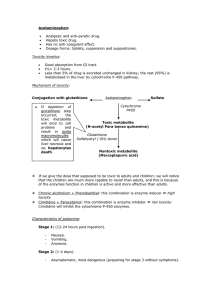
TOXICOLOGY LEC [PRELIMS] | S.Y 2023 – 2024 ● ● GUIDE QUESTION Knowledge of the toxicology of poisonous agents was published earliest in? a. b. c. d. e. Ebers Papyrus De Historia Plantarum De Materia Medica Lex Cornelia Treatise on Poisons and their Antidotes TOPIC OUTLINE I. History of Toxicology A. Antiquity B. 20th Century C. After World War D. 21st Century II. Principles of Toxicology A. Introduction B. Spectrum of Undesired Effects C. Characteristics of Exposure D. Dose-Response Relationship E. Variation in Toxic Response HISTORY OF TOXICOLOGY ANTIQUITY ● Ebers Papyrus ○ One of the oldest known writings ○ Contains information pertaining to many recognized poisons (hemlock, opium, lead, copper, antimony) ■ Opium - Papaver somniferum ○ Discovered in Egypt ○ Contains discussion on snake bites ● Hippocrates ○ Added a number of poisons and clinical toxicology principles to bioavailability in therapy and overdosage ● Theophrastus ○ A student of Aristotle ○ De Historia Plantarum (collection of plant sources) ● Dioscorides ○ Made the 1st attempt to classify poisons in De Materia Medica ○ A physician traveling Rome Paracelsus ○ Philippus Aureolus Theophrastus Bombastus von Hohenheim ○ A physician-alchemist who formulated many revolutionary views that remain integral structure of toxicology, pharmacology, and therapeutics ○ "All substances are poisons; there is none that is not a poison. The right dose differentiate a poison from a remedy” ○ Pioneered concepts: 1. Experimentation is essential in the examination of responses to chemicals 2. One should make a distinction between the therapeutic and toxic properties of chemicals 3. These properties are sometimes but not always indistinguishable except by dose 4. Once can ascertain a certain degree of specificity of chemicals and their therapeutic or toxic effect Magiendie, Orfila, & Bernard laid the groundwork for pharmacology experimental therapeutics, and occupational toxicology ○ Orfila - Spanish physician, Forensic toxicology ○ Magiendide - Physician and experimental physiologist who studied the MOA of emetine and strychnine ■ Cardiologist ■ Source of emetine - Ipecac ● Use: emetics ● Before, ipecac was widely used as a treatment for poisoning (not practiced now because it can do more harm) ■ Strychnine blocks glycine receptors ● Now used as insecticide but can cause muscle spasm ○ Claude Bernard - An introduction to the Study of Experimental Medicine 1 of 6 20TH CENTURY TOXICOLOGY ● 1850’s ○ Advent of anesthetics and disinfectants ■ Disinfectant - inanimate object ■ Antiseptic - animate ■ Joseph Lister - Father of antiseptics ● Applied phenol/carbolic acid to the wound of the mother during delivery ○ Prevalent use of “patent” medicines lead to several incidents of poisonings ● 1890’s ○ Discovery of radioactivity and vitamins, and start of Preclinical trials ● 1930’s ○ The National Institutes of Health (NIH) was established as a response to the tragic consequence of acute kidney injury after taking sulfonamide in glycol solutions ■ Ethylene glycol is used as an anti-freeze ■ Metabolized by alcohol dehydrogenase to glycolaldehyde. Glycolaldehyde is metabolized by aldehyde dehydrogenase to glycolic acid and can cause acidosis to the patient . Glycolic acid can also become oxalic acid which can precipitate inside the kidney leading to kidney injury AFTER WORLD WAR 2 ● 1950’s ○ Commitment of US FDA to toxicology (Ban any products found to be carcinogenic in lab animals or humans) ● 1960’s ○ Thalidomide → Phocomelia ; attempts to understand the effects of chemicals on the embryo and fetus ■ Thalidomide was marketed as treatment for morning sickness in Europe and it caused phocomelia. C deformity of hands & feet ■ Thalidomide → Pregnancy Category X; currently used for resistant leprosy 21ST CENTURY TOXICOLOGY ● Sequencing of the human genome and other organisms has markedly affected all biological sciences ● Deeper understanding of epigenetics has provided novel approaches in studying the fetal origin of adult diseases (cancer, diabetes, and neurodegenerative diseases). PRINCIPLES OF TOXICOLOGY ● ● ● ● ● ● ● ● INTRODUCTION TOXICOLOGY - Study of adverse effect of chemicals on living organisms Toxic substances can be classified based on its: ○ Origin (Toxins vs. Toxicant) ■ TOXINS - Naturally occurring harmful chemicals ■ TOXICANTS - Toxic substances that are produced or are by-product of human-made activities (synthetic) ■ XENOBIOTICS Foreign substances that include: a variety of synthetic chemicals (natural or synthetic) ○ Physical state (gas, dust, liquid) ○ Chemical stability (explosive, flammable, corrosive) ○ General chemical structure (aromatic amine, halogenated hydrocarbon) ○ Ability to cause significant toxicity (extremely toxic, very toxic, slightly toxic) ○ Mode of action (alkylating agents, cholinesterase inhibitors) TOXICOLOGIST - an individual trained to examine and communicate the nature of a toxicant's properties and identify approaches to prevent or mitigate harm done to human, animal, and environmental health MECHANISTIC TOXICOLOGIST - identifies the cellular, biochemical, and molecular mechanisms by which chemicals exert toxic effects on living organisms. ○ Study the mechanism of action HAZARD ASSESSMENT TOXICOLOGIST conducts toxicity testing that provides comprehensive information for the evaluation of a chemical's safety and to meet important regulatory requirements ○ Assess/test the possible hazard REGULATORY TOXICOLOGIST has the responsibility for deciding, on the basis of data provided by descriptive and mechanistic toxicologists, whether a drug or other chemical poses a sufficiently low risk (or, in the case of drugs, a favorable risk/benefit profile) to be marketed for a stated purpose. ○ Establish standards and policies (like FDA) COMPUTATIONAL TOXICOLOGIST - develop and implement computer-based models to predict adverse health effects resulting from the interaction of chemicals with biological organisms OCCUPATIONAL TOXICOLOGIST - responsible for conducting research and making recommendations for the prevention of work-related injury and illness 2 of 6 ○ ○ Company toxicologists Make standards and policies appropriate for work FORENSIC TOXICOLOGY - covers the medicolegal aspects of the deleterious effects of chemicals on animals and humans ○ The expertise of forensic Toxicologists is used to aid in establishing the cause of death and determining its circumstances in a post mortem investigation CLINICAL TOXICOLOGY - physicians who receive specialized training in emergency medicine and poison management ○ Do first aid ENVIRONMENTAL TOXICOLOGY - Focuses on the impact of chemical pollutants in the environment on biological organisms. ● ● ● CHECKPOINT 1 ● What is the difference between side effects and adverse effects? ○ Side effect - can be positive or side; not that harmful; cannot cause death ○ Adverse effect - deleterious; can cause death ● ● ● ● ● ● ● ● SPECTRUM OF UNDESIRED EFFECTS ALLERGIC REACTIONS - an adverse reaction of the immune system to a chemical in response to a previous exposure to that chemical or to a structurally similar one. ○ Genetic predisposition - if both parents are allergic to a specific substance, the baby is also allergic to that substance ○ Sensitization - patient must have a prior exposure to the substance ○ Once sensitization has occurred, allergic reactions may result from exposure to relatively very low doses of chemicals IDIOSYNCRATIC REACTIONS - abnormal reactivity of an individual to a chemical based on its genetics or other individual sensitivity factors. IMMEDIATE VS. DELAYED TOXICITY IMMEDIATE - occurs rapidly after a single administration DELAYED - occurs after a lapse of some time (months or years) REVERSIBLE VS. IRREVERSIBLE TOXICITY Depends of the ability of the injured tissue to adapt, repair, and regenerate ● LIVER & GIT - reversible ● CNS & Heart - irreversible ● ● ● ● ● ● ● ● ● ● Labile - unlimited