Accuracy of Photographic Assessment Compared With Standard Anthropometric Measurements
advertisement

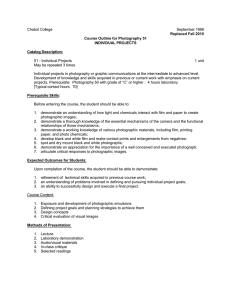
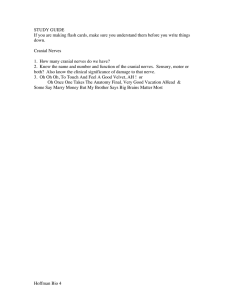
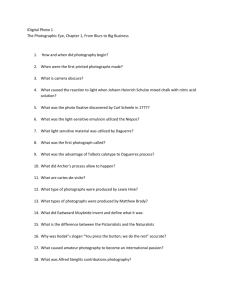
Accuracy of Photographic Assessment Compared With Standard Anthropometric Measurements in Nonsynostotic Cranial Deformities Heidrun Schaaf, M.D., D.D.S., Jan-Falco Wilbrand, M.D., D.D.S., Rolf-Hasso Boedeker, Ph.D., Hans-Peter Howaldt, M.D., D.D.S., Ph.D. Objective: Anthropometric landmarks of the skull have traditionally been used to describe cranial deformities resulting from nonsynostotic plagiocephaly or brachycephaly. Recently, digital photography has become an important tool for characterizing facial and cranial pathologies. The purpose of this study was to compare standard anthropometric cranial measurements with measurements taken from cranial photographs. Patients: Standardized digital images in the supracranial view and cranial anthropometric measurements were obtained from 122 children between the ages of 3 and 15 months. The photographs were assessed using Quick CephH software. The cephalic index and cranial vault asymmetry index were used to indicate the degree of cranial deformity. Children were classified into plagiocephaly, brachycephaly, and the combination of both. To determine interobserver variability, two clinicians separately measured the cephalic index and cranial vault asymmetry index from digital photographs in 70 infants of the plagiocephalic group. Results: To compare interassay reliability for these methods of obtaining the cephalic index and cranial vault asymmetry index, the differences between photographically and anthropometrically derived values were plotted against anthropometrically derived values alone (Bland-Altman plots). The photographic method satisfied the limits of agreement (cephalic index, 7.51%; cranial vault asymmetry index, 6.57%) and showed slightly lower values represented by the respective bias (cephalic index, 1.79%; cranial vault asymmetry index, 3.03%). Comparison between observers revealed excellent agreement, detected by the intraclass correlation coefficient of .982 for the cephalic index and .946 for the cranial vault asymmetry index. Conclusion: Our results demonstrate that digital photography is a reliable tool for quantifying cranial deformities. Furthermore, it is rapid, noninvasive, and reproducible. However, we continue to use both methods in clinical practice. KEY WORDS: anthropometry, brachycephaly, digital photography, plagiocephaly Photographic anthropometry was used in clinical medical genetics long before digital photography was implemented. In particular, photographic evaluations help to clarify verbal descriptions of craniofacial morphometry (Ferrario et al., 1993; Butler et al., 1995; Hovis and Butler, 1997; Butler et al., 1998). Since the introduction of digital photography, many have commented on its promise as a diagnostic tool, but a reliable, standardized method of photographic assessment has yet to be defined (Guyot et al., 2003). Various studies have attempted to implement digital photography in clinical assessment and verify its reliability and reproducibility. In ophthalmology, a standardized digital photography system with computerized eyelid measurement was developed (Coombes et al., 2007). In the field of orthodontics, researchers characterized facial morphology using standardized photographs and compared their results with standard cephalometric measurements (Ferrario et al., 1993; Zhang et al., 2007). The diagnostic evaluation of cranial deformities via digital photographic methods is promising for several reasons. When treating children, taking photographs is relatively quick and does not deleteriously affect the child Dr. Schaaf is Specialist–Maxillofacial Surgery and Senior Staff Member and Dr. Wilbrand is Senior Staff Member, Department of Maxillofacial Surgery, University Hospital Giessen and Marburg GmbH, Giessen, Germany. Dr. Boedeker is Chair, Institute of Medical Informatics, University of Giessen, Germany. Dr. Howaldt is Chair, Department of Maxillofacial Surgery, University Hospital Giessen and Marburg GmbH, Giessen, Germany. Submitted February 2009; Accepted January 2010. Address correspondence to: Dr. Heidrun Schaaf, Department of Maxillofacial Surgery, University Hospital Giessen, Klinikstrasse 29, 35385 Giessen, Germany. E-mail Heidrun.Schaaf@uniklinikum-giessen. de. DOI: 10.1597/09-026 447 448 Cleft Palate–Craniofacial Journal, September 2010, Vol. 47 No. 5 FIGURE 1 Representative images of the most common positional head deformities. A: Plagiocephaly. B: Brachycephaly. C: A combination of deformities. The picture shows the full supracranial view of the skull including both ears and the tip of the nose; parents support the head in slight extension. or the parents. A digital picture is an archivable document like a snapshot and measurements are repeatable. The photograph is a more objective method than the caliper and less dependent on the examiner. The major advantage of the