British Journal of Orthodontics/Vol 6/1979/125-143 Printed in Great Britain
The Straight-Wire Appliance
Lawrence F. Andrews, D.D.S.
2025 Chatsworth Boulevard, San Diego, Ca 92107, USA
Abstract. Qualities of the Straight-Wire Appliance are summarized, and its background and clinical use
reviewed. A need for objectively established treatment goals impelled a study of naturally excellent occlusions.
Consistent characteristics were identified. Their apparent suitability for most patients indicated the feasibility
of a new appliance, preprogrammed to take patients to such goals with reduced wire bending, shorter treatment
time and chair time, and greater consistency and exactness in end results. A bracket-siting method is recommended; terminology is defined; appliance design features and extraction bracket options are described.
Discussion includes advantages of the SWA, misconceptions and a comparison with other appliances.
When the Straight-Wire Appliance was introduced
to the profession in 1970 it seemed advisable for
transitional purposes, to explain the 'SWA' with
reference to its closest kin, and so it was sometimes
called 'a sophisticated edgewise appliance'. Actually,
although it employs an edgewise slot, the SWA fits
no existing appliance category because of certain
innovations in concept, in implementation, and in
effects or results:
the bracket slot in relation to the crown. (Edgewise bracket bases are contoured only horizontally.)
5. The distance from the base of the slot to the base
of the bracket varies for each tooth type,
satisfying in/out requirements.
6. Built-in guidance (tip, torque and in/out)
minimizes archwire manipulation, making tooth
movement more direct, saving treatment time
and chair time, and improving consistency in end
results.
7. The guidance features are preprogrammed to
reflect research findings that are consistent with
the requirements of functional occlusion. Thus,
better occlusal goals are promoted, although
these goals can be modified by the SWA user.
8. Bracket design facilitates accurate bracket
placement at a crown site more reliable than any
reference point previously used in this process.
This site is a 'part of the package' of the StraightWire approach, and it is sustained by an explicit
rationale. Final slot location no longer varies
because of faulty reference points or inconsistencies in banding techniques.
9. Extraction Brackets are available, and provide
anti-tip and anti-rotation features which promote bodily movement.
10. Each bracket carries its own identification as to
tooth type- a convenience that will grow in
value as direct bonding evolves.
I. Each bracket is customized for its tooth type,
reflecting several considerations including relative size of teeth, gingival and hygienic factors,
ease of clinical use, patient comfort, and
reduction of occlusal interference by brackets.
2. Pre-angulated slots accomplish mesiodistal tooth
tip, permitting the bracket to be placed 'squarely'
on the crown instead of being angulated. This
eliminates the potential for 'rocking' that is
inherent in the two-point contact of an angulated
bracket.
3. The bases of the brackets are inclined for each
tooth type, to achieve proper tooth 'torque' with the centre of each slot at the same height as
the middle of the clinical crown (an essential for
Straight-Wire technology). This innovation replaces the edgewise slot-torque that is not
compatible with true straight-wire treatment.
SWA slots are not torqued, although they may
appear to be because of the design of the face
of the bracket.
4. SWA bases are contoured vertically as well as
horizontally, resulting in good bracket-to-tooth
fit and a dependable, reproducible location of
How it Started
© Copyright Lawrence F. Andrews 1979.
Uneasiness about treatment objectives provided the
impetus for the underlying research. During my
125
L. F. Andrews
early years of orthodontic practice my own treatment goals often were, frankly, estimations of what
I thought ought to be (about) right for the patient at
hand. The work of America's most skilled orthodontists - models shown at national and other
orthodontic meetings - revealed many different
occlusal schemes and tooth positionings. There was
no evident explanation either for the case-to-case
variations in any one orthodontists's results, or for
the major differences doctor-to-doctor. The ensuing
research was based on the premise that what nature
does in its own best products should be worthy of
emulation. This was not an entirely new concept.
Bolton, for example, included excellent untreated
dentitions in a sample reported in 1958. Dewel
(1949) wrote of useful referents and norms offered
by 'nonorthodontic normals.' The project here
reviewed amounted to a study of the best static
occlusion that occurs naturally, compared with the
best end results achieved by leading American
orthodontists. (Functional occlusion is discussed
later in this article.) The findings have been reported
elsewhere (Andrews, 1972). For readers not
familiar with that report, here is a tight summary:
A gathering of plaster models was begun, and
the resultant collection is believed still to be unique:
120 models of dentitions that had never had
orthodontic treatment and that needed none, in
the professional judgment of the many sources of
the material (other orthodontists, general dentists,
university faculty and students). The teeth were
straight and pleasing in appearance with no obvious
defects, and the bite looked generally correct.
The relationships and positions of the crowns in
these models were subjected to detailed study. Six
significant characteristics were found to be notably
consistent in occurrence, and they were designated
'the Six Keys to Normal Occlusion'. As Wheeler
(1965) perceived long ago, ' ... in anatomy,
variations must be expected . . .. Nevertheless,
certain tendencies may be discovered, and those
tendencies must be considered in order to acquire
perspective ... definite tendencies may ... have
important practicable application.'
The next step was methodical examination of the
other group of models - the treated cases shown by
skilled orthodontists. Eleven hundred and fifty
such models were studied from 1965 to 1971.
Findings strengthened the inferences drawn from
the nonorthodontic normals. There were indeed
significant differences between nature's best and
many of orthodontia's best. And the lack of any one
of the six signal · keys was predictive of other
inadequacies.
126
A condensed general description of the findings is
given in the illustrations (pages 128-129).
The SWA is designed to efficiently reach the Six
Keys as an end result, if that is what the orthodontist
using it wants. For certain cases, however, that
objective is not attainable. I have never suggested
that the Keys are realistic for treatment of the
extreme or abnormal variations that every dentist
sees occasionally.
I do not think such extreme or abnormal cases
account for more than five per cent of our patients.
We are talking, you see, about normal distribution
- the familiar bell shape on a statistical graph. The
great hump in that bell encompasses most cases.
When we say the basically normal dentitions can be
treated to the Six Keys, 'normal' has far more scope
than 'average' or 'median'. As Graber (1972)
expressed it: 'A cardinal axiom to begin with is
that the normal in physiology is always a range,
never a point.'
The original report of the Keys research
(Andrews, 1972) noted that some conditions
require help from other specialists such as the oral
surgeon, or from the general dentist. My course
syllabus lists some of the problems that place a
patient outside the basically normal group. It
states in italics: 'To (orthodontically) achieve these
goals with all patients is not feasible ... ' Then it
adds, ' ... but to stop short of them when they are
attainable may be unacceptable' (Andrews, 1975).
Functional Occlusion
The Six Keys research dealt with static occlusion.
It is entirely appropriate to ask whether the results
can be reconciled with demands for good functional
occlusion.
I am not sure that even all educators have fully
recognized that a new era has come of age in our
specialty. Today, we have the burden or privilege
of orthodontically achieving functional occlusion.
Not enough recognition has been given to Or
Ronald H. Roth for his role in this event. I gladly
acknowledge my debt to him for demonstrating to
the profession a sound functional occlusion scheme
that is orthodontically attainable even in extraction
cases. Happily, the requirements of functional
occlusion are totally compatible with advanced
standards for static occlusion. The concordance of
findings in these two areas is significant. So is their
coincidence in timing. Is it reaching too far to
suggest that substantiation lies in this circumstance,
so that when occlusion is approached from different
directions, the conclusions of independent re·
The Straight-Wire Appliance
searchers coincide? I am not saying that Roth's
findings and the Keys are identical; the answers to
different questions were being sought, and are still
developing. But the answers are so mutually supportive that they seem complementary.