regenerative capacity (skin) Quiescent - limited regenerative capacity (liver) Permanent - no regenerative capacity (brain) LOCAL VS. SYSTEMIC TOXICITY LOCAL - site of first contact between the toxicant and biologic substance SYSTEMIC - absorption and distribution of toxicant from its entry point to a distant site at which deleterious effects are produced CHEMICAL INTERACTIONS ADDITIVE - Combined response of 2 chemicals are equal to the sum of responses to each chemical given alone (e.g., 2 + 3 = 5) SYNERGISTIC - Combined response of 2 chemicals are much greater than the sum of the responses to each chemical when given alone (e.g., 2 + 2 = 20) POTENTIATION - None substance does not produce any toxicity on a particular tissue or system but when added to another chemical makes that chemical much more toxic ○ Drug B is non toxic but once you co-administer it with Drug A, it becomes toxic ANTAGONISM - occurs when two chemicals administered together interfere with each other's actions or one interferes with the action of the other ANTAGONISM RECEPTOR ANTAGONISM - occurs when two chemicals that bind to the same receptor produce less of an effect when given together relative to the addition of their separate effects. Often termed as blockers ○ Pharmacologic Antagonism CHEMICAL ANTAGONISM - direct chemical reaction between two compounds that produces a less toxic product ○ Antagonism will directly bind with the poison/toxin ○ Heparin and protamine sulfate → neutralization reaction DISPOSITIONAL ANTAGONISM - occurs when the absorption, distribution, biotransformation, or excretion of a chemical is altered so that the concentration and/or duration of the chemical at the target organ is reduced ○ Inhibitors FUNCTIONAL ANTAGONISM - occurs when two chemicals counterbalance each other by producing opposing effects on the same physiological function, often through different signaling pathways ○ Physiological Antagonism 3 of 6 ● ● ● ● TOLERANCE TOLERANCE - Repeated exposure to a chemical can reduce its pharmacologic and/or toxicologic actions ○ Chronic exposure to a toxicant or drug will lead to down-regulation (reduce in pharmacologic or toxicologic effect) CROSS-TOLERANCE - Occurs when structurally related chemicals cause diminished responses. ○ If you are tolerant to lorazepam, you are also tolerant to clonazepam since they have the same structure DISPOSITIONAL TOLERANCE - Occurs when the amount of chemical reaching the site of action decreases over time, leading to the reduced responsiveness of the tissue to stimulation CHEMICAL/CELLULAR TOLERANCE - May result from a lower availability of receptors and/or mediators CHECKPOINT 2 ● What is the difference between tolerance and tachyphylaxis? ○ Both are a result of chronic exposure ○ Tolerance → down-regulation happens slowly ○ Tachyphylaxis → down-regulation happens rapidly ● ● ● ● Why do most injuries in the liver due to toxicants are reversible? Recall a drug that can cause damage to the brain/CNS. ○ Because they have limited regenerative capacity ○ Example is Paracetamol ■ Toxic metabolite of paracetamol is NAPQI (N-acetyl-parabenzoquinone imine) ■ Chemical name: N-acetyl-paraaminophenol ■ Toxic dose of paracetamol: more than 4 grams ■ Treatment of choice is n-acetylcysteine Why do most injuries in the brain due to toxicants are irreversible? ○ Because they have no regenerative capacity CHARACTERISTICS OF EXPOSURE Toxicity to a biological system requires that sufficient concentration: of the "active" form of a chemical accumulate at the site of action for a requisite period of time To characterize fully the potential hazard of a specific chemical, one needs to know not only the type of effect it produces, and the dose required to produce that effect, but also the information about the chemical, route of exposure, and disposition. ● ● ● ROUTE AND SITE OF EXPOSURE The vehicle or the inert material in which the toxicant is dissolved, and other formulation ingredients can markedly alter chemical absorption after ingestion, inhalation or topical exposure In addition, the route of administration can influence the toxicity of chemicals An approximate descending order of effectiveness for the route of exposure would be: ○ Intravenous > Inhalation > Intraperitoneal > Subcutaneous > Intramuscular > Intradermal > Oral > and Dermal ■ Intraperitoneal → within or administered through the thin, transparent membrane that lines the walls of the abdominal DURATION AND FREQUENCY OF EXPOSURE ACUTE EXPOSURE - <24 hours; Single Administration ● SUBACUTE EXPOSURE - 1 month or less; repeated exposure ● SUBCHRONIC EXPOSURE - 1 to 3 months; repeated exposure ● CHRONIC EXPOSURE - >3 months; repeated exposure ● Why is it important to determine the type of exposure? ● So that we can do proper treatment ● Acute exposure to benzene will cause CNS depression but if you are exposed chronically, it can cause leukemia ● ● DOSE-RESPONSE RELATIONSHIPS GRADED-DOSE RESPONSE RELATIONSHIP Response of an individual organism to increasing doses of a chemical (individual-dose response) QUANTAL-DOSE RESPONSE RELATIONSHIP Characterizes the distribution of individual responses to different doses in a population of organisms GRADED-DOSE RESPONSE RELATIONSHIP Response of a particular receptor-effector system against increasing concentration of drug ● Relationship of drug concentration and effect ● Efficacy and potency parameters can be derived ● EFFICACY ○ Maximal effect a drug can produce ○ Represented by Emax ● POTENCY ○ Amount of drug required to produce a specific effect (50%) ○ Represented by EC50 (dose that causes 50% of maximal effect) in graded ● 4 of 6 ○ dose-response and ED50 in quantal dose-response curve The lower the EC50, the more potent the drug is ○ ○ ○ ○ ○ ○ ○ ○ ● ● ● ● Drug A is more effective than Drug B since it has a higher Efficacy than drug B. Both drugs have different potency as well. ● ● The 2 drugs both have different potency but they have the same ceiling dose (same efficacy). Drug A is more potent than drug B which means that drug A can produce the effect with a lower dose than drug B. QUANTAL-DOSE RESPONSE RELATIONSHIP Minimum concentration needed to produce a specific response in each member of a population ● Median effective dose (ED50), Median toxic dose (TD50), and median lethal dose (LD50) can be derived ○ The lower the LD50, the more lethal the poison is ● Maximal effect of drug is not determined (vs. Graded dose-response) ● THERAPEUTIC INDEX ○ Ratio of TD50 and ED50 ● THERAPEUTIC WINDOW ○ Range between TD50 and ED50 ● NARROW THERAPEUTIC INDEX DRUGS (WALA Cyang PaPa VasTeD pa!) ○ Warfarin ○ Aminoglycosides ● ● ● Lithium Amphotericin B Carbamazepine Phenytoin Phenobarbital Vancomycin Theophylline Digoxin VARIATION IN TOXIC RESPONSES Selective Toxicity Modifying Factors ○ Genetics (Genetic Polymorphism) ○ Age ○ Sex ○ Circadian Rhythm ○ Microbiome ANIMAL TESTING ACUTE TOXICITY TESTING ○ Typically performed in rodents ○ These studies aim to approximate the LD of a chemical within 14 days after a single exposure ○ Approaches to determine the doses and dosing includes: fixed dose (OECD 420), stepwise method (OECD 423), up-and-down procedure (OECD 425) SUBACUTE TOXICITY TESTING ○ Determine toxicity of a chemical after repeated administration ○ 10 animals/sex/dose (rodents). 