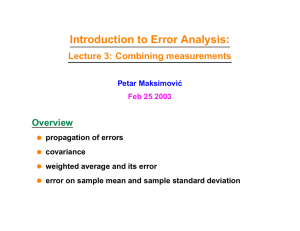
Lycopenes and related compounds G. Tang, Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University, Boston, MA, USA Published by Elsevier Ltd. This is a reproduction of G. Tang, Lycopenes and Related Compounds, Editor(s): Benjamin Caballero, Encyclopedia of Human Nutrition (Third Edition), Academic Press, 2013, Pages 124–130, ISBN 9780123848857, https://doi.org/10.1016/B978-0-12-375083-9.00176-8. Introduction Chemical and Physical Properties of Lycopene; its Food Sources and Enteric Absorption Tissue Contents and Kinetics of Lycopene Turnover Functional Properties and Tissue Health Health, Research Models, and Epidemiological Evidence Evidence for Possible Anticancer Protection by Lycopene Lycopene and Cardiovascular Disease Other Disease-Related Investigations Conclusions Further Reading 438 438 441 442 442 443 443 444 444 444 Introduction Lycopene, the most abundant pigment in ripe red tomatoes and in a few other fruits, is one of the major carotenoid pigments that is widely present in the diet of the human population. Figure 1 illustrates the chemical formula of selected carotenoids that occur widely both in human diets and in the noncellular fraction of human blood in most regions of the world. Carotenoids are yellow-to-red in color, with lycopene being nearer the red end of the carotenoid series. However, unlike the other carotenes and cryptoxanthins, it does not possess a beta-ionone ring structure at either end of the molecule, and this precludes it from becoming a precursor of vitamin A in humans and animals. Nevertheless, it is readily transformed from the all-trans form that is characteristic of most plants and plant foods for animals and humans, to a range of mono- and di-cis forms within the animal's body. In addition, oxidation to epoxides and hydroxylated derivatives occurs, although the control of these oxidation pathways and the nature of their products are not yet well understood or characterized. In plant tissues, where it is synthesized, lycopene is thought to help protect vulnerable photosynthetic tissues from light- and oxygen-catalyzed damage. Its role in humans and other animals, which can only obtain the pigment from their diet, is less well understood. Indeed it remains unproven that there is an essential role for lycopene in animal tissues. Nevertheless, considerable research effort is currently being undertaken to test hypotheses that are attempting to link human dietary and tissue lycopene levels to the risk of degenerative diseases, such as vascular diseases, cancers, etc., especially in older people. As discussed in more detail below, this research is being performed in a wide range of tissue culture and animal model systems and human epidemiological studies. In this article, some key aspects of the chemical and physical properties, the dietary sources, biochemical status indices, and biological significance of lycopene will be described. Chemical and Physical Properties of Lycopene; its Food Sources and Enteric Absorption Lycopene (molecule weight 536.9) is the most commonly encountered of that subgroup of the naturally occurring carotenoids that have a straight-chain poly-isoprenoid molecule without any terminal β-ionone ring structures (Figure 1). The chain length and number of conjugated double bonds determine the absorption spectrum, which peaks at 472 nm with a molar extinction coefficient, ɛ1% of 3450. It is one of the most nonpolar members of the carotenoids, and in organic solution it is also one of the most easily oxidized and thus is easily destroyed, which necessitates the use of rigorous precautions against its oxidative destruction during its extraction and analysis from plants, foods, animal tissues, and body fluids. Currently, such analytical determination is usually based on high-performance liquid chromatography (HPLC), using either its characteristic light absorption property, or its natural fluorescence, or its redox character, for detection and quantitation by absorbance or fluorometric or electrochemical detection. The lycopene content of selected commonly consumed foods is listed in Table 1. The original information can be found in the US Department of Agriculture (USDA) ARS recent publication (2010), Nutrition Data Laboratory Home Page. It is interesting to find out that in south Asia, the fruit Gac (Momordica cochinchinensis) contains more lycopene, almost three-fold more, than does the tomato fruit. Another characteristic that greatly affects lycopene stability and the problems of its storage and analysis is the phenomenon of cis–trans isomerization. Naturally occurring lycopene in tomatoes, the major human food source of this carotenoid, is