Let me illustrate with one example the elements
shared. As every dental student knows, tooth types
are specialized, each for its own roles. A tooth, like
a carpenter's tool, is damaged by being subjected to
the wrong type or duration of stress. Therefore, just
as a journeyman cabinetmaker shields his saw
blade from vagrant contacts, so nature provides
'mutually protective occlusion' (a functional occlusion scheme) to guard human teeth against
improper abrasions and stresses.
In desirable static occlusion the teeth are harmoniously located and positioned in the jaws, and
the mandible and maxilla are in the appropriate
skeletal relationship. Such dentitions, I submit,
should exhibit the Six Key static characteristics,
and also allow the teeth to function according to the
mutually protective occlusal scheme endorsed by
Roth: i.e., without undesirable cusp interferences,
and with no problems of the type caused in the
TMJ when the mandible must always detour
excessively to prevent collisions or sideswipings by
cusps which, at that point in mastication, should
have no contact. In a smoothly functioning society
of teeth, the individuals mate intimately when they
should; and when they should not, they avoid contact
Without help from compensatory mandibular movement that abuses the TMJ. It is an intricate but
automatic scheme of behaviour: when teeth are not
productively collaborating they ostracize each other.
Now we can tie static and functional goals
together. Centric occlusion and centric relation
should coincide. This is a major consideration. In
my writing and lecturing I have assumed it as
axiomatic. Roth wants it stated, not assumed.
Given that condition, the Six Keys 'are consistent
With desirable functional-occlusion goals' (Roth,
1975). He has said more, to the same point (Roth,
1976), but those few words tell the story.
We orthodontists have much left to learn and
much yet to refine. But evidence to date sustains
confidence that advanced static and functional
occlusion goals not only are compatible but seemingly validate each other. As Ramfjord and Ash
0966) foresaw: ' ... good anatomic relationships
Provide the best background for functional harmony'.
Central Tendency
The SWA is designed to take advantage of some
basic facts about dental anatomy (the 'tendencies'
Wheeler referred to) and the known characteristics
of excellent occlusion. That is what makes it a
practical orthodontic tool. Nature's grouping of
individuals (making any one species more alike
than unlike - called by some 'the central tendency')
is of immense value to physicians and dentists. For
decades, orthodontists have properly exploited it in
some ways. The shape of bands for a given tooth
type is the same regardless of size. And we do not
have to stock an infinite variety of sizes. Nor do we
use all sizes with the same frequency. Band trays
from the manufacturer are supplied with some
sizes in greater quantities than other sizes - a
familiar application of what we know about
normal distributions and use to predict needs.
Size
Tooth size has no effect on angulation or inclination, which are important. When an individual has
small teeth, all his teeth are generally (with some
qualifications) found to be proportionally small.
The same consistency exists in dentitions with large
teeth. Even root-length is best studied in terms of its
ratio to tooth-length in the same individual (Plets
et a/, 1974). As for in/out, alignment is not a matter
of whether a patient's teeth are large or small. True
tooth-size discrepancies, of clinical significance,
are the exception rather than the rule.
Shape
No two tooth types are identical, but teeth of any
one type are very much alike. No dentist would
have difficulty describing or carving any specific
tooth type. Scramble lOO extracted teeth, toss them
on a table, and which of us could not easily identify
each tooth?
Contact points and angulations
One of the important similarities within a given
tooth type is the location of contact points. The
commonality of this feature has been precisely
described (Wheeler, 1965). This being true, the
angulations of teeth of any one type must have
much in common - be the teeth large, small, wide
or narrow.
Optimal Treatment Objectives
Each patient must be examined and diagnosed as
an individual, but in angulation, inclination and
in/out, most individuals' teeth vary within so
limited a range that they can be treated to the same
goals. The SWA is programmed to deliver treatment
127
L. F. Andrews
Six Keys to Normal Occlusion
Key 1. Molar relationship. (A) The distal surface of the
distal marginal ridge of the upper first permanent molar
contacts and occludes with the mesial surface of the
mesial marginal ridge of the lower second molar.
(B) The mesio-buccal cusp of the upper first permanent
molar falls within the groove between the mesial and
middle cusps of the lower first permanent molar. (C)
The mesio-lingual cusp of the upper first molar seats
in the central fossa of the lower first molar.
Key 2. Crown angulation, the mesio-distal 'tip'. In
normally occluded teeth, the gingival portion of the
long axis of each crown is distal to the occlusal portion
of that axis. The degree of tip varies with each tooth type.
Key 3. Crown inclination, the labio-finguaf or buccofinguaf
'torque'. Crown inclination is the angle between a line
90 degrees to the occlusal plane, and a line tangent to
the middle of the labial or buccal clinical crown. (A)
Anterior crowns (central and lateral incisors): In
upper incisors, the occlusal portion of the crown's
labial surface is labial to the gingival portion. In all
other crowns, the occlusal portion of the labial or buccal
surface is lingual to the gingival portion. In the
non-orthodontic normal models, the average inter-incisal
crown angle was 174 degrees.
128
Occlusa!Piallf
The Straight-Wire Appliance
(B) Upper posterior crowns (cuspids through molars):
lingual crown inclination is slightly more pronounced in
the molars than in cuspids and bicuspids.
(C) Lower posterior crowns (cuspids through molars):
lingual inclination progressively increases.
Key 4. Rotations. Teeth should be free of undesirable
rotations. If rotated, a molar or bicuspid occupies
more space than normally- a condition unreceptive to
normal occlusion. A rotated incisor can occupy less
space than normal
Key 5. Tight contacts. In the absence of such
abnormalities as genuine tooth-size discrepancies,
contact points should be tight.
Key 6. Curve of Spee. A flat occlusal plane should be
f treatment goal as a form of overtreatment. Measured
rom the most prominent cusp of the lower second
molar to the lower central incisor, no curve was deeper
than 1·5 mm in the nonorthodontic normals. (A) A
deep curve of Spee results in a more confined area
for the upper teeth, creating spillage of upper teeth
mesially and distally. (B) A flat curve of Spee is most
receptive to normal occlusion. (C) A reverse curve
of Spee results in excessive room for the upper teeth.
129
L. F. Andrews
to optimum end results with few if any archwire
bends needed because of tooth morphology.
It seems evident that orthodontics, orthodontists,
and patients all would benefit if treatment goals
could be objectified. The Six Keys are offered for
consideration as one step in that direction. The
Keys are being evaluated or taught at leading
schools of orthodontics, and have been applied by
hundreds of doctors. I believe that several years of
clinical results now credibly sustain the proposition
that the Keys are suitable treatment objectives for at
least 90 per cent of North America's orthodontic
patients - the large majority who, sharing the
preponderant alikeness of any species, have teeth
within the normal ranges of shape and size.
New Appliance Needed
The occlusion research was launched to get a better
understanding of occlusion and how it was related
to the buccolabial surfaces of the crowns at the
bracket site. There was no intention originally to
produce a new appliance, but the need for one
became evident. Orthodontists are a dedicated
company of specialists who strive hard for excellence; some of the explanation for their widely
diverging end results seemed to lie in the nature of
traditional appliances. A commonality of objectives for most patients meant that it should be
feasible to develop an efficient appliance, economical in time and energy requirements, for getting to
these goals. Like many orthodontists, I had been
laboriously doing 'ballpark' wirebending for certain
teeth for virtually all my patients - for example, to
get torque and tip in the upper anteriors, and in/out
alignment, and progressive torque for the lower
posterior teeth. For any one of those purposes, the
amount of bend was similar for most patients - a
fact confirmed when measurements of the nonorthodontic normal models provided the needed
standards and goals for each tooth type. These
data seemed totally compatible with the existing
body of knowledge about contact-point locations
and other relevant factors including aesthetic goals
and occlusion. Why, then, plod through the same
processes for every patient and every tooth, to
achieve effects that an advanced appliance could
deliver?
