E BOOK Design and Analysis of Pragmatic Trials Chapman & HallCRC Biostatistics Series 1st Edition by Song Zhang , Chul Ahn , Hong Zhu
advertisement

Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Contents
1 Pragmatic Randomized Trials......................................................................1
1.1 Introduction .............................................................................................1
1.2 Cluster Randomized Designs ...............................................................6
References ....................................................................................................... 23
2 Cluster Randomized Trials......................................................................... 31
2.1 Introduction ........................................................................................... 31
2.2 Continuous Outcomes.......................................................................... 32
2.3 Binary Outcomes...................................................................................43
2.4 Count Outcomes.................................................................................... 52
2.5 Cluster Size Determination for a Fixed Number of Clusters ......... 59
References ....................................................................................................... 61
3 Matched-Pair Cluster Randomized Design for Pragmatic Studies ....... 65
3.1 Introduction of Matched-Pair Cluster Randomized Design ..........65
3.2 Considerations for Pragmatic Matched-Pair CRTs........................... 67
3.3 Matched-Pair Cluster Randomized Design with Missing
Continuous Outcomes.......................................................................... 68
3.4 Matched-Pair Cluster Randomized Design with Missing
Binary Outcomes...................................................................................80
3.5 Further Readings................................................................................... 88
Appendix......................................................................................................... 91
References ....................................................................................................... 93
4 Stratifed Cluster Randomized Design for Pragmatic Studies ........... 97
4.1 Introduction of Stratifed Cluster Randomized Design .................. 97
4.2 Considerations for Pragmatic Stratifed CRTs .................................. 98
4.3 Stratifed Cluster Randomized Design with Continuous
Outcomes.............................................................................................. 100
4.4 Stratifed Cluster Randomized Design with Binary Outcomes.........105
4.5 Further Readings................................................................................. 112
References ..................................................................................................... 115
5 The GEE Approach for Stepped-Wedge Trial Design ........................ 119
5.1 Introduction ......................................................................................... 119
5.2 A Brief Review of GEE........................................................................ 122
5.3 Design SW trials with a Continuous Outcome............................... 125
5.4 Design SW Trials with a Binary Outcome....................................... 142
Get all Chapters For Ebook Instant Download by email
at
v
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
vi
Contents
5.5 Longitudinal and Crossover Cluster Randomized Trials............. 148
Appendix A: Derivation of Equation (5.8) ............................................... 161
Appendix B: Derivation of Equations (5.9) and (5.10)............................ 163
Appendix C: Sample Size for Cross-Sectional SW Trials ....................... 165
Appendix D: Derivation of Equation (5.15) ............................................. 166
Appendix E: Proof of Theorem 1 ............................................................... 167
Appendix F: Proof of Theorem 2 ............................................................... 168
References ..................................................................................................... 169
6 The Mixed-Effect Model Approach and Adaptive Strategies for
Stepped-Wedge Trial Design ................................................................... 173
6.1 A Brief Review of Mixed-Effect Models .......................................... 173
6.2 Sample Size Calculation Based on Cluster-Step Means ................ 174
6.3 Adaptive Strategies for SW Trials..................................................... 185
6.4 Further Readings................................................................................. 193
References ..................................................................................................... 197
Index ..................................................................................................................... 201
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
1
Pragmatic Randomized Trials
1.1 Introduction
Clinical trials have been broadly classifed as pragmatic or explanatory
trials. Schwartz and Lellouch [1] probably frst used the terms “explanatory”
and “pragmatic” to differentiate trials. The term “explanatory” was used
for trials that test whether an intervention works under optimal situations
that control heterogeneity as much as possible to isolate the intervention
effect. The term “pragmatic” was used for trials that evaluate whether an
intervention works in real-life routine practice conditions, which makes
results widely applicable and generalizable. Explanatory trials are valuable
for understanding questions of effcacy in an ideal patient population.
Exploratory clinical trials, especially randomized clinical trials (RCTs),
are designed as experiments with the ability to determine cause–effect
relationships. They enroll highly selected subjects who may not represent
the target population. Exploratory trials follow a strict treatment protocol to
evaluate whether an intervention is effcacious and safe [2]. Findings from
explanatory trials do not appear to be directly generalizable to a real-world
clinical setting with real-world patients.
The most distinctive features of pragmatic clinical trials (PCTs) are that
they compare clinically relevant alternative interventions and include a
broadly diverse population of study participants with few eligibility criteria.
These features lead to increased feasibility and broader generalizability to
the target population. Typically, the fndings from pragmatic trials have
high generalizability. In contrast, explanatory trials are the most likely
experiments where any differences between intervention groups resulted
from scientifc testing under rigorously controlled conditions.
Pragmatic and explanatory trials are not distinct concepts since trials may
incorporate differing degrees of pragmatic and explanatory components. A
trial can be designed to have some aspects that are more pragmatic than
exploratory and vice versa. For example, a trial may have an explanatory
element with strict eligibility criteria. Still, it may have a pragmatic aspect
of a trial with minimal to no monitoring of practitioner adherence to the
study protocol and no formal follow-up visits. Overall, there is a continuum
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
2
Design and Analysis of Pragmatic Trials
between pragmatic and explanatory trials, with many trials having both
pragmatic and explanatory elements included [3].
Tools have been developed to help researchers design pragmatic trials
[3–6]. Gartlehner et al. [5] proposed a simple instrument to distinguish
pragmatic from explanatory trials. They used a binary system (yes/no) to
evaluate if the trial was pragmatic or exploratory using the seven study design
criteria, even though they acknowledged that explanatory and pragmatic
components exist in a continuum. Thorpe et al. [6] introduced the PragmaticExplanatory Continuum Indicator Summary (PRECIS) tool, which enabled
investigators to design trials with the explanatory-pragmatic continuum
in ten domains. They identifed some weaknesses, including unclear face
validity and inter-rater reliability, lack of a scoring system, redundancy
in some PRECIS domains, and the need for more guidance on using the
tool. They developed a validated tool, Pragmatic-Explanatory Continuum
Indicator Summary version 2 (PRECIS-2), by addressing the weaknesses
while keeping the strengths of the original PRECIS tool [3]. PRECIS-2 is a
nine-spoked wheel, with each spoke representing a domain that denotes a
critical element of a trial design. Nine domains of PRECIS-2 are eligibility
criteria, recruitment, setting, organization, fexibility in delivery, fexibility
in adherence, follow-up, primary outcome, and primary analysis. Each
element of the nine domains is scored on a fve-point Likert scale (from 1
denoting very explanatory “ideal conditions” to 5 indicating very pragmatic
“usual care conditions”) to facilitate domain discussion and consensus. For
interactive tools on the PRECIS-2, see https://www.precis-2.org/.
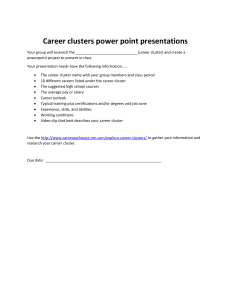
We mark each spoke to represent the location on the explanatory (hub)
to pragmatic (rim) continuum, connect the dots on a blank wheel graph in
PRECIS-2, and link each of them to their immediate neighbor, as in Figure 1.1.
Figure 1.1 shows the scores of each item in the PRECIS-2 wheel for a clinical
trial to be developed. Predominantly explanatory trials produce spoke and
wheel diagrams close to the hub, whereas pragmatic trials produce diagrams
close to the rim. A pragmatic trial is “designed to test the intervention in the
full spectrum of everyday clinical settings to maximize applicability and
generalizability” [7].
An important feature of healthcare PCTs is leveraging the available data,
such as the electronic health record (EHR) or insurance claims data, to cut
costs and personnel effort associated with traditional exploratory trials.
EHR is an appealing tool to identify, recruit, and enroll trial participants,
perform randomization, follow participants over time, and collect patientrelevant outcome data because the data does not require participants’
contact or adjudication. Assessing study outcomes via linkage with EHRs
decreases the burden on the participants and the research team [8]. EHRs
have been used to evaluate the effectiveness of various interventions in some
pragmatic trials [9–12]. In addition, pragmatic trials nested within EHRs can
help overcome the limitations of explanatory trials, including high cost, time
burden, and limited generalizability [13, 14].
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
3
FIGURE 1.1
The PRagmatic-Explanatory Continuum Indicator Summary 2 (PRECIS–2) wheel. Adapted
from BMJ2015;350:h2147.
1.1.1 Statistical Issues in Pragmatic Randomization Trials
An ideally conducted randomized clinical trial (RCT) ensures that the
observed difference in outcomes between control and intervention groups
is only attributed to the absence or presence of the intervention. Missing
data may seriously compromise the credibility of causal inferences from
PCTs. Missing data ubiquitously occur in PCTs that use electronic health
records (EHRs) or insurance claims data and may compromise the causal
inference if missing data is inappropriately handled. Missing data can happen due to various reasons, such as participants’ missing scheduled visits or
dropout from the study. PCTs may have a high proportion of missing values
since some providers may drop out of the trial or fail to collect specifc data
from all individuals at follow-up visits. The probability that individuals are
lost to follow-up or miss their follow-up appointment may depend on both
provider- and individual-level characteristics. Therefore, missing data must
be appropriately handled using valid statistical approaches in the design
and analysis of PCTs to draw valid inferences [15]. An apparent reason to
properly deal with missing outcomes is to retain the statistical power of the
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
4
Design and Analysis of Pragmatic Trials
original randomized clinical trial design. Statistical power is the probability
of detecting a meaningful effect, given that such an effect exists.
Missing data mechanisms are commonly summarized into three
categories [16]. Data are considered missing completely at random (MCAR)
if missingness is independent of the observed outcomes and covariates.
MCAR is a strong assumption and is not likely in most clinical trials. MCAR
indicates whether missing data is entirely unrelated to either observed or
unobserved data. A more sensible assumption is missing at random (MAR),
where missingness does not depend on unobserved data after conditioning
on the observed data. A likelihood-based analysis using only the observed
data can be valid under MAR if the analysis adjusts for those variables
associated with the probability of not being observed. Data are termed
missing not at random (MNAR) if missingness is dependent on unobserved
data values even after conditioning on fully observed data.