photograph is that the landmarks can be selected on a static surface without any movement. Furthermore, it gives the opportunity for unbiased assessment by masking the observer, for example, in clinical trials. The use of clinical digital photography offers the quick transfer to other colleagues for interdisciplinary discussion. Several pictures can be taken with slightly varying perspectives, and the ones fulfilling the requirements for standardized photography can be selected. However, very few previous studies have examined the use of this method in assessing cranial deformities. An early study applied superior and frontal photographs of the head to evaluate the degree of plagiocephaly (Donegan et al., 1996); whereas, a more recent report described a measurement methodology based on black-and-white photography (Clarren, 1981). A very recent review by McGarry et al. (2008) described standard head shape measurements used in the treatment of children with deformational plagiocephaly and concluded that further research in this field is required to facilitate classification. In a recent publication discussing the effect of conservative treatment of positional plagiocephaly, Bialocerkowski et al. (2005) emphasized the need for a standardized outcome measure. The cephalic index (CI) and cranial vault asymmetry index (CVAI) were initially introduced to help define head deformity in the treatment of positional plagiocephaly (Loveday and de Chalain, 2001). However, a previous prospective cohort study that examined infants with a wide range of CI values and oblique cranial length ratios predicted that the majority of cases would resolve before 2 years of age without treatment (Hutchison et al., 2004). Craniofacial anthropometric measurements are obtained using sliding calipers, which are widely touted as a simple, cheap, and noninvasive method of evaluating deformity (Farkas, 1994; Littlefield et al., 1998; Kelly et al., 1999; Mulliken et al., 1999; McGarry et al., 2008). However, previous studies have questioned the reliability of using calipers as diagnostic devices in cranial measurements. For example, care is required to accurately locate bony landmarks and to prevent inaccurate measurements due to the displacement of soft tissue; furthermore, it is difficult for the infant to remain still for the extended period required to complete all measurements (St. John et al., 2002). Our objective was to evaluate the clinical value of standardized photographic measurements compared with the traditional cranial measurements obtained using calipers. The CI and CVAI were calculated for both methods. MATERIAL AND METHODS Digital photographs were obtained from 122 children between the ages of 3 and 15 months, all of whom had been diagnosed with nonsynostotic cranial deformities. Figure 1 shows three representative images of the most common positional deformities assessed here, including plagiocephaly, brachycephaly, and a combination of both. This study included children for whom photographic documentation and clinical measurements were obtained before treatment with a molding helmet. Photographs and clinical measurements were obtained on the same day. Photographs were selected in agreement with European standards, according to the additional picture set for standardized facial and cranial photography (Ettorre et al., 2006; Schaaf et al., 2006). All photographs were taken under standardized conditions using a single-lens reflex (SLR) camera. The local ethical committee approved the study protocol. Schaaf et al., PHOTOGRAPHIC VERSUS STANDARD ANTHROPOMETRIC MEASUREMENTS IN CRANIAL DEFORMITIES 449 Digital SLR cameras provide high-quality pictures combined with the possibility of variation of lenses. For this study we used a fixed focal length (90 to 105 mm), highquality macro lens, which assures a maximum depth of field. Lighting is performed by multi-flashlight installation with three soft boxes positioned with a constant distance of 1 to 1.5 m at either side and above the patient. The background for all pictures is a light blue color (‘‘sky blue,’’ RAL 5012). Under these conditions, high aperture settings (f . 16) and short exposure time (.125 milliseconds) mostly have been used. For each picture taken, a manual setting of exposure time and aperture setting is possible because digital pictures can be assessed immediately and the setting can be adjusted. A constant distance from the infant to the camera is desired. The height of the camera is positioned at the same level as the focal point. The full supracranial view of the skull included both ears and the tip of the nose as anatomical landmarks. Rotation of the head should be avoided and can be controlled by the appearance of these landmarks and their symmetry. Children were placed on parents’ lap in front of the blue background. Then the full supracranial oblique images with slight extension of the head, showing the nose and zygoma, were obtained while the head was supported by the parents’ arm. This method facilitates the detection of skull deformities with midfacial involvement. Previous work has identified parameters that are useful in the evaluation of cranial deformities. The CI is an anthropometric measure based on the ratio of head width to head length. Width was measured from the left euryon to the right euryon, and length was measured from the glabella to the opisthocranion on both the digital photograph and on the patient. The glabella is defined as the most prominent midline point between the eyebrows and is identical to bony glabella on the frontal bone (Farkas, 1994). Opisthocranion is the point situated in the occipital region of the head and is most distant from the glabella; that is, it is the most posterior point of the line of greatest head length (Farkas, 1994). In contrast, the calculation of the CVAI requires diagonal measurements A and B, and as such, we recorded the distances from the right frontotemporale to the left euryon and vice versa. These landmarks and distance measures were also consistent with standard documentation in anthropometry (Farkas, 1994). The CVAI is used to indicate asymmetrical deformity and is calculated as follows: CVAI 5 (diagonal A 2 diagonal B) 3 100/ diagonal A, where A , B (Loveday and de Chalain, 2001). Therefore, CVAI represents a meaningful assessment method independent of head size. A single clinician using a metric anthropometric spreading caliper (Bertillon AA 842 C, 320 mm [12L inches]; Aesculap AG, Tuttlingen, Germany) performed all clinical measurements. For the photographic measurements the Quick CephH software (Quick CephH Studio; Quick CephH Systems, San Diego, CA, USA), an orthodontic diagnosis and treatment planning application for cephalometric analysis, was used (Fig. 2). The children’s photographs were imported to the program for application of an individual analysis with anthropometric landmarks. Linear measurements on photographs can be obtained easily by clicking on two anthropometric landmarks in the picture. The computer program generates a numerical value. Both parameters CI and CVAI were a quotient of two distances, so the results are independent of a unit and of comparative value. Data analyses were performed by SAS 9.1.3 (SAS Institute, Cary, NC, USA). Bland-Altman plots were generated to compare and analyze data gathered using each method (Bland and Altman, 1986). Therefore the differences between photographic and clinical anthropometric measurement methods were plotted against the clinical anthropometric measurement alone. The BlandAltman scatter diagram shows the bias, that is, the average difference between the methods (ideal bias 5 0) and the limits of agreement, defined as 1.96 standard deviations that describe the range for 95% of comparison points. In addition, the precision of the estimated limits of agreement were determined by calculating the 95% confidence intervals for the limits of agreement (Bland and Altman, 1999). To evaluate interobserver variability, two different investigators examined digital photographs from the plagiocephalic group (n 5 70). Intraobserver and interobserver variation were determined considering the betweenand within-subject variation by intraclass correlation coefficient (ICC) under an analysis of variance framework using PROC GLM of SAS. In order to determine the interrater reliability, the ICCs were calculated by an SAS macro provided by Hamer (1990) using the ratio of mean squares from the variance table. Out of the six different ICCs proposed by Shrout and Fleiss (1979), ICC (3,k) was chosen, which is applicable when all subjects are rated by the same raters, who are assumed to be the entire population of raters. In addition, reliability is given for the mean of all ratings assuming no subject-by-rater interaction. Using the ICC statistics, interrater reliability of ..81 was defined as excellent agreement, between .61 and .80 as good agreement, between .41 and .60 as moderate agreement, between .21 and .40 as fair agreement, and less than .21 as poor agreement. The ICCs were calculated using a SAS macro (Hamer, 1990). RESULTS In total, we collected photographs of 122 children who were treated from 2004 to 2007; subjects were included only if their photographs were suitable for standardized photographic measurements. Seventy infants were diagnosed with a plagiocephalic deformity, five with brachycephaly, and 47 with a combination of both deformities. The median age at the initial examination was 28.29 weeks 450 Cleft Palate–Craniofacial Journal, September 2010, Vol. 47 No. 5 FIGURE 2 Method of photographic measurement using Quick CephH software for tracing photographs. A: The CI was established based on the ratio of head width to length. B: The diagonal measurements were recorded for the CVAI. for those with plagiocephaly, 27.29 weeks for those with brachycephaly, and 29.86 weeks for those with combined deformities. To compare photographic and clinical anthropometric measurement methods, differences between the CI values derived from photography (CI-photo) and those derived from anthropometry (CI-anthropometry) were plotted against the values