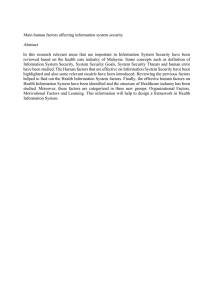
KPJ Healthcare: the first 30 years Zizah Che Senik, Rosmah Mat Isa, Noreha Halid, Adlin Masood, Soo-Wah Low and Khairul Akmaliah Adham Information about the authors can be found at the end of the article. The study was funded by a UKM University-industry research grant, code INDUSTRI-2013-042, titled ‘‘Business sustainability and strategies for growth’’. The authors wish to thank Rafeah Ariffin of KPJ Healthcare for her support of this case publication, and Siti Khadijah Mohd Ghanie for her research assistance. This case was developed based mainly on information gathered from the public domain. It is intended exclusively to facilitate the teaching and learning of strategic management and managerial economics theories and does not imply effective or ineffective managerial decisions. Disclaimer. This case is written solely for educational purposes and is not intended to represent successful or unsuccessful managerial decision making. The author/s may have disguised names; financial and other recognizable information to protect confidentiality. DOI 10.1108/EEMCS-06-2013-0081 Planning for the future By the end of 2009, Kumpulan Perubatan Johor (KPJ) Healthcare Group was the largest public-listed healthcare service provider in Malaysia. It recorded a revenue of RM1.5 billion (approximately USD0.5 billion) and a net profit after tax of RM115 million (approximately USD38 million) (KPJ Healthcare, 2009a). At the time KPJ operated 19 hospitals in Malaysia and managed two hospitals in Indonesia (see Exhibit 1 that shows the location of KPJ hospitals). In addition, it operated a nursing and health science college which supplied nurses not only for its hospitals, but also for the general need of the country. In 2009, KPJ Healthcare Group was listed as one of Malaysia’s top 100 companies due to its market capitalization that accounted for more than RM1.3 billion (KPJ Healthcare, 2009a). KPJ’s Managing Director and CEO, Datin Paduka Siti Sa’diah Sheikh Bakir (Siti Sa’diah), was also awarded Malaysia’s CEO of the year for 2009 (News Straits Times, 2010). In 2008, however, the effect of the US financial crisis was felt in many countries, including in Europe. While its impact on Malaysian economy was not profound in early 2008, the economy could be more affected later due to the nation’s trade and investment linkages with countries affected by the crisis. By 2009, the Malaysian economic situation had experienced some distress over the financial downturn (Mahani and Rasiah, 2009). Given this situation, the demand for KPJ’s hospital services, which mainly targeted affluent segment of the market, could be expected to decrease. Furthermore, despite the growth in the Malaysian medical tourism sector, the number was expected to shrink by approximately 10 percent due to the world economic downturn in 2008 (Ang, 2009). Hence, the demand for KPJ’s hospital services, which targeted the medical tourism segment of the market, could be expected to decrease. By the end of 2009, pressure was mounting on Siti Sa’diah and her management team to make urgent decisions on how to survive the economic slowdown and grow the company’s business. The team had three options: 1. KPJ Healthcare Group could expand its business by focusing on the medical tourism market, which was expected to continue growing in the next few years; 2. KPJ could expand its college business, in particular because of the need to provide nurses to its own hospitals and also to support overall rapid expansion of the medical markets (Barnett et al., 2010); or 3. KPJ could further expand its international market. In thinking about its growth strategies, KPJ’s management team also had to address the issue of funding the business expansions. In 2006, in the effort to raise funds for its business expansion, KPJ initiated a major shift in its corporate strategy from being an entirely asset-based company to one that stayed light on its assets through securitization. This was accomplished with the establishment Al-‘Aqar KPJ Real Estate Investment Trusts (REIT), which had played an important role in facilitating KPJ’s strategic expansions (KPJ VOL. 3 NO. 4 2013, pp. 1-20, Q Emerald Group Publishing Limited, ISSN 2045-0621 j EMERALD EMERGING MARKETS CASE STUDIES j PAGE 1 Healthcare, 2005). The team wondered if this financing strategy is the best option to support