nearly 100% all-trans (Figure 1), but during the processing of food, and then during the processes of absorption and accumulation in animal tissues, there is a progressive increase in the proportion of a variety of cis-forms. Most of these cis-forms contain 438 Encyclopedia of Human Nutrition, 4th edition, Volume 2 https://doi.org/10.1016/B978-0-12-821848-8.10197-0 Lycopenes and related compounds 439 All-trans lycopene 5-cis lycopene All-trans -carotene All-trans -carotene OH HO Lutein Figure 1 Structures of lycopene and certain other carotenoids found in human blood and tissues. a single cis-bond (mono-cis-lycopene), and the 5-, 9-, 13-, and 15- mono-cis-lycopenes account for more than 50% of the total lycopene in human serum. Smaller quantities of di-cis-lycopenes are normally also present. Curiously, another food source of lycopene, red palm oil, has a much higher natural proportion of the cis-forms of the pigment. Isomerization is catalyzed by low pH; therefore, 440 Lycopenes and related compounds stomach acid is believed to be a major factor in the conversion of the all-trans-lycopene ingested from tomatoes and their products to a mixture of cis-forms in the digestive tract. There is also evidence that further isomerization occurs between the digestive tract and the portal lymphatic lipid micelles. The cis-isomers differ from the all-trans form in their absorption and inter tissue transportation properties, and also in their functional characteristics; for instance, they are more soluble in lipophilic solvents and structures are less likely to aggregate into crystalline forms. More research data suggested that the greater bioaccessibility of cis-forms compared with all-trans form of lycopene was the reason for higher proportion of the cis form in tissues. A recent report showed that cholesterol membrane transporter SR-B1 was involved in lycopene intestinal absorption. However, lycopene and its various forms in association of physicochemical differences and their related biological consequences have yet to be adequately explored. Of all the most common naturally occurring carotenoids, lycopene is by far the most efficient in reacting with and quenching singlet oxygen, 1O2, which is a non-free-radical excited and reactive form of oxygen. This form of oxygen reacts rapidly with lycopene to yield nonexcited triplet oxygen and excited triplet lycopene. The latter then dissipates its extra energy by solvent interactions, thus regenerating nonexcited lycopene and preserving its original structure by recycling. However, another of its chemical interactions with molecular oxygen appears to result in irreversible oxidation to yield one or more cyclic epoxides, which then probably undergo ring-opening. Nevertheless, there are many unresolved questions about the nature and importance of the many degradation pathways that are believed to result in the irreversible destruction of lycopene both in vitro and in vivo. As a food component, consumption of lycopene in tomato is well tolerated and generally safe. The possible side effect of high consumption of tomato products would be mild digestive upset. Lycopene from tomatoes is permitted as a food color. Lycopene is an essential intermediate in the pathway for synthesis of the β-ionone ring-containing carotenoids such as β-carotene in plant tissues, and in most plant tissues it is present in only minor amounts. However, in a few, including tomato fruit, watermelon, and red grapefruit, this conversion to the β-ionone ring products by the enzyme lycopene cyclase is hindered, so that the intermediate carotenoid forms, lycopene, phytoene, and phytofluene, accumulate instead. Table 1 Lycopene (mg) content of selected foods, sorted by nutrient content collected from the USDA Nutrient Database for Standard Reference, Release 23 Food description Lycopene content (mg per 100 g) Tomatoes, sun-dried 45.9 Tomato products, canned, paste, without salt added 14–28.8 Sauce, pasta, spaghetti/marinara, barbecue, ready-to- 4.4–12.7 serve Catsup (Ketchup) 16.7 Sauce, salsa, ready-to-serve 10.5 Vegetable juice cocktail, canned 9.7 Tomato juice, canned, with salt added 9.0 Pasta with meatballs in tomato sauce, canned entree 7.2 Soup, minestrone, canned, reduced sodium, ready-to- 4.1–6.4 serve or tomatoes, canned, stewed, prepared with equal volume water Watermelon, raw 4.5 Tomatoes, red, ripe, canned, stewed 4.1 Spaghetti with meat sauce, frozen entree 3.2 Soup, clam chowder, manhattan, canned, prepared with 2.9–4.3 equal volume water with bean, pork, beef noodle or chunky vegetable, etc. Papayas, raw 1.8 Tomatoes, red, ripe, raw, year round average 2.6 Pizza, pepperoni, cheese, meat and vegetable topping, 1.8–2.0 regular crust