3-4 animals/sex (dog) ○ 14 or 28 days DEVELOPMENTAL & REPRODUCTIVE TOXICITY ○ DEVELOPMENTAL TOXICOLOGY - study of adverse effects on the developing organism occurring any time during the life span of the organism that may result from exposure to chemical or physical agents before conception (either parent), during prenatal development, or postnatally until the time of puberty ○ REPRODUCTIVE TOXICOLOGY - study of the occurrence of adverse effects on the male or female reproductive system that may result from exposure to chemical or physical agents ○ TERATOLOGY - the study of defects induced during development between conception and birth SUBCHRONIC TOXICITY TESTING ○ Determines the no observable adverse effect level (NOAEL), lowest observable adverse effect level (LOAEL) organ involvement 5 of 6 ○ Conducted in 2 species (rat & dog for FDA, & rat or mouse for EPA) ○ 90 days (most common test duration) CHRONIC TOXICITY TESTING ○ Performed similarly to subchronic studies except the period of exposure is longer than 3 months ■ 6 months - 2 years in rodents ■ 1 year (or longer) in nonrodent species NEUROTOXICITY ASSESSMENT IMMUNOTOXICITY ASSESSMENT EYE AND SKIN IRRITATION AND CORROSION ● ● ● ● (Memo since it will be included in the exam↓) FDA DRUG RISK CLASSIFICATION CATEGORY Warfarin, Statins Methotrexate, ADR TYPE OF EFFECT CHARACTERISTICS EXAMPLE A Augmented Dose-dependent (Predictable) Hypoglycemia from insulin B Bizarre Dose-independent (Unpredictable) Anaphylaxis Aspirin-induced asthma C Chronic Use Prolong treatment (Long term exposure) D Delayed After years of treatment Carcinogenesis E End of Use Occurs after withdrawal Cushing syndrome after abrupt discontinuation of corticosteroids F Failure of Therapy ● Augmented - as you increase the dose, the effect also increases DESCRIPTION A Controlled studies in humans show no risk to the fetus B No controlled studies have been conducted in humans; animal studies show no risk to the fetus C No controlled studies have been conducted in animals or humans D Evidence of human risk to the fetus exists; however, benefits may outweigh risks in certain situations X X (Absolute Contraindication) Pregnancy after using oral contraceptive pills Controlled studies in both animals and humans demonstrate fetal abnormalities; the risk in pregnant women outweighs any possible benefit CATEGORY A (Safe) EXAMPLE Levothyroxine, Folic Acid Levo fo B (Prescribed only as needed for maternal health) Metformin, Hydrochlorothiazide C (Prescribed only in pregnancy if benefit clearly outweigh the risks) Tramadol, Gabapentin D (Not recommended in pregnancy; prescribed if absolutely necessary) Alprazolam, Clonazepam Met Hy Tra Gab AlClo 6 of 6 4. Inappropriate repair and adaptation *toxicity is usually noteworthy at steps 3 and 4 ● GUIDE QUESTION Toxication (or metabolic activation) is the biotransformation of a toxicant to a more toxic and reactive species. Which of the following is not a reactive chemical species commonly formed by toxication? a. b. c. d. e. ● ● ● ● ● Electrophiles Nucleophiles Superoxide anions Hydroxy radicals Hydrophilic organic acids DELIVERY TO THE TARGET Before it reaches the target molecule, the toxicant is absorbed, distributed, eliminated, and activated Exposure at the target site is an absolute requirement for any mechanism of toxicity Xenobiotic disposition ○ Defined as the absorption, distribution, biotransformation, and elimination of a toxicant ○ Critical determinant of target organ toxicity along with sensitivity of target sites to toxicity INTRODUCTION Mechanism of toxicity describe how an adverse effect occurs Knowledge of mechanisms of toxicity is essential for developing risk assessments for chemical exposure, as such data are relevant to determining the likelihood that chemical exposure may cause harmful effects Mechanistic toxicology data are also useful for developing more predictive biomarkers of toxicity, developing approaches to antagonize or prevent toxicity, and gaining insight into fundamental physiologic, biochemical, and molecular processes that underlie normal and abnormal organ function ● ● Shows us what will happen if we are exposed to a toxicant 4 critical events 1. Delivery of the toxicant to the target organ 2. The interaction or the reaction of the toxicant with the target molecule 3. Cellular dysfunction and toxicity Body has a defense mechanism to protect us from the toxicant: ○ Presystemic elimination ○ Distribution away from target ○ Excretion ○ Detoxification ABSORPTION & PRESYSTEMIC ELIMINATION ● Absorption is defined as the process by which toxicants cross body membranes to enter the systemic circulation ● Absorption occurs along the entire length of the gastrointestinal tract and is usually determined by the extent to which the compound exists in its nonionized, lipid-soluble form ● In the skin, the stratum corneum layer of the epidermis is a major barrier to absorption, but once through this barrier, compounds are typically 7 of 15 absorbed by diffusion into the venous or lymphatic capillaries to enter the systemic circulation ● ● ● Presystemic elimination is a process by which a toxicant is eliminated prior to reaching the systemic circulation ○ Presystemic elimination in the git is also known as first-pass effect The gastrointestinal tract epithelium may eliminate or modify a compound directly Many toxicants absorbed from the gastrointestinal tract pass via the portal circulation directly into the liver where they are modified by biotransformation enzymes and excreted into bile DISTRIBUTION OF TOXICANTS OCCURS BY PASSIVE OR ACTIVE PROCESSES ● Tissue distribution is the process by which a toxicant reaches its target site ● Affected by 4 factors: ○ Porosity of the Capillary Endothelium ■ Liver sinusoid VS. BBB → liver highly fenestrated than BBB ■ Or fenestration of the capillary endothelium ● Butas butas sa capillary ○ Presence of Specialized Transport Processes Potential for Accumulation within Cellular Organelles Binding to proteins or Other Macromolecules ■ Acidic drugs/Toxicants → Albumin ■ Basic drugs/Toxicants → alpha-I-acid glycoprotein (orosomucoid) ■ Only free drugs or toxicants can exert their action. If a drug is bound to a macromolecule, it cannot bind to its receptor ○ ○ ELIMINATION PROCESS AFFECT DELIVERY OF TOXICANTS REABSORPTION AND EXCRETION ● Enterohepatic circulation → cycle in which a compound is excreted into bile to enter the intestine where it is modified to facilitate intestinal reabsorption rather than fecal elimination ○ Mostly, drugs and toxicants that underwent glucuronidation will favor enterohepatic circulation because they are mainly eliminated via the bile ○ Once the glucuronide reaches the intestine, where your gut bacteria is located, glucuronic acid is hydrolyzed with the action of beta glucuronidase facilitating the reabsorption of the toxicant or drug ● In the kidney, reabsorption mechanisms are highly pH-dependent, as the generally acidic milieu of urine favors reabsorption of weak acids. (Henderson-Hasselbalch Equation) ○ Acidic drugs are absorbable or reabsorbable in an acidic medium ■ If you want to excrete → alkalinize the urine ■ Ex. Aspirin - to facilitate its accretion, give sodium bicarbonate, a urinary alkalinizer. ○ Basic drugs are absorbable or reabsorbable in an basic medium ■ To excrete - acidify the urine. You cam give ammonium chloride, a urinary acidifier ● The route and rate of excretion largely depend on the physicochemical properties of the toxicant. The major excretory organs for non-volatile compounds are the liver and kidneys, which are most efficient at removing water soluble, usually ionized compounds ○ Toxicant, in order to be excreted, should be hydrophilic, charged, & ionized 8 of 15 ● ● ● ● The excretion of non-volatile highly lipophilic compounds is much less efficient than that of water soluble compounds. Biotransformation may facilitate elimination of these compounds, but other than processes of accretion of highly lipophilic compounds include accretion in the bile secretion directly into the intestinal contents, and excretion in milk lipids in mammary glands Volatile lipophilic compounds diffuse through pulmonary capillaries to be excreted in expired air Drugs or toxicants will undergo phase 1 and phase 2 metabolism in the liver. ○ Phase 1 aka functionalization because you have to expose the functional group of the drug or toxicant (reduction, oxidation, hydrolysis) ○ Phase 2 aka conjugation reaction because you have to add conjugates (sulfate group, methyl group, glucuronic acid) The reaction that is important in enterohepatic circulation