OA-Assessment-of-the-Older-Person
advertisement

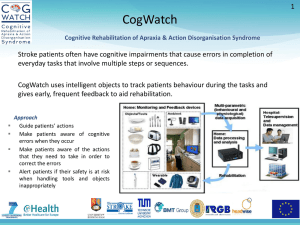
Expert Led Session: ‘The Assessment of the Older Person’ Dr Gareth Thomas Dr Mark Worthington Consultant Psychiatrists for Older People Lancashire Care NHS Foundation Trust MRCPsych Examinations • Features in both Paper A and B • Old Age CASC Scenarios from this presentation – – – – History taking from patient and informant Cognitive Assessment Physical Examination ECG interpretation Aims and Objectives • Aim – Gain an overview of the assessment of an older person • Objectives – Understand the principles of assessing the older person which includes history taking, mental state examination, risk assessment and a holistic formulation – Understand the basics of a cognitive assessment – Understand the importance of assessing for delirium in the older person Overall Process • History • Mental State Examination • Focused Physical Examination • Investigations • Formulation • Risk Assessment • Multidisciplinary Management Plan History Taking Referral Information • Who made the referral? • Is the patient already known to MH Services or is this a new referral? • What has been their journey to this point? • Has the patient come from home or are they in a care setting? (what type?) • Detained under MHA (1983) or DOLS? Presenting Complaint • Why the patient has presented • What What is the patients perception of their difficulties? • Most distressing symptom(s) History of Presenting Complaint • • • • Onset and evolution of symptoms Is this a new problem? When did they last feel like their old self? Has there been any recent trigger events – – – – Changes in the social situation Changes to physical health Changes in care patterns Medication changes • Has the patient sought any help so far? • What interventions have occurred so far? Relevant Psychiatric History • • • • Current or previous diagnoses? Admissions to hospital - ?under MHA Are there any specific relapse signs? Interventions and their success… if not successful then why not? • Does the patient engage with services? • Informant history/ review old notes / discuss with relevant teams and GP Physical Health • Comorbidity common • Information from GP • May need general medical notes • Are they under a specialist currently – who & where? • Any investigations ongoing? • Do we need to liaise with other specialties? Medications • Polypharmacy is common • Find out any recent changes in medications • Compliance – does patient know what and why they are taking medications? • Don’t forget OTC medicines & allergies • Who gives the medications? • Is this with the assistance of carers or does the patient self medicate? Family History • Psychiatric illness • Neurological diseases • Dementia Personal and Social History • Not always easy at the first interview • Overview from birth to now • Can help to put problems into context • Level of education and occupational history indicates levels of expectation in formal cognitive assessments • Current situation important – – – – Living arrangements Care packages and what they help with Any deficits identified in care Are there any Lasting Powers of Attorney for health or finances? Alcohol And Drug History • Never assume the older person doesn’t drink or take drugs • Every patient must be asked! • Drinking pattern: – – – – – Estimate units consumed in average week Frequency Features of harmful use or dependence? Duration May be reflection of bereavement or isolation or may be a long standing issues Forensic History • Explore previous criminal convictions • Any pending cases? • Difficulties in later life might be pointer to developing problem (Lots of high profile celebrity cases involving the older person highlights the importance of asking about this) Pre-Morbid Personality • • • • How would the patient describe themselves when well? How would others describe them? How do they usually cope with difficulties / stress? How outgoing are they usually? • Have social/life changes meant previous abnormal personality traits have surfaced now? Mental State Assessment Mental State Examination • • • • • • Appearance and Behaviour Speech Mood Thoughts Perceptions Cognitions (we will focus on this aspect in a few minutes) • Insight The Assessment of Capacity • This is a complex assessment and is decision specific • It is important for complex decisions such as admission to hospital, treatment and placement decisions that a record of the patient’s capacity is documented and acted on accordingly NB: There is an MRCPsych LEP specifically about the Legal aspects of OA Psychiatry in year 2 which covers Capacity Physical Examination Physical Health Review • Full systems review • Focused examination (based on hx and presenting complaint) • Bloods, urine studies and relevant imaging important • Must act on findings • Discuss with seniors and refer if appropriate NB: There is an MRCPsych LEP specifically about Delirium Risk Assessment ‘The possibility of beneficial and harmful outcomes and the likelihood of their occurrence in a stated timescale’ Risk Assessment (Safety Profile), An Introduction To The Arrangements For Risk Assessment In Lancashire Care NHS Trust Risk Assessment • These are elements that should be thought about when assessing patient and brought together in formulating the risk – Suicide/self harm risks – Neglect/history of neglect – Harm to others – Treatment/illness related risks – Substance misuse – Social circumstances • Risk should be assessed regularly & be multidisciplinary Formulation •Description of: Biological •Problem & assessment •Differentials •Aetiology Predisposing Perpetuating Protective •Further investigations •Treatment / Management plan (MDT) •Prognosis Psychological Social Cognitive Assessment What is cognitive assessment? • Cognition – Not just memory – Includes other higher cortical functions such as orientation, perception, language, planning, judgement, & comprehension • Cognitive assessment – Starts with history taking – It is useful to be aware of the relation of function to different brain areas Basic Neuropsychology FRONTAL Problem solving, judgement, emotion regulation, & personality PARIETAL Visuospatial abilities, praxis OCCIPITAL: Vision TEMPORAL Language, speech, memory, naming Temporal lobes • Verbal memory • Language • Visual memory – Naming – Comprehension – Repetition • Reading • Writing (dysgraphia) • Prosopagnosia – (parieto-temporal) Parietal lobes • • • • Calculations* R-L disorientation* Finger agnosia* Dyspraxia • Receptive dysphasia • Naming / agnosia • Dysgraphia* *=Gerstmann’s syndrome • Constructional apraxia • Neglect / inattention • Topographical disorientation • Anosognosia Frontal lobes • Luria (hand sequence) • Go-no-go (inhibitory control) • Similarities (conceptualisation) • Cognitive estimates (abstraction) • Letter / category fluency (initiation) History taking & Assessment • What problems have they / others noticed with their memory? (if any) – – – – – – Do they struggle to remember days / dates? Have they forgotten recent events? Do they forget appointments / medication ? Do they tend to misplace things around the home? Do they ask repetitive questions? Do they ever get lost / struggle with route finding? – When did the symptoms start? Was it sudden? – Have they progressed slowly & steadily or step-wise? History taking continued… • Enquire about symptoms in other cognitive domains – – – – – Attention and alertness (including fluctuations) Language: Speech / Reading / Writing Executive function (planning, multitasking etc.) Spatial & perceptual functioning Praxis • Activities of daily living (ADLs) – Are they still able to do their domestic tasks – Any problems using household appliances / managing finances / driving? – Do they need assistance? • Psychological and behavioural symptoms – – – – Any changes in personality / out of character behaviours? Features of depression or anxiety? Delusions or hallucinations? Changes in sleep / appetite? General History • Past psychiatric history – History of treatment for depression • Past medical history – Vascular risk factors / CVA – Gait changes / falls – Bowel and bladder problems • Family History – Psychiatric or neurological illness – Dementia • Personal History – Age on leaving education; occupation – Drug & alcohol history • Risks – E.g. Self-neglect, driving, wandering, falls, fire, medication, financial abuse, aggression, carer stress, lack of insight Cognitive Assessment: The Practical Aspects Basic Screening Tests • MMSE© / AMTS • Quick & easy to use • Limited range of abilities – Don’t measure executive functioning – Poor memory assessment – Poor sensitivity • Other standard tools: e.g. MOCA / ACE-III For an informal assessment you don’t have to, or can’t always use a standardised tool…. Sometimes you have to improvise A simple mnemonic ORIENTATION REGISTRATION ATTENTION LANGUAGE MEMORY (RECALL) EXECUTIVE FUNCTION DRAW SHAPES Orientation Time: Please can you tell me….. • • • • • What time of day it is? (approx.) What day of the week it is today? What is the date? What month is it now? What year is it? Place: Could you tell me…… • • • • • What is the name of this building? What floor of the building are we on? Which town / city are we in? What is the name of the county? What country are we in now? Registration • Tell the patient you are going to say three words which you would like them to repeat • Can repeat the instruction up to five times • Inform them you will be asking again later Attention Serial subtraction OR Month of the year in reverse Language & Comprehension • Naming – 2 objects • Comprehension – Multi-stage instruction • Repetition – Words and sentence • Reading – Read and follow sentence • Writing – Ask to write sentence of their choice Memory / Recall • Anterograde – Ask them to repeat the items learnt earlier • Retrograde – What is the name of the current prime minister? – What year did World War II end? Executive Function • Motor – 3 stage Luria task – Alternating hand movements • Similarities – – – – Apple and orange? Table and chair? Tennis & rugby? Poem & statue? Draw Shapes • Copy wire diagram • Draw clock face Summary • A structured approach is important • Have low threshold for cognitive assessment • Devise a way of remembering the areas to be covered • A holistic approach to assessment / management is important • Cognitive assessment is easy if you’ve practiced! – With each other – But especially with real patients Further Reading • Butler R., Pitt B. Seminars In Old Age Psychiatry. Royal College Of Psychiatrists. Gaskell. 1993 • Risk Assessment (Safety Profile), An Introduction To The Arrangements For Risk Assessment In Lancashire Care NHS Trust • Young J, Meagher D, & MacLullich A. Cognitive assessment of older people. BMJ 2011;343: d5042 www.bmj.com/content/343/bmj.d5042 • For more detailed information on cognitive assessment the following is a useful and succinct article: – C M Kipps, J R Hodges. Cognitive assessment for clinicians. Journal of Neurology, Neurosurgery & Psychiatry 2005;76:i22-i30 http://jnnp.bmj.com/content/76/suppl_1/i22.full