- No category
Scapular Dyskinesis in Railway Workers: Lahore Study
advertisement
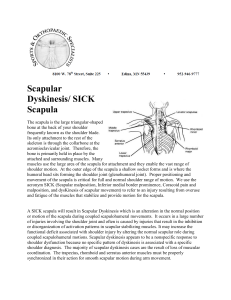
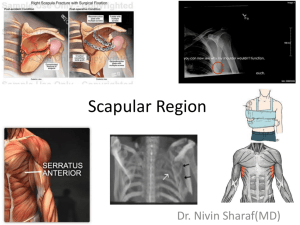
INTRODUCTION PREVELANCE OF SCAPULAR DYSKINESIS AMONG RAILWAY WORKERS WITH SHOULDER PAIN IN LAHORE Shoulder pain is the third most prevalent musculoskeletal condition in primary care The prognosis for musculoskeletal shoulder discomfort varies by individual, with an average of 50%. A systematic review of the global prevalence and incidence of shoulder pain Research suggests that shoulder pain is associated with certain factors, including being female, performing manual movements above the shoulder level, using vibrating tools, sitting in a cervical spine flexion position, standing work, performing repetitive physical work, and daily computer use . In addition to biomechanical job limits, psychosocial risk factors such as high demand, lack of autonomy, and insufficient social support, as well as psychological diseases including depression and anxiety, have been found. Prevalence and factors associated with shoulder pain in the general population: a cross-sectional study Shoulder pain is a common musculoskeletal problem caused by a variety of diseases affecting the shoulder's architecture, particularly the rotator cuff tendons, which are prone to inflammation, degeneration, and rips due to their unique location between moving bones. As a musculoskeletal disorder, shoulder discomfort is a major cause of morbidity and functional disability in everyday life and professional activities, which raises social and economic costs for people, companies, and the state. The following options best describe the ergonomic variables' exposure frequency during a workday. These variables include repetitive movements, heavy lifting, vibration/tremor during the working day, sitting position, forward leaning position, weighted sitting position, postural orthostatic, forward flexed, kneeling, and lying posture. Prevalence and factors associated with shoulder pain in the general population: a cross-sectional study SHOULDER JOINT The articulation of the upper extremities with the trunk or axial skeleton is accomplished via the shoulder, a complicated joint. It is essential to the operation of the hands and arms. ANATOMY The shoulder is made up of a network of soft tissues that cover the skeleton. The scapula is a flat, triangular bone that forms the posterior side of the shoulder girdle. It has 17 muscle attachments, and half of the primary shoulder joint is formed by its anterior projection, known as the glenoid. Muscles include the trapezius, which is a broad flat muscle originating from the posterior upper spine and inserting on the lateral scapula, clavicle, and acromion. Its role is in stabilization of the scapula, and rotation to enable movement in the scapula-thoracic plane. The serratus anterior, innervated by the long thoracic nerve, originates from the margin of the first 8 ribs. Its function is in scapular motion, as it pulls the inferior aspect of the scapula laterally and forward, enabling shoulder abduction beyond 90 degrees via motion in the ST plane. The posterior muscles along the scapula's medial border, known as the rhomboid muscles, support the scapula's depression. The levator scapulae, which attaches at the medial scapula after emerging from the cervical spine, rotates and elevates the scapula to permit movement in the scapular plane. The acromioclavicular (AC), sternoclavicular (SC), scapulothoracic (ST), and glenohumeral (GH) joints make up the four minor joints that make up the shoulder complex. Anatomy and physical examination of the shoulder SCAPULA Complex shoulder kinematics are coordinated and maintained in large part by the scapula. For glenohumeral (GH) and scapulothoracic (ST) movements, the rotator cuff (RC) and the scapula regulate energy and force transfer. From a biomechanical standpoint, the range of motion (ROM) of the shoulder encompasses over 65% of a spherical joint whose stability is guaranteed by a number of elements, including ligaments, muscle activity, and bone integrity. By preventing excessive translations that could jeopardize the integrity of