is glucuronidation ○ Most drugs or toxicants that will undergo this type of reaction will be excreted t the bile ○ Once the bile reaches the large intestine, where the bacteria are mostly located, glucuronides will be hydrolyzed using an enzyme called beta glucuronidase ■ Present in our gut bacteria ○ Once the glucuronic acid is removed from the toxicant or the drug, it is reabsorbed in the hepatic portal vein papuntang systemic circulation TOXICATION AND DETOXIFICATION ● Although some xenobiotics are directly toxic, many others produce toxicity through metabolites formed following exposure. Biotransformation of xenobiotics that increases toxicity is referred to as metabolic activation or a toxification process ● ● Toxication process forms electrophiles, free radicals (superoxide, peroxidase, hydroxyl radicals), and Nucleophiles Detoxification: to be eliminated from the body more efficiently - must be hydrophilic and ionized ○ Electrophiles - conjugation with glutathione (a thiol nucleophile) ○ Free radicals - starts with superoxide dismutase (SOD), followed by catalase, glutathione peroxidase, or peroxidation ○ Nucleophiles - conjugation ○ No functional group - Phase I & Phase 2 REACTION OF THE ULTIMATE TOXICANT WITH TARGET MOLECULE ● Toxicity is initiated by a reaction between the ultimate toxicant and its target molecule, with subsequent events leading to dysfunction or injury ● Determinants of interaction of ultimate toxicant with the target molecule: ○ ATTRIBUTES OF TARGET MOLECULES ■ Ability to react with the target & adversely affect its function ■ Ability to reach an effective concentration at target site ■ Alter the target in way that is related to toxicity ○ TYPES OF REACTION ■ Noncovalent binding - between nonpolar interactions or the formation of H bond and ionic bonds; reversible ■ Covalent binding - irreversible and permanent (organophosphates action on Acetylcholinesterase) ■ Electron transfer - some chemicals can oxidize your ferrous iron to ferric (nitrites) ■ Enzymatic reaction - botulinum toxin can hydrolyze the fission proteins of Acetylcholine preventing the release of acetylcholine ○ EFFECTS OF TOXICANT ON THE TARGET MOLECULES ■ Dysfunction of target molecules (by binding of the toxicant to the receptor, mimicking the effect of indigenous ligands) ■ Destruction of target molecules (especially DNA to certain substances that can damage DNA) ■ Neoantigen formation (urushiol and penicillins are haptens; by themselves, they cannot produce allergic reaction, but once they combine with a protein in the body, 9 of 15 they become allergenic. They can induce allergic reaction) CELLULAR DYSFUNCTION & RESULTANT TOXICITIES ● Toxicity will emerge here - Atropine is an anticholinergic. Its effect is mostly sympathetic. - For atropine toxicity: Atropine toxicity can be treated by cholinergic substances like physostigmine Mode of action of BZD - increase frequency of GABA A receptor opening (Barbiturates increase the duration of GABA A receptors) When GABA A receptor is opened, it will lead to influx of chloride channel leading to hyperpolarization of the cell leading to sedation TOXICANTS THAT WILL ALTER CELLULAR REGULATION ● Cellular Dysregulation ○ Dysregulation of Gene Expression - - - There are several ligands, agonists, or hormones that can affect your gene expression. One of them is estrogen. Once estrogen binds to nuclear receptor, nuclear receptor will go inside the nucleus and will dimerize leading to transcription of different proteins There are several toxicants that can inhibit this function such as bisphenol A, nonylphenol, phthalate, DDT (Dichlorodiphenyltrichloroethane - used as insecticide but it was withdrawn because of its toxicity) Binding if endocrine disrupting chemicals following to the estrogen receptor result to estrogenic effect - ● Dysregulation of Ongoing Cellular Function ○ Toxicant-Neurotransmitter Interaction Another example of neurotransmitter toxicant interaction is the interaction between organophosphate and acetylcholinesterase. Acetylcholinesterase is an enzyme responsible for the breakdown of acetylcholine. If this is inhibited, Ach will remain in the synapse, leading to excessive parasympathetic activity. (SE: DUMBBELS) Symptoms of organophosphate poisoning can be treated by atropine. We can give pralidoxime if aging has not yet happened. 10 of 15 - Organophosphate, at a given time, will irreversibly inhibit acetylcholinesterase. Another example is cocaine, tricyclic antidepressants, and amphetamine. The main elimination of norepinephrine is via reuptake to your presynaptic vesicle, that’s in comparison to your acetylcholine (via degradation secondary to acetylcholinesterase) secondary to norepinephrine transporter. This is inhibited by cocaine, tricyclic antidepressants, and amphetamine. If inhibited, norepinephrine will remain at the synapse, leading to excessive sympathetic activity. ○ - Toxicant-Transducer Interactions DDT, pyrethroids, ciguatoxin (toxin from fish) act on voltage-gated Na+ channels. They facilitate the opening of the channel leading to neuronal activation and overexcitation and convulsion. CELLULAR DYSFUNCTION IN THE CELL MAINTENANCE Impaired Cellular Maintenance ● Impaired Internal Maintenance ○ Impaired ATP synthesis ■ ■ REVIEW/SEARCH for the other name of the complexes ● COMPLEX 1 = NADH oxidoreductase/dehydrogenase ● COMPLEX 2 = Succinate-CoQ reductase/dehydrogenase ● COMPLEX 3 = Q-cytochrome c oxidoreductase ● COMPLEX 4 = cytochrome c oxidase ● COMPLEX 5 = ATP SYNTHASE ● There are several toxicants that can inhibit your electron transport chain. An example is 2,4-Dinitrophenol and Aspirin overdose. They are called uncouplers. It increases permeability of cells facilitating the release of hydrogen ions needed for ATP synthesis. Complex I = (-) by Rotenone Complex III = (-) by Anti(three)mycin Complex IV = (-) by Azide, Cyanide (CN-), Carbon Monoxide (CO) (4 letters) Complex V = (-) by Oligomycin (5 letters) ○ Impaired Membrane Function ■ Ethanol and organic solvent increase membrane fluidity Impaired External Maintenance ○ Toxicities Interfering with Cells Specialized to Provide Support to Other Cells, Tissues or Whole Organism ■ Inhibition of hepatic synthesis of coagulation factors by coumarin and warfarin DYSREPAIR AND ADAPTATION MECHANISMS OF REPAIR ● MOLECULAR ○ Some chemical alteration (via oxidation) and are simply reversed (through reduction). ○ Other toxicants trigger misfolding of proteins. Proteins (enzymes) are typically folded into a globular form. Chaperone proteins (HSP90) prevents unfolding secondary to toxicants ● - Lipid solvents destroy plasma membrane Hydrocarbons destroy lysosomal membranes ● CELLULAR ○ Autophagic removal of damaged cell organelles (lysosomal process) - lysosomes are aka cell-eating organelles (autophagy self eating) TISSUE ○ Depends on the ability of the injured tissue to repair, and regenerate MECHANISMS OF ADAPTATION ● Adaptation is a biological process by which an organism develops increased tolerance to the harm itself. It involves responses acting to preserve or regain the biological homeostasis in the face of increased harm ● Theoretically, adaptation to toxicity may result from biological changes causing: ○ (1) Diminished delivery of the causative chemical(s) to the target, ○ (2) Decreased size or susceptibility of the target, 11 of 15 ○ ○ (3) Increased capacity of the organism to repair itself, and (4) Mechanisms to compensate for the toxicant inflicted dysfunction TOXICITY RESULTING FROM INAPPROPRIATE REPAIR AND ADAPTATION ● NECROSIS ○ Cell death ensues when repair mechanisms are inefficient or the molecular damage is not readily reversible. ○ Sometimes progression to tissue necrosis can be interrupted by apoptosis and cell proliferation. ● FIBROSIS ○ Fibrosis is characterized by excessive formation and deposition of connective tissue with abnormal composition of the ECM (extracellular membrane) ○ In general, fibrotic conditions