Building treatment into the appliance to improve
consistency of results, or to ease the doctor's
workload, was not a new concept. It had been
suggested by Angle. Progress had been made when
Holdaway and others began angulating brackets on
bands; when Lee introduced the edgewise torque
bracket; and when Jarabak recommended torque
130
in the bracket and angulation of the bracket. But
by the 1960s, although we had bands for each
tooth type we were, for the most part, still using
untorqued edgewise brackets. Torqued brackets
were available, but in no less than 5-degree increments. Many doctors were ordering brackets
angulated on bands, but there was no consensus
about the right number of degrees, and little if any
advice was offered by manufacturers. No bracket
had angulated slots. We did not have brackets of
varying thickness to satisfy in/out requirements.
No brackets had vertical curvature in the base and
none had torque built into the base. There was much
to be done in improving precision and consistency
of results, and in transferring standardized, routine
work from the chores of the doctor to the role of
the appliance.
The Six Keys could be preprogrammed.
Appliance design could take advantage of known
commonalities and uniformities, conducting teeth
at least to proximities of angulation, inclination
and in/out objectives. Ultimate detailing, if indicated in some cases, would be a suitable application of the doctor's expertise.
Design Challenges
However, it is one thing to decide the positions
teeth should be in; it is quite something else to deal
with the dynamics of getting them there efficiently.
Here we encounter opposite and equal effects,
interrelationships of three-dimensional forces and
movements - a fabric of complexities.
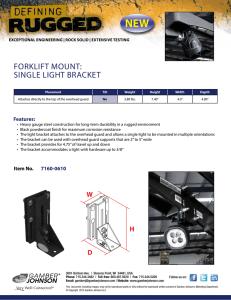
One example is in the effect that anterior archwire
torque has on the tip of upper anterior teeth.
Failure to understand this can result in improper
posterior occlusion or undesirable spaces. This
phenomenon is shown in the 'Wagon Wheel'
illustration (Fig. 1).
'There is no such thing as an isolated orthodontic
act .... Much more effort is required to prevent or
control unwanted movements than to apply the
primary forces' (Thurow, 1970). A proper appliance
might reconcile the interwoven forces and responses.
But how to cope with the dynamics of this compleX
puzzle? Since, within any one dentition, tooth types
always are significantly different each from the
other, each would require its own bracket - a
bracket type for each tooth type. This had never
been done.
Bracket siting
Moreover, regardless of the sophistication of
bracket or appliance, if it is not located properlY•
The Straight-Wire Appliance
900
A- ------
nP
&
TORQUE
Furthermore, historically, clinicians have related
bracket to band, then band to tooth, a two-step
procedure offering two opportunities for error.
Such a range in practice is one of the reasons why
end results vary from orthodontist to orthodontist,
community to community, and country to country.
Is it any wonder, then, that we orthodontists have
so much trouble communicating with each other;
that often, when trying to discuss a certain case or
treatment in general, we have to diverge to specify
our individual procedures in banding or bracketing?
'Two millimetres' - from what? 'Three degrees' very well, the angle between which two lines? So
the creation of an appliance with built-in treatment
destinations had to be founded on prior selection
of a precise and unchanging crown site where the
essential measurements would originate. For such
a site to have scientific reliability, it had to be
dependably locatable and refindable. Successful use
of any appliance (but especially one with built-in
treatment) is equally dependent on knowledge and
utilization of such a point. The method now to be
described will yield extra benefits for every orthodontist, regardless of what appliance he uses at
present or will use next year.
The siting method
Fig. 1. The wagon wheel. Anterior archwire torque
negates archwire tip in a ratio of 4:1. Clinical result is
that the gingival portions of the crowns converge 1° for
each 4° of lingual torque placed in the wire.
all that has been programmed into it is proportionately altered. For instance, the torque required in
the gingival one-third of a crown can be from 5 to
40 degrees different from that required by the
occlusal half. Traditional bracket placement technique often involves measurement from an un?ependable reference point or line, such as an
Incisal edge. Central incisor edges commonly have
been altered by fracture, chipping or wear. The
height of central incisor crowns varies from patient
to patient, so any chosen, constant distance from
t~e incisal edge for bracket placement will bring
different inclination results from patient to patient.
Another trouble source exists in the simple fact that
different clinicians use different reference points in
the banding procedure. (Even using the same poor
?ne could be a gain.) Some measure or 'eyeball'
Incisors, but with posterior teeth simply band to the
lllarginal ridges. Some arbitrarily band occlusally,
some gingivally, thus facing different torque
requirements for guiding a tooth to a given position.
Whether we use bands or direct bonding, we should
think in terms of bracket placement. We should
never speak of banding, but call the process
'bracketing'. Many of us were trained to think in
terms of the long axis of the tooth, meaning
crown-plus-root. But our work is almost always
keyed to the buccal or labial surface of the crown.
Thus, as crowns are our usual clinical base, they
should also be our communication base or referent.
(The clinical rather than the anatomical crown is
always my meaning.)
Primarily, we require a procedure that yields
uniform, constant bracket-siting - keyed from
dependable features of the clinical crown. Buccolabial crown surfaces differ in contours from one
tooth type to another. Is there a 'common denominator', an easily identified location common to all
crowns? All of us have studied the development of
teeth. We know that they form embryonic lobes that
fuse together, creating the total crown. The resulting
morphology includes consistent developmental
landmarks. Among these are the ridges and grooves
on the crown's labial or buccal surfaces. These
ridges and grooves can be easily recognized, and are
not significantly subject to environmental alterations
such as chipping, wear and fracture. For several
years now, users of the Straight-Wire Appliance
131
L. F. Andrews
have made good use of these landmarks by successfully and consistently placing brackets at the
midpoint of the long axis of the clinical crown. I
recommend that every orthodontist consider the
advantages of this procedure.
The LACC
Where is the long axis of the clinical crown (LA CC)?
1. Viewed from the buccolabial perspective: For
molars the LACC is identified by the dominant
vertical groove on the buccal surface. For all
other teeth it is at the vertical mid-developmental
ridge, the most prominent portion in the central
area of the buccolabial surface.
2. Viewed from mesiodistal perspective, the LACC
is represented by a line tangent to the middle of
the crown's labial or buccal surface. For molars
it parallels the dominant groove. For all other
teeth, it parallels the mid-developmental ridge
(Fig. 2).
in a healthy gingiva. If in doubt, you can measure
from the cemento-enamel junction when establishing the midpoint of the clinical crown. Nature,
then, has made it simple for us. All we lack is a
brief word or term for this chosen site. We want to
refer to a point on the Long Axis so why not call
it the LA-point? True, that site-name does not
contain a reminder that we mean the clinical
crown's long axis midpoint; but nobody ever
speaks of an 'LA-point' in reference to any other
axis: so the proposed abbreviation, having only
one usage, should suffice.
This landmark is refindable and is more reliable
than any other in use; more consistent, less exposed
and less vulnerable to environmental hazards.