Complete case analysis may be valid if the probability of being a complete
case is independent of the outcome given the covariates in the analysis
model. However, the complete case analysis will lead to larger estimates of
standard errors due to the reduced sample size. Complete case analysis may
be unacceptably ineffcient if more than a small proportion of individuals
are omitted. Additional approaches include single imputation, multiple
imputation, and model-based methods. Single imputation approaches
replace each missing value with a single value based on the sample mean, a
regression-based prediction, the last observation carried forward (LOCF), or
other strategies. In single imputation, the imputed values will be assumed
to be the real values, as if no data were missing. Although single imputation
approaches can give unbiased estimates, standard errors are generally too
small because they do not refect uncertainty about the values of the missing
observations.
Rubin [17] proposed a procedure called multiple imputation to address
this problem. Multiple imputation allows for the uncertainty about the
missing data by generating different plausible imputed data sets, analyzing
each flled-in data set separately, and combining the analyses into a single
summary analysis with simple averaging formulas. In cluster randomized
trials (CRTs), multiple imputation approaches need to incorporate the withincluster correlation in the multi-level design to ensure valid inferences since
ignoring clustering in the multiple imputation can lead to an increase in type
I errors [18]. If clusters are included as a fxed effect in the imputation model,
imputations lead to excessive between-cluster variability, especially if cluster
sizes are small and intracluster correlation is small [19].
In traditional RCTs, potential participants are identifed, contacted, and
enrolled. They opt-in to traditional RCTs by giving informed consent.
Potential participants decide whether or not to participate in trials after
having received and understood all the research-related information.
Barriers to enrollment are often high in traditional RCTs since the trial may
require extra clinic visits, procedures, and interviews. As a result, consent
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
5
rates are often low, and only a small portion of the eligible population
eventually enrolls due to high barriers in traditional RCTs. Pragmatic clinical
trials aim to increase the proportion of the target population who eventually
enroll in the trial. Pragmatic trials increase generalizability by conducting
randomized controlled trials under routine clinical practice conditions
instead of specialized research settings [1]. A robust approach in pragmatic
trials is an opt-out consent process, in which the default is participation rather
than non-participation. In an opt-out process, the staff informs potential
study participants at their clinic visit. In an opt-out model, trial participants
are included automatically but can opt out completely or with restrictions by
allowing selected data to be used. The opt-out consent process is generally
expected to result in a more diverse sample of trial enrollees, including
many who would not enroll under the traditional opt-in consent process.
Unconsented randomized trials must be carefully restricted to contexts
where risks are very low and overseen by experienced institutional review
boards (IRBs). Pragmatic trials frequently incorporate an opt-out model for
the consent process, while traditional RCTs use opt-in consent.
Another feature of healthcare pragmatic clinical trials is a cluster randomized trial (CRT). CRTs are particularly useful for evaluating the effectiveness
of interventions at the level of health systems, practices, or hospitals [20].
Many challenges and sources of bias in PCTs are related to CRTs [21, 22].
In CRTs, treatment allocation often cannot be blinded to participants, study
staff, or providers. In addition, there may be differences in the types of participants enrolled between treatment groups because the assignment of participants to treatment groups generally cannot be concealed. In pragmatic
trials, CRTs are often the most feasible study design to avoid contamination
in real-world settings.
One example of contamination is that if a physician simultaneously
provides care to patients assigned to the intervention and control groups,
leakage of intervention information might occur between two groups,
resulting in an observed intervention effect that is diluted and biased toward
the null. A CRT is more complex to design, requires more study subjects, and
needs more complex analysis than an individualized randomized trial (IRT).
A well-recognized statistical issue in CRTs is that responses tend to be more
similar within clusters than across clusters. This within-cluster similarity is
quantifed by the intracluster correlation coeffcient (ICC). There has been
an extensive investigation into design methods for CRTs to account for
ICC properly. Furthermore, the size of the clusters generally varies among
clusters. These features present statistical challenges in designing pragmatic
cluster randomized trials [23–25].
Due to practical and fnancial constraints, CRTs typically randomize a
limited number of clusters. When there are a small number of clusters with
diverse settings and populations, simple randomization can result in study
groups that differ substantially on critical clinical variables or potential
confounders. Unbalanced intervention groups constitute a potentially severe
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
6
Design and Analysis of Pragmatic Trials
methodological problem for CRTs because an imbalance in crucial baseline
characteristics between intervention groups diminishes the case for causal
inference, which is the fundamental strength of the randomized clinical
trial [26]. Therefore, investigators planning a CRT should consider balancing
baseline characteristics.
PCTs often require more participants to achieve adequate statistical
power to detect clinically meaningful differences. Assessment of repeated
outcomes on the same individual may be necessary to examine the effect of
an intervention over time. In cluster randomized trials, the need for greater
statistical effciency may encourage the adoption of multiple-period CRTs
such as parallel arm longitudinal, crossover, and stepped wedge CRTs that
measure outcomes repeatedly in the same cluster (and the same individuals)
over time. Standard statistical methods for the analysis of IRTs may not
be appropriate. Statistical analysis must incorporate the design features of
pragmatic CRTs, such as clustering, repeated measurements, and correlations
over time.
The correlation structure in CRTs is much more complicated than that
in IRTs. For example, matched-pair CRTs and multiple-period CRTs must
incorporate complex correlation structures. Matched-pair CRTs need
to include the following correlations for the design of trials [27, 28]: the
within-cluster correlation ( r1 ), the within-matched individual (study unit)
correlation ( r2 ), and (3) the within-matched cluster correlation ( r3 ). If
matching occurs at the cluster level, the correlation structure would depend
only on r1 and r3 with r2 = r3 . Multiple-period CRTs such as longitudinal,
crossover, and stepped wedge CRTs need to incorporate within-subject or
longitudinal correlation, the conventional intracluster correlation, and crosssubject cross-period correlation [29–34]. The repeated measurements may
burden patients regarding quality of life, satisfaction, and costs. Moreover,
the proportion of missing data is usually higher due to repeated measures
over a longer duration, which cannot be ignored in the design of trials.
1.2 Cluster Randomized Designs
A cluster randomized trial (CRT) randomly assigns groups of individuals
to each intervention group rather than individuals. In an individually
randomized trial (IRT), individuals are randomized to each intervention
group, and the intervention is applied at the individual level. A cluster
randomized trial has been frequently used in health services research,
primary care, and behavioral sciences [23, 35–40].
In designing a CRT, one of the frst decisions to be made is the choice of
clusters. For example, in a cancer screening CRT [41], one needs to determine
if one will use a physician or a clinic as a cluster. If a physician shares a nurse,
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
7
Pragmatic Randomized Trials
one may not use a physician as a cluster due to possible contamination. In
a CRT, naturally occurring groups or clusters of individuals are the experimental units randomized to each intervention group. The clusters of individuals in CRTs have included families, churches, schools, work sites, clinics,
healthcare centers, and communities. CRTs help evaluate interventions when
interventions are delivered at the cluster level or when there is a risk that
IRTs will contaminate interventions between intervention groups. Cluster
randomization is often advocated to minimize treatment contamination
between intervention and control participants. For example, in a smoking
cessation trial, people in the control group might learn about experimental smoking cessation and adopt it themselves. Contamination of control
participants leads to a reduction in the point estimate of an intervention’s
effectiveness, which may lead to the rejection of an effective intervention
as ineffective because the observed effect size was neither statistically nor
clinically signifcant. In addition to minimizing potential “contamination,"
CRTs can also have practical advantages over IRTs because of ethical considerations, lower implementation costs, ease of obtaining the cooperation
of investigators, enhancement of subject compliance, or administrative convenience. The design and conduct of a CRT require special considerations.
The lack of independence among individuals in the same cluster, i.e., withincluster correlation, creates unique methodological challenges in design and
analysis. That is, observations on subjects from the same cluster are likely
more correlated than those from different clusters. The correlation within
clusters, which is quantifed by the intracluster correlation coeffcient (ICC),
r , may result in substantially reduced statistical effciency relative to trials
that randomize the same number of individuals.
In CRTs, the total variance of an observation can be divided into two components, s 2 = s B2 + s W2 , where s W2 is the within-cluster variance and s B2 is
the between-cluster variance. That is, s W2 is the variance of observations
within a cluster and s B2 is the variance of cluster-level means. The degree
of similarity or magnitude of clustering is typically measured by ICC ( r ).
ICC is defned as the proportion of the total variance in the outcome that is
attributable to variance between clusters [23, 35]. The intracluster correlation is
r=
s B2
s B2
=
s 2 s B2 + s W2
.
The reduction in effciency is a function of the variance infation due to
clustering, also known as the design effect or variance infation factor (VIF),
given by VIF = 1 + (m - 1)r , where m denotes the cluster size when cluster
sizes are equal across clusters.
Inferences are frequently done at the individual level, while randomization
is at the cluster level in CRTs. Thus, the unit of randomization may be different
from the unit of analysis. In this case, the lack of independence among
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
8
Design and Analysis of Pragmatic Trials
individuals in the same cluster presents unique methodological challenges
that affect both the design and analysis of CRTs. Suppose one ignores the
clustering effect and analyzes clustered data using standard statistical
methods developed to analyze independent observations. In that case, one
may underestimate the true p-value and infate the type I error rate of such
tests. Therefore, clustered data should be analyzed using statistical methods
that account for the dependence of observations on subjects within the same
cluster. If one fails to incorporate the study design’s clustered nature during
the study’s planning stage, one will obtain a smaller sample size estimate
and statistical power than planned. The analysis of data collected from a
CRT must also account for clustering. Analyses at the cluster level (i.e., using
summary measures for each cluster) are generally not statistically effcient.
Individual-level analysis can account for clustering using generalized
estimating equations (GEE) or generalized linear mixed models (GLMM).
These modeling techniques also allow for adjusting both cluster-level and
individual-level covariates.
CRTs are less effcient than IRTs since outcomes of subjects in the same
cluster tend to be positively correlated. In addition, it is not always feasible
to increase the sample size, even though effciency can be improved
by increasing the sample size. Thus, alternative strategies have been
proposed, such as reducing residual variance by matching, stratifcation,
balancing, including covariates, taking repeated measurements, and using
a crossover design. Turner et al. [42, 43] reviewed the design and analysis
of methodological developments in group-randomized trials. Textbooks are
available for the design and analysis of CRTs [23, 35–40].