Grapefruit, raw, pink and red, all areas 1.4 Fast foods, cheeseburger; single, regular patty, with 1.0 condiments Fast foods, hamburger; single, regular patty; with condiments Beans, baked, canned, with franks 0.4 Salad dressing, Russian dressing, Thousand Island 0.6–3.6 dressing, French dressing, reduced fat, etc. Source: http://www.ars.usda.gov/ba/bhnrc/ndl Lycopenes and related compounds 441 In the US, tomato products provide more than 85% of the total quantity of lycopene consumed by the human population. Mean lycopene intakes in the US are considerably greater than they are in the UK, where the mean daily intake is thought to be less than one-third that in the US, while lycopene intakes in Far Eastern countries such as China and Thailand appear to be much lower still. Wild tomatoes originated in Central America and were introduced into Europe following the opening up of the New World, and were later introduced back into North America from Europe. Because tomatoes are the major source of dietary lycopene in many human populations, some epidemiological studies have been designed on the simplistic assumption that tomato consumption can be used as a general proxy for lycopene consumption, and that any disease associations with tomato consumption can be attributed to the biological effects of lycopene. However, tomatoes also contain significant amounts of other carotenoids, vitamin C, bioflavonoids such as naringenin, and phenolic acids such as chlorogenic acid. Much of the existing epidemiological evidence for possible beneficial effects of lycopene (see the following sections.) cannot distinguish unequivocally between the biological effects of lycopene and those of the many other bioactive constituents present in tomatoes. The bioavailability of lycopene from raw tomatoes is low, but it is greatly increased by cooking or by commercial processing such as conversion to soup, sauce, ketchup (catsup), etc., and its availability is also increased by increasing the fat content of the food. A survey conducted by National Health and Nutrition Examination Survey (NHANES) in years 2007–2008 on “what we eat in America”, showed that the average intake of lycopene from food was 5.5 mg per day per person, see Table 2. More information can be obtained from the USDAs web page. Bioavailability of synthetic lycopene in an oil capsule was reported as better than from cooked and pureed tomatoes when taken by human subjects. Interactions with other carotenoids are complex and have only partly been studied, for instance β-carotene in the same dish seems to increase the absorption of lycopene, but large doses of β-carotene given separately seem to decrease the lycopene content in serum. The strength of the correlation between dietary lycopene intake and blood (serum or plasma) lycopene concentration varies greatly among studies and clearly depends on many factors, one of which is the degree of sophistication of the food table values, since subtle differences in food sources and meal composition affect its bioavailability very considerably. Tissue Contents and Kinetics of Lycopene Turnover Once absorbed, passively from lipid micelles by the enterocyte, lycopene enters the portal lymphatics and thence the liver, from which it enters the peripheral bloodstream, mainly in association with the β-lipoproteins, in which it is transported to the peripheral tissues. Its half-life in plasma is of the order of 12–33 days; longer than that of β-carotene, which is less than 12 days. Clearly, many of these factors are interdependent, and there is a need for further clarification of the key independent determinants of lycopene status, and whether plasma levels can provide an adequate picture of tissue and whole body status. Patients with alcoholic cirrhosis of the liver have greatly reduced hepatic lycopene concentrations; indeed, hepatic lycopene seems to offer a sensitive index of hepatic health. Studies of organ concentrations (Table 3), suggest a gradient from circulating levels in plasma to different ones in specific tissues. The different carotenoid ratios between organs (not shown) also indicate selective transport and accumulation. However, the mechanisms involved are poorly understood. No lycopene is detectable in the retina or lens of the eye, where lutein and zeaxanthin are found; however, lycopene is present in the ciliary body. Table 2 Daily lycopene intake from food consumed by the US population – mean amount consumed per individual and percentages of lycopene consumed with meals and snacks by age and gender Gender and age Lycopene (SE) mg Percentage of lycopene intake in meals and snacks Males ≥20 years Sample size, n=2662 6.8 (0.3) Breakfast, 7 Lunch, 31 Dinner, 51 Snacks, 11 Females ≥20 years Sample size, n=2758 4.6 (0.3) Breakfast, 4 Lunch, 27 Dinner, 57 Snacks, 13 Males and females ≥2 years Sample size, n=8529 5.5 (0.2) Breakfast, 5 Lunch, 30 Dinner, 53 Snacks, 12 Abbreviation: SE, standard error. Source: http://www.ars.usda.gov/services/docs.htm?docid=18349. 