ling411-06-Classification&Laterality - OWL-Space
advertisement

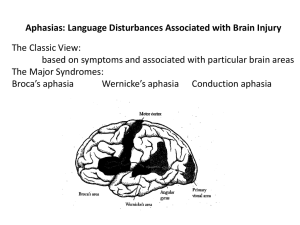
Ling 411 – 06 I. Classifications of Aphasia II. Laterality III. Varieties of Anomia Classifications “Classifications are a necessary evil” Antonio Damasio (1998) Problems of classification Different aphasics almost never share the same set of symptoms (Benson&Ardila 111) • Variations “are so plentiful as to be the rule” (B&A 117) • A single type of aphasia may have distinctly different loci of pathology (B&A 117) Conduction aphasia (117) • Parietal lobe • Arcuate fasciculus • Insula(?) Transcortical motor aphasia (118) Differing interpretations of sets of symptoms Different approaches to classification Wide variation in classification schemes Influential ones in history of aphasiology: • Wernicke-Lichtheim 1881, 1885 • Head 1926 • Goldstein 1948 • Luria 1966 • Benson 1979 • Benson & Ardila 1996 • Damasio 1998 But .. • All recognize just a small number of basic syndromes • Most of the variation in classification schemes is just terminological (Benson&Ardila 120) Damasio’s Classification (1998:34ff) Wernicke’s aphasia Broca’s aphasia Conduction aphasia Transcortical sensory aphasia Transcortical motor aphasia Global aphasia Anomic aphasia Alexia Pure word deafness Atypical aphasias The 1996 Benson & Ardila Classification (B&A: 119) Pre-Rolandic PeriSylvian ExtraSylvian Broca Aphasia Post-Rolandic Wernicke Aphasia Conduction Aphasia Extrasylvian Motor Aphasia Extrasylvian Sensory Aphasia Not included in above scheme: (1) Problems with reading & writing (2) Anomic aphasia (3) Global aphasia Features of the 1996 B&A Classification (B&A: 119) Based on two anatomical dichotomies: • Pre- vs post-Rolandic • Perisylvian vs. extrasylvian For every type, two subtypes • But the two subtypes can be just two ends of a continuous scale, not distinct subtypes Alternatives to usual terms: • “Extrasylvian” instead of “transcortical” • “Broca” instead of “Broca’s” • ‘Wernicke” instead of “Wernicke’s” A major anatomical-functional dichotomy: Front (anterior) vs. Back (posterior) Front • Action and planning of action • Process oriented Back • Perception • Perceptual integration • Object oriented Damasio vis-à-vis Benson & Ardila Damasio Wernicke’s aphasia Broca’s aphasia Conduction aphasia Transcortical sensory aph. Transcortical motor aph. Global aphasia Anomic aphasia Alexia Benson & Ardila Wernicke aphasia Broca aphasia Conduction aphasia Extrasylvian sensory aph. Extrasylvian motor aph. Global aphasia Anomic aphasia Wernicke II or Posterior extrasylvian Front-Back dichotomy and aphasia: Alternative terms/emphases Fluent Non-fluent Receptive* Expressive* Sensory Motor Posterior Anterior *But: (1) Very few aphasic patients are completely free of receptive difficulties (2) Virtually no aphasic is entirely without expressive problems (B&A 112) Damasio’s Categories as Anterior vs Posterior Aphasias (Or: Pre-Rolandic vs Post-Rolandic) Anterior Broca’s aphasia Transcortical motor aphasia Posterior Wernicke’s aphasia Conduction aphasia Transcortical sensory aphasia Alexia Pure word deafness Others: Global Aphasia: Both anterior and posterior Anomic aphasia: Can be either or both Atypical aphasias Extra-Sylvian Aphasic Syndromes According to Benson & Ardila “Extra-Sylvian” (a.k.a. “Transcortical”) Extrasylvian motor aphasia • Type I • Type II Extrasylvian sensory aphasia Sometimes just called ‘anomic aphasia’ • Type I • Type II Extra-Sylvian Aphasic Syndromes In all perisylvian syndromes, repetition is faulty In all extra-sylvian aphasic syndromes, repetition is intact (why?) “Aphasia without repetition disturbance almost invariably indicates pathology outside the perisylvian region” (B&A 1996:146) Extrasylvian motor aphasia Nonfluent output • Delayed initiation • Terse, poorly elaborated utterances • Incomplete sentences • Verbal paraphasia Good comprehension Good repetition Extrasylvian motor aphasia, Type I Left dorsolateral prefrontal damage • Anterior and superior to Broca’s area Non-fluent output, but repetition good Articulation is normal Difficulty following commands • Understand command but do not respond Damage anterior