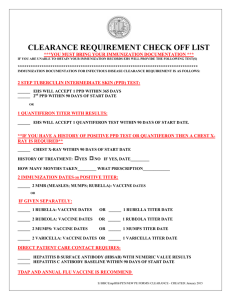
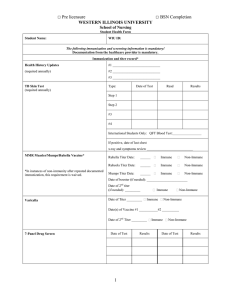
PR I N C E G E O R G E ’S COMMUNITY COLLEGE Prince George’s Community College Division of Health, Wellness & Hospitality Health Assessment Requirements A health assessment, completed by a physician, is required for each Allied Health and Nursing student. Most of our clinical sites are requiring evidence of immunization and a current PPD test in order to meet The Joint Commission standards for all employees, volunteers, and students. If a student’s health assessment is not current, clinical placement may be denied by the agencies. In order for you to proceed without any interruptions to your clinical program, you must have a health assessment performed. All health assessment information released to the specific Allied Health or Nursing Program is retained in the student’s file by the program. Any information about you will remain confidential and will only be shared with the requesting clinical agency. It will be the clinical agency, not the College that will make any final determinations about your placement. If you have any questions, please contact your program director. Revised July 28, 2021 Name: Program Name: PRINCE GEORGE'S COMMUNITY COLLEGE Last First DIVISION of HEALTH WELLNESS & HOSPITALITY Health Assessment Record Student ID# _ Date of Birth Name (Last) Phone (Home) (First) Gender (M/F) (Work) Street City Rev. 7/28/21 Page 1 State Name: Date: Zip Directions: This form is required of each Allied Health or Nursing student enrolled in a clinical program. It is intended to assess the general health and immunization status of the student, and to verify that the student meets minimum health requirements and technical standards necessary to perform essential duties in the clinical area. The Health Assessment Form is in compliance with Prince George’s Community College’s policy of equal opportunity and nondiscrimination, and the Americans with Disabilities Act of 1989. Part I “Personal Health History” is to be completed by the student. Part II “Technical Standards” and Part III “Laboratory Studies and Immunization Status” are to be completed by the examiner. All information is confidential and will not be disclosed to any party without permission of the student. I consent to the disclosure of the information on this form to the Division of Health, Wellness & Hospitality of PGCC. (Student Signature) PART I. Personal Health History: Chicken Pox Rubeola (10-day measles) Rubella (German measles) Mumps Tuberculosis Rheumatic Fever Hearing problems Vision problems Glasses/contacts Seizure/convulsions Allergies Chest pain/angina Heart disease (Date) Check (√) either yes or no in the “Now” column AND the “Past” column. NOW Yes No PAST Yes No Shortness of breath High blood pressure Hepatitis Thyroid problems Diabetes Kidney disease Orthopedic problems Back problems/injury Arthritis Cancer Anemia Bleeding tendency Drug/Alcohol dependency (palpitations; arrhythmias) If “yes” to any of the above, explain: Rev. 7/28/21 Page 2 Name: Date: NOW Yes No PAST Yes No Do you carry hospitalization/medical insurance? Yes No The student is financially responsible for any injury or illness sustained while on campus or at the clinical site. First aid and appropriate referrals are provided by the Wellness Center, Bladen Hall, Room 132. Consult individual health science programs’ Student Manual for the proper procedures for reporting an incident. Medications taken regularly (over-the-counter and prescription): Any major illness in past year requiring on-going care or therapy by a health professional? Yes Explain No Any hospitalizations, injuries, restriction of physical activity? Give dates and specify problem: Currently under Medical treatment? Yes No Specify condition being treated and name and address of health professional consulted: Have you had any mental health problems? Yes No If yes, please specify problem and date(s) Professional consulted: Name: Address: Date: Do you grant permission to the Wellness Center staff and health sciences faculty to contact physicians or other professionals who have assisted you with medical and/or mental health problems? Yes No Student’s signature Date: Student’s Acknowledgement I hereby acknowledge that the personal health history information is true and complete to the best of my knowledge and nothing has been omitted which would interfere with my physical and/or mental ability to perform assigned functions in my clinical area. Student’s signature Date: If after reviewing the candidate’s Health Assessment Record, the health sciences program has questions regarding the candidate’s ability to meet the technical standards, the program may refer the student back to their primary physician for a more detailed summary and/or refer the candidate to the Disabilities Support Services Office to document their disability (if any) and to request academic accommodations to ensure equal access in program participation. Students can contact the Disability Support Services Office (L-101A), dss@pgcc.edu or call (301) 546-0838 (voice) or (301) 546-0122 (TTY) to establish eligibility for services and academic accommodations. If eligible for services, the Disability Support Services Office will provide the candidate with a Student/Faculty Accommodation Form which must be submitted to the program faculty prior to the start of the semester in order to receive requested accommodation(s). 