1.2.1 Completely Randomized Cluster Trial Design
The completely randomized cluster trial design is analogous to the completely randomized individual trial design, except that clusters are randomized instead of individuals. The completely randomized cluster trial design
is the most widely understood CRT design. Clusters are randomly assigned
to intervention and control groups using simple randomization. Both the
sample size calculation and the subsequent statistical analysis must consider
the ICC induced by cluster randomization since the responses of observations within a cluster are usually correlated. Donner et al. [44] provided a
sample size estimate for the number of subjects in a completely randomized
cluster trial design, which can be obtained by multiplying a design effect
(DE) by the required number of subjects calculated under an IRT. Under
equal cluster sizes, the design effect can be computed as DE = 1 + (m - 1)r ,
where r is the ICC and m is the cluster size. Let nind be the number of subjects required for an IRT. Then, the number of subjects needed for a CRT is
n = nind × {1 + (m - 1)r } . The design effect, 1 + (m - 1)r , is usually greater than
one since r is generally positive. The design effect is also called the variance
infation factor (VIF). Let m be the average cluster size, and x represent the
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
9
coeffcient of variation of the cluster sizes. For the unequal cluster sizes, the
DE can be approximated by DE = 1 + [(x 2 + 1)m - 1]r , which gives a slight
overestimate of the design effect [45]. It was recommended that trials account
for variable cluster size in their sample size calculations if x is greater than
or equal to 0.23 [45]. The effect of adjustment for variable cluster size on
sample size is negligible when x is less than 0.23. For unequal cluster sizes,
VIFs were provided for continuous outcomes [24], binary outcomes [25], and
count outcomes [46], respectively. Variation in cluster sizes affects the sample
size estimate or the power of the study. Guittet et al. [47] and Ahn et al. [48]
investigated the impact of an imbalance in cluster size on the power of trials
through simulations for continuous and binary outcomes, respectively.
The primary analysis approaches are cluster-level analyses and individuallevel analyses such as mixed-effects models and generalized estimating
equations (GEEs) [49]. Cluster-level analysis is a two-stage approach with
estimating a summary measure of the outcome for each cluster frst and
then analyzing the summaries using standard methods for independent
data. Variance-weighted cluster-level analysis has been proposed to improve
effciency when clusters are not of the same size. Mixed-effects models
and GEEs have been frequently used for the analysis of individual-level
data. However, these methods can lead to infated type I error rates when
the number of clusters is small. For mixed-effect models, small-sample
corrections to circumvent the infated type I error rate involve degrees-offreedom corrections [50–52]. For GEEs, the corrections typically involve
corrections to standard errors [53, 54].
Example: Colorectal cancer screening is effective but underused.
Guidelines for recommended tests and screening intervals depend
on specifc risks. To facilitate risk-tailored testing in the primary care
context, Skinner et al. [41] developed a tablet-based Cancer Risk Intake
System (CRIS). CRIS asks questions about risk before appointments and
generates tailored printouts for patients and physicians, summarizing
and matching risk factors with guideline-based recommendations. In
a pragmatic CRIS trial, physicians were randomly allocated to either
a comparison or risk-based CRIS group. In this CRIS trial, a physician
corresponds to a cluster. Based on the assignment of his or her physician, each patient was assigned to the CRIS intervention or a comparison
group. A CRT was selected over an IRT to avoid contamination and for
logistical reasons such as ease of administration.
The investigators plan to conduct a CRIS trial in Hispanic men and women
of 40–65 years old. The primary outcome is participation in risk-appropriate
colorectal cancer testing (yes/no, 1 = participation in any risk-appropriate testing, 0 = non participation). We anticipate about 20% of the comparison group
will participate in appropriate testing based on pilot and published data [55].
We will assume that the CRIS group will yield at least a 32% participation
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
10
Design and Analysis of Pragmatic Trials
rate. In an IRT ( r = 0 ), we need a sample size of 206 subjects per intervention group using a 5% signifcance level and 80% power. Suppose that each
physician recruits 23 patients (m = 23). With r = 0.02 , the design effect, also
called the variance infation factor, is DE = 1 + (23 - 1) × r = 1.44, meaning that
the CRT requires 1.44 times as many patients as required for an IRT, all else
being equal. CRT needs to recruit 297 (= 206 × DE ) patients per intervention
group. Since each physician recruits 23 patients per intervention group, the
number of physicians (n) to be recruited is 13. Cluster sizes are expected to
be unequal because a different number of patients will be recruited among
physicians. The required number of physicians can be estimated using the
design effect computed under variable cluster sizes for binary outcomes [25].
In some cluster randomization trials such as the GOODNEWS (Genes,
Nutrition, Exercise, Wellness, and Spiritual Growth) [56], the number of clusters cannot exceed a specifed maximum value due to practical considerations
such as the fxed expense of maintaining staff to collect data and conduct
an intervention in each cluster. In those trials, the sample size requirement
should be provided for the number of subjects per cluster instead of the
number of clusters per group. Donner and Klar [23] and Taljaard et al. [57]
provided the sample size formula for the number of subjects required per
cluster, assuming the number of subjects in each cluster is fxed in advance.
1.2.2 Restricted Randomized Designs: Strategies to Improve
Efficiency for CRTs
Cluster randomization trials with relatively few clusters have been widely
used to evaluate healthcare strategies. For CRTs with a limited number of
available clusters, a practical limitation of the simple completely randomized
parallel design is an imbalance in baseline characteristics (covariates) across
intervention groups, which would threaten the internal validity of the
trials. Randomization does not ensure that the intervention groups will be
balanced in crucial baseline characteristics when a limited number of clusters
are used in CRTs. Unbalanced intervention groups constitute a potentially
severe methodological problem for CRTs because observed differences in
outcomes between intervention groups may not be due to the intervention
but due to the differences in the underlying study populations [26]. That
is, an imbalance in crucial baseline characteristics between intervention
groups diminishes the case for causal inference, which is the fundamental
strength of the randomized trial. Therefore, investigators planning a cluster
randomized trial should consider balancing baseline characteristics. In
addition, an imbalance can lead to differences between crude and adjusted
estimates of intervention effects, which hinders the interpretability and face
validity of the fndings [23, 26].
Various restricted randomization methods have been proposed to minimize imbalance in CRTs. Ivers et al. [26] provided the advantages and
limitations of different allocation techniques, including matched-pair,
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
11
stratifcation, minimization, and covariate-constrained randomization, and
guided in choosing the best allocation technique for CRTs.
1.2.2.1 Matched-Pair Cluster Randomized Design
Matched-pair designs have been frequently used in community intervention
trials. For example, Kroeger et al. [58] conducted a matched-pair cluster
randomized trial of interventions against Aedes mosquitoes. The primary
outcome was the number of containers per house that were positive for
immature stages of the mosquito. Pairs of clusters of households were
randomized to a package of window curtains and water container covers
treated with insecticide, or to control (no intervention). A matched-pair
cluster randomized design seems attractive since matching before random
assignment of clusters to interventions can signifcantly improve the effciency
of causal effect estimation [59]. Matched-pair CRTs are widely conducted
by pairing the intervention and control clusters based on selected common
features related to the primary outcome to mitigate baseline imbalance and
improve statistical power. In a matched-pair cluster randomized design,
clusters are formed into pairs based on similar baseline characteristics such
as cluster size, geographic location, or other features potentially related to
the primary outcome measure. One cluster within each pair is randomly
allocated to an intervention and the other to a control.
For a matched-pair cluster randomized trial, the matching would be both at
an individual level and at a cluster level. Matching reduces between-cluster
variability in estimating the intervention effect, reducing the standard error
and increasing power and precision. Several authors examined the effect
of matching in randomized community intervention trials using t-tests [60,
61]. Suppose that there are n clusters in each intervention group, and the
continuous outcome is analyzed by paired and unpaired t-tests for matched
and unmatched data, respectively. For unmatched analysis with continuous
outcomes, the degrees of freedom will be 2(n - 1) for a t-test statistic that
compares the outcome between the two intervention groups. For a matched
analysis, with n-matched cluster pairs, the degree of freedom will be n - 1
for a t-test statistic. That is, the matched analysis has half the degrees of
freedom of the unmatched analysis. A matched-pair cluster randomized
trial has less power than an unmatched cluster randomized trial since a less
degree of freedom for a t-distribution corresponds with a larger critical value
[23, 37]. Therefore, the gain in correlation within a pair must be larger than
the homogeneity within a pair for matching to be worthwhile in a matchedpair CRT [60]. Let rM be the matching correlation, defned as the standard
Pearson correlation for the outcome computed over the paired clusters.
Matching will yield an effciency gain only if the matching correlation,
rM , is suffciently high to offset the reduction in degrees of freedom. For
this reason, it is worthwhile to match only cluster-level factors known to
be strongly associated with the outcome [23]. Breakeven values of rM are
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
12
Design and Analysis of Pragmatic Trials
the smallest possible correlations that matching must induce for matchedpair cluster randomization to detect a smaller effect size than the unmatched
cluster randomization [37, 59]. The approximate reduction in the design effect
for a matched-pair design compared with a completely randomized design
is 1 - rM [23, 62]. The design effect will be reduced by 30% if the matching
correlation ( rM ) is 0.3. Therefore, an effciency gain will be obtained through
matching only if rM is suffciently large to offset the reduction in degrees of
freedom. When the number of clusters is large, ineffective matching is not
a severe problem. However, matching or not is an important design issue
in CRTs when the number of clusters to be randomized is relatively small.
Martin et al. [60] compared the statistical power between the matched-pair
cluster randomized design and a completely randomized parallel design
when the number of matched-pair clusters is small to moderate. They showed
that when the number of available pairs is ten or less, then matching should
be used only if rM is at least 0.2.
For the analysis of continuous outcomes, cluster-level analysis can be
done using statistical methods such as paired t-test, Wilcoxon signed-rank
test, and permutation test. Let di be the mean difference in the continuous
outcome between clusters in the ith matched-pair. A simple approach to test
an intervention is applying the standard paired t-test to the mean differences
di , i = 1, 2,..., n , where n is the number of matched cluster pairs. The paired
t-test assumes that the di is normally distributed with a mean ( D ) and an
equal variance across the matched-pairs. Since cluster sizes generally vary
across matched-pairs, the assumption of equal variances is violated. When
clusters are not the same size, variance-weighted cluster-level analysis has
been proposed to improve effciency. When the number of matched-pair
is large, violation of the normality assumption is not serious since di will
have an approximately normal distribution with the central limit theorem.
The Wilcoxon signed-rank test or Fisher’s permutation test can be used as
an alternative to the paired t-test in the presence of obvious non-normality
or heterogeneity in the variances of the di [23]. These approaches take
advantage of avoiding normality assumptions. Wilcoxon signed-rank test
is applied to di based on the ranks of the di instead of the actual values.