Fusion and ridge lines are unlikely to be changed in
a human lifetime. We can gratefully accept them as
more of Nature's guidelines. When we do so, we
acknowledge the utility of the tooth portion made
readily available to us - the clinical crown. Its long
axis is not parallel to that of our old standby, the
long axis of the tooth. The LACC is far more
practical for measuring and for other uses. No
X-rays needed, no guessing; this axis can be directly
seen, touched, even marked with a pencil and shown
in a mirror to the patient. Its tip and torque can be
promptly and precisely established, and then
watched during the progress of treatment.
Moreover, keying to the long axis of the crown
makes accurate bracket placement much easier.
One simply places the vertical components of each
Straight-Wire bracket (e.g., the tie-wings) parallel
to the LACC, and the base point of the bracket at
the LA-point.
Terminology
The LA-point
The long axis of the clinical crown (LA CC) and the
LA-point have been discussed. Needed are brief
explanations of a few other word usages. Some
elements here are applicable only in connection
with use of the Straight-Wire Appliance.
The vertical line, the LACC, is easy to find; but how
far 'up' on it should the bracket be placed? At its
midpoint (Figs. 2 and 4). The crown has no
obvious horizontal axis or equator, so you judge
the point, just as you would easily select the midpoint on a 5 millimeter line. The accuracy of this
procedure has been measured and found satisfactory. It is as accurate as judging the middle of
the sella turcica on a lateral headfilm - a common
diagnostic procedure that has been proven reliable
with experiments.
The depth of the sulcus probably averages I mm
Bracket Base: The most lingual portion of the
bracket stem (Fig. 3).
Bracket Stem: The portion of a bracket between the
bracket base and the most lingual portion of the slot
(the slot base) excluding tie-wings (Fig. 3).
Slot Base: The lingual wall of the slot (Fig. 3).
Base Point: On the bracket base, the point that
would fall on a lingual extension of the slot axis
(Fig. 3).
Slot Axis: The buccolingual (or labiolingual)
centreline of the slot. It is equidistant from the
Fig. 2. The long axis of the clinical crown, and the
LA-point.
132
The Straight-Wire Appliance
A
Tie wings
-- Identification mark
--Slot
- -Welding tabs
L_L --~--- L- .J
~ts
8
Tiewi~n--
- ldentilication mark
1
Vertical
V_,,__,
.
Base
Slot po1nt-j .·
Base-- ___
base~-
~
-3=-
~
Face
·
--Slot po1nt
Stem
ne wingsFig, 3. Bracket components.
gingival and occlusal slot walls and is centered
111esiodistally. When the bracket is properly placed,
the slot axis, if extended lingually, would include
~he base point and the LA-point, and it would be
Included by a labial or buccal extension of the
Andrews plane.
Slot Point: The centre point of the slot axis (Fig. 3).
The Andrews Plane: Assuming no curve of Spee,
an imaginary plane that would intersect the crowns
of properly positioned teeth at their LA-points,
separating the occlusal and gingival portions of
each crown; or, in the case of an individual tooth
Whether malpositioned or not, the plane that would
Fig, 4. Andrews Plane and the LA-point.
designate those same portions of the crown as
occlusal or gingival (Fig. 4). In full Straight-Wire
technology, the extended plane also includes the
base point and the slot axis. (If there is a curve of
Spee, the geometric form would technically be a
curved surface instead of a plane.)
Crown Angulation: Crown 'tip'. It will be described
in terms of degrees, plus or minus. The degree of
crown tip is the angle formed by the long axis of the
clinical crown (as viewed from labial or buccal
perspective) and a line perpendicular to the occlusal plane. A 'plus reading' is awarded when the
gingival portion of the LACC is distal to the
incisal portion. A 'minus reading' is given when the
gingival portion of the LACC is mesial to the
incisal portion (Fig. 5).
Crown Inclination: Crown 'torque'. It will be
expressed in degrees, 'plus' or 'minus'. A plus
reading is given if the gingival portion of the crown
is lingual to the incisal portion (Fig. 6B). A minus
reading is earned when the gingival portion is labial
or buccal to the incisal portion (Fig. 6A).
Fig. 5. Crown angulation or 'tip'.
133
L. F. Andrews
Upper Central hcisor
Fig. 6. Crown inclination or 'torque'.
SWA Design and Comparisons
We have examined the reasons for pre-programming suitable treatment into the appliance. We
have explored why bracket placement is vital, and
we have proposed a new siting location and
A
·~~~-t ----:- 1
2
-
c
Fig. 7. (A) Rolling potential of a flat-base bracket on
curved surface of a crown, indicating effects on torque,
on height of slot, and on horizontal distance of slot from
intended bracket site-which affects in/out requirements.
(B) Three of the possible bracket positions inherent in
the rolling potential described above. (C) Bracket with
vertically curved base eliminates the rolling potential,
assuring consistent location of slot in relation to bracket
site.
134
Upper Second Bicuspid
Fig. 8. (A) Untorqued edgewise brackets located at
LA-point. (B) Pretorqued edgewise brackets located at
LA-point; and (far right) two such brackets
superimposed. (C) Straight-Wire brackets on the
LA-point.
appropriate terminology. Now let us scrutinize
another concept adopted early in the design
process: that at the conclusion of active treatment,
the bracket slots should form so straight a line that
a flat and unbent rectangular archwire could be
placed in them without bends or torsion, or one
already there would be under no stress (Figs. 7C,
8C and 9G).
The SWA, if used as designed, utilizes a 'straight'
wire throughout treatment. Significant to the entire
SWA concept is a fact worth noting: at the beginning of treatment, when SWA slots are as 'maloccluded' as are the teeth, the slots actually are
nearly enough aligned so they will accept an
archwire that is merely deflected, not kinked. Now
link that beginning-of-treatment fact with an
image of the same slots at the conclusion of active
treatment. The progress of all slots toward the
end-result has been co-ordinated - travelling
straight vector lines, the positional relationships
always clear.
Not counting the advantages during treatment,
what other values exist in having the archwire
straight when the teeth are properly positioned?
I. This portion of the treatment plan terminates
itself, automatically. A flexed archwire provides
force only until it returns to its original passive
form. When it stops working, its passivity is a
signal that the goals are reached. You know that
'you are there'.
The Straight-Wire Appliance
~I
~~-
,1 ,, i \"
A~~~
··~M~RR·
C-~~~R
D~~RF'f-
·~~R~
F~~~R~
G-~~Ffp~Fig, 9. Potential variations in locations of slots at
conclusion of active treatment (lower posterior teeth).
Rows A, Band C: untorqued edgewise brackets. Rows D,
E and F: pre-torqued edgewise brackets. Row G:
Straight-Wire Appliance brackets.
2. Even if a patient misses an appointment, no
unplanned overtreatment occurs, because the
appliance is self-limiting.
3. The archwire is straight because the slots are
lined-up, and their single-file ranking reflects the
same condition in the crowns' LA-points. An
arrow would follow the slot axis and then pierce
the base point and the LA-point; all are on the
Andrews plane. Thus you have an integrated,
relatively simple and easily understood set of
relationships. The angulations, the inclinations,
the bracket sitings, the built-in treatment
process itself - all are referenced to the same
known point on every tooth, a landmark that
you can return to, or that another orthodontist
can find if he must repeat or extend your
procedure because of patient transfer.
Occasionally, at the beginning of treatment,
some prefer the use of multiple loops. This is not
truly a departure from Straight-Wire treatment, for
the working area of the wire (between the loops) is
straight before insertion and is only deflected.