3 PART II. Students: Place a checkmark by your health program. If you are unable to comply with the technical standards, describe, on a separate sheet of paper, what reasonable accommodations are necessary. Examiner: Please review the appropriate technical standards and evaluate as part of your assessment. Technical Standards for the Health Information Management Program Yes No (1) Work up to 8-10 hours performing physical tasks such as walking, sitting, lifting, bending, and turning. (2) Perform fine motor movements needed to manipulate instruments and equipment. (3) Communicate effectively, using auditory and visual skills. (4) Establish and work toward goals in a consistently responsible manner. Technical Standards for the Medical Assisting, Paramedic, Nuclear Medicine, Nursing, Radiography, and Respiratory Therapy and Surgical Technology Programs (Circle program) *Standard 8 applies only to the Radiography and Nuclear Medicine Programs. Yes No (1) Work up to 8-10 hours performing physical tasks such as walking, sitting, lifting, bending, and turning. (2) Perform fine motor movements needed to manipulate instruments and equipment. (3) Communicate effectively, both verbally and written, with peers, patients, and physicians. (4) Monitor and assess patient’s needs using auditory and visual skills. (5) Work as a member of the health care team to care for patients while maintaining high standards of professionalism. (6) Work safely with patients who are susceptible to or are in the contagious stage(s) of communicable disease(s). (7) Establish and work toward goals in a consistently responsible manner. *(8) Monitor radiation exposures by the visual and auditory mode, while delivering ionizing radiation. Health Assessment (within the last six months) How long has this person been under your care? Date of last health assessment/physical exam Please check all items: Normal Abnormal Posture Head and neck (include thyroid) Nose Mouth Throat and tonsils Ears (include auditory acuity) Eyes (include visual acuity) Lungs and chest (include breasts) Heart Normal Abdomen (include hernia) Pelvic with Pap Smear (optional/Female) Testicular exam (Male) Spine and musculoskeletal system Skin and lymph nodes Neurologic Mental status (recent memory, calculating ability, orientation) Abnormal or significant findings, including pregnancy Rev. 7/28/21 Page 4 Name: Date: Abnormal PART III. Laboratory Studies and Immunization Status (Documentation indicating result, action and date required) 1. Hepatitis B Vaccine: (Required) Dates: #1 / / #2 / / #3 / / 6. TB Test: (2 step TB procedure - required annually) a. TB test (Mantoux PPD): #1 PPD Planted: #1 PPD Read: Titer Results (HBs Ab): Date: / / 2. Measles, Mumps, Rubella (MMR) Immunization: Titers indicating immunity will be accepted in lieu of MMR immunization. a. Two MMR’s or titers showing immunity is required. #1 / / #2 / / b. Rubeola (measles) Titer: Immune □ non-immune □ c. Mumps Titer: / / Immune □ non-immune □ d. Rubella (German Measles) Titer: / / Immune □ non-immune □ / / 4. Polio Titer: Date: Immune □ / / / / non-immune □ / / mm duration / / NOTE: A history of positive PPD skin test requires: a. Documented Negative CXR within 5 years Date: / / and / gm/dL (within last 6 months) / 8. Urinalysis: (within 6 months) Glucose: negative □ positive □ Protein: negative □ positive □ Date: / / 5. Varicella: (Chicken Pox) (Will not accept self-reporting, must have titer or immunizations) Varicella Immunization: #1 / / #2 / b. CXR: (required for current positive reaction) Normal □ abnormal □ Date: / _/ 7. Hemoglobin: Date: / / non-immune □ Varicella Titer: Date: Immune □ / mm duration / / b. Annual Review of TB symptoms by health care provider: Positive □ Negative □ Date: / / 3. Tetanus/Diphtheria/Pertussis (T-DAP): (required within last 10 years) Date of last booster: TB Test (Mantoux PPD): #2 PPD Planted: #2 PPD Read: / 9. Current Seasonal Flu Vaccine: Date given: / / Type: Lot #_ Exp. Date _/ / NOTE: Immunization requirements are subject to change based on policy changes of the clinical facilities. / This student is cleared on the basis of the personal history, health assessment, immunizations, and laboratory test results to participate in clinical laboratory experience. [The examiner can be a physician (MD) or certified nurse practitioner (CNP)]. (Examiner’s signature) (Date) (Type or print examiner’s name) Rev. 7/28/21 Page 5 (Office telephone) Name: Date: