST for Children
Clinical Care & Training – Provide state-of-the-art training,
supervision and learning environments that will maximize the
adoption of evidence-based interventions for traumatized
children and adolescents.
•
•
•
•
•
•
•
•
•
Website
List serve
Free on-line assessments and feedback reports (CBCL, UCLA)
2 Day Conference April 15 & 16 with one of the developers of TF-CBT
Post-conference Consultation 6 – months
Yearly conference
On-line trainings
Tele-video Conferences
Certification of completion of TF-CBT training
Website
Trauma-Focused Cognitive-Behavioral Therapy
Dissemination Process
PRE-IMPLEMENTATION PHASE
Clinician registers for free on-line tutorial of
TF-CBT through tfcbt.musc.edu
Clinician registers for TF-CBT certification
process through AR BEST website (TBN)
Clinician completes on-line tutorial of TFCBT; receives 10 continuing education credits
Clinician sends certificate of TF-CBT
completion to UAMS; registers for face-to-face
training at UAMS April 1-2
IMPLEMENTATION PHASE
Face-to-face training held at UAMS April 1-2
Phone consultation with Learning
Collaborative twice monthly for six months
List Serve
Website Access
Technical Assistance
Identification of State Champions
Enrollment of clients in TF-CBT
(minimum of two per clinician for
certification)
Completion of standardized assessments
Completion of treatment record
EVALUATION
SUSTAINABILITY
Clinician certification
Website posting of clinician’s
completion of training
Clinician eligible for consultant
training
Contact Info
Benjamin A. Sigel, MS, LPE
BASigel@uams.edu
Adam H. Benton, PhD, LPP
AHBenton@uams.edu
Psychiatric Research Institute
University of Arkansas for Medical Sciences
4301 W. Markham
Little Rock, AR 72205
Phone (501) 526-8200
Fax (501) 526-5296
Effective Psychotherapy