(With extraction cases, in the intermediate and later
stages of treatment it usually is necessary to install
second order bends unless SWA Extraction
Brackets are used.)
Design features
Straight-Wire technology is dependent, first, on the
use of specific, reliably locatable bracket-siting
points: the LACC and the LA-point. It is also
dependent on certain appliance design features.
The SWA includes some proprietary features not
found collectively in conventional edgewise or
pretorqued appliances. Among SWA innovations
are torque built into the base of all brackets, a base
contoured vertically as well as horizontally, tip
built into the bracket, and in/out and molar offset
built into the appliance.
Torque in the bracket base
Here we deal with the first of the crucial elements in
SWA design: torque - or buccolingual or labialingual inclination.
Exactly how is torquing accomplished by the
SWA? The bracket base is inclined in relation to
the stem, allowing the stem to be parallel to the
Andrews plane (Figs. 7C, SC and 9G). Making the
torquing function a product of the base design
allows all slots (at the completion of active treatment) to be aligned with each other and thus
receptive to a flat, unbent rectangular archwire. A
separate bracket for each tooth type is necessary,
with proper torque for each tooth type built into
the bracket base. Nothing in SWA design, except
compound base curvature and slot tip, is so vital to
effectiveness of the appliance.
Traditional non-torqued edgewise brackets are
not suitable for Straight-Wire technology, because
manual manipulation of the archwire is required
for torque and height (as well as for in/out and
molar offset) (Figs. SA and 9A).
Pretorqued edgewise brackets are also unsuitable
for Straight-Wire technology, because the torque is
in the face rather than the base of the bracket. They
do eliminate the need for some manual torquing of
the archwire, but second order bends are required
135
L. F. Andrews
because the slots' relationships to the Andrews
plane vary, proportionately to the tooth torque for
each tooth type, requiring adjustments to be made
in the archwire. Figure 8B shows pretorqued
edgewise brackets in place on an upper central
incisor and a bicuspid. The central crown has
positive inclination and the bicuspid a negative
inclination. The pretorqued slot method cannot
produce alignment of the slots at the conclusion
of active treatment, for the slot centres are not at the
same height as the LA-points. This is because each
bracket's stem is at a right angle to the base of its
pretorqued bracket, and the LA-point, base point
and slot point are not and cannot be simultaneously
on the Andrews plane. The third drawing in
Figure 8B shows positive 7-degree and negative
7-degree pretorqued edgewise brackets superimposed. When their bases are parallel, the slot
centres line up; but that would occur clinically only
if the crowns' surfaces were parallel. In fact, the
crown surfaces are not parallel when the upper
central incisor and upper bicuspid are properly
positioned, so the slots do not line up.
Figure 9F shows pretorqued edgewise brackets
located at the LA-points. Note that the slots do not
fall on the Andrews plane. They require progressive
archwire height adjustment (second order bends)
if they are to receive a full-size archwire passively.
This dilemma might appear to be resolvable by
machining the slots progressively more gingivally,
to allow them to line up. But Figure 90 shows what
would happen if this were attempted: the slots
would run out of bracket material. If, alternatively,
the brackets were sited progressively more gingivally on the crowns, the judgment error in placing
them would be likely to be unacceptable.
vertical bracket base during bracket placement. So
is the height of the slot in relation to the occlusal
plane or Andrews plane, destroying proper relationships between the LA-point and the slot axis.
Third, the various positions involve the distance
of the slot from the tooth's surface, affecting in/out
requirements.
The variation in torque requirement is illustrated
in Figure 10, showing a bracket rolled through a
range of 7 degrees, a mere 50 per cent of its potential
range with this tooth. The tooth shown, a lower
first bicuspid, does not even have the greatest
crown curvature. To appreciate the full significance
of this factor, visualize the continuing up-and-down
flow that could exist within one arch if flat-base
brackets were rolled (each bracket in an opposite
direction) to their maximum points of variation
(Figs. 7A, B and 9C, E). Bracket bases that are
not curved vertically are easy for the manufacturer
to make but place the burden on the orthodontist,
for he must compensate for inherent slot location
variables throughout treatment.
Compound contoured bases
Fig. 10. Effect on torque of flat-base bracket's rolling
potential.
The base of each bracket must be contoured to fit
firmly and unchangingly when the bracket is
installed 'squarely' (not angulated) at the chosen
site. This is the second of 'the crucial elements in
SWA design.' Most conventional appliances have
simple horizontal curvature in the bracket base.
The Straight-Wire Appliance added vertical curvature. It is the combination of horizontal and
vertical curvature that is referred to as 'compound
contour' or 'compound curvature'.
Installing a bracket with a vertically flat base
against the vertically curved surface of a tooth
allows a variety of slot-to-crown positions. Figures
7 (A and B), 9 (C and E) and 10 show the problems.
Torque is affected by the variety of possible slot
positions due to the rolling potential of the flat
136
-LA. point
A
8
c
Lower Second Bicuspid
Angulated slots
Correct mesiodistal angulation is delivered by a
process that is direct and cleanly efficient. A gently
flexed archwire is inserted into slots that are exactly
as maloccluded as are the untreated teeth. Even
though the slots are angulated for tip, each bracket
is squarely aligned with the LACC (Figs. 2 and 11 A).
As the archwire straightens itself, it carries the
teeth to their desired tip positions. Most important
of all, manual wirebending with its large judgmenterror factor is eliminated. Most routine chores are
reduced to inserting a series of progressively larger,
stiffer archwires, decreasingly flexed as the tooth
positions improve and the bracket slots approach
The Straight-Wire Appliance
EDGEWISE
This is a
comparison of the use
ol the variable thickness,
Standard Straight Wire
Appliance brackets- which
eliminate tlrst order arch wire
bends and molar ol/set bends
with the conventional
'
[:';.
STRAIGHT· WIRE
APPLIANCE
edge~:~~i~:~~~~~~;;:J)~hlch
archwlfe bends
and molar
ol/set bends.
'LAce""
Fig. 11. (A) When tip is built into the slot, the bracket
can mate solidly with the tooth. (B) When bracket is
~ngulated on tooth to accomplish tip, a rocking potential
ts created.
the formation of a single row. The ultimate lining-up
of the slots occurs simultaneously with the achievement of the preprogrammed tip. Meanwhile there
has been no zig-zagging, no trial and error, no
need for re-estimations of multiple directions, no
guessing about interacting compound forces, no
compensatory manipulations to offset misjudgment
or inaccurate manual wirebending. Because the
bracket need not be angulated to achieve slot tip,
there is no concern about variable slot location or
rocking on a two-point base contact.
If a bracket with a base curved horizontally is
angulated on the tooth to achieve tip, this creates a
two-point contact between tooth and two diagon~lly-opposite corners of the bracket base, resulting
In a potential for rocking (Fig. llB). The bracketrolling range of 7 degrees shown in Figure I0 for an
Unangulated bracket would be replaced by a rocking
Potential of more than 7 degrees, if the bracket were
angulated on the tooth. Even a sophisticated
bracket such as the SWA with compound curvature
and torque built into the base could also rock if
angulated on the tooth. That is why the slot must be
angulated, not the bracket.
In/Out and molar Offset
No one who has manipulated in/out and molar
f!set bends into wires for thousands of patients
W1ll be surprised that measurement of the nonor~hodontic normal models proved these features
SUitable for building into the appliance. Figure 12
shows how this is done in the SWA.
h Tooth types differ in buccolabial prominence at
t e LA-point, but there is a constant pattern in
Upper teeth, and a different but constant pattern in
0
1
•
:
1
(
Fig. 12. lnfout and upper molar offsets in the SWA.
lo:wer te7th . (For example, molars are most promment, mc1sors least prominent in both arches·
. the upper arch the lateral' incisors are less'
but m
prominent than the central incisors.) Because the
relative prominences are constant and known the
designer can vary the thickness of the bra~kets
accordingly - inversely, of course. Elimination of
~rst o~der archwire bends has several advantages,
mcludmg accuracy, time-saving, and the enabling
of en masse space closures without bracket interference from wirebends.
A 10~ o_ffset for the distal cusps of the upper
molars 1s mcorporated in the SWA brackets for
those teeth.
Other aspects
Designing an individual bracket for each tooth
type permits innovations not involving the slot or
base. SWA tie-wings, instead of being symmetrical,
step-out farther on the gingival sides of posterior
brackets, resulting in easier ligation and less
frequent gingival impingement (Fig. 13). The vertical tie-wings also are the convenient guides regularly used in siting the bracket in relation to the
crown, for they straddle and parallel the LACC.
O~e furthe~ speci~l design element in the StraightWire Apphance 1s that every bracket is visibly
ide~tified as to its tooth type. Drop a tray, and your
ass1stant can readily re-sort the brackets.
Extraction Brackets
The SWA Standard brackets are primarily for
non-extraction cases, so are right for about half of
our patients. Beyond those, they can be and are
used by some doctors for extraction cases; but this
137
L. F. Andrews
Anti-rotation
Fig. 13. Gingival wings of posterior brackets, in SWA,
are stepped out. Results: easier ligatlon and less
frequent gingival impingement.
application requires the use of auxiliaries and/or
first-order archwire bends to discourage rotation,
plus second order bends to discourage tipping.
SWA Extraction Brackets, like SWA Standard
Brackets, have standard amounts of built-in tip,
torque and in/out. In addition, they provide two
functions not needed in Standard Brackets: anti-tip
and anti-rotation.
When we translate a tooth, we have no way of
applying a force exactly where it should exert itself
for maximum efficiency. Ideally, the focus of force
should be more centrally and apically located - at
the focal point of resistance to movement. But we
cannot attach a bracket at the tooth's centre of
resistance because it lies below the cemento-enamel
junction. Instead, the bracket takes hold of an
available point on the crown. The LA-point is the
best we can do, but with all its virtues it is still,
from an engineering standpoint, the 'wrong' place,
in two ways:
1. Since our primary forces are applied at the
buccal surface of the crown, when we pull or
push mesiodistally the tooth rotates:
2. At the same time, the root tags along behind,
unless the orthodontist uses second order
archwire bends or angulates the bracket on the
tooth.
SWA Extraction Brackets compensate for both
the rotation tendency and the tipping tendency
during translation.
138
Anti-rotation is accomplished by the bracket as a
function of the slot's horizontal relationship to the
bracket base (Fig. 140, F, H). The total amount of
anti-rotation needed is proportional to the distance
the tooth is to be moved, and includes allowances
for an additional factor: when active treatment is
completed, the buccal surfaces of teeth naturally
rotate toward the extraction site. This occurs in
serial extraction cases before treatment, and in
most extraction cases after treatment, even if space
closure and root paralleling were completed. SWA
Extraction Bracket design provides the right
increment of anti-rotation to compensate for the
predictable post-treatment phenomenon.
When a doctor uses SWA Standard brackets in
extraction cases, in addition to anti-rotation
measures, he must apply second order archwire
bends or angulate the bracket on the crown (which
has undesirable effects that have already been
discussed). SWA Extraction Brackets will permit
such cases to be treated for the most part with
unbent archwires.
Anti-tip
SWA Extraction Brackets overcome mesiodistal
tipping tendency as a function of the slot's vertical
relationship to the bracket base (Fig. 14C, E, G),
and the use of a lever or 'Power Arm' that provides
proper moment of force (Fig. 14C, E, G). As with
anti-rotation, the total amount of anti-tip provided
is proportional to the distance the tooth is to be
moved and includes an allowance for the root's
natural rebound that will complete a net effect that
leaves the tooth with the desired degree of tip. Is
I00 per cent precision always achieved in the final
net effect? Of course not. The state of orthodontic
science (or 'art' if you prefer) is a long way from
enabling us to manage compound forces and
individual tissue conditions (or individual patients)
with flawless control. But anti-rotation and anti-tip
features provided in the Extraction Brackets
accomplish chores that the doctor must otherwise
attend to by archwire manipulation, and to a large
extent by guess.
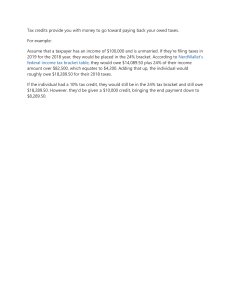
Three types of extraction brackets
Up to specified maximums, the amounts of anti-tip
and anti-rotation needed are proportional to the
distance of translation, and include an allowance
for overtreatment factors. There are three Extraction Brackets designed for each cuspid, and
three for each posterior tooth type except upper
molars, for which there are four (Table 1). A
The Straight-Wire Appliance
Standard Cuspid Bracket [ID
Standard SW bracket for upper right
cuspid with normal 11 o slot tip (no
anti-tip).
The Standard upper right cuspid
bracket has a bilaterally symmetrical
profile (no anti-rotation).
B
A
ANTI-TIP
ANTI-ROTATION
Minimum Extraction Bkt. [I]
/:::-_)
~
Power Arm for proper moment of
force.
Minimum Extraction Bracket with 2°
anti-tip (11 +2=130 total tip).
c
~
~
The minimum Extraction Bkt. has 2o
anti-rotation and has one
identification notch on the occlusal
portion of its base.
D
Medium Extraction Bkt. ~
Power Arm for proper moment of
force.
The medium Extraction Bkt. has 40
anti-rotation and has two identifying
notches on the occlusal portion of its
base.
Medium Extraction Bkt. with 30 antitip (11 +3=140 total tip).
E
F
Maximum Extraction Bkt. [3]
Power Arm for proper moment of
force.
The maximum Extraction Bkt.
has 6° anti-rotation and has three
identifying notches on the occlusal
portion of its base.
Maximum Extraction Bkt. with 40
anti-tip (11 +4= 150 total tip).