can develop in any organ, but liver, lung, kidney and heart are noteworthy ○ fibrosis - usually in permanent cell or quiescent cells ■ due to no or limited regen cap. ● - Necrosis = pathologic; accompanied by an inflammation (pus); dirty Apoptosis = no inflammation and often physiologic; programmed cell death; no adjacent inflammation; step by step process CARCINOGENESIS Manifestations of Carcinogenesis (lead to tumor formation) ● Failure of DNA repair ● Failure of apoptosis ● Failure to terminate cell proliferation 12 of 15 ● ● GUIDE QUESTION Which of the following statements about weak base overdose is most correct? a. b. c. d. Urinary excretion would be accelerated by administration of NH4Cl, an acidifying agent Urinary excretion would be accelerated by giving NaHCO3, an alkalinizing agent Less of the drug would be ionized at blood pH than at stomach pH Absorption of the drug would be slower from the stomach than from the small intestine INTRODUCTION DISPOSITION ● Absorption, distribution, biotransformation, & elimination of chemical or xenobiotics ● Determines the toxicants concentration at the site of action TOXICOKINETICS ● Quantitative characterization of xenobiotic disposition ● Mathematical representation of disposition ○ Example: volume of distribution and half life ● Toxicants usually pass through cells ● Basic unit of cell membrane is a lipid bilayer composed primarily by phospholipids, glycolipids, & cholesterol ○ Polar heads – oriented towards outer and inner surface ○ Hydrophobic tails – oriented inward and face each other ○ Numerous proteins are inserted or embedded in the plasma membrane: ■ Integral protein- Transverse the whole bilayer. If it is removed, it will disrupt the plasma membrane. Hence, it is an integral part of the plasma membrane. ■ Peripheral action – It can be in the inner or outer surface only of the membrane. If it is removed, it will not disrupt the plasma membrane. ● Most of the toxicants, for them to exert effect, they must pass several barriers like the plasma membrane (composed of two →bilayer) PERMEATION Movement of drug/toxicant molecules into and within the biologic environment Before a drug can be absorbed, it must permeate DIFFUSION ● Movement of solutes from higher to lower concentration (downhill) ● Do not use transport proteins and energy (passive) ● Governed by Fick's law ○ Aqueous Diffusion ■ Across epithelial membrane tight junction and endothelial lining of blood vessel ○ Lipid Diffusion ■ Passive movement across the lipid bilayer TRANSPORT BY SPECIAL CARRIERS ○ NOT governed by Fick's Law ○ Facilitated Diffusion – Downhill, Passive → (SLC) ○ Active Transport – Uphill, Active → (ABC) ENDOCYTOSIS ● Type of movement of molecule if the molecule is very large ● Once a large molecule is in contact with plasma membrane, it will bind to a receptor which will trigger the engulfing of the plasma membrane = it will eat the molecule ● Other name is “cell eating” Diagram representing the different movement of molecules Simple diffusion and facilitated diffusion is the movement of molecules from high to low concentration = it will follow concentration gradient and will not use any energy Active transport is against the concentration gradient (from high to low concentration) and will use energy - Saturability 13 of 25 - - When all of the transport carriers or proteins are occupied, they cannot transfer any solute anymore. Active Transport It’s against the concentration gradient It uses transport protein and energy It is saturable Table 1. Human ABC Transporters: Gene Family Overview and Major Transporters Involved in Xenobiotic Disposition ABC Subfamily Genes in Family Gene Symbols A 12 ABCA1-10, 12, 13 B 11 ABCB1-11 C 13 ABCC1-13* D 4 ABCD1-4 E 1 ABCE1 F 3 ABCF1-3 G 5 ABCG1, 2, 4, 5, 8 FICK’S LAW OF DIFFUSION ● Predicts the rate of movement of molecules across a barrier ● Concentration and Surface area are directly proportional to rate of movement ○ ↑ Concentration and Surface area = ↑rate of movement across a membrane ● Thickness is inversely proportional to rate of movement ○ ↑Thickness = ↓ rate of movement across a membrane Question: Compare which has the higher solute movement: 50 mg Drug A or 500 mg Drug B. Answer: 500 mg Drug B Explanation: Since according to Fick’s Law, the higher the concentration, the higher the solute movement. HENDERSON-HASSELBALCH EQUATION 14 of 25 ● ● ● ● Electrostatic charge of an ionized molecule attracts water dipoles and results in the polar, relatively water-soluble and lipid-soluble complex. ○ Ionized (charged) → Polar molecules → lipid insoluble (Lipophilic, Hydrophilic) ○ Non-ionized (uncharged) → lipid soluble (Lipophilic, Hydrophobic) → absorbable (LUNA: Lipophilic, Uncharged, Non-ionized, non-polar = Absorbable) Most toxicants and drugs exist as weak bases or weak acids → pH of the medium determines the fraction of molecules charged (ionized/nonabsorbable) of uncharged (non-ionized/absorbable) Henderson-Hasselbach equation predicts the fraction of molecules in an ionized state. WEAK ACIDS (WA) ○ Neutral molecules that can dissociate into anion and proton (H+) ○ PROTONATED waka acids → uncharged/non-ionized → lipophilic → absorbable (LUNA) ■ pH = pKa + log [A-/HA] ○ ABSORPTION ■ Weak acids are readily absorbable in acidic medium ○ ION TRAPPING ■ Weak acids are readily excreted in basic medium ○ ○ ○ ○ Pyrimethamine ● When it combines with protons it forms a cation. ● The more absorbable form is Deprotonated form (no protons) = uncharged. Question ● A patient will experience Aspirin poisoning. What will you give to facilitate excretion of the aspirin? ● Answer: Sodium bicarbonate ○ Weak bases are readily absorbable in basic medium. ○ It is absorbable in the small intestine compared to stomach ○ Readily excreted in acidic medium ● ● ● ● ● ● Aspirin is a weak acid. It can exist as an anion plus a proton. In a medium where protons predominate, weak acids exist as neutral or non-ionized Example of medium in the body with many protons: ○ Stomach – because HCl with dissociate into Cl- and H+ Mnemonics: ○ AAA ■ Acidic drugs are ■ Absorbable in ■ Acidic medium ○ AEB ■ Acidic drugs are more ■ Excretable in ■ Basic medium ○ BAB ■ Basic drugs are ■ Absorbable in ■ Basic medium ○ BEA ■ Basic drugs are more ■ Excretable in ■ Acidic medium Neutral molecules that can form a cation by combining with a proton (H+) DEPROTONATED weak bases uncharged/non ionized → Lipophilic absorbable (LUNA) ■ pH = pKa + log [/HB+] ABSORPTION ■ Weak bases are readily absorbable in basic medium ION TRAPPING ■ Weak bases are readily excreted in acidic medium ■ Mostly exist as ionized form ● ● ● ABSORPTION Movement of toxicants from the site of administration to the systemic circulation. Main sites: GIT, Lungs, & Skin ○ Toxicants that enter through the GIT must pass through the liver. ○ Some of these toxicants will be metabolized before they reach the systemic circulation which is called as “first pass effect” or also known as “presystemic elimination” GASTROINTESTINAL (GI) TRACT GIT may be viewed as a tube transversing the body. Although it is within the body, its contents remain outside the body. Absorption of toxicants can take place along the entire GIT ○ Organic acid or base- absorb by simple diffusion where it exists in its most lipid soluble form ○ In unionized and ionized form Numerous transporters are expressed in the GIT ○ Particles and particulate matter – particle size is the main determinant (rather than LUNA) ○ Compared to organic acid and base their absorption is more dependent on their sites. WEAK BASES (WB) 15 of 25 ● ● Chemicals can alter absorption Antidiarrheal) First-pass effect/Presystemic elimination (Laxatives, ● SKIN Skin comprises of 2 major layers Epidermis ● Thin outer portion, composed of several layers. Outermost layer of epidermis is composed of dead cells with keratin ● Stratum corneum ○ Toxicants move across via Passive diffusion ● LUNGS Toxicants that are absorbed by