442 Lycopenes and related compounds Table 3 Concentrations of lycopene reported in human tissues Tissue Range of mean or median (in Italics) lycopene concentrations (nmol per g weight) Adrenal Testis Liver Brain Lung Kidney Stomach, colon Breast, cervix Skin Adipose tissue Prostate Plasma 1.9–21.6 4.3–21.4 0.6–5.7 2.5 0.2–0.6 0.1–0.6 0.2–0.3 0.2–0.8 0.4 0.2–1.3 0.1–0.6 0.2–1.1 Note: Values were gathered from 12 publications, all based on HPLC analysis. Functional Properties and Tissue Health The capacity for quenching of singlet oxygen has been mentioned above; the exceptionally high rate constant, K=3.1×1010 mol−1 s−1, renders it one of the most efficient of known quenchers of this powerful oxidant. In the plant, it probably protects chlorophyll, which produces singlet oxygen as a by-product of photosynthesis. In experiments with lymphoid cells, lycopene provided better protection against singlet oxygen damage than several other carotenoids tested. In skin exposed to UV light, lycopene disappears much more rapidly than β-carotene. Lycopene is also able, in model systems, to inhibit the peroxidation of polyunsaturated lipids and the oxidation of DNA bases to products such as 8-hydroxydeoxyguanosine (8-OHdG). It can react directly with hydrogen peroxide and nitrogen dioxide. In addition, lycopene supplementation may modify DNA through DNA repair mechanisms. Several studies in tissue culture have shown a reduction in the formation of oxidation damage products such as malondialdehyde, and have found less injury to cells exposed to oxidants such as carbon tetrachloride, if lycopene (or other carotenoids) is present. Another characteristic of lycopene and other carotenoids that may be relevant to inhibition of cancer cell growth is the modulation of gap junction cell–cell communication processes. In particular, carotenoids including lycopene have been shown to enhance the efficacy of the protein, connexin43, which helps to ensure the maintenance of the differentiated state of cells and to reduce the probability of unregulated cell division, which is deficient in many tumors. They may also interact with and enhance the synthesis of binding proteins that down-regulate the receptor for the growth-promoting hormone insulin-like growth factor1 (IGF-1). In one small clinical intervention with tomato drinks, it was reported that changes in circulating lycopene were inversely and significantly correlated with those of IGF-1. In certain circumstances, lycopene can reduce low-density lipoprotein (LDL) -cholesterol levels, possibly by inhibiting hydroxymethylglutaryl CoA reductase (HMGCoA reductase), the rate-limiting enzyme for cholesterol synthesis (see the Section on Lycopene and Cardiovascular Disease). Lycopene was shown to have modest hypocholesterolemic properties in one small clinical trial. Lycopene has shown significant antimigration and anti-invasion activity in association of its induction of nm23-H1 expression, a metastasis suppressor gene. Health, Research Models, and Epidemiological Evidence Table 4 summarizes the various types of evidence that have been used to test the hypothesis that lycopene may have healthpromoting or protective properties in man. The ultimate proof of efficacy, which would be long-term controlled intervention studies with clinical diseases or mortality as the end points, are extremely difficult, expensive, and time-consuming to obtain, and cannot address all possible benefits in a single intervention trial. The two disease categories that have so far received most attention for possible long-term benefits of lycopene have been the amelioration of cancers and of heart disease. Both benefits are plausible in view of the physicochemical and biological properties of lycopene outlined above, because both categories of disease are characterized by tissue damage, which is thought to be induced or exacerbated by reactive oxygen species in the environment or those generated within the body. Lycopenes and related compounds Table 4 443 Types of evidence being sought to show that a nutrient such as lycopene may protect against oxidation-induced or other disease processes 1. Model in vitro systems, for example, oxygen-derived free-radical trapping in cell free chemical mixtures. 2. Tissue (cell and organ) cultures, for example, reduction of optical opacity development in cultured eye lenses; reduced growth rates or apoptosis in tumor cell cultures; and protection of key macromolecules, especially nucleic acids. 