Ref: BMMS 2001 and 2010
advertisement

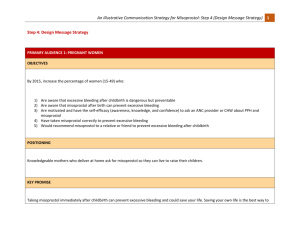
Scaling Up Misoprostol for Community-Based Prevention of Postpartum Hemorrhage in Bangladesh Dr. Tapash Ranjan Das PM (MCH) & Deputy Director (MCH), DGFP & Dr. Abu Jamil Faisel Project Director, Mayer Hashi project (an Associate Award of the RESPOND project) & Country Representative EngenderHealth Bangladesh A mother’s story Background The maternal mortality rate in Bangladesh decreased from 322 deaths per 100,000 live births in 2001 to 194 per 100,000 in 2010. Postpartum hemorrhage (PPH) is still the leading cause of maternal death (31% in 2010). Facility deliveries increased from 15% in 2001 to 23% in 2010. The government emphasizes the use of community skilled birth attendants (CSBAs) for home births and the development of a midwifery cadre to increase skilled attendance at facilities. EngenderHealth, through the USAID-funded Mayer Hashi project, supports the Ministry of Health and Social Welfare in preventing PPH through a twopronged approach: – Active management of the third stage of labor (AMTSL) at the facility level in 21 low-performing districts – Community-based distribution and use of misoprostol (Ref: BMMS 2001 and 2010) Major Milestones Establishment of the National PPH Prevention Task Force, Secretariat at EngenderHealth (October 2006) Approval of misoprostol for prevention of PPH by the Directorate General of Drug Administration and its inclusion in the updated essential drug list (May 2008) Approval of the piloting of community-based distribution of misoprostol using fieldworkers (August 2008) Agreement and approval of the effective misoprostol dose for preventing PPH for national use—400 mcg (March 2010) Approval of the scale-up plan for misoprostol by the National Technical Committee (NTC) of Directorate General of Family Planning (DGFP) (May 2010) Approval of the national scale-up plan developed with technical assistance from EngenderHealth (September 2010) Pilot Phase 1st pilot: Tangail District (Nov. 2008–June, 2009) – Implemented by DGFP, DGHS, and NGOs – Technical assistance, training, monitoring, and misoprostol distribution by EngenderHealth Formal evaluation of Tangail pilot (Oct. 2009) 2nd pilot: Cox’s Bazar (Nov. 2009–Mar. 2011) Mayer Hashi project: – Transferred skills and developed skills of DGFP and DGHS to implement pilot – Conducted training of trainers and provided onsite technical assistance to conduct training and orientation – Misoprostol distributed through govt. system All misoprostol tablets donated by Venture Strategies Innovations; produced locally Implementation Strategy Training of all fieldworkers (one day) Identification and registration of pregnant women by trained government and NGO fieldworkers Counseling and education by the fieldworkers of pregnant women, their intended birth attendants, and family members, using behavior change communication (BCC) materials Raising of community awareness through BCC activities and courtyard meetings, with emphasis on facility delivery Distribution of misoprostol tablets by government/NGO fieldworkers Follow-up of postpartum women by government/NGO fieldworkers Back-up of fieldworkers by trained facility-based health care providers, for management of complications Results of Pilot Programs Tangail: 71% of the expected pregnant women were registered. Among them, of those who delivered at home, 94% used misoprostol. There were no reported cases of misuse. 0.4% (39) of users reported minor side effects (fever, shivering). 0.3% (25) of users reported complications (retained placenta, PPH due to other cause) and were referred to hospital. An estimated nine maternal deaths were averted by the use of misoprostol. Cox’s Bazar: 69% of expected pregnant women were registered. Among them, of those who delivered at home, 95% used misoprostol. There were no reported cases of misuse. 0.8% (134) of users reported minor side effects (fever, shivering). 0.1% (26) of users reported complications (retained placenta, PPH due to other cause) and were referred to hospital. An estimated 10 maternal deaths were averted by misoprostol use. Four women died at home due to obstructed labor and mishandling by TBA. Lessons Learned Misoprostol can be effectively distributed through trained and supervised fieldworkers. One-day training was found to be sufficient for the fieldworkers. Service provider attendance is not required during misoprostol use, and wellcounseled women themselves can correctly use misoprostol to prevent PPH. Misoprostol can reduce PPH compared to previous delivery, as reported by the clients. Delivery attendants need to be educated on misoprostol’s benefits, so they will not prevent women from using the tablets. A few women reported misoprostol-induced side effects. The distribution of misoprostol after 32 weeks pregnancy is advisable. Close collaboration with the government, through implementation of pilots and provision of scientific evidence and continuous technical assistance, increases the chances of developing scalable programs. Challenges Raising community awareness about misoprostol use and removing myths and misperceptions about delivery and PPH Registering and reaching all pregnant women for misoprostol distribution Ensuring the accuracy and consistency of information provided through the government’s cascade training Ensuring that women use misoprostol, through consistent monitoring, supervision, and follow-up Ensuring the reporting of misoprostol use through the government’s management information system Ensuring a continuous supply of misoprostol for prevention of PPH Preventing inappropriate use once misoprostol is available countrywide National Scale-Up Incorporated misoprostol into the Health, Population and Nutrition Sector Development Program and Operational Plans (2011–2016) Allocated budget in the Operational Plans for implementation of scale-up Developed implementation modalities for both DGFP and DGHS Sent out implementation guidelines/circulars to both DGFP and DGHS field staff Tested training and BCC materials approved by DGFP and DGHS and handed over by Mayer Hashi Planned for a phased scale-up, and in July 2011 began scale-up in four districts, with technical assistance from Mayer Hashi Currently processing bulk procurement of misoprostol tablets Thank You