Fisher’s one-sample permutation test uses the magnitude and the ranks of
the di . A limitation of the exact permutation test is that we need a minimum
of six matched-pairs of clusters to obtain a two-sided p-value of less than
0.05. For an individual-level analysis, generalized estimating equation (GEE)
and mixed-effects models can be used to analyze the continuous outcomes
from matched-pair CRTs.
For the analysis of binary outcomes, Donner and Klar [23] provided statistical methods such as the standard Mantel–Haenszel one degree of freedom
chi-square test, Liang’s chi-square test for analyzing 2 × 2 tables [63, 64], paired
t-test, Wilcoxon signed-rank test, and one-sample permutation test. The data
from a matched-pair CRT with a binary outcome variable may be summarized
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
13
in a series of n 2 × 2 tables, where n is the number of matched cluster pairs
with the row for responses (yes/no) and the column for intervention groups
(intervention/control). The standard Mantel–Haenszel one degree of freedom
chi-square test for analyzing matched-pair clustered data can lead to spurious
statistical signifcance since the test ignores the clustering effect. It is recommended not to use a standard Mantel–Haenszel chi-square test to analyze
binary outcomes in a matched-pair CRT. Liang [63] developed a chi-square test
for the analysis of 2 × 2 tables by relaxing the binomial assumptions. Liang’s
chi-square test may apply to CRTs when there are at least 25 pairs. The paired
t-test can be applied to the difference di for the matched-pair CRTs, where di is
the difference in the proportions of response between intervention and control
groups in the ith pair. Individual-level analysis can be conducted using a generalized estimating equation (GEE) or generalized linear mixed model (GLMM).
Shipley et al. [65] provided a sample size formula and power of the test
that compares the incidence rates between two groups in matched-pair cluster randomized trials. They investigated the factors affecting the power of
matched-pair CRTs and provided an example where the power of a CRT is
compared to that of an IRT. Donner and Klar [23] provided the sample size
formulas that compare the means, proportions, and incidence rates between
two groups in matched-pair cluster randomization designs. Rutterford et al.
[66] provided the variances for binary and continuous outcomes for matchedpair cluster randomization trials, which can be used for sample size estimation. Missing data is common in matched-pair cluster experimental designs.
Investigators often encounter incomplete observations of paired outcomes.
For pairs of observations, some subjects contribute complete pairs of outcomes from both intervention groups. In contrast, some subjects contribute
only one outcome from either an intervention or control group.
In sample size calculation, one common approach to handle such missing
data is to use a simple adjustment that divides the sample size estimate
under no missing data by the expected follow-up rate. Xu et al. [27, 28] used
the GEE method to derive a closed-form sample size formula for matchedpair cluster randomization design with continuous and binary outcomes
by treating incomplete observations as missing data in a marginal linear or
logistic regression model. The sample size formula was developed using a
general correlation structure for the outcome data, including three intraclass
correlations: (1) the within-cluster correlation ( r1 ), which describes the
similarity between outcomes from different study units within the same
cluster under the same treatment; (2) the within-matched individual (study
unit) correlation ( r2 ), which describes the similarity between outcomes
from two matched individuals under different treatments; (3) the withinmatched cluster correlation ( r3 ), which describes the similarity between
outcomes from different study units within two matched clusters but under
different treatments. The within-matched individual correlation is required
if matching is done at the individual level. However, if matching occurs only
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
14
Design and Analysis of Pragmatic Trials
at the cluster level, the correlation structure would depend only on r1 and
r3 with r2 = r3 .
Example: COMMIT (Community Intervention Trial for Smoking
Cessation) is a cluster randomized trial employing a matched-pair
design [67]. The community was chosen as the unit of randomization
in the COMMIT since the interventions were conducted on communities rather than individuals. The investigators selected 22 communities
and matched these communities based on several factors expected to be
related to the smoking quit rates, such as community size, geographical proximity, age and sex composition, degree of urbanization, and
socioeconomic factors. The COMMIT design included 11 matched-pair
communities. Each member of the 11 community pairs was randomly
assigned to receive active intervention and the other to receive control
surveillance. This trial aims to assess the effect of a community program encouraging people to stop smoking. The rates of quitting smoking in the intervention and control communities were compared using a
matched-pair analysis, based on the permutation distribution. Gail et al.
[67] provided a detailed discussion of permutation tests for the design
and analysis of the COMMIT.
1.2.2.2 Stratifed Cluster Randomized Design
Matched-pair cluster randomized design can help minimize the differences
between intervention groups for prognostic factors potentially related to an
outcome and can improve the power and precision of the study. However,
there is a possibility that substantial imbalances in other essential factors
arise between intervention groups. If there are a small number of categorical
covariates, a simple way to handle imbalances is to use a stratifed cluster
randomized design. Stratifcation involves grouping clusters into two or
more strata that are expected to be similar to the outcome of interest. The
clusters within each stratum are then randomly allocated between the
intervention groups.
In stratifed CRTs, stratifcation factors often include cluster size, clusterlevel socioeconomic status, geographic location, and the healthcare system.
Cluster size is commonly used as a stratifying factor because cluster size
may be associated with critical cluster-level factors and has been recognized
as a surrogate for within-cluster dynamics that predicts outcomes in cluster
randomization trials [23]. The conventional randomization procedure might
fail to achieve balance in cluster size between intervention groups, leading to
biased estimation of an intervention effect. One possible solution is to adopt
the stratifed cluster randomization design, where clusters are frst grouped
into strata based on size (e.g., small, medium, and large) and then randomized to intervention groups within each stratum. Stratifed CRTs are popular
because they increase the chance of the intervention groups being well balanced regarding identifed prognostic factors at baseline and may increase
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
15
statistical power. The stratifed design may be viewed as replicating a completely randomized parallel design in each stratum.
The continuous outcomes in a stratifed CRT can be analyzed using a t-test
based on the weighted mean difference [23]. The stratum-specifc effects are
measured by the difference of the means ( di ) in the ith stratum. The variance
of di is computed incorporating an intracluster correlation among subjects
within a cluster. The weighted statistic is set up based on the weighted mean
difference with weights chosen to refect the relative information in the di
[68]. A standard Mantel–Haenszel statistic was extended to analyze binary
outcomes, incorporating intracluster correlation ( r ) among observations
within a cluster [62]. If r is equal to zero, the generalized Mantel–Haenszel
statistic is identical to a standard Mantel–Haenszel statistic. GEE and GLMM
can be used to analyze the binary and continuous outcome data by adjusting
individual-level as well as cluster-level covariates from a stratifed cluster
randomized design. Donner [69] extended the sample size formula for the
Cochran–Mantel–Haenszel statistic with binary outcomes [70]. Donner’s
sample size formula assumes the cluster size to be equal within strata
but different across strata. With varying cluster sizes, commonly used ad
hoc approaches have assumed the cluster sizes to be constant within each
stratum, which may underestimate the required number of clusters for each
group per stratum and lead to underpowered clinical trials. Xu et al. [71]
extended Donner’s sample size formula [69], incorporating the variability in
cluster size with the coeffcient of variation ( x ) of cluster size. Wang et al. [72]
also accommodated the variability of cluster size and proposed the closedform sample size formula for cluster size-stratifed CRTs with continuous
outcomes. The sample size formulas of Xu et al. [71] and Wang et al. [72]
are fexible to accommodate an arbitrary randomization ratio and varying
numbers of clusters across strata.
The advantages of stratifed CRTs include increased precision (and power)
and balanced treatment groups. The number of strata increases rapidly as the
number of stratifying factors increases. Suppose that there are two categories
in each stratifcation factor. The number of strata is 2k when the number of
stratifcation factors is k. Relatively few stratifcation factors can be included
in stratifed cluster randomized designs since the number of strata increases
exponentially as the number of stratifcation factors increases.
Example: In a pragmatic stratifed cluster randomization trial called
“Improving chronic disease management with PIECES (NCT02587936)”,
primary care clinics were randomly allocated to either an intervention
or standard medical care group using a randomized permutation block
within each healthcare system. The stratum is each of the four large
healthcare systems participating in the study. The unit of randomization
is a primary care clinic. The cluster randomization design with clinics
receiving collaborative primary care–subspecialty care vs standard care
limits the risk of cross-contamination between intervention and control
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
16
Design and Analysis of Pragmatic Trials
groups. Based on the assignment of the clinic where a patient goes, each
patient will be assigned to either the intervention or standard medical
care group. Evaluation will be performed to determine treatment effects
on disease-specifc hospitalizations, ER visits, cardiovascular events,
and deaths.
The sample size was estimated based on comparing one-year unplanned allcause hospitalization rates between the control and intervention groups. The
sample size formula developed by Donner [69] for stratifed randomized trials was employed. Preliminary data showed that the rate of unplanned allcause hospitalization during the one-year follow-up period was 14% across
all four large healthcare systems in the standard medical care group. The
hospitalization rate in the intervention group is expected to be 3% lower
than that in the standard medical care group. A generalized linear mixed
model will be used to investigate if there is a signifcant difference in the
rate of unplanned all-cause hospitalization during the one-year follow-up
period between the intervention group and the standard medical care group.
Electronic health records show that the number of patients with coexistent
CKD, hypertension, and diabetes are 4,419, 4,738, 4,175, and 1,093 in healthcare systems 1, 2, 3, and 4, respectively. The numbers of clinics are 25, 40, 50,
and 9 in healthcare systems 1, 2, 3, and 4, respectively. A preliminary dataset
obtained an intracluster correlation coeffcient (ICC) of 0.015. If we assumed
ICC = 0.015 to detect a 3% difference in the rate of unplanned all-cause hospitalization, a total of 10,991 patients are needed to achieve 80% power at a
two-sided 5% signifcance level. We would need to enroll 3,367, 3,610, 3,181,
and 833 patients from healthcare systems 1, 2, 3, and 4, respectively. Here,
10,991 patients are 76.2% of 14,425 patients from the four healthcare systems
participating in the study. Waiver of consent has been obtained from all
institutional review boards (IRBs) overseeing the research, and no informed
consent will be obtained from patients. An opt-out option is available for
patients in the intervention and control groups. A small number of opt-out
requests are expected based on the nature of the interventions.
1.2.2.3 Covariate-Constrained Randomized Design
Unbalanced intervention groups lead to a potentially severe methodological problem for CRTs. Simple or matched-pair or stratifed randomization
often cannot adequately balance multiple cluster-level covariates between
intervention groups when the number of clusters is small. Therefore, covariate-constrained randomization was proposed as an allocation technique
to achieve balance when clusters can be recruited before randomization.