the company’s future expansion. Overview of the Malaysian healthcare industry up to 2009 This section first presents a brief background information on Malaysia and general information on the development of healthcare industry; it then provides brief descriptions on the sectors of hospital operations, medical tourism, and nursing education. Malaysia in brief Malaysia is located in Southeast Asia and has a land area of approximately 330,000 km2. The country comprises of Peninsular Malaysia and East Malaysia, which is made up of 13 states and three federal territories. By 2010, Malaysia had a population of slightly less than 29 million people; approximately one-third of the population was below the age of 18 and about 5 percent was over 65 years old (MyCC, 2012). Malaysia had progressed from mainly a producer of raw materials into a full-fledged emerging economy, while also rapidly attracted investments of multinational corporations especially since the 1980s. In 2010, the country’s economy comprised of services sector, 48.2 percent, manufacturing sector, 41.4 percent, and agriculture sector, 10.5 percent (MyCC, 2012). Healthcare industry in Malaysia The Malaysian healthcare industry was divided into two sectors, the public and the private health care sectors, both of which were expanding rapidly. The public healthcare program, which was subsidized by the government, was used by the majority of Malaysians. The private commercial healthcare sector, on the other hand, was mainly targeted at the affluent segment of the population. Even though private healthcare providers had existed before the 1970s, their contribution in the healthcare services was not significant as the Malaysian Government was the main healthcare provider (Rasiah et al., 2011). The more affluent Malaysians would go abroad for treatments that were not available in Malaysia. Since the 1980s, the Malaysian Government began to seriously promote heavy investment in strategic industries among the private sectors, and the healthcare industry was one of the industries that took this challenge seriously. Profit seeking had resulted in high growth in the private healthcare service. Incidentally, the percentage of affluent consumers increased, which then leads to higher demand for customer service in healthcare. By 1982, the government’s policy to expand the private healthcare sector was in line with private investment in other public amenities such as power, water, telecommunication, and public healthcare (Rasiah and Ishak, 2001 cited in Rasiah et al. (2011)). At the same time, the government’s share in overall healthcare financing continued to decrease while investments by state development corporations and expenditures of other governmentlinked conglomerates increased through their investment in hospital operations. In 1991, healthcare was included in the Malaysian Privatization Master Plan (EPU, 2001; Rasiah et al., 2011). Since then, the private healthcare sector began to experience rapid growth. Hospital operations industry By the end of 2009, about 70 percent of the healthcare services in the country were provided by the public healthcare system, while 30 percent was provided by the private healthcare system. Correspondingly, private healthcare expenditures continue to rise over the years and exceeded public healthcare expenditures by the late 2000s (Rasiah et al., 2011). The number of private hospitals increased from 50 with about 2,000 beds in 1980, to about 210 with 10,000 beds in 2009. In the same year, approximately half of the 25,000 doctors and 30 percent of the 54,000 nurses in the country were employed in the private sectors, while the remaining was employed in the public sector (Chan, 2010). The private hospitals generally targeted the affluent segment of the market and focused more on customer service in comparison to the public hospitals. In return for their services, many private hospitals charged high consultation and treatment fees. The competition for health professionals between public and private hospital was high. However, better pay and j j PAGE 2 EMERALD EMERGING MARKETS CASE STUDIES VOL. 3 NO. 4 2013 work environment in the private hospitals (mainly from the high fees that they charged), gave them an advantage in attracting the professionals (Dahlui and Aziz, 2012). By 2009, Malaysian hospitals were also treating a significant number of foreign