the lungs are gases, vapors of volatile or volatilizable liquids, & aerosols GASSES & VAPORS ● Vapors – gas form of substance that can also exist as a liquid or solid at atmospheric pressure & normal temperature ● Most organic solvents evaporate and produce vapor & some solids can sublimate into a gaseous form ● Once inhaled, gasses first pass through the nose that partially protects the lungs from injury ● Once inhaled into the lungs, gas molecules diffuses from alveolar space into the blood ● Through nostrils it protects the lungs from the toxicants AEROSOLS ● Absorption is determined by aerosol size & water solubility of any chemicals ● Site of deposition of aerosols and particulates depend largely on the size ○ 5 mcm or larger (coarse particles) deposited in nasopharyngeal region ○ 2.5 mcm (fine particles) - tracheobronchial region ○ 1 mcm and smaller -alveolar sacs ● In the nasopharyngeal region, the defense mechanism is sneezing and secretion of mucus ● In the tracheobronchial region, the defense mechanism includes coughing. ○ Pseudo Columnar ciliated epithelium contains ciliated cells which is a type of cell that produces mucus ○ Toxicants can be trapped in the mucus, and it will be swept up by the cilia. It will be swallowed, sneezed, or spit. This is called the mucus ciliary; it will bring toxicants up. ○ In~ 2.5 mcm or smaller the defense mechanism are the alveolar macrophages Dermis ● Thick middle portion composed of connective tissues ● Hydrophilic toxicants are more likely to penetrate through the skin appendages ● In some books, there are 3 layers. The 3rd layer is called the subcutaneous layer. ● The epidermis is composed of 5 or sometimes 6 layers ● Toxicants that are very lipophilic can pass through the epidermis through passive diffusion ● The Stratum Lucidum is found in very thick skin (E.g. palms and soles) ABSORPTION OF TOXICANTS AFTER SPECIAL ROUTES OF ADMINISTRATION ● Chemicals may be administered by other routes, including ○ Intravenous ■ toxicant directly introduced to the systemic circulation ○ Intraperitoneal ■ Rapid absorption due to peritoneal and mesenteric blood supply ■ Most chemical enters the liver via portal circulation → First pass effect ○ Subcutaneous & Intramuscular ■ slower absorption rates ● ● DISTRIBUTION Movement of toxicant from systemic circulation to the tissue (target action) The rate of distribution to organs or tissues is determined primarily by blood flow and rate of diffusion out of the capillary bed into the cells of an 16 of 25 ● ● ● ● ● ● organ/tissue & affinity of a xenobiotic for various tissues Where is the fastest distribution of toxicants? In the brain or fats? ○ Brain, Liver Kidneys - ↑blood flow, ↑distribution ○ This is in comparison to bone, skin and fats with low distribution Protein binding: ○ Acidic drug – binds to Albumin ○ Basic drugs – binds Alpha 1 acid glycoprotein also know as orosomucoid The initial distribution is dominated by blood flow, whereas the eventual is determined largely by affinity In order for a drug to bind to its receptor, it should be a free drug. But there are certain drugs/toxicants that are bound to protein, if bound to protein it can exert its pharmacologic/toxic effect. Acidic Drug - bound to albumin Basic Drugs - bound to alpha 1-acid glycoprotein APPARENT VOLUME OF DISTRIBUTION ● Volume in which the amount of drug would need to uniformly dissolved in order to produce the observed blood concentration ● If chemical distributes only to the plasma compartment (no tissue distribution), it has a high plasma concentration → Low Vid ● If chemical is distributed throughout the body the effective plasma concentration is low→ High Vid ● Binding to and/or dissolution to various storage sites of the body (Fat. Liver, Bone) am important factors in determining distribution STORAGE OF TOXICANTS IN TISSUES ● Only free fraction of chemicals will bind to the target molecule, binding to or dissolving in certain body constituents greatly alters the distribution of xenobiotics ● The compartment where a toxicant is concentrated but is not the major site of toxicity for that chemical is describe as a storage depot ● As chemical is biotransformed or excreted from the body more is released from the storage site → Longer 1/12 ● Storage depot ○ PLASMA PROTEINS ○ LIVER & KIDNEY ○ FAT ○ BONE(lead can be stored in the bone) EXCRETION URINARY EXCRETION ● Toxic compounds are excreted in urine by the same mechanisms the kidney uses to remove the end product of intermediary metabolism from the body (Glomerular filtration, tubular excretion, and Active tubular secretion) ● Depending of the physicochemical properties of the compounds, it may be reabsorbed across the tubular cells back into the bloodstream ● Xenobiotics can also be excreted into urine by active secretion ● If the drug and urine is acidic, reabsorption happens. Therefore, it all depends on the pH of the medium and the physicochemical of the agent. FECAL EXCRETION ● Excretion of toxicants via the feces can result from direct elimination of non-absorbed compounds in the GIT, from delivery to the GIT via bile, and from secretion into luminal contents from the enterocytes ● There are certain drugs that are eliminated via bile, especially those that underwent Phase II, Glucuronidation. So, inside the stomach, and most especially inside the colon, wherein there is a large population of bacteria that hydrolyzes the glucuronic acid from the toxicant, leading to reabsorption. EXHALATION ● Substances that exist predominantly in the gas phase at body temperature are eliminated mainly by the lungs ● The usual route of excretion for highly lipophilic and volatile toxicants. OTHER ROUTES ● CSF ● Milk ● Sweat and Saliva ○ Rifampin is excreted through this route, representing red or orange discoloration 17 of 25 ● ● ● BIOTRANSFORMATION It is the conversion of chemicals to more water soluble compounds. It’s the end product of metabolism- to eliminate or to excrete the compound A more water-soluble compound is excretable Xenobiotic ● a chemical compound (drug, pesticide, carcinogen) that is foreign to a living organism Endogenous ● chemical growing or originating from within. ● Originates or produce inside the body ○ Example: Epinephrine (produced in the adrenal medulla) Substrate ● a substance to be catalyzed ● A substrate is a substance that is acted upon by the enzyme - “substance to be catalyzed” ○ Enzyme catalyzes that reaction - ● ● Ethanol or ethyl alcohol is acted upon by alcohol dehydrogenase into acetaldehyde HOW ENZYMES WORK? Help to speed chemical reactions by lowering activation energy (without consuming itself) Allowing the reaction to occur quickly Reaction between Substrate A and Substrate B Y-axis = energy use x-axis = time. The reaction between the two substances, without the enzyme, uses a lot more energy in comparison to the reaction with enzyme. This allows the reaction to occur more quickly Enzymes lower activation energy without consuming itself ● ● Enzymes play a vital role in biotransformation Transformation/Metabolism of Xenobiotics can either be beneficial or harmful ○ Depending on the dose and circumstances 2 PHASES OF METABOLISM PHASE I ● Addition of a functional group ● Aka Functionalization reaction ○ Because of the addition/exposure of the functional group of a substance which results to a slightly polar molecule that can be inactive or active PHASE II ● Conjugation of the modified xenobiotic with another substance ● Aka Conjugation reaction ○ Because of the addition of conjugates to the parent molecule ○ These conjugates are either glucuronic acid from glucuronidation, sulfate from sulfation, methyl group from methylation, etc. ● After phase 2 reaction, the metabolite is usually very polar and inactive. Hence, it is readily excretable ● Conjugated products ○ Larger molecule than substrate ○ Generally polar in nature = water soluble ○ Have polar ability to cross cell membranes ■ This means they are less likely to be re-absorbed PHASE I REACTIONS HYDROLYSIS ● Reaction with the addition of water to a reactant (OH + H) ● Substances that will undergo hydrolysis are the following ○ Esters ○ Amines ○ Hydrazine ○ Carbamates ● Ex: procaine → p-aminobenzoic acid + diethylaminoethanol 18 of 25 ○ ○ Procaine - An ester local anesthetic ■ Local anesthetics can be divided into esters and amines When it is hydrolyzed it will yield to para aminobenzoic acid (PABA) and diethylaminoethanol ■ ■ ■ 1. 