Once cluster-level baseline data are obtained, the randomization process
can begin. Moulton [73] described the covariate-constrained randomization
(CCR) procedure that enumerates all the possible allocations of participating clusters when clusters and their covariates are known in advance. A
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
17
æwö
randomization scheme is randomly chosen from all the possible ç ÷ ranègø
domization schemes, where w is the total number of clusters and g is the
number of clusters assigned to one study arm. For example, if we design a
CRT with ten clusters, fve of which are assigned to intervention and fve
æ 10 ö
to control, there are ç ÷ = 252 unique allocations of ten clusters evenly
è5ø
assigned to two arms. The randomization scheme is randomly selected from
a subset of all possible randomization schemes using a score that assesses
covariate imbalance. CCR calculates a score that assesses covariate imbalance from all the possible allocation schemes, limits the randomization space
to prespecifed constraints, and then selects a scheme from the constrained
list to implement an acceptable allocation.
Example: The reminder–recall (R/R) immunization trial compared the
population-based R/R approach with the practice-based R/R approach
to increase up-to-date immunization rates in 19- to 35-month-old children in 16 counties in Colorado [74]. The population-based intervention
used collaborations between primary care physicians and health department leaders to develop a centralized R/R notifcation using telephone
or mail for all parents whose children were not up to date on immunizations. The practice-based group invited practices to attend a webbased training on R/R using the Colorado Immunization Information
System (CIIS). Sixteen counties were randomized equally to each of the
two R/R approaches. Within each stratum (rural, urban), they generated
70 possible combinations of eight counties into two study groups and
standardized county-level variables by computing simple z scores for
each measure. Let xi be the cluster-level variable with x as the mean
of xi and s as the standard deviation across clusters. To allow each
measure to contribute approximately equally to the balancing process, cluster-level variables were standardized using a simple z score,
zi = (xi - x)/ s . For each possible randomization, clusters were allocated to a treatment group. Next, the absolute value of the difference
between the allocated treatment groups on the original county-level raw
variables was computed for each randomization. The balance criterion
measures the overall imbalance. The best 10% randomizations for rural
and urban counties were designated as the optimal set.
1.2.3 Multiple-Period Cluster Randomized Designs
CRTs have lower effciency than IRTs due to correlation among subjects
within the same cluster. Effciency can be improved by increasing the sample size. However, increasing the sample size is not always possible since
the number of clusters and cluster sizes are often limited. One strategy to
increase effciency is to implement a multiple-period design within a CRT.
That is, multiple-period CRTs extend traditional CRTs over time, with each
cluster contributing observations over prespecifed time points, possibly
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
18
Design and Analysis of Pragmatic Trials
switching between intervention groups. The most basic type of multipleperiod CRTs is a longitudinal cluster randomized trial (LCRT), where clusters of subjects are randomly assigned to either a control or an intervention
group and measured repeatedly at prespecifed time points in the assigned
group for the duration of the study [75, 76]. Crossover cluster randomized
trials (CCRTs) and stepped-wedge cluster randomized trials (SW-CRTs) are
two other types of multiple-period CRTs.
CCRTs [77–80] aim to increase statistical power compared to LCRTs by
alternating clusters between control and intervention groups. In CCRTs,
clusters of subjects are randomly assigned to different sequences of
treatments over the study period. Correlation structures are complicated
in LCRTs and CCRTs due to the longitudinal and clustered nature of trials.
Wang et al. [76] used the GEE method to derive a closed-form sample size
formula for LCRTs using a general correlation structure for the outcome
data, including (1) correlation among repeated measurements from the
same subjects (within-subject or longitudinal correlation), (2) correlation
between concurrent measurements from different subjects within the same
cluster (the conventional intracluster correlation coeffcient, ICC), and (3)
correlation between nonconcurrent measurements from different subjects
within the same cluster (cross-subject cross-period correlation). Ignoring
the above correlations leads to biased estimation and improper sample
size estimation. Generalized linear mixed model (GLMM) and generalized
estimating equation (GEE) approaches have been commonly used for
sample size estimation and statistical analysis. SW-CRTs [81–85] randomize
clusters of subjects to one of the intervention sequences. Each sequence
requires that clusters start in the control condition and then switch to the
intervention condition one at a time at prespecifed time points. Hemming
et al. [86] provided a tutorial on sample size calculation for multiple-period
cluster randomized trials using the Shiny CRT Calculator (https://clusterrcts
.shinyapps.io/rshinyapp/).
There are three major types of multiple-period CRTs [30, 86]. One is a
closed-cohort design, where all subjects are recruited at the beginning of
the trial, repeatedly assessed throughout the study; hence, longitudinal
measurements are collected from the same subjects. New subjects cannot join
the trial as it is ongoing. Another is a cross-sectional design, where subjects
are selected for measurements at a specifc time point and will not be selected
again at a later time point. That is, different subjects are assessed at each time
point. The other is an open-cohort design, where subjects join and leave the
clusters over time. That is, some subjects are repeatedly assessed throughout
the study, while others can leave or join in the middle of the study.
1.2.3.1 Longitudinal Cluster Randomized Design
In longitudinal cluster randomized trials (LCRTs), clusters of subjects, such
as those formed by clinics and communities, are randomly assigned to
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
19
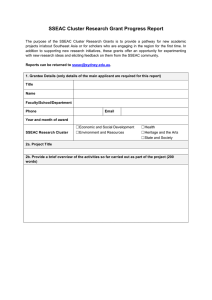
FIGURE 1.2
Diagrams of the LCRT and CCRT with two sequences. (Blank and shaded cells represent
control and intervention, respectively.)
the intervention groups and are measured repeatedly at prespecifed time
points throughout the study [87]. The upper panel in Figure 1.2 illustrates
the intervention scheme of an LCRT design, which has been widely used in
behavioral and health service research. Examples include longitudinal community intervention studies or family studies with repeated measures on
each subject [88–90]. For instance, in community intervention trials, outcome
measures such as blood pressure or quality of life is collected on each subject
from each community over time.
In clinical trials with repeated measurements, the responses from each subject are measured multiple times during the study period. Two approaches
have been widely used to assess the intervention effect: one that compares
the rates of change and the other that compares the time-averaged responses
between the intervention groups. Sample size and power formulas were
developed to compare the time-averaged responses and the rates of changes
over time using GEE [75] and GLMM [91–93]. For example, Wang et al. [76]
provided closed-form sample size and power formulas for comparing the
time-averaged responses based on the GEE approach. These formulas are
fexible to incorporate unbalanced randomization, different missing patterns,
arbitrary correlation structures, and randomly varying cluster sizes, providing a practical yet robust sample size solution. Hooper et al. [94] showed how
to calculate sample size for a longitudinal cluster randomized trial with a
repeated cross-section or closed cohort design. Sample size formulas were
presented for open cohorts and the impact of the degree of “openness” on
sample size [95]. For proper statistical inferences, generalized linear mixed
model (GLMM) and generalized estimating equation (GEE) approaches have
been commonly used in analyzing data from LCRTs.
Example: Bosworth et al. [89] conducted an LCRT on blood pressure (BP)
control at a Veterans Affairs (VA) Medical Center. Physicians were randomly allocated to either the control group or the intervention group.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
20
Design and Analysis of Pragmatic Trials
In this LCRT, a physician corresponds to a cluster. Based on the assignment of his or her physician, each patient was assigned to either the
control or intervention group and followed over time. In the intervention group, primary care providers (PCPs) received computer-generated
decision support designed to improve guideline-concordant medical
therapy at each clinic visit. In the control group, PCPs received a standard reminder at each visit. BP values were obtained at each primary
care visit according to VA standards. An LRCT was selected over a longitudinal individual randomized trial to avoid contamination and for
logistical reasons such as ease of administration. The primary outcome
was the proportion of patients who achieved a BP of less than 140/90 mm
Hg (less than 130/85 for diabetic patients) over the 24-month intervention. A hierarchical mixed-effects logistic regression model was used to
investigate if there were signifcant differences in BP control in the three
intervention groups compared to the hypertension reminder control
group. The model included patient-level random effects in the form of
a patient-level random intercept and slope to account for the correlation
between a patient’s repeated BP measurements. The model also included
a provider group-level random effect to account for the correlation of
patients within the same provider.
1.2.3.2 Crossover Cluster Randomized Design
In crossover cluster randomized trials (CCRTs), clusters of subjects are randomly assigned to different sequences of interventions over the study period.
Each cluster receives each intervention in a separate period. For example, the
lower panel of Figure 1.2 illustrates a typical CCRT with two treatments. In
a two-period, two-intervention CCRT design, the so-called AB/BA design,
in which each cluster is randomly assigned to one of two groups of the trial.
Subjects within clusters in the frst group receive intervention A in the frst
period of the trial and intervention B in the second period, and subjects
within clusters included in the second group receive intervention B in the
frst period and intervention A in the second period.
CCRTs are frequently employed in clinical research [77–80, 96–98]. With
the crossover design, clusters are randomized to a sequence of intervention
conditions rather than just one intervention condition. CCRTs with two
periods were commonly applied. Many studies have also investigated and
employed CCRTs with multiple periods [77, 99, 100]. CCRTs increase statistical
effciency because each cluster receives both intervention conditions, which
allows comparisons within clusters [100]. The comparisons within clusters
help to eliminate chance imbalances between intervention and control
conditions on cluster-level characteristics even in studies with a small
number of clusters. CCRTs can have more power to detect a given treatment
effect than the cluster-randomized non-crossover trials with the same
number of subjects. Thus, CCRTs can be especially useful when the number
of available clusters is limited. A crossover design may be cost-effective
if enrolling a cluster costs much or if there are few available clusters. The
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
21
principal drawback of the CCRT is that the effects of one intervention may
“carry over” and alter the response to subsequent interventions. CCRTs
cannot be conducted if receiving the intervention in the frst period would
affect observations in the second period. For example, a training/education
intervention for smoking cessation could not be crossed over because there
would not be a way to remove the effects of the intervention during the
control period once a group received the training/education intervention.
However, the crossover design could be implemented if the intervention
does not have lingering effects. In a Nordic diet study, Danish municipal
schools were randomized to intervention sequences assuming that the effect
of the intervention in the frst period would not carry over into the second
period [97, 98].