patients. In 2008, an estimated 400,000 foreign patients were treated at Malaysian hospitals; this number was forecasted to increase by 20 percent each year (Chan, 2010). In 2009, the Malaysian healthcare industry was estimated to be worth RM25.2 billion (USD8.4 billion). In the same year, approximately 4.3 percent of the country’s GDP was allocated to the healthcare sector (MGCC, 2011). In addition to getting treatment at hospitals, Malaysians also visited traditional medicine practitioners that included Chinese, Indians, Malays, and homeopathy medicine. These treatments were mostly complementary to modern medicine or medical services provided by the hospitals. Most Malaysians sought treatments at the hospital for curative type service. Generally, a small hospital could evolve from a small clinic operation. To be established as a group of hospitals with goodwill and branding, however, would take some time. For example, KPJ Group took about 20 years to establish its name in the market, while Pantai Hospital Group, the second largest hospital chain in Malaysia had been in the market for 30 years. Medical tourism sector Medical tourism can be defined as ‘‘patient movement from highly developed nations to less developed areas of the world for medical care, bypassing the services offered in their own communities’’ (Wikipedia, 2013). Especially since the 1990s, this industry had evolved into an important business in Asia and had experienced high growth since then (Rasiah et al., 2011). The promotion of Malaysia as a healthcare hub for traditional remedies and modern medical treatment contributed to the further development of private hospital provider market into the 2000s (EPU, 2006, 2010). Even though medical tourism in Malaysia was lagging behind the established neighboring medical tourism countries such as Singapore and Thailand, it had evolved into an affordable and highly developed healthcare hub in Asia (Ang, 2009). In fact, despite the decline in global economy, medical tourism in Malaysia had emerged as one of the fastest growing healthcare segments in the last few years (The Borneo Post, 2013). The number of foreigners visiting Malaysia for medical tourism had grown three times since 2003, reaching a total of about 340,000 tourists in 2007 with revenues of about RM250 million (USD83 million) (Ang, 2009). In 2009, the medical tourism revenue had increased to about RM290 million (USD97 million) (William, 2011), with increasingly large numbers of private hospitals in Malaysia actively participating in the sector. The industry aimed to receive around two million medical tourists by the year 2020 (ETP, 2012). Most medical tourists in Malaysia were from neighboring countries such as Indonesia (69 percent) and Singapore (12 percent). Other medical tourists were from Japan, Australia, the UK, the Gulf Cooperation Council (GCC), and European countries. The medical treatments sought by these patients included cardiac, cosmetics, ophthalmology, dental, diagnostic services, and orthopedics (ETP, 2012). Travelling overseas to obtain healthcare services is not entirely a new phenomenon, but increased globalization, advances in technological innovation, savviness of global citizens, and higher mobility resulted in many healthcare services increasingly accessible across the borders. Increased globalization, as well as improved logistics of human and information enabled the quality of healthcare service to become more standardized (Segouin et al., 2005). Moreover, the World Trade Organization (WTO) had undertaken various efforts to reduce trade barriers and promote cross-border investments, which had encouraged trade in industries, including in the healthcare services. All these had provided opportunities for healthcare operators who were prepared to venture beyond their home base to internationalize their operations and/or attract patients to their home operations. In addition to these specific healthcare measures, developments in other areas had also strengthened the integration of healthcare services in ASEAN countries. For example, the implementation of visa exemption for intra-ASEAN travel by ASEAN nationals had reduced the hassle of cross-border travelling. Additionally, the liberalization of air travel within the j j VOL. 3 NO. 4 2013 EMERALD EMERGING MARKETS CASE STUDIES PAGE 3 region had reduced the cost of air travel while improvement in flight services had resulted in a more convenient intra-region travel (ASEAN, 2012). Malaysia had been aggressively promoting medical tourism in the last one decade. In 2010, 35 private hospitals were promoting their services throughout the country; 85-90 percent of the patients was from the ASEAN countries and about 10-15 percent was from Japan, Australia, the UK, the Middle East and Europe. Patients from the USA and Canada were also showing increasing interests in medical tourism. By 2008, the arrival of health tourist increased to approximately 370,000, generating a revenue of approximately RM300 million (USD100 million), from 340,000 tourists and revenues of about RM250 million (USD83 million) recorded in 2007 (MGCC, 2011). Among others, Malaysia’s stable political climate, comparable medical service costs and quality, as well as competitive pricing put the country in a good position to attract a bigger share in the medical tourism sector (Dahlui and Aziz, 2012). Nursing education sector Although there was a significant increase in the number of nurses from about 20,000 in 1996 to about 48,000 in 2006, Malaysia still faced a critical shortage of nurses (Ministry of Health Malaysia, 2007; Barnett et al., 2010). Malaysia would require 174,000 nurses by the year 2020 to reach the targeted nurse to population ratio of 1:200 required by the World Health Organization (The Star, 2004; Barnett et al., 2010). Malaysia needs to overcome this shortage to provide high quality healthcare services and also be in a competitive position. There was a large demand for qualified nurses both locally and internationally, and shortage of nurse was a worldwide problem (The Star, 2004; Kingma, 2007). Countries such as the UK, the USA, and the Middle East also relied on nurses from other countries, including Malaysia (The Star, 2004; Barnett et al., 2010). Malaysia was one of the selected providers of nurses due to the comparatively low salary, good education background, high English fluency, and good clinical practices exposures (Barnett et al., 2010). However, in 2006, there were only about 48,000 trained nurses in Malaysia (Ministry of Health, 2007) and this had resulted in Malaysian hospitals hiring foreign nurses from other countries including from India and Philippines (eTawau, 2013). In the effort to overcome the shortage of nurses, Malaysian authority had identified nursing as a critical field and encouraged public and private institutions to provide nursing courses and increase their intake of nursing students. The Malaysia Government allocated a special fund which provided almost a 100 percent loan to nursing students (eTawau, 2013). In 2005, about 50 higher education institutions provide nursing education and about 30 private nursing colleges were established (eTawau, 2013). Masterskill Education Group Berhad (MEGB), which was incorporated in 1997, was a premier provider of nursing education in Malaysia (Nursing School, 2010). Another player in this industry was MAHSA College (Kolej Medikal Ahli Sains Bersekutu) which was established in 2004. This college offered diploma as well as degree programs in nursing, including twinning programs with Teeside University and Northumbria University in the UK (Nursing School, 2010). Another institution which provides nursing education was Nilai University College which was established in 1988. Its nursing programs had received accreditation from leading universities in the UK, Australia, New Zealand, Switzerland and Canada (Nursing School, 2010). KPJ Healthcare Berhad, 1979-2009 The history of KPJ Healthcare Berhad began in 1979 as a healthcare division of the Johor Corporation (JCorp). In 1968, JCorp was established as a State Investment Corporation in Johor, Malaysia. It was among the largest conglomerates in Malaysia, with core businesses in industries of palm oils, foods and fast-food restaurants, specialist healthcare services, hospitality, property and logistic/services (JCorp, 2011). In 1979, KPJ Healthcare Berhad began to develop the concept for Johor Specialist Hospital. After two years of development and construction, the Johor Specialist Hospital began its operation in 1981. It was the first private hospital in the state of Johor. In 1988, the division was incorporated as a private limited company under the name of Kemajuan Intisari, and assumed its present name in 1989. In 