Anatomic Midline
advertisement

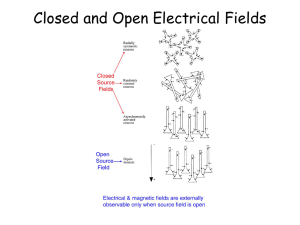
Relationship between the Anatomic & Physiologic Midline in Spinal Cord Stimulation Nicholas Kormylo MD1, Tobias Moeller-Bertram MD1, Kerry Bradley MS2, Joanne Olecko MS2, Brad Hershey MS2, Michael Gallucci MS2, Nitzan Mekel-Bobrov PhD2, Lilly Chen MD2, Jay Schnitzer MD PhD2 1University of California, San Diego, San Diego, CA 2Boston Scientific Neuromodulation, Valencia, CA Company Confidential 1 Disclaimer This study was supported by Boston Scientific Neuromodulation. No disclosures to report. Company Confidential 2 Background: Anatomic vs Physiological Midline •Lead placement at physiologic midline can maximize dorsal column (DC) stimulation • Law 1987 • Holsheimer et al 1993 • Barolat et al 1993 • North et al 2002 •However, anatomic and physiologic midline may not be coincident Company Confidential 3 Background: Anatomic vs Physiological Midline •Only 27% of combinations from leads on radiological midline result in symmetric paresthesia •Contacts may be as far as 3mm lateral to radiological midline and still generate bilateral paresthesia Company Confidential 4 Anatomic vs Physiologic Midline: Modern Technology Assessment Objective: Investigate relationship between anatomic/radiologic midline and physiologic midline in modern SCS Study Design: • Prospective, Single-center, Single-visit, Retrospective Analysis Evaluated: • N = 10 (7M/3F; 13 ± 9 months post-IPG) • Chronic pain patients with low back/leg pain implanted for > 3 months with: – Precision Plus™ SCS IPG – 1 or 2 Linear™ octapolar percutaneous leads positioned between T8-10 (verified by fluoroscopy) – 500us, 50Hz Company Confidential 5 Anatomic vs Physiologic Midline : Performance With patient in supine position, a variety of pre-randomized bipole combinations were programmed, on the most midline lead, determined by subject-reported paresthesia L-R balance. For each combination, subjects drew location of paresthesia on electronic body figure at usage amplitude (80% of range between perception and max tolerable). Company Confidential Figure adapted from North et al 2002 6 Anatomic vs Physiologic Midline: Data Analysis Methods: Paresthesia Symmetry Paresthesia Coverage: Body figure segmented along lines defined by Barolat et al 1993 Total Left Pixels Total pixels to left and right side of body tallied Paresthesia Symmetry = Total Left Pixels / (Total Right Pixels + Total Left Pixels) Average the symmetry scores for all bipoles using a given cathode Regression of cathode position with respect to anatomic midline and symmetry of paresthesia. Company Confidential Total Right Pixels 7 Anatomic vs Physiologic Midline: Data Analysis Methods: Cathode Position Cathode Position: •Only fluoro images deemed to be ‘pure AP’ •Definition: Anatomic Midline: •the piecewise continuous line joining the geometric midpoint between the pedicles •at multiple vertebral levels (T7 T11) flanking the leads. •To determine contact offset from Anatomic Midline: •calculated the perpendicular distance of the center of each programmed cathode •from estimated anatomic midline Company Confidential 8 Anatomic vs Physiologic Midline: Correlation Analysis Paresthesia Distribution vs Anatomic Midline Paresthesia 100% to Left Side of Body Anatomically Offmidline, but Symmetric Paresthesia Paresthesia Balanced on Both Sides Near Anatomic Midline, but highly Asymmetric Paresthesia R2 = 0.522 P < 0.001 Paresthesia 100% to Right Side of Body -5 -4 -3 -2 -1 0 1 2 3 4 5 Number of mm Left (-) or Right (+) of Anatomic Midline Company Confidential 9 Anatomic vs Physiologic Midline: Conclusions • We observed high coincidence of perfectly symmetrical paresthesia and anatomic cathode ‘midlinity’ •Approximately 20% of subjects demonstrated clear deviations from anatomic-physiologic midline coincidence. • Contributed to significant variability in the data (SE = 0.05) • Our results suggest that percutaneous leads may be less sensitive to anatomic/physiologic midline discrepancy than leads with wide contacts Company Confidential 10