Sample size formulas have been proposed for the two-period, twointervention, cross-sectional CCRTs [101, 102, 78]. Sample size formulas for
continuous and binary outcomes were developed for the cross-sectional, twoperiod, two-intervention CCRTs using GEE approaches, accounting for both
the within-period and inter-period correlations [31]. Sample size formulas
for cross-sectional CCRTs were extended for cohort CCRTs by extending
the two-period nested exchangeable correlation structure to a two-period
block exchangeable correlation structure. Using GEE approaches, sample
size formulas were developed incorporating the missing data patterns and
arbitrary correlation structures [76].
Example: The Head Positioning in Acute Stroke Trial (HeadPoST) is a
two-period pragmatic CCRT conducted at 114 hospitals in nine countries
[80]. The trial aimed to compare the effects of the lying-fat position with
those of the sitting-up position, initiated soon after a stroke and maintained for 24 hours. Hospitals were randomly assigned to two sequences.
The frst sequence received the lying-fat position and then crossed over
to the sitting-up position. The second sequence received two positions
in the reverse direction. The degree of disability in the modifed Rankin
scale score was collected for each patient. The primary outcome was the
degree of disability at 90 days, as assessed with the modifed Rankin
score ranging from 0 to 6, with higher scores indicating more signifcant
disability and 6 indicating death. The primary endpoint of the intervention effect, as assessed using the modifed Rankin scale, was analyzed
using a hierarchical ordinal mixed-effect logistic regression model with
four adjustment variables (fxed intervention effect [lying fat vs sitting
up], fxed period effect, random cluster effect, and effect of the interaction between random cluster and period).
1.2.3.3 Stepped-Wedge Cluster Randomized Design
Stepped-wedge cluster randomized trials (SW-CRTs) have been increasingly
adopted in behavioral and health services research [82–84]. An SW-CRT is a
type of crossover CRT, in which the different clusters switch interventions at
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
22
Design and Analysis of Pragmatic Trials
different time points. An SW-CRT extends the traditional CRT so that every
cluster provides control and intervention observations, thus, somewhat
acting as its own control. The design includes a baseline period where none
of the clusters receive the intervention of interest. That is, all clusters receive
the control at the baseline. Then, one or more randomly allocated clusters are
scheduled to switch from a control to an intervention group at prespecifed
time points until all clusters are exposed to the intervention of interest.
Outcomes are measured at every time point. The key feature of the SW-CRT
design is the unidirectional crossover of clusters from the control to the
intervention groups on a staggered schedule, which induces confounding
of the intervention effect over time. SW-CRTs have a unique feature that
allows the stepwise introduction of interventions to a population, making it
suitable to examine the effectiveness of interventions in real-world settings
[103, 104]. Figure 1.3 illustrates a typical stepped-wedge cluster randomized
design. The horizontal axis indicates time, and the vertical axis indicates the
sequences. Each sequence includes one or more clusters of subjects.
SW-CRTs have several advantages. First, every cluster ends up getting
the intervention. Switching every cluster to intervention motivates patients
and doctors and mitigates the ethical dilemma of withholding an effective
intervention when it is believed to be superior to the control [105]. Second, it
is more effcient because comparisons from two directions provide evidence
of effectiveness, which will lead to higher statistical power over parallel CRTs
[106]. One is vertical comparison of clusters between intervention and control
at each time point. The other is horizontal comparisons of observations before
and after switching to intervention within each cluster. Third, outcomes are
measured longitudinally, offering insight into the temporal trend of the
intervention effect.
On the other hand, SW-CRTs present various challenges to researchers,
which include longer trial duration, higher risk of attrition, diffculty in
blinding, complex informed consent procedure, and complex data analysis.
For example, the correlation structure is much more complicated than that
in completely randomized cluster designs. The repeated measures may burden patients regarding quality of life, satisfaction, and costs. Moreover, the
FIGURE 1.3
An illustration of an SW-CRT with T = 4 time points and S = 3 sequences. (Each cell represents a
data collection point. Shaded and blank cells represent intervention and control, respectively.)
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
23
proportion of missing data is usually higher due to repeated measurements
over a longer duration, which cannot be ignored in the design.
Many researchers have investigated sample size calculation methods
for cross-sectional SW-CRTs [103, 107–109], where the correlation structure
is more straightforward. There have been relatively fewer publications
on sample size methods for closed-cohort SW-CRTs, some of which were
purely simulation-based [110], some based on the linear mixed-effect model
approach [94, 111], and some based on the Bayesian method [112]. Sample size
formulas were proposed for closed-cohort SW-CRTs using the GEE approach
[30, 32], which considered three types of correlations: within-period, interperiod, and within-individual correlations. Wang et al. [29, 30] provided the
closed-form sample size formulas for SW-CRTs with continuous and binary
outcomes using GEE, which can be applied to either the closed-cohort or
cross-sectional SW-CRTs by modifying the correlation structures. The sample size method is fexible to address pragmatic issues such as missing data
due to various mechanisms or complicated correlation structures.
Mixed-effects regression and generalized estimating equation (GEE)
have commonly been used in analyzing SW-CRTs. Li et al. [34] provided an
overview of mixed-effects regression models that have been applied to the
design and analysis of SW-CRTs.
Example: The Acute Coronary Syndrome Quality Improvement in Kerala
(ACS QUIK) trial was a pragmatic, cluster-randomized, stepped-wedge
clinical trial in which 63 hospitals were randomized to receive the quality improvement tool kit intervention at 1 of 5 predefned, 4-month steps
over 24 months after a period of usual care [113]. During fve predefned
steps over a 24-month study period, hospitals were randomly selected
to move in a one-way crossover from the control group to the intervention group. The primary outcome was the composite of all-cause death,
reinfarction, stroke, or major bleeding at 30 days. Mixed-effects logistic
regression models were used to analyze the primary outcome, 30-day
major adverse cardiovascular events, with a random cluster (hospital)
effect and a fxed time effect for every 4-month step. There was no statistically signifcant difference in 30-day composite event rates between the
control phase of 6.4% and the intervention phase of 5.3% after adjusting
for the effects of cluster and temporal trends.
References
1. D. Schwartz, and J. Lellouch. Explanatory and pragmatic attitudes in therapeutical trials. Journal of Clinical Epidemiology, 20(8):637–648, 1967.
2. D.L. Sackett. Clinician-trialist rounds: 16. mind your explanatory and pragmatic
attitudes! – Part 1: What? Clinical Trials, 10(3):495–498, 2013.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
24
Design and Analysis of Pragmatic Trials
3. K. Loudon, S. Traweek, F. Sullivan, P. Donnan, K. Thorpe, and M. Zwarenstein.
The precis-2 tool: Designing trials that are ft for purpose. BMJ, 350:h2147, 2015.
4. R.E. Glasgow, T.M. Vogt, and S.M. Boles. Evaluating the public health impact
of health promotion interventions: The re-aim framework. American Journal of
Public Health, 89(9):1322–1327, 1999.
5. G. Gartlehner, R.A. Hansen, D. Nissman, K.N. Lohr, and T.S. Carey. A simple
and valid tool distinguished effcacy from effectiveness studies. Journal of
Clinical Epidemiology, 59(10):1040–1048, 2006.
6. K.E. Thorpe, M. Zwarenstein, A.D. Oxman, S. Treweek, C.D. Furberg, D.G.
Altman, et al. A pragmatic–explanatory continuum indicator summary (precis):
A tool to help trial designers. Journal of Clinical Epidemiology, 62(5):464–475, 2009.
7. N.A. Patsopoulos. A pragmatic view on pragmatic trials. Dialogues in Clinical
Neuroscience, 13(2):217–224, 2011.
8. M. Rifai, D. Itchhaporia, and S. Virani. Pragmatic clinical trials—Ready for
prime time? JAMA Network Open, 4(12):e2140212, 2021.
9. J.P.W. Bynum, D.A. Dorr, J. Lima, E.P. McCarthy, E. McCreedy, R. Platt, et al.
Using healthcare data in embedded pragmatic clinical trials among people
living with dementia and their caregivers: State of the art. Journal of the American
Geriatrics Society, 68(Suppl 2):549–554, 2020.
10. F.P. Wilson, M. Shashaty, I. Testani, J. Aqeel, Y. Borovskiy, S.S. Ellenberg, et al.
Automated, electronic alerts for acute kidney injury: A single-blind, parallelgroup, randomised controlled trial. Lancet, 385(9981):1988–1974, 2015.
11. B.L. Strom, R. Schinnar, F. Aberra, W. Bilker, S. Hennessy, C.E. Leonard, et al.
Unintended effects of a computerized physician order entry nearly hard-stop
alert to prevent a drug interaction: A randomized controlled trial. Archives of
Internal Medicine, 170(17):1578–1583, 2010.
12. L.G. Hemkens, R. Saccilotto, S.L. Reyes, D. Glinz, T. Zumbrunn, O. Grolimund,
et al. Personalized prescription feedback using routinely collected data to
reduce antibiotic use in primary care: A randomized clinical trial. JAMA
Internal Medicine, 177(2):176–183, 2017.
13. L.D. Fiore, and P.W. Lavori. Integrating randomized comparative effectiveness
research with patient care. New England Journal of Medicine, 374(22):2152–2158,
2016.
14. K.A. McCord, R.A. Al-Shahi, S. Treweek, H. Gardner, D. Strech, W. Whiteley,
et al. Routinely collected data for randomized trials: Promises, barriers, and
implications. Trials, 19(1):29, 2018.
15. R.J. Little, R. D’Agostino, M.L. Cohen, K. Dickersin, S.S. Emerson, J.T. Farrar, et
al. The prevention and treatment of missing data in clinical trials. New England
Journal of Medicine, 367(14):1355–1360, 2012.
16. D.B. Rubin. Inference and missing data. Biometrika, 63(3):581–590, 1976.
17. D.B. Rubin. Multiple Imputation for Nonresponse in Surveys. John Wiley & Sons,
1987.
18. M. Taljaard, A. Donner, and N. Klar. Imputation strategies for missing
continuous outcomes in cluster randomized trials. Biometrical Journal.
Biometrische Zeitschrift, 50(3):329–345, 2008.
19. R.R. Andridge. Quantifying the impact of fxed effects modeling of clusters in multiple imputation for cluster randomized trials. Biometrical Journal.
Biometrische Zeitschrift, 53(1):57–74, 2011.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
25
20. M.L. Anderson, R.M. Califf, and J. Sugarman. Ethical and regulatory issues of
pragmatic cluster randomized trials in contemporary health systems. Clinical
Trials, 12(3):276–285, 2015.