1988, the company acquired the Tawakal Hospital in Kuala Lumpur which was facing serious j j PAGE 4 EMERALD EMERGING MARKETS CASE STUDIES VOL. 3 NO. 4 2013 financial problems (KPJ Healthcare, 2009b). In 1989, KPJ acquired the Ipoh Specialist Hospital in Perak. In the same year, Datin Paduka Siti Sa’diah was appointed as the company’s CEO. In 1990, KPJ acquired the Kuantan Specialist Hospital in Pahang. Later, in 1991, it acquired some shares in Pusat Pakar Utara, which later changed its name to Kedah Medical Centre. In the same year, KPJ opened its Puteri Nursing College with the objective of providing nursing education and providing the human resources required by its group of companies and also the country. In 1993, KPJ acquired a medical centre in Johor which later changed its name to Puteri Specialist Hospital. In 1994, KPJ Healthcare Group was listed on the main board of Kuala Lumpur Stock Exchange (KLSE) (KPJ Healthcare, 2005). In 1995, the group’s construction of Ampang Specialist Hospital was completed and the hospital was opened for operation. KPJ then partnered with Penawar Hospital through a joint-venture agreement of 30-70 percent share (KPJ Healthcare, 2005). In 1995, KPJ entered into a contract to manage Rumah Sakit (RS) Selasih Hospital in Padang, a province on the island of Sumatera, Indonesia. In 1996, KPJ began to manage RS Medika Permata Hijau in Jakarta, the capital city of Indonesia. By 1997, it added Damansara Specialist Hospital to its hospital portfolio. In 1998, KPJ partnered with JCorp to develop and operate Klinik Waqaf An-Nur. This program was part of JCorp’s CSR initiative. In the year 2000, KPJ purchased Medical Specialist Centre in Penang, which was later known as Bukit Mertajam Specialist Hospital. In 2002, KPJ established a joint-venture project with the Kelantan State Economic Development Corporation to operate the Perdana Specialist Hospital in Kota Bharu, Kelantan. In 2002, KPJ established a subsidiary, Pharmaserv Alliances, which functioned as a wholesaler and distributor of pharmaceutical, medical product, and other hospital related products focusing on servicing KPJ-owned hospitals. In 2003, KPJ operated its first hospital in East Malaysia, the Kuching Specialist Hospital (KPJ Healthcare, 2005). In 2004, KPJ signed an agreement with the United Group Bangladesh to offer consultation and commissioning services to the United Hospital in Dhaka. KPJ then signed a contract with the United Group to manage the United Hospital which comprised of 450 beds. In 2004, KPJ jointly operated the Seremban Specialist Hospital with Majlis Islam Negeri Sembilan. In 2005, KPJ acquired 65 percent equity in Damai Specialist Centre in Kota Kinabalu, Sabah, a state in East Malaysia. In 2006, KPJ acquired 60 percent shares in Selangor Medical Centre and 75 percent of PT Khasanah Putera, Jakarta. In 2007, KPJ signed a contract to deal with management services at two private hospitals in Saudi Arabia, the New Jeddah Clinic Hospital and the Jeddah Clinic Hospital Kandarah (KPJ Healthcare, 2007). Figure 1 shows the organization structure of KPJ Group by the end of 2009. It shows that all of KPJ’s subsidiaries are hospital operations or hospital-related services which include one nursing education academy, two pharmaceutical distributions companies, and other hospital supporting facility providers (Figure 1). By the end of 2009, all of KPJ’s hospital operations provided general medical and specialists treatments and services. By then, KPJ Group employed 680 medical consultants (doctors and specialists) and about 7,000 staff; approximately half of them were nurses and allied health personnel while the remaining half were support staff. The company had spent about RM7.5 million (about USD2.5 million) in human capital development to support its operations. The group had served two million patients and about 15,000 (about 1 percent) of them were medical tourists (KPJ Healthcare, 2009a). In 2005, the value of the global healthcare travel market was USD20 billion, and at the end of 2009, it was estimated that the value would grow to between USD40 and USD60 billion by 2010. KPJ Group recognized medical tourism as a potential source of revenue and growth. The group had obtained all the necessary accreditations for its hospitals and had conducted extensive promotions in its targeted overseas’ markets. KPJ had also established links