derived from anthropometry to generate a Bland-Altman plot (Fig. 3). As shown in Figure 3, the photographic method satisfied the limits of agreement, which describe 1.96 standard deviations (7.51%). We noted a bias of 1.79% (i.e., the average of the values of the CIphoto measurement method were slightly lower than the average of the CI-anthropometry values). The precision, which describes the range for 68% of comparison points, is 3.83, which was within acceptable ranges. Looking for the most optimistic interpretation, considering the outer 95% confidence intervals for the limits of agreement, all but one difference value lies outside of these limits. Very similar results were obtained for CVAI values (Fig. 4), which fell within the limits of agreement (6.57%) and showed a slightly higher bias of 3.03% versus the CI comparison. The precision of 3.36 is nearly the same as for the CI values, and considering the outer 95% confidence intervals for the limits of agreement, only four values lie outside of these limits. However, plots for both indices showed that photographically derived values were progressively underestimated as the anthropometrically derived values increased. Table 1 shows the CI and CVAI data of all infants classified into the groups plagiocephaly, brachycephaly, and combined positional head deformity. FIGURE 3 Bland-Altman plots were used to compare the differences between photographically and anthropometrically derived values of cranial index (CI-photo 2 CI-anthropometry) against anthropometrically derived CI values. The dotted-dashed line (— - — - —) in the middle of the plot represents the mean value of differences (bias); whereas, the outer dotteddashed lines represent the limits of agreement (±1.96 standard deviations). The dashed lines (- - -) represent the lower/upper 95% confidence interval of the lower/upper limit of agreement. Schaaf et al., PHOTOGRAPHIC VERSUS STANDARD ANTHROPOMETRIC MEASUREMENTS IN CRANIAL DEFORMITIES 451 DISCUSSION FIGURE 4 Bland-Altman plots were used to compare the differences between photographically and anthropometrically derived values of cranial vault asymmetry index (CVAI-photo 2 CVAI-anthropometry) against anthropometrically derived CVAI values. The dotted-dashed line (— - — - —) in the middle of the plot represents the mean value of differences (bias); whereas, the outer dotted-dashed lines represent the limits of agreement (±1.96 standard deviations). The dashed lines (- - -) represent the lower/upper 95% confidence interval of the lower/upper limit of agreement. Besides the main aim of the study (the comparison of photographic and clinical anthropometric measurements), interobserver variability was assessed as a side target. Here, we chose the main group of infants with the diagnosis plagiocephaly (n 5 70) because this group represents the major diagnosis in head deformities. Comparison between observers who separately evaluated the plagiocephalic group was performed by variance decomposition using general linear modeling analysis. The ICC calculation provides the within-observer variabilities, which were 3.36% for the CI and 2.324% for the CVAI. Therefore, the probability that the difference between two measurements from two different observers on the same child will be larger than 5.08 (for the CI) and 4.226 (for the CVAI), respectively, is less than 5%. (Calculated by 1.96 3 SQRT(2 3 3.36) 5 5.08 and 1.96 3 SQRT(2 3 2.324) 5 4.226 for the CI and CVAI, respectively). The interrater reliability estimated by the ICCs revealed .982 for the CI and .946 for the CVAI. Both values can be counted as an excellent agreement between observers. The method of obtaining anthropometric measurements using sliding calipers is frequently described in the literature. The comparison between photographic and clinical measurement is rarely discussed. An investigation on eyelid position in Graves ophthalmopathy describes a fair to moderate agreement between these methods (Edwards et al., 2004). Although previous studies examined the reliability and validity of anthropometric measurements, interobserver variability has been scrutinized lately (Mortenson and Steinbok, 2006). We also investigated interobserver variability for the photographic method and found relatively little variability, with an interrater variability of 3.36% for the CI and 2.324% for the CVAI. Our ICC results of .982 for the CI and .946 for the CVAI seem to be comparable with other investigations. In the literature the interrater reliability of plagiocephalometry on 50 children, measured three times by two examiners with a thermoplastic strip and a tracing method on a photocopy, is described. For the interrater reliability using Bland-Altman plots, investigators found 5.8% for the CI and an ICC of .92 (van Vlimmeren et al., 2006). In another investigation on caliper measurements with 71 children, two examiners and three measurement sets, ICCs indicated strong intrarater reliability (.98 to .99); whereas, interrater reliability was moderate, with ICC values of .42 (Mortenson and Steinbok, 2006). By