21. V. Palin, T.P. Van Staa, S. Steels, et al. A frst step towards best practice recommendations for the design and statistical analyses of pragmatic clinical
trials: A modifed Delphi approach. British Journal of Clinical Pharmacology, in
press.
22. S. Hahn, S. Puffer, D.J. Torgerson, and J. Watson. Methodological bias in cluster
randomised trials. BMC Medical Research Methodology, 5(1):10, 2005.
23. A. Donner, and N. Klar. Design and Analysis of Cluster Randomization Trials in
Health Research. Oxford University Press, 2000.
24. A.K. Manatunga, M.G. Hudgens, and S. Chen. Sample size estimation in cluster
randomized studies with varying cluster size. Biometrical Journal, 43(1):75–86,
2001.
25. S. Kang, C. Ahn, and S. Jung. Sample size calculations in cluster randomized
studies with varying cluster size: A binary case. Drug Information Journal,
37(1):109–114, 2003.
26. N.M. Ivers, I.J. Halperin, J. Barnsley, J.M. Grimshaw, B.R. Shah, K. Tu, et al.
Allocation techniques for balance at baseline in cluster randomized trials: A
methodological review. Trials, 13:120, 2012.
27. X. Xu, H. Zhu, and C. Ahn. Sample size considerations for matched–pair cluster
randomization design with incomplete observations of continuous outcomes.
Contemporary Clinical Trials, 104:106336, 2021.
28. X. Xu, H. Zhu, A. Hoang, and C. Ahn. Sample size considerations for matched–
pair cluster randomization design with incomplete observations of binary
outcomes. Statistics in Medicine, 40(24):5397–5416, 2021.
29. J. Wang, J. Cao, C. Ahn, and S. Zhang. Power analysis for stepped wedge cluster
randomized trials with binary outcomes. Statistical Theory and Related Fields, 5,
2021.
30. J. Wang, J. Cao, C. Ahn, and S. Zhang. Sample size determination for stepped
wedge cluster randomized trials in pragmatic settings. Statistical Methods in
Medical Research, 2021.
31. F. Li, A. Forbes, E. Turner, and J. Preisser. Power and sample size requirements
for gee analyses of cluster randomized crossover trials. Statistics in Medicine,
38(4), 2021.
32. F. Li, E.L. Turner, and J.S. Preisser. Sample size determination for GEE analyses
of stepped wedge cluster randomized trials. Biometrics, 74(4):1450–1458, 2018.
33. F. Li, L. Turner, and J. Preisser. Sample size determination for gee analyses of
stepped wedge cluster randomized trials. Biometrics, 74(4):1450–1458, 2018.
34. F. Li, K. Hughes, K. Heming, M. Taljaard, E. Melnick, and P. Heagerty. Mixedeffects models for the design and analysis of stepped wedge cluster randomized
trials: An overview. Statistical Methods in Medical Research, 30(2):612–639, 2021.
35. C. Ahn, M. Heo, and S. Zhang. Sample Size Calculations for Clustered and
Longitudinal Outcomes in Clinical Research. CRC Press, 2014.
36. D.M. Murray. Design and Analysis of Group–Randomized Trials. Oxford University
Press, 1998.
37. R.J. Hayes, and L.H. Moulton. Cluster Randomised Trials, 2nd Edition. Chapman
and Hall/CRC, 2017.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
26
Design and Analysis of Pragmatic Trials
38. S. Eldridge, and S. Kerry. A Practical Guide to Cluster Randomised Trials in Health
Services Research. Wiley, 2012.
39. M.J. Campbell, and S.J. Walters. Ow to Design, Analyse and Report Cluster
Randomised Trials in Medicine and Health Related Research. UK Wiley, 2014.
40. S. Teerenstra, and M. Moerbeek. Power Analysis of Trials with Multilevel Data.
CRC Press, 2016.
41. C.S. Skinner, E.A. Halm, W.P. Bishop, C. Ahn, S. Gupta, D. Farrell, et al.
Impact of risk assessment and tailored versus nontailored risk information on
colorectal cancer testing in primary care: A randomized controlled trial. Cancer
Epidemiology, Biomarkers and Prevention, 24(10):1523–1530, 2015.
42. E.L. Turner, F. Li, J.A. Gallis, M. Prague, and D.M. Murray. Review of recent
methodological developments in group–randomized trials: Part 1–Design.
American Journal of Public Health, 107(6):907–915, 2017.
43. E.L. Turner, M. Prague, J.A. Gallis, F. Li, and D.M. Murray. Review of recent
methodological developments in group–randomized trials: Part 2–Analysis.
American Journal of Public Health, 107(7):1078–1086, 2017.
44. A. Donner, N. Birkett, and C. Buck. Randomization by cluster-sample size
requirements and analysis. American Journal of Epidemiology, 114(6):906–914, 1981.
45. S.M. Eldridge, D. Ashby, and S. Kerry. Sample size for cluster randomized
trials: Effect of coeffcient of variation of cluster size and analysis method.
International Journal of Epidemiology, 35(5):1292–1300, 2006.
46. J. Wang, S. Zhang, and C. Ahn. Sample size calculation for count outcomes
in cluster randomization trials with varying cluster sizes. Communications in
Statistics – Theory and Methods, 49(1):116–124, 2020.
47. L. Guittet, P. Ravaud, and B. Giraudeau. Planning a cluster randomized trial
with unequal cluster sizes: Practical issues involving continuous outcomes.
BMC Medical Research Methodology, 6(17):1–15, 2006.
48. C. Ahn, F. Hu, and C. Skinner. Effect of imbalance and intracluster correlation
coeffcient in cluster randomized trials with binary outcomes. Computational
Statistics and Data Analysis, 53(3):596–602, 2009.
49. C. Leyrat, K. Morgan, B. Leurent, and B. Kahan. Cluster randomized trials
with a small number of clusters: Which analyses should be used? International
Journal of Epidemiology, 47(1):321–331, 2018.
50. F.E. Satterthwaite. An approximate distribution of estimates of variance
components. Biometrics, 2(6):110–114, 1946.
51. M.G. Kenward, and J.H. Roger. Small sample inference for fxed effects from
restricted maximum likelihood. Biometrics, 53(3):983–997, 1997.
52. P. Li, and D.T. Redden. Comparing denominator degrees of freedom approximations for the generalized linear mixed model in analysing binary outcome
in small sample cluster–randomized trials. BMC Medical Research Methodology,
15:38, 2015.
53. M.P. Fay, and B.I. Graubard. Small-sample adjustments for wald-type tests
using sandwich estimators. Biometrics, 57(4):1198–1206, 2001.
54. L.A. Mancl, and T.A. DeRouen. A covariance estimator for GEE with improved
small–sample properties. Biometrics, 57(1):126–134, 2001.
55. C.S. Skinner, S.M. Rawl, B.K. Moser, A.H. Buchanan, L.L. Scott, V.L. Champion,
et al. Impact of the cancer risk intake system on patient-clinician discussions
of tamoxifen, genetic counseling, and colonoscopy. Journal of General Internal
Medicine, 20(4):360–365, 2005.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
27
56. M.J. DeHaven, M.A. Ramos-Roman, N. Gimpel, J. Carson, J. DeLemos, S.
Pickens, et al. The goodnews trial: A community-based participatory research
trial with African-American church congregations for reducing cardiovascular disease risk factors – Recruitment, measurement, and randomization.
Contemporary Clinical Trials, 32(5):630–640, 2011.
57. M. Taljaard, A. Donner, and N. Klar. Accounting for expected attrition in the
planning of community intervention trials. Statistics in Medicine, 26(13):2615–
2628, 2007.
58. A. Kroeger, A. Lenhart, M. Ochoa, E. Villegas, N. Alexander, M. Levy, et al.
Effective control of dengue vectors with curtains and water container covers
treated with insecticide in mexico and Venezuela: Cluster randomised trials.
British Medical Journal, 332:1247–1252, 2006.
59. K. Imai, G. King, and C. Nall. The essential role of pair matching in clusterrandomized experiments, with application to the Mexican universal health
insurance evaluation. Statistical Science, 24(1):29–53, 2009.
60. D.C. Martin, P. Diehr, E.B. Perrin, and T.D. Koepsell. The effect of matching on
the power of randomized community intervention trials. Statistics in Medicine,
12(3):329–338, 1993.
61. P. Diehr, D.C. Martin, T. Koepsell, and A. Cheadle. Breaking the matches in a
paired t-test for community interventions when the number of pairs is small.
Statistics in Medicine, 14(13):491–504, 1995.
62. A. Donner. Some aspects of the design and analysis of cluster randomization
trials. Journal of the Royal Statistical Society, Series C, 47(1):95–113, 1998.
63. K. Liang. Odds ratio inference with dependent data. Biometrika, 72(3):678–682, 1985.
64. K. Liang, T.H. Beaty, and B.H. Cohen. Application of odds ratio regression
models for assessing familial aggregation from case–control studies. American
Journal of Epidemiology, 124(4):678–683, 1986.
65. M.J. Shipley, P.G. Smith, and M. Dramax. Calculation of power for matched pair
studies when randomization is by group. International Journal of Epidemiology,
18(2):457–461, 1989.
66. C. Rutterford, A. Copas, and S. Eldridge. Methods for sample size determination
in cluster randomized trials. International Journal of Epidemiology, 44(3):1051–
1067, 2015.
67. M.H. Gail, D.P. Byar, T.F. Pechacek, and D.K. Corle. Aspects of statistical design
for the community intervention trial for smoking cessation (commit). Controlled
Clinical Trials, 13(1):16–21, 1992.
68. D. Schwartz, R. Flamant, and J. Lellouch. Clinical Trials. Academic Press, 1980.
69. A. Donner. Sample size requirements for stratifed cluster randomization
designs. Statistics in Medicine, 11(6):743–750, 1992.
70. R.F. Woolson, J.A. Bean, and P.B. Rojas. Sample size for case-control studies
using cochran’s statistic. Biometrics, 42(4):927–932, 1986.
71. X. Xu, H. Zhu, and C. Ahn. Sample size considerations for stratifed cluster
randomization design with binary outcomes and varying cluster size. Statistics
in Medicine, 38(18):3395–3404, 2019.
72. J. Wang, S. Zhang, and C. Ahn. Power analysis for stratifed cluster randomisation
trials with cluster size being the stratifying factor. Statistical Theory and Related
Fields, 1(1):121–127, 2017.