with insurance providers abroad, operated patient referral centers, and strengthened its online marketing system. At the same time, the Malaysian Government had recognized medical tourism as a strategic tourism sector. For example, the government had set up the Malaysia Healthcare Travel Council (MHTC) that support networking among relevant groups with the objective of promoting growth in medical tourism (KPJ Healthcare, 2009a). j j VOL. 3 NO. 4 2013 EMERALD EMERGING MARKETS CASE STUDIES PAGE 5 Figure 1 Organization structure of KPJ Group, end of 2009 Source: KPJ Healthcare (2009a) In 2009, KPJ had set a mission to deliver quality healthcare services through achieving ‘‘cohesiveness within the group and creating high standards of personal excellence’’ (KPJ Healthcare, 2009a, p. 30). Specifically, in 2007, its five-year plan was to achieve revenues of RM2 billion (about USD0.7 billion) by 2012. In achieving this plan, the company had operationalized two goals: 1. increase the number of hospitals; and 2. expand internationally (KPJ Healthcare, 2009a). Financing KPJ’s growth: 2006-2009 In early 2006, KPJ initiated a financing option, the REIT, to support its strategic expansion initiatives and submitted the application to the Securities Commission. On 24 July 2006, KPJ launched the Al-‘Aqar KPJ REIT, which was listed on the Bursa Malaysia on 10 August 2006. As an investment vehicle, the Al-‘Aqar REIT invested primarily in ‘‘Syariah-compliant’’ income-producing real estate and provided returns to its unit-holders using the income streams from its property portfolios (KPJ Healthcare, 2006). ‘‘Syariah-compliant’’ instrument refers to all types of investments that meet the requirement specified by the Islamic law. KPJ included six hospital buildings into the Al-‘Aqar REIT for a consideration of RM461.25 million, which was a 4.12 percent discount from the market value. With this asset liquidation, KPJ had agreed to accept a 47.06 percent stake in Al-‘Aqar REIT in the form of REIT units in addition to the portion paid in cash. KPJ made a long-term lease agreement of 15 years with Al-‘Aqar REIT to use hospital buildings as well as an option for renewal for another 15 years with increasing rental rate. KPJ had also agreed to bear all maintenance costs for the leased hospital buildings. The six hospitals properties comprised two hospitals in Johor, the Johor Specialist Hospital and Puteri Specialist Hospital; three hospitals in Selangor, the Ampang Puteri Specialist Hospital, Damansara Specialist Hospital and Selangor Medical Centre; and one hospital in Perak, the Ipoh Specialist Hospital (Al-‘Aqar KPJ REIT, 2006). Al-‘Aqar KPJ REIT played a vital role in supporting KPJ’s expansion. The strategy of injecting hospital properties into Al-‘Aqar KPJ REITallowed KPJ to unlock its asset values and ease up its cash flow to fund new hospital developments and acquisitions. Since 2006, KPJ continued j j PAGE 6 EMERALD EMERGING MARKETS CASE STUDIES VOL. 3 NO. 4 2013 its effort to include five more hospital properties into Al-‘Aqar REIT, the Kuantan Specialist Hospital in Pahang, the Kedah Medical Centre in Kedah, the Perdana Specialist Hospital in Kelantan, the Sentosa Medical Centre in Kuala Lumpur, and the KPJ Kajang Specialist Hospital in Selangor. By the end of December 2008, with the two asset injection exercises, KPJ had unlocked its assets worth RM651.1 million. The third asset injection, which was completed in September 2009, had realized additional assets worth RM292 million from nine properties: Seremban Specialist Hospital, Taiping Medical Centre, Damai Specialist Hospital in Kota Kinabalu, Bukit Mertajam Specialist Hospital, KPJ Penang Specialist Hospital, Tawakal Hospital, and KPJ Tawakal Specialist Hospital (KPJ Healthcare, 2007, 2008, 2009a). Since the launching of Al-‘Aqar REIT, KPJ had injected more than RM1 billion worth of assets into Al-‘Aqar REIT which enabled KPJ to realize its properties values and cash flow. KPJ’s asset injections were used to reduce gearings to cut interest costs, fund working capital and capital expenditures, and implement strategic expansions and other developments (JCorp, 2011). KPJ’s shareholders net profit increased by 81 percent from RM41 million in 2006 to RM74.2 million in 2007. In the same year, the earnings per share (EPS) increased to 36 sen (Malaysian cent) per share against 20.3 sen (Malaysian