and superior to Broca’s area (Brodmann areas 45, 46, and/or part of area 9) (B&A 1996:152) Extrasylvian motor aphasia, Type II Damage to supplementary motor area • Occlusion of left anterior cerebral artery Non-fluent output, but good repetition Difficulty initiating speech Perhaps a purely motor disorder that does not involve basic language functions • (in which case it isn’t really a type of aphasia) Supplementary motor area Supplementary motor area Important in initiating action (not just speech) Extrasylvian sensory aphasia Speech is fluent Good repetition Comprehension is impaired Naming is impaired Paraphasia is frequent, even verbose • Semantic substitutions • Neologisms Echolalia (patients repeat words of examiner) Pointing is impaired Two subtypes Extrasylvian sensory aphasia, Type I Damage to temporal-parietal-occipital junction area • I.e., lower angular gyrus and upper area 37 Fluent spontaneous output Poor comprehension Naming strongly impaired Semantic paraphasia Extrasylvian sensory aphasia, Type II Damage to upper angular gyrus Fluent output Variable ability to comprehend speech Naming strongly impaired Few semantic paraphasias Repetition excellent Many circumlocutions Comparing Extra-Sensory Aphasia, Types 1 and 2 Type 1 Damage to TPO junction area Fluent spontaneous output Poor comprehension Naming strongly impaired Semantic paraphasia Repetition good Type 2 Damage to upper angular gyrus Fluent output Variable ability to comprehend speech Naming strongly impaired Few semantic paraphasias Repetition excellent Many circumlocutions Laterality Cerebral dominance for language Linguistic abilities are subserved by the left hemisphere in about 97% of people • 99% of right-handed people • A majority of left-handers But this is just a first approximation More refined look Some information is bilaterally represented • Highly entrenched items • Initial consonants of high-frequency words (?) • Some people have more bilateral representation than others • Women and left-handers tend to have more bilateral representation than men and righties Pitch, intonation, and other prosodic features subserved by RH Semantic information is in both LH and RH • But different aspects of semantic information Metaphor, irony, sarcasm, pragmatic features, inferencing, subserved by RH The Role of RH in semantics Conceptual information, even for a single item, is complex • Therefore, widely distributed • A network • Occupies both hemispheres RH information is more connotative • LH information more exact Left dominance for language in left-handers Wada test (Milner 1975), on left-handers • 69% aphasic after injection of left brain • 18% aphasic after injection of right brain • 13% aphasic after injection on each side Goodglass 1993:57 Right dominance for language in right-handers Crossed aphasia: Term for right-handers who suffer aphasia after RH injury Incidence of crossed aphasia is estimated at 1% Goodglass 1993:58 The genetics of laterality Matings of left-handed parents produce no more than about 50% left-handed offspring Annett’s theory (1985) • A single right-shift gene (rs+) • If rs++, right-handed (LH dominant) • If rs+-, right handed (LH dominant) • If rs-- (right-shift gene absent).. Can go either way Depends on environment, experience 50% probability of becoming left-handed Left hemisphere vs. right hemisphere Left hemisphere Right Hemisphere • Analytical thinking • Holistic thinking • Digital • Analog • Heightened contrast • Fuzzy boundaries • Proof • Hunches, intuition Question: What anatomical differences are responsible? Corpus Callosum (revealed by excision of top of right hemisphere) Corpus Callosum Separated right and left hemispheres Cutting corpus callosum separates them Isolated RH: • Limited one-word reading comprehension Some grasp of meanings But unable to make judgments about sound Isolated LH: • Awareness of both sound and meaning Varieties of anomia: Semantic categories Anomic aphasia Perhaps part of a continuum with extrasylvian sensory aphasia Comprehension is good in many cases • Unlike extrasylvian sensory aphasia Production and repetition are good Cannot be reliably localized • Many different