G
H
Fig. 14. Comparisons-SWA Standard and Extraction
Brackets. SWA Standard Brackets are designed
specifically for non-extraction cases. When used on
teeth requiring translation they need supplemental wire
bends (for anti-tip and anti-rotation). Examples above are
of the Standard and three Extraction Brackets for an
upper cuspid. Compared to Standard Brackets (A and B),
Straight-Wire Extraction Brackets have additional slot tip
(anti-tip), and power arms and anti-rotation. There are
three Extraction Brackets for each posterior tooth type
including cuspids. A minimum Extraction Bracket (C and
D) has 2 anti-tip and 2° anti-rotation and is recommended
for teeth requiring up to 2 mm of translation and on teeth
adjacent to extraction sites so that they will properly
mate with the tooth that is being translated. A medium
Extraction Bracket (E and F) has 3° anti-tip and 4o
anti-rotation and is recommended for use on teeth to be
translated 2-4 mm. A maximum Extraction Bracket (G and
H) has 4° anti-tip and 6° anti-rotation and Is
recommended for use on teeth to be translated more
than 4 mm. Straight-Wire Extraction Brackets reduce or
eliminate the need for any primary archwire bends.
minimum Extraction Bracket has r anti-tip and
2o anti-rotation and is recommended for teeth
are shown of the Standard and three Extraction
Brackets for an upper cuspid.
requiring up to 2 mm of translation. Minimum
Extraction Brackets are also recommended for a
tooth bordering on an extraction site but not itself
translated, to mate it better with the tooth that was
translated. A medium Extraction Bracket, with 3 o
anti-tip and 4 o anti-rotation, is recommended for
teeth to be translated 2-4 mm. Maximum Extraction Brackets, with 4° anti-tip and 6° antirotation, are recommended for use on teeth to be
translated more than 4 mm. In Figure 14 examples
Anti-torque is a unique feature of upper molar
Extraction Brackets. Upper molars are the only
three rooted teeth and they require special consideration when they are moved mesially. Their
dominant lingual root causes their buccal surfaces
to rotate not only mesially (which is resolved by the
anti-rotation feature of the bracket), but also to
rotate gingivally. This gingival rotation intrudes
Anti-torque
139
L. F. Andrews
Series
TABLE 1
Straight-Wire Appliance brackets: cuspid through
2nd molar
Upper
Lower
Tip
Tip
Rotation
E-1
E-2
E-3
so
70
so
go
oo
20
40
so
1st bicuspid (dlstal movement)
20
oo
5
5
40
20
E-1*
E-1*
so
40
E-2
E-2
so
so
E-a•
E-3*
20
40
so
so
oo
20
40
so
2nd bicuspid (mesial movement)
20
oo
5
5
oo
20
E-1
E-1
40
-10
E-2
E-2
so
-20
E-3*
E-3
20
oo
-10
-20
oo
20
40
so
1st and 2nd molar (mesial movement)
so
20
5
10°
5
go
oo
E-1
E-1t
12°
20
-10
E-2
E-2t
14°
10
E-g* -20
E-3*t
1S0
oo
oo
E-4 Class 11
oo
20
40
so
Rotation
Cuspid (distal movement)
oo
5
11°
20
E-1*
13°
40
E-2
14°
so
E-3
1S0
5
*Scheduled to be available mld-1979.
t Contain anti-torque.
Standard Bracket= S, minimum Extraction Bracket= E-1, medium
Extraction Bracket= E-2, maximum Extraction Bracket= E-3.
the buccal cusps and extrudes the lingual cusps,
resulting in potential lateral excursion interferences.
In the upper molar Extraction Bracket, the antitorque feature not only discourages extrusion of the
lingual cusps during translation but intrudes them
at the conclusion of treatment as a form of overtreatment.
The amount of anti-torque for the minimum
Extraction Bracket is 4° (4+9= 13 total degrees),
5° for the medium (5+9= 14°), and 6° for the
maximum (6+9= 15°).
Class II molar brackets
Class II molar brackets (E-4 in Table I) are for
upper molars that are to be treated to a Class II
position. An upper bicuspid only extraction case or
congenitally missing upper laterals would be examples of this situation. In this position, the long
axis of the upper molar crowns should be upright
and no distal buccal offset is needed. Class II molar
brackets meet this need with 9° torque but no tip
and no molar offset.
140
Extraction Brackets are arranged into groups called
Series. Each Extraction Bracket Series has been
specially designed to treat one of the nine most
frequently encountered malocclusions that require
extraction.
Incisor Bracket Sets
The amount of incisor bracket torque needed can
vary from patient to patient depending on skeletal
differences and treatment mechanics. Treatment
planning includes a prediction of post-treatment
skeletal relationship and desired incisor inclination.
Accordingly, individual incisor brackets of various
torque are available. These brackets are also
available in pre-arranged sets A, S, and C for the
three most common skeletal variations. Set A is
recommended for Class II skeletal tendency. Set S
(Standard) is recommended for Class I skeletal
relationships. Set C is recommended for Class Ill
skeletal tendencies (Table 2). All sets have standard
amounts of tip.
TABLE 2
Incisor bracket sets*
Set A 1
Upper torque
Lower torque
-20
40
20
40
20
40
-20
40
Set S (Standard)2
go
Upper torque
-10
Lower torque
70
-10
70
-10
go
-10
Set C 3
Upper torque
Lower torque
12°
-so
12°
-so
so
-so
so
-so
* All sets have standard amounts of tip.
' Recommended for Class 11 skeletal tendencies.
• Recommended for Class I skeletal relationships.
'Recommended for Class Ill skeletal tendencies.
Misconceptions and Myths
Some doctors have misinterpreted the r tip in the
lower SWA Standard brackets for lower molars to
mean that the crowns will end up being r mesially
inclined. The SWA will not produce that effect if
properly used. The key here is proper bracket
placement. SWA brackets are designed for parallel·
ing of their vertical components with the long axis
of the clinical crown.
For example, the long axis of the lower molar
crown is the dominant groove on the buccal surface.
This axis forms an angle of 2° with a line perpen-
The Straight-Wire Appliance
dicular to the occlusal plane of that tooth. When
the Straight-Wire molar brackets are properly
located, the 2° tip in the bracket offsets the 2° distal
tip of the crown's long axis. So the molar, at the
conclusion of treatment, will be as upright as with a
zero-angulation edgewise bracket that uses the
occlusal surface or marginal ridges of the crown as
a reference point.
Flexibility
Another misconception is that the SWA is wedded
to a specific technique. Immediately prior to the
1976 AAO meeting in New York, a symposium of
seven orthodontists presented a two-day course
entitled, 'The Straight-Wire Appliance: Seven
Perspectives.' The speakers were Drs Richard Litt,
Bonham Magness, Melvin Mayerson, Ronald
Roth, Wayne Watson, Don Woodside and myself.
No two of the group presented the same approach.
Their individual focuses related the SWA to direct
bonding, Tweed mechanics, group practice advantages, utility arches, sectional arch mechanics, and
activator treatment for gross correction followed
by SWA treatment for finished mechanics. I think
this panel demonstrated once and for all that the
Straight-Wire concept and the use of the enabling
technology (the SWA) are coherent and integrated
but flexible, receptive and compatible with a
remarkable range of individual clinical techniques.
Wire bending
This matter requires reviewing because there is a
common inference that no wire-bending at all is
ever necessary with the SWA. I grant that the name
'Straight-Wire Appliance' may imply that, and for
the most part it is true, provided the full range of
brackets (Standard and Extraction) is used appropriately. When that is done, first, second and
third order bends are seldom necessary. Second
order bends (to promote bodily movement), are
required, however, if only SWA Standard brackets
are used in extraction cases.
Bracket placement
It is not justified to infer that in order for the SWA
to work properly, it must be sited on the crown
With more precision than an orthodontist can
routinely achieve. Anything new in clinical procedure meets dogged resistance. To some, the
Unfamiliar seems likely to be difficult. True,
bracket-siting with the SWA involves two innovations; together, they constitute a bracket placement technique. The new technique is scientifically
sounder than older methods, in terms of achieving
accuracy. Moreover, it is easier rather than more
difficult. Why? Because orthodontists find it easier
to place one straight line parallel to another than
to angulate a bracket at an estimated angle. They
find it equally easy to select the midpoint of a short
linear distance.