3. Animal studies demonstrating a reduction of oxidation-induced damage or disease with lycopene supplements or with lycopene-rich foods such as tomatoes or tomato products. 4. Human observation studies using intermediate biochemical markers: for example, inverse relationships between lycopene intakes or blood levels and biochemical markers, such as lipid or DNA oxidation products. 5. Studies using pathology-related intermediate markers, for example, arterial thickening or reduced arterial elasticity; precancerous polyposis, etc. 6. Relationships (without intervention) between tomato intakes or estimated lycopene intakes or lycopene contents of serum, plasma, or tissues (e.g., fat biopsies) and actual disease prevalence or incidence in human cross-sectional, case–control, or prospective epidemiological studies. 7. Intervention studies: lycopene supplements producing a reduction in biochemical markers of oxidation damage or in functional markers, or, eventually, in actual human disease incidence or progression. Evidence for Possible Anticancer Protection by Lycopene Most of the indications with respect to cancer come from human studies linking tomato intake, total estimated lycopene intake, and serum or plasma lycopene concentrations to the subsequent development of cancers (Table 5). There is a small amount of evidence from experimental animal studies, for instance, rat and mouse dimethylbenzanthracene-induced mammary tumor studies have supported the hypothesis, as has a model of spontaneous mammary tumor formation in one strain of mice, but many of the animal models of tumor promotion have been criticized as being too dissimilar from the likely processes of spontaneous tumor genesis in humans. Partly for historical reasons, there has been a particular interest in prostate cancer (Table 5). A large and early trial in the US (US Health Professionals Follow-up Study) reported an impressive difference between groups with high and low intakes of tomatoes and hence of lycopene for subsequent prostate cancer development, which was not shared with other carotenoids. Plausibility was enhanced by the fact that although human prostate lycopene concentrations are not especially high on an absolute basis (Table 3), they are higher than those of other carotenoids in this tissue. Subsequent studies have had variable outcomes. A small pilot study reported that tomato oleoresin supplements given for a short period to prostate cancer sufferers who were due for radical prostatectomy resulted in smaller tumor size and other apparent benefits, but this trial now needs to be repeated on a larger scale. Although lycopene has shown protective effects against prostate cancer and inhibits the progression in patients with benign prostate hyperplasia, there is insufficient evidence to recommend the use of lycopene supplements for cancer patients. Several studies have provided evidence for protection of certain regions of the digestive tract against tumor occurrence or growth. Two studies, one in Iran and another in Italy, found an inverse relationship between esophageal cancer and tomato consumption. Two Italian and one Japanese studies reported evidence for protection against gastric cancer, and two studies claimed a reduction in pancreatic cancer. A case–control study on histologically confirmed pancreatic cancer cases and population-based controls in eight Canadian provinces reported that dietary intake of lycopene, provided mainly by tomatoes, was associated with 31% reduction in pancreatic cancer risk among men when comparing the highest and lowest quartiles of intake. Results with other cancers have been mixed and inconclusive. Lycopene and Cardiovascular Disease Table 6 summarizes the evidence. The European Multicentre Euramic Study reported that risk of developing myocardial infarct was inversely related to lycopene intake, after appropriate adjustment for other cardiovascular risk factors. Some Scandinavian studies Table 5 Summary of evidence for association of dietary intake of tomato, or serum or plasma concentrations of lycopene, with possible protection against prostate cancer Number of studies Locations Total number of participants 2 Greece, Canada 937 7 3 USA, UK, Canada, New 3824 Zealand USA 954 1 3 Netherlands USA 723 Note: Significant association=p<.05 and NS=no significance (p>.05). Types of trial Outcome conclusion Case–control (intake of tomato or lycopene, Significant association or blood level) As above NS Prospective studies based on dietary estimates As above Prospective studies based on serum or plasma lycopene Significant association NS Inconclusive; one study found a marginal (p=.05) benefit versus aggressive cancer 444 Table 6 Lycopenes and related compounds Summary of evidence for association of relatively high serum or plasma lycopene with reduced risks of cardiovascular disease (CVD) Study Location Sex (total participants) Types of trial and outcome measures Outcome conclusion Euramic M (1379) C-C, MI Significant association with protectiona M+F (462) M+F (369) M+F (216) M+F (392) M (210) Kuopio (KHID) Europe, multicenter USA USA Netherlands Italy Sweden and Lithuania Finland Kuopio (ASP) Finland M+F (520) Physicians’ Health Study Women's Health Study USA C-C, IMT NS NC-C, MI in smokers NS C-C, PC Significant association with protection CS+PFU, PC NS CS, mortality from heart NS disease PFU, acute coronary event or Significant association with protection stroke IMT Significant protection for males; not significant for Females C-C, CVD NS M (case 499+matched free CVD,499) F (case 483+matched free CVD C-C, CVD 483) ARIC Street Rotterdam Bruneck Linkoping–Vinus USA M (725) Significant association with protection Abbreviations: C-C, case–control study; NC-C, nested case–control study; CS, cross-sectional study; PFU, prospective follow-up study; MI, myocardial infarct; IMT, intima-media thickness estimate; PC, plaque count; NS, no significant evidence for protection. Note: Significant association with protection is p<.05, generally after appropriate adjustment for other known CVD risk factors. a No association with plasma b-carotene in this study. have subsequently supported this claim; moreover, lycopene is capable of reducing LDL-cholesterol levels, possibly by inhibiting hydroxymethylglutaryl CoA reductase (HMGCoA reductase), the rate-limiting enzyme for cholesterol synthesis. Other Disease-Related Investigations In an organ culture model, some evidence for protection of rat lenses against induction of cataractogenesis has been reported. There is good reason to believe that carotenoids in general may play a role in the protection of ocular tissues against the damaging effects of UV light and of reactive oxygen substances, whose exposure to light carries some analogy with the known functions of carotenoids in plant tissues. A possible protective role in the ciliary body and iris has been proposed, but not yet tested. Conclusions Clearly lycopene possesses chemical and biological properties which make it a very attractive candidate for tissue protection and reduction of disease, especially degenerative diseases. Lycopene probably interacts more efficiently with one particular reactive oxygen species, singlet oxygen, than any other commonly occurring nutrient. It appears to share with several other carotenoids the capacity to reduce lipid peroxidation and DNA oxidative damage, and to enhance cell–cell gap junction communication and to protect normal IGF-1 function. It may reduce cholesterol formation and its tissue accumulation in some circumstances. Studies related to cancers and cardiovascular disease are ongoing and are attracting increased research interest. Further Reading Basu, A, Imrhan, V., 2007. Tomatoes versus lycopene in oxidative stress and carcinogenesis: Conclusions from Clinical trials. European Journal of Clinical Nutrition 61, 295–303. Britton, G, 1995. Structure and properties of carotenoids in relation to function. The FASEB Journal 9, 1551–1558. Clinton, SK, 1998. Lycopene: Chemistry, biology, and implications for human health and disease. Nutrition Reviews 56, 35–51. Haseen, F, Cantwell, MM, O'Sullivan, JM, Murray, LJ., 2009. Is there a benefit from lycopene supplementation in men with prostate cancer? A systematic review. Prostate Cancer and Prostatic Disease 12, 325–332. International Symposium on the Role of Tomato Products and Carotenoids in Disease Prevention, 2002. 14 review articles by different authors, plus 17 symposium abstracts. Experimental Biology and Medicine 227, 843–937. Kavanaugh, CJ, Trumbo, PR, Ellwood, KC, 2007. The U.S. Food and Drug Administration's evidence-based review for qualified health claims: Tomatoes, lycopene, and cancer. Journal of the National Cancer Institute 99, 1074–1085. Mossine, VV, Chopra, P, Mawwhinney, TP., 2008. Interaction of tomato lycopene and ketosamine against rat prostate tumorigenesis. Cancer Research 68 (11), 4384–4391. Nguyen, ML, Schwartz, SJ, 1999. Lycopene: Chemical and biological properties. Food Technology 53, 38–45. Rao, AV, Agarwal, S, 1999. Role of lycopene as antioxidant carotenoid in the prevention of chronic diseases: A review. Nutrition Research 19, 305–323. Weisburger, J, 1998. International symposium on lycopene and tomato products in disease prevention. Proceedings of the Society for Experimental Biology and Medicine 218, 93–143.