the joint, the RC and scapula enable three-dimensional shoulder movements . Scapular resting posture and motion are frequently altered in patients with shoulder abnormalities (i.e., aberrant 3D GH angulation, subacromial space dimension, GH strain, muscle strength, and shoulder muscle activation). [HTML] Scapular dyskinesis: from basic science to ultimate treatment The scapula moves normally in a combination of three movements: Rotating upward or downward around a horizontal axis perpendicular to the scapula's plane Rotation of the scapula in both internal and exterior directions around a vertical axis Tilt of the scapula anteriorly and posteriorly around a horizontal axis [PDF] Prevalence of Scapular Dyskinesis in Swimmers: A Cross-sectional Study SCAPULAR KINEMATICS Complex shoulder kinematics are coordinated and maintained in large part by the scapula. Energy and force transfer for glenohumeral (GH) and scapulothoracic (ST) movements are controlled by the scapula and the rotator cuff (RC) . From a biomechanical standpoint, the shoulder's range of motion (ROM) encompasses over 65% of a spherical joint, whose stability is guaranteed by a number of elements, including ligaments, muscle activity, and bone integrity By preventing excessive translations that could jeopardize the integrity of the joint, the RC and scapula enable three-dimensional shoulder movements Scapular resting posture and motion are frequently altered in patients with shoulder abnormalities (i.e., improper 3D GH angulation, subacromial space dimension, GH strain, muscle strength, and shoulder muscle activation) [HTML] Scapular dyskinesis: from basic science to ultimate treatment SCAPULAR DYSKINESIS Scapular dyskinesis (SD) is a disorder characterized by abnormal scapular mobility or function Type I SD is a posterior displacement from the posterior thorax of the inferior medial angle.Type II SD is a posterior displacement from the posterior thorax of the entire medial border of the scapula and Type III SD is an early scapular elevation or excessive/insufficient scapular upward rotation (dysrhythmia) during dynamic observation. [HTML] Scapular dyskinesis: from basic science to ultimate treatment The scapula's clinical significance due to conflicting reports on how it can both positively and negatively affect shoulder function. This is probably because of three important aspects of scapular function First, during arm movement, synchronous and simultaneous muscle activation and stabilization are made possible by the large number of muscles that attach to the scapula. Because of the many degrees of freedom that are made possible by this, different people can perform the same task in different ways. Second, only one planar movement is possible due to the thorax's ellipsoid shape. The thorax's shape and the different fiber orientations of the muscles acting on the scapula are both responsible for the absence of single plane movement. Complex rotations and translations make up scapular motion, which is essential for the scapula to work as a component of scapulohumeral rhythm, the combined motion of the scapula and moving arm that forms the foundation of efficient upper extremity use. The internal/external rotation, upward/downward rotation, and anterior/posterior tilt of the scapula are referred to as accessory arthrokinematic motions. whereas the medial/lateral and elevation/depression scapular translations can be described as physiological movements like the voluntary gross actions of rotation, abduction, or humeral flexion. Active motion should be described by medial translation, which is the dynamic movement of the scapula around the thorax posteriorly towards the vertebral column, and lateral translation, which is the dynamic movement of the scapula around the thorax anteriorly towards the chest. Retraction and protraction should be used to describe the scapula's end position once the movement has stopped. Current views of scapular dyskinesis and its possible clinical relevance OTHER NAMES A change or departure in the scapula's typical resting or active position during shoulder movement is known as scapular dyskinesis, or SICK scapula syndrome. Scapular