2. 3. 4. ENZYMES INVOLVED IN HYDROLYSIS Carboxylesterases (found in serum & tissues) a. Hydrolyze endogenous lipid compounds b. Generate pharmacologically active metabolites (usually) Cholinesterases a. Limit the toxicity of organophosphate i. Acetylcholinesterase → Degrades acetylcholine ii. Butyrylcholinesterase → Degrades acetylcholine but is usually metabolizes xenobiotics Epoxide hydrolase a. Detoxify electrophilic epoxides (cause cellular toxicity and genetic mutations) Beta-glucuronidase a. Hydrolyzes xenobiotic glucuronides from phase II reaction i. Xenobiotic glucuronides are polar and inactive molecules. They are readily excretable. ii. Once they are acted upon by beta-glucosidase in the intestine, it will hydrolyze the glucuronic acid from the parent compound, then the parent compound can be reabsorbed via the enterohepatic circulation. b. Enterohepatic circulation REDUCTION ● Substrate gains electrons ○ Their valance decreases, that’s why they are called oxidizing agents ● Occur with xenobiotics in which oxygen content is low ● Reduction reactions frequently results in activation of a xenobiotic than detoxification ○ Most toxicants/chemicals that will undergo reduction usually results in an increase in pharmacologic action or toxicity ● Example: Azo reduction nitrogen – nitrogen double bonds ○ Nitro reduction- NO2 ■ Both are catalyzed by CYP450 & NADPH- quinone oxidoreductase ○ Nitrobenzene + H2 → aniline + 02 Nitrobenzene will reduce to form aniline Aniline can cause methemoglobinemia where the ferrous components of hemoglobin are converted to ferric. Methemoglobin has a reduced capacity to carry oxygen compared to hemoglobin OXIDATION ● Reactions in which substrate loses electrons ● Gain valence (VILEORA) ○ Valence Increase, Loses Electron, Oxidation, Reducing Agent 1. 2. - - ENZYMES INVOLVED IN OXIDATION Alcohol dehydrogenase a. Primary alcohol → aldehydes b. Secondary alcohols → ketones c. Primary alcohols when they are oxidized by alcohol dehydrogenase, they will yield an aldehyde. If it’s a secondary alcohol, it will yield ketones Aldehyde dehydrogenase a. Aldehydes → carboxylic acids (NAD-cofactor) b. Aldehydes can be further oxidized into a carboxylic acid using aldehyde dehydrogenase c. Both alcohol dehydrogenase and aldehyde dehydrogenase will use NAD as cofactor d. While CYP2E1 uses NADPH as cofactor It shows the different metabolism pathways of ethanol or alcohol. The major metabolism pathway of ethanol is through alcohol dehydrogenase (ADH) which will result in acetaldehyde. Pathogenesis of liver damage among alcoholics. Some of the alcohol will be metabolized using CYP2E1. However, this enzyme (CYP2E1) degenerates reactive oxygen species that can damage the liver. The minor metabolism is through catalase 19 of 25 - 3. 4. 5. Once acetaldehyde is form, it is metabolized to acetic acid, a carboxylic acid using the aldehyde dehydrogenase (ALDH) Monoamine oxidase (MAO) a. Oxidative deamination of primary, secondary, and tertiary amines, including serotonin, epinephrine, norepinephrine and some xenobiotics Prostaglandin H synthase a. Arachidonic acid → (cyclooxygenase)→ prostaglandins b. Prostaglandins- mediates the formation of inflammation and platelet clog formation or platelet aggregation Cytochrome P450 (CYP) a. Found in hepatic smooth ER microsomes b. Heme containing c. Classified into subfamilies based on amino acid sequence identity. d. Named in a specific manner e. It is responsible mostly for phase I reaction f. The most common CYP is CYP3A4. i. Most of the drug is metabolized by this enzyme g. CYP2D6, an important enzyme in degrading CNS drugs FACTORS THAT CONTRIBUTE TO DECREASE CYP ENZYME ACTIVITY 1. A genetic mutation a. gives rise to the poor and intermediate metabolizer genotypes. 2. Exposure to environmental factors (infectious disease or an inflammation process) a. suppresses CYP enzyme expression b. E.g. Hepatitis 3. Exposure to a xenobiotic a. inhibits or inactivates a pre-existing CYP enzyme b. By inhibiting cytochrome P450, one drug can impair the biotransformation of another leading to an increase in plasma level of other drug, leading to an exaggerated pharmacologic or toxicologic response to the second drug, and decrease its excretion FACTORS THAT CONTRIBUTE TO INCREASE CYP ENZYME ACTIVITY 1. Gene duplication leading to over-expression of a CYP enzyme. 2. Exposure to drugs and other xenobiotics that induce the synthesis of cytochrome P450 3. Stimulation of pre-existing enzyme by a xenobiotic. a. Induction of cytochrome P450 by xenobiotics increases CYP enzyme activity. b. By inducing cytochrome P450, one drug can stimulate the metabolism of a second drug and thereby decrease plasma levels, decrease or ameliorate its therapeutic effect, increase in excretion INDUCERS INHIBITORS Increases the number of CYP → increase in metabolism → decrease in pharmacologic action Decrease the number of CYP → decrease in metabolism → increase in pharmacologic action (PPRCO) (MEDICKAV-G) ● Phenytoin ● Phenobarbital ● Rifampicin ● Carbamazepine ● Omeprazole ● Metronidazole ● Erythromycin ● Disulfiram ● Isoniazid ● Cimetidine / Chloram ● Ketoconazole ● Amiodarone / Allopurinol ● Valproic acid ● Grape Juice 1. Phenytoin + Paracetamol Q1. What will happen if you co-administer Phenytoin and Paracetamol? ● Answer: Since Phenytoin is an enzyme inducer, it will induce formation of CYP 450 or stimulate the action of pre-existing CYP. ● This will lead to an increase the metabolism of Paracetamol leading to a decrease in plasma level and decrease in pharmacologic and toxic effects and increase in excretion ● ↑ metabolism ● ↓ Plasma ● ↓ pharmacologic and toxic effect ● ↑ excretion 2. Omeprazole + Amlodipine Q2: What will happen if you co-administer Omeprazole and Amlodipine at the same time? ● Answer: Since Omeprazole is an enzyme inducer, it will induce the formation of CYP and stimulate the existing CYP leading to greater metabolism of Amlodipine 3. Ketoconazole + Losartan What will happen if you co-administer Ketoconazole and Losartan at the same time? ● Answer: Since Ketoconazole is an enzyme inhibitor, it will inhibit the action of pre-existing CYP, leading to these effects in Losartan: ○ ↓ metabolism ○ ↑ in plasma levels ○ ↑ in pharmacologic action and toxicity of 20 of 25 ○ 4. Losartan ↓ in excretion ● ● Metronidazole + Gliclazide What will happen if you co-administer Metronidazole and Gliclazide at the same time? ● Answer: Since metronidazole is an enzyme inhibitor, it will inhibit the metabolism of Gliclazide ● ENVIRONMENTAL FACTORS KNOWN TO AFFECT CYP LEVELS ● Medications ● Foods ● Social Habits (alcohol consumption, cigarette, smoking) ○ Acute Alcohol consumption is an inducerinduces the formation of enzymes ○ Chronic alcohol consumption is an inhibitorinhibits the formation of enzymes ● Disease status (diabetes, inflammation, viral % bacterial infection, hyperthyroidism, hypothyroidism) ● It is possible that two or more CYP enzymes can contribute the metabolism of a single compound ● ● ● ● ● ● Information on which human CYP enzyme metabolizes a drug can help predict or explain drug interactions Inducers of cytochrome P450 increase the rate of xenobiotic biotransformation P450 induction lowers blood/toxicant levels, which compromises the therapeutic goal of drug therapy but does not cause an exaggerated response to the drug P450 induction can cause pharmacokinetic tolerance whereby larger drugs doses must be administered to achieve therapeutic