areas of damage can result in naming difficulty But different semantic categories may be impaired with different areas of damage • Maybe not a true syndrome: Benson&Ardila 2 Cases of Rapp & Caramazza (1995) E.S.T. (901b) – Left temporal damage • “Meaning spared, couldn’t say the word”: R&C J.G. (902a) – Left posterior temporal-parietal • Meaning spared, couldn’t spell the word correctly, but phonological recognition okay Cf. Rapp & Caramazza, Disorders of lexical processing and the lexicon (1995) Patient E.S.T. (Rapp&Caramazza 1995:901b) Left temporal damage Shown picture of a snowman • Unable to name it • “It’s cold, it’s a ma… cold … frozen.” Shown picture of a stool • “stop, step … seat, small seat, round seat, sit on the…” Shown written form ‘steak’ • “I’m going to eat something … it’s beef … you can have a [së] … different … costs more …” What can we conclude? Assessment of E.S.T. by Rapp & Caramazza Responses of E.S.T. indicate awareness of the meanings (SNOWMAN, STOOL, STEAK) Therefore, “meaning is spared” (acc. To R&C) Warning: Proceed with caution The assumption of Rapp&Caramazza is easy to make • I.e., that meaning (conceptual information) is spared But there’s more to this than meets the eye! As we have seen, complex functions are not localized • Only simple functions have locations Conceptual information, even for a single word • Is complex, has many components • Therefore, is widely distributed We only have evidence that some of the conceptual information is spared Patient E.S.T. – a closer look Left temporal damage Picture of a snowman • “It’s cold, it’s a ma… cold … frozen.” Picture of a stool • “stop, step … seat, small seat, round seat, sit on the…” Written form ‘steak’ • “I’m going to eat something … it’s beef … you can have a [së] … different … costs more …” These are not definitions This is connotative information • Vague semantic notions about the meanings Compare patient J.G. (902a) Damage: Left posterior temporal-parietal Meaning spared, couldn’t spell the word correctly, but phonological recognition okay • digit: D-I-D-G-E-T “A number” • thief: T-H-E-F-E “A person who takes things” These are actual definitions Don’t forget this – (repeating) Some information is bilaterally represented • Highly entrenched items • Initial consonants of high-frequency words (?) • Some people have more bilateral representation than others • Women and left-handers tend to have more bilateral representation than men and righties Pitch, intonation, and other prosodic features subserved by RH Semantic information is in both LH and RH • But different aspects of semantic information Metaphor, irony, sarcasm, pragmatic features, inferencing, subserved by RH (Repeating:) The Role of RH in semantics Conceptual information, even for a single item, is widely distributed • A network • Occupies both hemispheres RH information is more connotative • LH information more exact Connotative information in RH Tests on patients with isolated RH resulting from callosotomy RH has information about (many) nouns and verbs • Not as many as in LH Semantic information differently organized in RH Zaidel (1990): “… the right hemisphere is characteristically connotative rather than denotative … . The arcs [of the semantic network] connect more distant concepts … and the organizing semantic relationships are more loosely associative and dependent on experience” (125) Baynes & Eliason, The visual lexicon: its access and organization is commissurotomy patients (1998) Semantic information: E.S.T. and J.G. Patient J.G. – real definitions • digit: “A number” • thief: “A person who takes things” Patient E.S.T. – connotative information • snowman: “It’s cold, it’s a ma… cold … frozen.” • stool: “ … seat, small seat, round seat, sit on the…” • steak: “I’m going to eat something … it’s beef … you can have a [së] … different … costs more …” Conclusion about E.S.T. RH semantic information is intact LH semantic information is wiped out Phonological information is spared in both hemispheres Question: Why can’t the RH semantic information be conveyed to LH phonology? Corpus Callosum (revealed by excision of top of right hemisphere) Corpus Callosum end