cent) per share in 2006, while the return on equity (ROE) increased to 14 percent in 2007 from 8.4 percent in 2006. In 2008, KPJ profit before tax exceeded RM100 million; KPJ continued to perform well in 2009 and this has resulted in KPJ being listed in Malaysia’s top 100 companies based on market capitalization, which had reached about RM1.3 billion. In terms of economic value added (EVA), KPJ had also created good values for its investors. For the financial year ended 2006, 2007, 2008, and 2009, KPJ recorded EVA of RM9.1, RM23.4, RM43.2, and RM52.2 million, respectively, (KPJ Healthcare, 2006, 2007, 2008, 2009a). By 2009, Al-‘Aqar REIT had become one of KPJ’s key financing vehicles and it was expected to further facilitate KPJ’s business expansion. Al-‘Aqar REIT had enabled the unlocking of values of hospital and related properties to help KPJ raise funds to further expand and capitalize on strategic investment opportunities. This gave KPJ a distinct competitive edge in terms of its long-term strategic and financial needs (KPJ Healthcare, 2008). In short, Al-‘Aqar REIT served as an important financing vehicle for KPJ to unlock its capital investments in hospital buildings and redeploy them to other high yielding strategic business activities. Strategies for the future, 2009 and beyond Keywords: Service, Strategic management, Malaysia, Healthcare At the end of 2009, the CEO of KPJ Group, Siti Sa’diah, and her management team needed to make an urgent decision on the strategies to be pursued by the company. On hindsight, Siti Sa’diah and her team were satisfied with the group’s performance. They had benefited from the structural fundamental changes in society; ageing population, increasing lifestyle-related diseases, and rising middle-class group had contributed to the increased demand for healthcare services (Insider Asia, 2012). While the healthcare sector was a capital-intensive business, the group had established Al-‘Aqar KPJ to secure the capital required to support its growth. The gloomy economic situation, which affected the demands for the group’s upscale medical services, however, was not good news for the group. The team knew that this situation could result in lower revenues for the company, and might put the group’s plan to become the leading regional player in the healthcare business at risk. References Al-‘Aqar REIT Healthcare (2006), Annual Report 2006, available at: www.alaqar.com.my/index.php/ publications (accessed 16 January 2013). Ang, E. (2009), ‘‘Malaysian medical tourism growing’’, The Star, 14 February, available at: http://biz. thestar.com.my/news/story.asp?file¼/2009/2/14/business/3245091 (accessed 2 May 2013). ASEAN (2012), ASEAN Project Connectivity, Association of Southeast Asian Nations, available at: www. asean.org/resources/publications/asean-publications/item/asean-connectivity-project-informationsheets (accessed 2 May 2013). Barnett, T., Namasivayam, P. and Narudin, D.A.A. (2010), ‘‘A critical review of the nursing shortage in Malaysia’’, International Nursing Review, Vol. 57, pp. 32-39. j j VOL. 3 NO. 4 2013 EMERALD EMERGING MARKETS CASE STUDIES PAGE 7 (The) Borneo Post (2013), ‘‘Malaysia medical tourism sector has room to grow’’, The Borneo Post, 9 April, available at: www.theborneopost.com/2013/04/09/malaysia-medical-tourism-sector-has-room-to-grow/ (accessed 5 May 2013). Chan, L.J. (2010), ‘‘Malaysian medical milestones’’, Healthcare Malaysia, The Writer’s Publishing House, Ampang, pp. 15-17. Dahlui, M. and Aziz, N.A. (2012), ‘‘Developing health service hub in ASEAN and Asia region country report on healthcare service industry in Malaysia’’, in Tullao, T.S. and Lim, H.H. (Eds), Developing ASEAN Economic Community (AEC) into a Global Services Hub, ERIA Research Project Report 2011-1, ERIA, Jakarta, pp. 65-110. EPU (2001), Eighth Malaysia Plan 2001-2005, Economic Planning Unit, Government Printers, Kuala Lumpur. EPU (2006), Ninth Malaysia Plan 2006-2010, Economic Planning Unit, Government Printers, Kuala Lumpur. EPU (2010), Tenth Malaysia Plan 2006-2010, Economic Planning Unit, available at: www.pmo.gov.my/ dokumenattached/RMK/RMK10_Eds.pdf (accessed 16 January 2013). eTawau (2013), 4 Types of Nursing Colleges in Malaysia, available at: www.etawau.com/edu/ IndexCollegeNursing.htm (accessed 17 January 2013). ETP (2012), Inside Investor – Healthcare, Economic Transformation Programme, available