dyskinesis, which combines the words "dys" (alteration of) and "kinesis" (movement), describes abnormal scapular movement. [PDF] Prevalence of Scapular Dyskinesis in Swimmers: A Cross-sectional Study Although the term "winging" has been used interchangeably with dyskinesis, it is more appropriate for abnormal scapular motion caused by neurological impairment. [PDF] Prevalence of scapular dyskinesia among truck drivers: An observational study PREVELANCE The variety of factors, such as disparities in the populations that are being targeted, disparities in the definition and assessment of dyskinesis, and the use of clinical techniques for qualitative observational examination, which can result in inconsistent measurements. The majority of research indicates that people who need to perform repetitive overhead motions for their daily tasks are more likely to suffer from dyskinesis. Between 30 and 70 % of athletes who participate in sports like baseball, tennis, swimming, volleyball, cricket, kayaking, and surfing have dyskinesis. Depending on the anatomic diagnosis, studies conducted on symptomatic patients show an incidence ranging from 64% to 100%.Managing scapular dyskinesis Among athletes who play overhead and non-overhead sports, the frequency of SD is 54.5% and 33.3%, respectively . The frequency of SD in swimmers varies from 8.5% to 69%. [HTML] Scapular Dyskinesis and Associated Factors in Adult Elite Swimmers CAUSATIVE RISK FACTORS Clavicle fracture, scapular body, glenoid fracture, AC joint injury, GH joint internal derangement (labral injury, GH instability, biceps tendon injury, GH arthritis, adhesive capsulitis), rotator cuff injury, and post-traumatic scapular muscle injury are examples of pathoanatomical causative factors. Scapula snapping Neurologic injury (cervical radiculopathy, dorsal scapular nerve, spinal accessory nerve, long thoracic nerve) Soft tissue tightness (pectoralis minor, upper trapezius, latissimus dorsi, biceps, posterior GH capsule, and posterior shoulder muscles) and muscle weakness and inhibition are common alone or in conjunction with pain generators (lower trapezius weak, altered activation, rotator cuff impedement, weakness, imbalance, core weakness—observed in up to 50% of cases of dyskinesis, loss of voluntary control, altered activation, early in patients with periscapular pain of any cause). Managing scapular dyskinesis DIAGNOSTIC FEATURE The existence of scoliosis and an increase in thoracic kyphosis may directly affect scapular mobility,resulting in an irregular shape Scapular retraction and protraction may be impacted by excessive cervical lordosis.In less than fifteen seconds, a burn-like discomfort may indicate scapular muscular weakening. DIAGNOSTIC TESTS 1. Scapular assistance test : Assesses the glenoid involvement and the scapula's impact. The anterior serratus and inferior trapezius muscles are assessed during this process. The focus of rehabilitation is indicated by the removal or alteration of these muscles' symptoms. 2. Scapular retraction test : The lateral arms are relaxed at the side of their body in the first position. This position allows for the palpation and marking of the scapula's lower-medial angle on both sides. The next difficult step is to locate the reference point on the backbone. Both sides of the reference measurements are taken from the spine to the medial aspect of the scapula. The same is done with arms that have a maximal internal rotation of the glenohumeral joint and an abduction of 90° or less .scapula's slip test reveals that excessive protraction makes it more susceptible to dyskinetic patterns. The limit of abnormality is a 1.5 cm asymmetry, which is most frequently observed in 90° shoulder abduction. The patient's arms are relaxed at the side of their body in the first position. This position allows for the palpation and marking of the scapula's lower-medial angle on both sides. 