73. H. Moulton. Covariate-based constrained randomization of group-randomized
trials. Clinical Trials, 1(3):297–305, 2004.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
28
Design and Analysis of Pragmatic Trials
74. L.M. Dickinson, B. Beaty, C. Fox, W. Pace, W.P. Dickinson, C. Emsermann, and
A. Kempe. Pragmatic cluster randomized trials using covariate constrained
randomization: A method for practice-based research networks (PBRNs).
Journal of the American Board of Family Medicine, 28(5):663–672, 2015.
75. A. Liu, W.J. Shih, and E. Gehan. Sample size and power determination for
clustered repeated measurements. Statistics in Medicine, 21(12):1787–1801, 2002.
76. J. Wang, J. Cao, S. Zhang, and C. Ahn. A fexible sample size solution for
longitudinal and crossover cluster randomized trials with continuous
outcomes. Contemporary Clinical Trials, 109:106543, 2021.
77. J. Parienti, and O. Kuss. Cluster-crossover design: A method for limiting
clusters level effect in community-intervention studies. Contemporary Clinical
Trials, 28(3):316–323, 2007.
78. C. Rietbergen, and M. Moerbeek. The design of cluster randomized crossover
trials. Journal of Educational and Behavioral Statistics, 36(4):472–490, 2011.
79. S.J. Arnup, J.E. McKenzie, K. Hemming, D. Pilcher, and A. Forbes. Understanding
the cluster randomised crossover design: A graphical illustration of the
components of variation and a sample size tutorial. Trials, 18(1):381, 2017.
80. C.S. Anderson, H. Arima, P. Lavados, L. Billot, M.L. Hackett, V. Olavarra, et al.
Cluster-randomized, crossover trial of head positioning in acute stroke. New
England Journal of Medicine, 376(25):2437–2447, 2017.
81. C.N. Mhurchu, D. Gorton, M. Turley, Y. Jiang, J. Michie, R. Maddison, et al.
Effects of a free school breakfast programme on children’s attendance, academic
achievement and short–term hunger: Results from a stepped–wedge, cluster
randomised controlled trial. Journal of Epidemiology and Community Health,
67(3):257–264, 2013.
82. L.L. Bailet, K.K. Repper, S.B. Piasta, and S.P. Murphy. Emergent literacy
intervention for prekindergarteners at risk for reading failure. Journal of
Learning Disabilities, 42(4):336–355, 2009.
83. G. Bacchieri, A.J. Barros, J.V. Santos, H. Gonalves, and D.P. Gigante. A community
intervention to prevent traffc accidents among bicycle commuters. Revista de
Saude Publica, 44(5):867–875, 2010.
84. B.J. van Holland, M.R. de Boer, S. Brouwer, R. Soer, and M.F. Reneman. Sustained
employability of workers in a production environment: Design of a stepped
wedge trial to evaluate effectiveness and cost-beneft of the pose program. BMC
Public Health, 12:1003, 2012.
85. K. Hemming, M. Taljaard, J.E. McKenzie, R. Hooper, A. Copas, J.A. Thompson,
et al. Reporting of stepped wedge cluster randomised trials: Extension of the
consort 2010 statement with explanation and elaboration. BMJ, 363:k1614, 2018.
86. K. Hemming, J. Kasza, A. Hooper, R. Forbes, and A. Taljaard. A tutorial on sample size calculation for multiple-period cluster randomized parallel, cross-over
and stepped-wedge trials using the shiny crt calculator. International Journal of
Epidemiology, 49(3):979–995, 2020.
87. H.A. Feldman, and S.M. McKinlay. Cohort versus cross-sectional design in
large feld trials: Precision, sample size, and a unifying model. Statistics in
Medicine, 13(1):61–78, 1994.
88. S. Sabo, C. Denman, M.L. Bell, E. Cornejo Vucovich, M. Ingram, C. Valenica,
et al. Meta salud diabetes study protocol: A cluster-randomised trial to
reduce cardiovascular risk among a diabetic population of Mexico. BMJ Open,
8(3):e020762, 2018.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Pragmatic Randomized Trials
29
89. H.B. Bosworth, M.K. Olsen, T. Dudley, M. Orr, M.K. Goldstein, S.K. Datta, et
al. Patient education and provider decision support to control blood pressure
in primary care: A cluster randomized trial. American Heart Journal, 157(3):450–
456, 2009.
90. G. Grandes, A. Sanchez, I. Montoya, R. Ortega Sanchez-Pinilla, J. Torcal; PEPAF
Group. Two-year longitudinal analysis of a cluster randomized trial of physical
activity promotion by general practitioners. Plos One, 6(3):e18363, 2011.
91. M. Heo, Y. Kim, X. Xue, and M. Kim. Sample size requirement to detect an
intervention effect at the end of follow-up in a longitudinal cluster randomized
trial. Statistics in Medicine, 29(3):382–390, 2010.
92. M. Heo, and A.C. Leon. Sample size requirements to detect an intervention by
time interaction in longitudinal cluster randomized clinical trials. Statistics in
Medicine, 28(6):1017–1027, 2009.
93. M. Heo, X. Xue, and M. Kim. Sample size requirements to detect a two– or
three–way interaction in longitudinal cluster randomized clinical trials with
second–level randomization. Clinical Trials, 11(4):503–507, 2014.
94. R. Hooper, S. Teerenstra, E. de Hoop, and S. Eldridge. Sample size calculation
for stepped wedge and other longitudinal cluster randomised trials. Statistics
in Medicine, 35(26):4718–4728, 2016.
95. J. Kasza, R. Hooper, A. Copas, and A.B. Forbes. Sample size and power
calculations for open cohort longitudinal cluster randomized trials. Statistics in
Medicine, 39(13):1871–1883, 2020.
96. S. Patterson, L. McDaid, K. Saunders, C. Battison, A. Glasier, A. Radley, et
al. Improving effective contraception uptake through provision of bridging
contraception within community pharmacies: Findings from the bridge-it
study process evaluation. BMJ Open, 12(2):e057348, 2022.
97. C.T. Damsgaard, S.M. Dalskov, R.A. Petersen, L.B. Sørensen, C. Mølgaard,
A. Biltoft-Jensen, et al. Design of the opus school meal study: A randomised
controlled trial assessing the impact of serving school meals based on the new
Nordic diet. Scandinavian Journal of Public Health, 40(8):693–703, 2012.
98. C.T. Damsgaard, S.M. Dalskov, R.P. Laursen, C. Ritz, M.F. Hjorth, L. Lauritzen,
et al. Provision of healthy school meals does not affect the metabolic syndrome
score in 811-year-old children, but reduces cardiometabolic risk markers despite
increasing waist circumference. British Journal of Nutrition, 112(11):1826–1836,
2014.
99. G.R. Norman, and S. Daya. The alternating-sequence design (or multiple–
period crossover) trial for evaluating treatment effcacy in infertility. Fertility
and Sterility, 74(2):319–324, 2000.
100. K.L. Grantham, J. Kasza, S. Heritier, K. Hemming, E. Litton, and A.B. Forbes.
How many times should a cluster randomized crossover trial cross over?
Statistics in Medicine, 38(25):5021–5033, 2019.
101. B. Giraudeau, P. Ravaud, and A. Donner. Sample size calculation for cluster
randomized cross-over trials. Statistics in Medicine, 27(27):5578–5585, 2008.
102. A.B. Forbes, M. Akram, D. Pilcher, J. Cooper, and R. Bellomo. Cluster randomised crossover trials with binary data and unbalanced cluster sizes:
Application to studies of near–universal interventions in intensive care. Clinical
Trials, 12(1):34–44, 2015.
103. M.A. Hussey, and J.P. Hughes. Design and analysis of stepped wedge cluster
randomized trials. Contemporary Clinical Trials, 28(2):182–191, 2007.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
30
Design and Analysis of Pragmatic Trials
104. C.A. Brown, and R.J. Lilford. The stepped wedge trial design: A systematic
review. BMC Medical Research Methodology, 6(1):54, 2006.
105. S.J. Edwards. Ethics of clinical science in a public health emergency: Drug
discovery at the bedside. The American Journal of Bioethics, 13(9):3–14, 2013.
106. J.R. Hargreaves, A. Prost, K.L. Fielding, and A.J. Copas. How important is
randomisation in a stepped wedge trial? Trials, 16(1):359, 2015.
107. K. Hemming, T.P. Haines, P.J. Chilton, A.J. Girling, and R.J. Lilford. The stepped
wedge cluster randomised trial: Rationale, design, analysis, and reporting.
BMJ, 350:h391, 2015.
108. W. Woertman, E. de Hoop, M. Moerbeek, S.U. Zuidema, D.L. Gerritsen, and S.
Teerenstra. Stepped wedge designs could reduce the required sample size in
cluster randomized trials. Journal of Clinical Epidemiology, 66(7):752–758, 2013.
109. L.H. Moulton, J.E. Golub, B. Durovni, S.C. Cavalcante, A.G. Pacheco, V. Saraceni,
et al. Statistical design of THRio: A phased implementation clinic-randomized
study of a tuberculosis preventive therapy intervention. Clinical Trials, 4(2):190–
199, 2007.
110. G. Baio, A. Copas, G. Ambler, J. Hargreaves, E. Beard, and R.Z. Omar. Sample
size calculation for a stepped wedge trial. Trials, 16(1):354, 2015.
111. A.J. Girling, and K. Hemming. Statistical effciency and optimal design for
stepped cluster studies under linear mixed effects models. Statistics in Medicine,
35(13):2149–2166, 2016.
112. K.M. Cunanan, B.P. Carlin, and K.A. Peterson. A practical bayesian stepped
wedge design for community-based cluster-randomized clinical trials: The
British columbia telehealth trial. Clinical Trials, 13(6):641–650, 2016.
113. M.D. Huffman, P. Mohanan, R. Devarajan, A.S. Baldridge, D. Kondal, L. Zhao,
et al. Effect of a quality improvement intervention on clinical outcomes in
patients in india with acute myocardial infarction: The acs quik randomized
clinical trial. JAMA, 319(6):567–578, 2018.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
We Don’t reply in this website, you need to contact by email for all chapters
Instant download. Just send email and get all chapters download.
Get all Chapters For Ebook Instant Download by email at
etutorsource@gmail.com
You can also order by WhatsApp
https://api.whatsapp.com/send/?phone=%2B447507735190&text&type=ph
one_number&app_absent=0
Send email or WhatsApp with complete Book title, Edition Number and
Author Name.