blood levels due to increased drug biotransformation PHASE II REACTIONS CONJUGATION ● Conjugations result in a large increase in xenobiotic hydrophilicity – greatly facilities excretion of foreign chemicals (except methylation & acetylation) ○ Hydrophilicity means it loves water; hence it is readily excretable. ● Most conjugation enzymes are mainly located in the cytosol ● Phase II reaction is also known as conjugation reaction because you have to add conjugates to parent molecules which usually results to an inactive and very polar metabolite that is readily excretable (except for methylation & acetylation) ● Requires the co-substrate uridine diphosphate-glucuronic acid (UDP-glucuronic acid) Reaction is catalyzed by UDPglucuronosyltransferases (UGTs) ○ UGTs transfer glucuronic acid from the UDPglucuronic acid to the toxicant Endogenous substrate includes bilirubin, steroid hormones, and thyroid hormones Conjugates are polar, water-soluble metabolites ○ Once this metabolite reaches the large intestine, some of them are acted upon by beta glucuronidase (bacterias) in the large intestine ○ This will lead to the hydrolysis of glucuronic acid and the reabsorption of parent molecule → enterohepatic circulation Excreted from the body in bile or urine Cofactor availability can limit the rate of glucuronidation of drugs that are administered in high doses and are conjugated extensively, such as aspirin and acetaminophen ○ Aspirin and acetaminophen are usually metabolized via glucuronidation SULFONATION (SULFATE CONJUGATION) ● Catalyzed by sulfotransferases which produces a highly water-soluble sulfuric acid ester ● The co-substrate for the reaction is 3’phosphoadenosine- 5’-phosphosulfate (PAPS) which is synthesized from inorganic sulfate ● Involves the transfer of sulfonate from PAPS to the xenobiotic ● Conjugates are excreted mainly in urine ● Sulfonation is an effective means of decreasing the pharmacologic and toxicologic activity of xenobiotics METHYLATION ● Minor pathway of metabolism/ biotransformation. It results in lipophilic metabolites ● Decreases the water solubility of xenobiotics, it will result in lipophilic metabolites that are less likely to be excreted ○ It increases the plasma concentration of the drug and can lead to an increase in toxicity ● Masks functional groups that might otherwise be conjugated by other enzymes ● The co-substrate for methylation is S-adenosylmethionine (SAM) ○ We got methyl group from SAM and transfer to parent compound via O-Methylation, N-Methylation, S- Methylation ● Methylation can also lead to increased toxicity ACETYLATION GLUCURONIDATION 21 of 25 ● ● ● ● ● ● N-acetylation is a major route of biotransformation for xenobiotics ○ Aromatic amine → aromatic amide ○ Hydralazine → hydrazide N-acetylation of certain xenobiotics, such as isoniazid, facilitates their urinary excretion ○ Isoniazid - anti-tb drug N-acetylation is catalyzed by cytosolic Nacetyltransferase (NAT requiring the co-substrate acetyl - coenzyme A (acetyl CoA) ○ We get the acetyl group from this (acetylCoA) molecule and transfer it to the parent compound using the NAT NAT 1 and NAT2 (acetyltransferase in humans) Slow NAT2 acetylators are predisposed to drug toxicities ○ Means that these people metabolize drugs slower than others There are 2 types of acetylators: ○ 1. Fast acetylators – Philippine, Orientals, Asian ○ 2. Slow acetylators – Europeans DRUG TOXICITIES ● Excessive hypotension from hydralazine ● Peripheral neuropathy from isoniazid and dapsone ○ Vit B6 can be the treatment to isoniazid-induced peripheral neuropathy ● Systemic lupus erythematosus (SLE) from hydralazine and procainamide ○ “Drug induced lupus effect” – there are drugs that can induce lupus as HIPS ■ Hydralazine ■ Isoniazid ■ Procainamide ■ Sulfa Drugs ● Toxic effects if co-administration of anticonvulsant phenytoin with isoniazid AMINO ACID CONJUGATION ● Conjugation of xenobiotics containing ○ Carboxylic acid group with the amino group of amino acids glycine, glutamine and taurine ○ Aromatic hydroxylamine with the carboxylic acid group of amino acids serine and proline ● Amino acid conjugates of xenobiotics are eliminated primarily in urine ● Conjugation of hydroxylamines with amino acids is catalyzed by cytosolic aminoacyl-tRNA synthetases and requires ATP ● Catalyzed by a family of glutathione S-transferases that are present in most tissues TYPES OF CONJUGATION REACTIONS 1. Displacement reactions - glutathione displaces an electron-withdrawing group 2. Addition reactions - glutathione is added to an activated double bonds or strained ring system ● ● ● ● - - Glutathione conjugates formed in the liver can be effluxed into bile and blood, and they can be converted to mercapturic acids in the kidneys and excreted in urine. Conjugation with glutathione represents an important detoxification reaction: ○ Because electrophiles are potentially toxic species that can bind to critical nucleophiles (protein and nucleic acids) causing cellular damage and genetic mutations Glutathione is a cofactor for glutathione peroxidase important in protecting cells against lipid and hemoglobin peroxidation. (Primary use of Glutathione) ○ Side Effect is defined as any effect outside or other than therapeutic effect Conjugation with glutathione enhances the toxicity of a xenobiotic by: ○ Releasing a toxic metabolite ○ Being inherently toxic ○ Being degraded to a toxic metabolite Glutathione can inhibit the enzyme, Tyrosinase. Tyrosinase is needed to form Melanin, responsible for the dark pigment of our skin. Once we administer a huge amount of Glutathione, it will inhibit Tyrosinase. Glutathione is primarily used as a substrate for conjugation reactions. Side effect of Glutathione: Whitening Glutathione is primarily used now for dermatologic side effect GLUTATHIONE CONJUGATION ● Tripeptide glutathione comprises of glycine, cysteine, and glutamic acid 22 of 25 ● ● ● TYPES OF ANTIDOTES PHYSIOLOGICAL – opposite effects as that of poison CHEMICAL – changes the chemical nature of poison MECHANICAL – prevent absorption of poison SKIN DISCOLORATION ASSOCIATED SUBSTANCES Yellow Picric acid, Nitric acid Bleaching white Phenol Ash gray Mercuric chloride, physostigmine Deep brown Bromine Brown black Sulfuric acid, Iodine, Silver nitrate Bluish gray Silver salts Blue Cyanotics (opium, aniline, sulfides) Pale bonds on fingernails (Mee’s line) Arsenic Boiled lobster appearance Boric acid URINARY CHANGES ASSOCIATED SUBSTANCES Dark yellow Picric acid Yellow brown Aloe, Senna Green blue Methylene blue, phenol, triamterene, amiloride Wine (Red brown) Caffeine, Benzene, Rifampicin, Lead, Mercury, Carbon tetrachloride BOWEL CHANGES ASSOCIATED SUBSTANCES Black Charcoal, Bismuth, Iron, Manganese dioxide, Silver nitrate White Aluminum hydroxide Blue Boric acid, Methylene blue, Iodine Green Indomethacin, Iron, Cupric sulfate BLOOD CHANGES ASSOCIATED SUBSTANCES Cherry red blood Carbon monoxide, Cyanide 23 of 25 Dark red blood Nicotine Chocolate blood Aniline VISUAL CHANGES ASSOCIATED SUBSTANCES Optic neuritis (Red-green blindness) Ethambutol Purple vision Digitalis, Marijuana Partial or total blindness Methanol, Formic acid Bloodshot eyes Marijuana ODOR CHANGES ASSOCIATED SUBSTANCES Garlic odor Phosphorous, Selenium, Tellurium, Arsenic Mousy urine Coniine Bitter almond odor Cyanide Shoe polish Nitrobenzene Rotten eggs Hydrogen sulfide Mothballs Naphthalene Wintergreen Methylsalycylate Pear-like Chloral hydrate SYNTHETIC POISONS SOURCE Ethylene glycol Anti-freeze Picric acid Colorant in textile Aniline Crayons Nitrobenzene Shoe polish Hydrogen sulfide Sewer gas Asbestos Fire retardant Naphthalene Moth balls Eosin Lipstick POISON ANTIDOTE 24 of 25 Aniline or Nitrites 1% Methylene blue (0.1mg/kg) Cyanide Lilly Cyanide Kit (Amyl nitrite → Sodium Nitrite →Sodium thiosulfate Ethanol 5-10% glucose (for hypoglycemia) + thiamine Formaldehyde Diluted ammonia; Ammonium carbonate Irone Deferoxamine Methanol Ethanol 25 of 25