3. The lateral scapula's slip test : Reveals that excessive protraction makes it more susceptible to dyskinetic patterns. The limit of abnormality is a 1.5 cm asymmetry, which is most frequently observed in 90° shoulder abduction. The patient's arms are relaxed at the side of their body in the first position . This position allows for the palpation and marking of the scapula's lower-medial angle on both sides. The next difficult step is to locate the reference point on the backbone. Both sides of the reference measurements are taken from the spine to the medial aspect of the scapula. The same is carried out with arms that have a maximal internal rotation of the glenohumeral joint and an abduction of 90° or less. [PDF] Scapular dyskinesis: biomechanics, evaluation and treatment 4. Scapular dyskinesis test (SDT): People with SD can be categorized into three levels: normal motion, subtle dyskinesis, and evident dyskinesis. This is one of the numerous techniques frequently employed during a shoulder pathology evaluation that are listed in Supplement A. Despite this, the SDT has been shown to be a legitimate and dependable technique for detecting SD. https://pmc.ncbi.nlm.nih.gov/articles/PMC10324350/ 5 . Test of Dynamic Scapular Dyskinesis: This involves closely monitoring the scapular motion while doing weighted shoulder flexion and abduction. The patient abducts both arms after first flexing them forward while holding a 2-pound (1 kg) weight in each hand. A lack of coordinated motions (such as early scapular elevation or shrugging when lifting the arm, or quick downward rotation while lowering the arm) or winging, or prominence of the medial or inferior scapular boundaries, are observed by the clinician. A "yes" (dyskinesis is present) or "no" is used to indicate any departure from the norm. https://www.academia.edu/download/68372498/IJHSR010.pdf 6. Lateral Scapular Slide Test (LSST) : It is used to determine scapular position with the arm abducted 0, 45, and 90 degrees in the frontal plane. Measurements were taken in 3 different positions: Sitting/standing with arms resting on the side, Hands on the waist, Thumbs posterior (45 abduction), 90 degrees abduction and maximal internal rotation. Measurement should not be more than 1.5 cm according to current studies. Goniometry was used for finding the ranges of shoulder flexion and abduction and cervical ranges of flexion, extension, lateral rotation of right and left and right left rotation. https://www.academia.edu/download/91183431/prevalence-of-scapular-dyskinesia-in-bankers.pdf POPULATION Computer office workers frequently work with their heads forward for extended periods of time which can place a lot of strain on the cervical spine's supporting soft tissues and impair shoulder and scapular function, leading to scapular dyskinesis . [HTML] Neck and shoulder pain with scapular dyskinesis in computer office workers Swimmers: Swimming's repetitive overhead motions wear down the rotator cuff, scapular stabilizers, and anterior and posterior shoulder muscles This can lead to scapular instability and a decrease in scapulohumeral rhythm. These changes in scapular kinematics are thought to be clinically significant in swimmers because they are linked to shoulder pathology and decrease shoulder function efficiency and lead to Scapular dyskinesis which results from abnormalities in the scapula's dynamic movement or static position in swimmers. [HTML] Scapular Dyskinesis and Associated Factors in Adult Elite Swimmers Cricket is a worldwide sport that has historically been well-liked in Commonwealth countries. Fielding and bowling are the most dangerous sports for shoulder injuries because they require overhead throwing and excessive tension across the shoulder joint .Crickters with a variety of shoulder disorders have been observed to exhibit scapular dyskinesis, which is defined as changes in both static and dynamic scapular position and motion. [PDF] Prevalence of scapular dyskinesis in novice cricket players Dentist :Scapular stabilizer dysfunction is evident on the dominant side of dentists, particularly at the level of the medial border and inferior angle of the scapula. This dysfunction shows itself as dyskinetic scapula during movements and asymmetrical scapular position at rest. This could be caused by overuse, weakness, bad posture, or a mix of all three and leads toward scapular dyskinesis Prevalence of Scapular Dyskinesis in Working Dentists: An Epidemiological