The Straight-Wire Appliance carries its own
placement guidelines. They are the vertical tiewings; or, for molars, tie-wings or the mesial or
distal vertical portion of the main body of the
bracket, or of the molar tube. The bracketing
technique is just a matter of placing the straight,
vertical guidelines parallel to the long axis of the
clinical crown (the LACC), and then moving the
bracket up and down until its base point and slot
point are at the same height as the LA-point. Those
two steps amount to two judgments - one of
parallelism, one of midpoint. Having used edgewise for years when I began private practice, I can
confidently say that the SWA is easier to place
accurately; that when properly placed it produces
more consistent end results; and that if equal
amounts of siting error are introduced in a test
against edgewise, the SWA will in fact prove to be
more forgiving.
An Experiment
Let us test the accuracy of paralleling and finding a
midpoint as compared with estimating ('eyeballing') given angles. Suppose we hypothesize that
to satisfy gnathology's demanding standards
orthodontically, we must work within error limits
of only 2o in tip and r in torque, and 0·5 mm
vertically.
At one of my courses, I conducted an experiment
involving 54 orthodontists from a dozen or more
states. They represented various levels of experience
and included users of several different appliances.
Equipped with paper, pencil and straight-edges,
each participant was asked to draw two parallel
vertical lines about a half-inch long. Erasing was
permitted, but no measuring; this was a test of
ability to estimate parallelism. Next, they drew
four vertical straight lines, to which they added
lines to create estimated 2°, 5°, 9° and 11 o angles.
Finally, they drew an additional vertical line
approximately a half-inch long and marked its
estimated midpoint. Subsequently, each participant's results were measured with calipers, protractors and Boley gauges.
The findings showed great accuracy in placing
one line parallel to another, and in judging the
midpoint. In paralleling, the average error was
141
L. F. Andrews
0·194 °, and 92 per cent of the individual results
were within the acceptable range. Only four
exceeded the 2° 'tolerable' error and only one of
these four erred by as much as one additional
degree. In selecting the midpoint of a line approximately the length of a clinical crown, 91 per cent
of the participants missed dead centre by less than
0·5 mm. The average error was 0·165 mm. Only one
error exceeded I mm.
But what of the angle estimations, representing
the old method - angulating a bracket on a tooth
or band when tip is not built into the appliance?
Here are the results:
The estimated 2° angles ranged from 1·5° to 12°.
The average was 4°. Exactly one-third of the efforts
fell outside the allowable error range. The estimated
5° angles ranged from 5° to 18° and averaged 8°.
Outside the r permissible range: 46·3 per cent.
The 9° attempts varied from 6° to 34°, averaged
130, and 61 per cent erred by more than 2°. When
shooting at 11 o the doctors produced angles as
and as large as 26°. The average was
small as
15°. Nearly three of every four (74 per cent)
exceeded the tolerable r error. What those test
results add up to, obviously, is this: orthodontists
can place a Straight-Wire bracket, with its parallel
features, more accurately on the crown's long axis
and at its midpoint, than they can angulate a
bracket on a tooth or angulate a bracket on a band.
The midpoint and paralleling errors were well
within the 2° leeway specified by our hypothesis.
It is in estimating angles that inaccuracy surges to
unacceptable levels; and the SWA has its angulations already built in - both tip and torque. The
advantages will become evident to any doctor who,
in his own office, gives himself a similar set of tests.
r
What it is All About
I do not claim exemplary clinical achievements; the
quality of my end results may approach, but does
not equal, Nature's in her nonorthodontic normals.
The reader may be a more skilful technician than I,
but using the SWA, I have completed hundreds of
cases, and many more have been completed by
other orthodontists, with a gratifying rate of
success. The Straight-Wire principles are already
being evaluated or taught in many respected
orthodontic departments throughout the United
States, apd acceptance by clinical orthodontists is
growing at a remarkable rate. Progress in orthodontic
practice consists in a continual reduction of error.
Some imprecision in treatment results may arise
from variations in tooth morphology, but most
142
such variations fall within the range of normalcy
and do not seriously impede our work. Most
treatment errors pertain to imprecise tooth position
treatment errors pertain to imprecise tooth
positions, and can be traced to four areas:
1. Arbitrary decisions as to proper treatment
goals;
2. Inaccurate bracketing techniques;
3. Brackets that poorly represent or reflect tooth
morphology and positions;
4. Primary wire-bending and its undesirable side
effects.
An approach or appliance that reduces any of
these errors contributes to the effectiveness of our
work. So let us check the SWA against that list:
1. The Straight-Wire Appliance is preprogrammed
with sound treatment goals founded on research
(the Six Keys). This feature frees the doctor, in
the majority of his cases, from the burden of
estimating or guessing the positions and relationships that will compose good occlusion.
2. SWA bracket-siting features are designed for
mating with dependable crown landmarks,
ensuring improved accuracy and consistency in
placement.
3. Torque in the base and compound curvature in
the base of the SWA bracket allow the bracket
and slot, on each crown, to represent accurately
the relationship of the occlusal surface or
incisal edge to the LA-point.
4. Other SWA design elements work as a team to
fulfil the proper roles of an appliance. With tip,
torque and in/out alignment built into the
appliance, manual manipulation of the archwire
is greatly reduced, proportionately reducing
undesirable side effects.
Conclusion
The SWA is programmed to deliver treatment to
optimum end results with few if any archwire
bends. This is possible, basically, because of the
commonality of dental morphology in our species.
The SWA Standard brackets have been adequate
for some 50 per cent of my total patient load. SWA
Extraction Bracket Series will treat another 40
per cent with few if any archwire bends. Customizing the selection of individual Extraction Brackets
will encompass still others satisfactorily.
The Straight-Wire Appliance is not perfect. No
appliance can ever terminate the need for the
wisdom, experience and perspective of the doctor.
But I believe the SWA reduces the total error
The Straight-Wire Appliance
potential, leaving the orthodontist newly liberated
from delegable chores and thus free to focus on his
truly professional responsibilities in serving each
of his patients.
References
Andrews, L. F. (1972)
The six keys to normal occlusion,
American Journal of Orthodontics, 62, 296-309.
Andrews, L. F. (1975)
The Straight-Wire Appliance: Syllabus of Philosophy and
Techniques. Rev. ed.,
San Diego, California: Lawrence F. Andrews.
Bolton, W. A. (1958)
.
Disharmony in tooth size and its relation to the analysts
and treatment of malocclusion,
Angle Orthodontist, 28, 113-130.
Dewel, B. F. (1949)
Clinical observations on the axial inclination of teeth,
American Journal of Orthodontics, 35, 98-115.
Graber, T. M. (1972)
Orthodontics Principles and Practice, ed. 3, p. 180,
Philadelphia, Pennsylvania:
W. B. Saunders Company.
Plets, J. H., Isaacson, R. J., Speidel, T. M. and
Worms, F. W. (1974)
Maxillary central incisor root length in orthodontically
treated and untreated patients,
Angle Orthodontist, 44, 43-47.
Ramfjord, S. P. and Ash, M. M. Jr. (1966)
Occlusion, p. 90,
Philadelphia, Pennsylvania: W. B. Saunders Company.
Roth, R. H. (1975)
Personal Communication.
Roth, R. H. (1976)
Five-year clinical evaluation of the Andrews Straight-Wire
Appliance,
Journal of Clinical Orthodontics, 10, 836-850.
Thurow, R. C. (1970)
Atlas of Orthodontic Principles, p. Ill,
St Louis, Missouri: The C. V. Mosby Company.
Wheeler, R. C. (1965)
A Textbook of Dental Anatomy and Physiology, ed. 4, p. 381,
Philadelphia, Pennsylvania: W. B. Saunders Company.
143