at: http://etp. pemandu.gov.my/upload/InsideInvestor-Healthcare.pdf (accessed 17 January 2013). Insider Asia (2012), ‘‘Expansion, start up costs to cap margins’’, The Edge, 12 December, available at: www.theedgemalaysia.com/sports/227019-expansion-start-up-costs-to-cap-margins-.html (accessed 17 January 2013). JCorp (2011), Annual Report 2011, Johor Corporation, available at: www.jcorp.com.my/userfiles/file/ JCorpAR11Eng.pdf (accessed 16 January 2013). Kingma, M. (2007), ‘‘Nurses on the move: a global overview’’, Health Services Research, Vol. 42 No. 3, pp. 1281-1298. KPJ Healthcare (2005), Annual Report 2005, available at: http://kpj.listedcompany.com/misc/ar2005.pdf (accessed 10 January 2013). KPJ Healthcare (2006), Annual Report 2006, available at: http://kpj.listedcompany.com/misc/ar2006.pdf (accessed 10 January 2013). KPJ Healthcare (2007), Annual Report 2007, available at: http://kpj.listedcompany.com/misc/ar2007.pdf (accessed 10 January 2013). KPJ Healthcare (2008), Annual Report 2008, available at: http://kpj.listedcompany.com/misc/AR2008. pdf (accessed 10 January 2013). KPJ Healthcare (2009a), Annual Report 2009, available at: http://kpj.listedcompany.com/misc/AR2009. pdf (accessed 10 January 2013). KPJ Healthcare (2009b), ‘‘The billion ringgit woman’’, KPJ News, 13 December, available at: www. kpjhealth.com.my/news-detail.php?id¼148 (accessed 16 January 2013). Mahani, Z.A. and Rasiah, R. (2009), The Global Financial Crisis and the Malaysian Economy: Impact and Responses, UNDP, Kuala Lumpur, available at: www.undp.org.my/uploads/undp%20report%20-the% 20global%20financial%20crisis%20and%20the%20malaysian%20economy.pdf (accessed 30 June 2013). MGCC (2011), The Healthcare Sector in Malaysia, Malaysian-German Chamber of Commerce & Industry, available at: http://malaysia.ahk.de/fileadmin/ahk_malaysia/Bilder/Others/Healthcare_ 2011__latest_3__-_Michelle_Lim.pdf (accessed 16 January 2013). Ministry of Health Malaysia (2007), Health Facts, available at: www.moh.gov.my/images/gallery/stats/ heal_fact/health_facts_2007.pdf (accessed 1 May 2013). MyCC (2012), Malaysia – Country Profile, Malaysia Competition Commission, available at: www.mycc. gov.my/files/advocacy/Malaysia-UNCTADPAper1.pdf (accessed 10 January 2013). News Straits Times (2010), ‘‘Malaysia’s CEO of the year’’, News Straits Times, 13 March, available at: www.btimes.com.my/Current_News/BTIMES/Econ2007_pdf/CEO%20of%20the%20Year%202009 (accessed 10 January 2013). j j PAGE 8 EMERALD EMERGING MARKETS CASE STUDIES VOL. 3 NO. 4 2013 Nursing School (2010), Nursing Colleges in Malaysia, available at: www.nursingcollegemalaysia.com/ college.html (accessed 20 January 2013). Rasiah, R., Abdullah, N.R.W. and Tumin, M. (2011), ‘‘Markets and healthcare services in Malaysia: critical issues’’, International Journal of Institutions and Economics, Vol. 3 No. 3, pp. 467-486. Segouin, C., Hodges, B. and Brechat, P.H. (2005), ‘‘Globalization in health care: is international standardization of quality a step toward outsourcing?’’, International Journal for Quality in Health Care, Vol. 17 No. 4, pp. 277-279. (The) Star (2004), ‘‘Rising demand for nurses not met’’, The Star, 31 August, available at: http://thestar. com.my/news/story.asp?file=/2004/8/31/nation/8790168&sec=nation (accessed 1 May 2013). Wikipedia (2013), Medical Tourism, available at: http://en.wikipedia.org/wiki/Medical_tourism (accessed 16 January 2013). William, R. (2011), ‘‘Drawing in the medical tourists’’, The Edge, 7 March, available at: www.theedgemalaysia. com/in-the-financial-daily/182852-drawing-in-the-medical-tourists.html (accessed 16 January 2013). Exhibit 1. Map of KPJ Hospital locations in Malaysia and Indonesia Figure E1 Source: KPJ Healthcare (2009a) About the authors Zizah Che Senik is an Associate Professor at Faculty of Economics and Management, Universiti Kebangsaan Malaysia, Bangi, Malaysia. Rosmah Mat Isa and Noreha Halid are Associate Professors at UKM-Graduate School of Business, Universiti Kebangsaan Malaysia, Bangi, Malaysia. Noreha Halid can be contacted at: noreha@ukm.my Adlin Masood is a Fellow at UKM-Graduate School of Business, Universiti Kebangsaan Malaysia, Bangi, Malaysia. Soo-Wah Low and Khairul Akmaliah Adham are Associate Professors at UKM-Graduate School of Business, Universiti Kebangsaan Malaysia, Bangi, Malaysia. j j VOL. 3 NO. 4 2013 EMERALD EMERGING MARKETS CASE STUDIES PAGE 9