Implementation Science:
What Does it Mean to Educators?
Presenters:
Patricia O’Sullivan, EdD, UC San Francisco
Summers Kalishman, PhD, University of New Mexico SOM
What we will do today
Objectives for today’s session
Overview and background
Small group work and discussion
◦ vignette transformation
Objectives for today’s session
Describe the intersection between
implementation science and medical
education.
Apply the principles of implementation
science to medical education to advance
the way educators engage in medical
education that addresses patient-centered
care.
Background/History
Implementation science is considered key to
developing optimal healthcare delivery and is
often unclear to educators outside of
continuing education
AAMC’s Group on Educational Affairs
convened a writing group in 2012 to develop
manuscripts and provide guidance on
Implementation Science in Medical
Education.
What is Implementation Science?
Implementation science involves the
scientific study of methods to promote
the systematic uptake of research findings
and other evidence-based practices into
routine practice to improve the quality
and effectiveness of health services
Assumption
Hard-working, intelligent health care
workers and/or medical educators will
intuitively implement the best evidence
into practice without any need of a skill
set for implementation
True or False?
Principles of IS
collaboration,
improved capacity,
rigor and relevance,
efficiency and speed, and
cumulative knowledge
Glasgow RE,Vinson C, Chambers D, Khoury MJ, Kaplan RM, Hunter C. National institutes of health
approaches to dissemination and implementation science: Current and future directions. Am J Public
Health. 2012;102(7):1274-1281
Advantages of IS
Systematically-integrated approach to outcomes
achievement
Comprehensive understanding of the complexities of
health care
Streamlined access to patient data to enhance the
meaningfulness of clinical, educational and research
initiatives
Eliminating waste and redundancies = cost effectiveness
Improved individual and population health outcomes
Tools in Implementation Science
Individual change behavior models—yes
Implementation and Quality Improvement
models--yes
◦
◦
◦
◦
Plan-Do-Study-Act
Six Sigma
Diffusion of Innovation
Root cause analysis
Interprofessional teams—yes
Patient medical centered homes--yes
IS Constructs Applicable to MedEd
Planned behavior/reasoned action
Trans-theoretical model
PRECEED/PROCEED model
Pathman model
Learning transfer model
Force field analysis
These models must compliment and
work with educational models
Need for evidence is changing
Accreditation requirements focus on
implementation of evidence-based
approaches
◦ UGME, GME, CPD/CME, MOC
CLER “clinical learning environment
review”
◦ sponsoring institutions need to demonstrate
leadership in quality improvement, patient
safety and reduction of health care disparities
Focus:
Desirable Patient Outcomes
reconsider educational activities when
performance gaps exist at
individual,
community or
patient population levels
Vision
Medical education is the bridge between research and
practice
Inter-professional collaboration is a must
Environments need be conducive to continued learning
Value-added by medical education need to be proven via
alternative research designs
Medical education needs to re-imagine new possibilities
for engaging medical professionals in learning
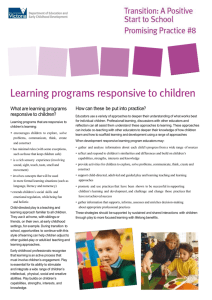
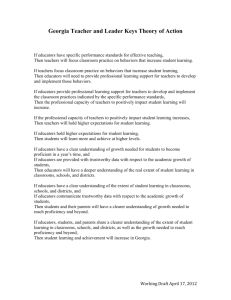
Medical Education as a Bridge between
Medical Research and Practice
Critical
Success
Factor 1:
Collaboration
& Integration
Medical
Research
Critical Success
Factor 2:
Culture of
Learning &
Development
Critical
Success
Factor 3:
Alternative
Research
Designs
Implementation Science Principles
(collaboration, improved capacity, rigor & relevance,
efficiency & speed, cumulative knowledge)
Medical
Practice
Educational research characteristics
align with IS
Conducted in social context (classroom, healthcare
office)
Low to no control over multiple variables
Need for progressive refinement of the study design
with each iteration
Large amounts of data about climate, learning and
system variables
Large undertakings in need of excellent coordination
Results reporting must include:
rich descriptions (environments, participants and variables)
study design and refinement
lessons learned
Potential for the future:
IS integration with education
1.
2.
3.
Strengthen interprofessional
collaboration and systems-level
integration,
Foster an environment conducive to ongoing learning and build educator
capacity,
Identify and apply alternative research
designs to demonstrate the value added
by medical education.
Small group exercise
Reports from Small Groups
 0
0