Study BANKERS The prevalence of scapular dyskinesia in this population must be ascertained in order to enhance work performance, reduce the risk of scapular dyskinesia in bankers and alleviate pain among office workers. https://www.academia.edu/download/91183431/prevalence-of-scapular-dyskinesia-in-ba nkers.pdf Athletes who play overhead sports have a prevalence of SD of 54.5%, while those who play non-overhead sports have a prevalence of 33.3%. The prevalence of SD in swimmers varies from 8.5% to 69%. https://www.mdpi.com/1648-9144/61/10/1885 FACTORY WORKERS Scapular dyskinesis is common in people who work in a variety of occupations, such as construction and manufacturing, as sugar factory workers frequently need to perform repetitive motion, heavy lifting, and extended periods of heavy labor. These jobs can put a lot of stress on the shoulder complex, especially the scapula. https://search.ebscohost.com/login.aspx?direct=true&profile=ehost&scope=site&authtype=crawler&jrnl=09701052&A N=180918218&h=amS%2Bz3A4HzbfXX9KfRJhyZdAIAi0DCsBN3v%2BGhiSjG%2FecBsbjkEU7vLaUOGuAoHtm3UE 5ddzi6YxerUTEiDpgA%3D%3D&crl=c PREGNANT LADY Due to ergonomically challenging breastfeeding positions, scapular dyskinesia is significantly more common in postpartum nursing mothers. https://jhrlmc.com/index.php/home/article/view/482 STROKE The first symptoms following a stroke are a low-tone flaccid stage without voluntary control, followed by a spastic stage that causes asymmetry in the scapulothoracic joint. Scapular mechanics were largely disregarded while the majority of stroke patients received treatment in all areas. Therefore, shoulder pain may result from untreated scapular dyskinesis. https://journalmsr.com/effects-of-proprioceptive-neuromuscular-facilitation-technique -on-scapular-dyskinesis-in-patients-with-subacute-stroke/ POPULATION Railway employees included welders, assistants, painters, blacksmiths, coachbuilders, coolies and manual machine handlers. https://www.researchgate.net/profile/Mahar-Safdar-Ali-Qasim/publication/354116664_Prevalenc e_of_Musculoskeletal_Disorders_among_Manual_Workers_in_Railway_Workshops_Lahore/lin ks/6125e468a8348b1a46042156/Prevalence-of-Musculoskeletal-Disorders-among-Manual-Work ers-in-Railway-Workshops-Lahore.pdf Railway maintenance workers' shoulder, elbow, wrist, hand, finger, neck, back, and knee symptoms have been related to biomechanical exposures, such as hand-arm vibration and repetitive activities like lifting, pushing, and bending. https://www.researchgate.net/profile/Siti-Amdan/publication/397231030_INTERNATIONAL_J OURNAL_OF_ENTREPRENEURSHIP_AND_MANAGEMENT_PRACTICES_IJEMP_ASSE SSMENT_OF_KNOWLEDGE_ATTITUDE_AND_PRACTICES_KAP_TOWARDS_THE_PR EVALENCE_OF_WORK-RELATED_MUSCULOSKELETAL_DISORDER_WMSD_AMON G_M/links/69096766a404d65709a232bb/INTERNATIONAL-JOURNAL-OF-ENTREPRENEU RSHIP-AND-MANAGEMENT-PRACTICES-IJEMP-ASSESSMENT-OF-KNOWLEDGE-ATT ITUDE-AND-PRACTICES-KAP-TOWARDS-THE-PREVALENCE-OF-WORK-RELATED-M USCULOSKELETAL-DISORDER-WMSD-AMONG.pdf Musculoskeletal conditions are more common and have serious repercussions for employees. According to earlier Asian studies, 65% of Indian Railway Sahayaks (coolies) had musculoskeletal symptoms. https://www.researchgate.net/profile/Mahar-Safdar-Ali-Qasim/publication/354116664_Prevalenc e_of_Musculoskeletal_Disorders_among_Manual_Workers_in_Railway_Workshops_Lahore/lin ks/6125e468a8348b1a46042156/Prevalence-of-Musculoskeletal-Disorders-among-Manual-Work ers-in-Railway-Workshops-Lahore.pdf SAHAYAKS/COOLIES/BAGGAGE HANDLERS/TRAIN PORTERS Every railway station has private staff members, such as coolies or train porters. Musculoskeletal disorders can be brought on by the nature of work for coolies or train porters. https://www.rmj.org.pk/fulltext/27-1580486548.pdf Sahayaks engage in demanding labor and intense physical exertion on a daily basis. These exercises involve pushing, carrying, and lowering weights while assuming awkward postures (bending and twisting), as well as frequently lifting large objects above shoulder height. https://www.tandfonline.com/doi/abs/10.1080/10773525.2018.1507187
 0
0
advertisement



Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users