triplicating anthropometric measurements obtained by a single experienced examiner, Littlefield found an intrarater repeatability of 61 mm (Littlefield et al., 1998). Altogether, though, Mortenson states that no study exists that has investigated the interrater reliability of multiple, nonanthropometric examiners (Mortenson and Steinbok, 2006). The clinical significance or relevance can be discussed. Our results show that an experienced examiner can identify the relevant landmarks repeatedly within an acceptable range, which does not affect the clinical diagnosis or treatment procedure. Computed tomography imaging is an accurate, threedimensional technique to describe head asymmetry (Glat et TABLE 1 Comparison of Anthropometrically and Photographically Derived Measurements of Cranial Index (CI, %) and Cranial Vault Asymmetry Index (CVAI, %) in Infants With Plagiocephalic, Brachycephalic, or Combined Positional Head Deformities Variable Diagnosis n Minimum Median Maximum Mean 6 SD CI-anthropometry CI-photo CI-anthropometry CI-photo CI-anthropometry CI-photo CVAI-anthropometry CVAI-photo CVAI-anthropometry CVAI-photo CVAI-anthropometry CVAI-photo Plagiocephaly Plagiocephaly Brachycephaly Brachycephaly Combination Combination Plagiocephaly Plagiocephaly Brachycephaly Brachycephaly Combination Combination 61 70 5 5 44 47 69 70 5 5 46 47 73.5 76.6 106.3 101.8 95.0 93.2 0.7 1.5 0.7 1.5 5.1 5.1 90.3 89.2 108.7 104.1 104.0 101.5 16.4 12.8 3.0 2.6 15.9 13.4 109.8 103.4 114.5 114.2 123.5 115.9 28.2 23.8 6.1 3.7 33.7 26.4 90.1 6 8.2 89.8 6 6.3 109.3 6 3.1 105.9 6 4.8 105.4 6 6.9 101.8 6 5.1 15.9 6 6.6 12.5 6 4.8 3.0 6 2.1 2.6 6 0.8 16.8 6 6.5 13.9 6 4.9 452 Cleft Palate–Craniofacial Journal, September 2010, Vol. 47 No. 5 al., 1996; O’Broin et al., 1999), but the required radiation exposure is not justifiable in infants with nonsynostotic skull deformities that can be diagnosed clinically. Accordingly, a previous report compared digital photographic techniques with a tracing method using a flexicurve ruler to evaluate plagiocephaly in infants (Hutchison et al., 2005). In this previous publication, the photographic technique showed much less variability than the flexicurve method, and although the flexicurve method produced a similar head circumference, ear angle measurements were particularly unreliable (Hutchison et al., 2005). Photographic methods also have been used to identify landmarks or digitize the head band (Hutchison et al., 2004, 2005; Zonenshayn et al., 2004). Photographic evaluation is extremely advantageous in young children because it is rapid, noninvasive, reproducible, and provides a good clinical outcome. However, problems may be encountered in children with long hair or those who were photographed in a nonstandard position. As such, a standardized procedure must be used to obtain photos for cephalometric measurements. Previous studies have provided several recommendations to ensure high quality and consistency among photographs taken from a standard set of views (Ettorre et al., 2006; Schaaf et al., 2006). CONCLUSION Our results demonstrate that the evaluation of cranial asymmetry based on digital photography is both accurate and comparable to using standard anthropometry. However, a standardized method must be applied to obtain reliable results. The quick, simple technique described here was particularly useful in children; it facilitated the diagnostic evaluation of CI and CVAI values and was helpful in treatment planning and communication with parents. In our hands, digital photography proved to be a very useful tool regarding head shape, but the wellestablished caliper method in anthropometry should not be omitted for the time being. Acknowledgments. We thank Christine Scheibelhut and Dr. Joern PonsKühnemann (Institute for Medical Statistics, University of Giessen, Germany) for their professional biometric support in this study. REFERENCES Bialocerkowski AE, Vladusic SL, Howell SM. Conservative interventions for positional plagiocephaly: a systematic review. Devel Med Child Neurol. 2005;47:563–570. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8:135–160. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. Butler MG, Hovis CL, Angulo MA. Photoanthropometric study of craniofacial traits in individuals with Prader-Willi syndrome on shortterm growth hormone therapy. Clin Genet. 1998;53:268–275. Butler MG, Levine GJ, Le JY, Hall BD, Cassidy SB. Photoanthropometric study of craniofacial traits of individuals with Prader-Willi syndrome. Am J Med Genet. 1995;58:38–45. Clarren SK. Plagiocephaly and torticollis: etiology, natural history, and helmet treatment. J Pediatr. 1981;98:92–95. Coombes AG, Sethi CS, Kirkpatrick WN, Waterhouse N, Kelly MH, Joshi N. A standardized digital photography system with computerized eyelid measurement analysis. Plast Reconstr Surg. 2007;120:647–656. Donegan HA, O’Flaherty DC, Kernohan WG. Towards computer assisted evaluation of plagiocephaly. Med Inform (Lond). 1996;21: 155–167. Edwards DT, Bartley GB, Hodge DO, Gorman CA, Bradley EA. Eyelid position measurement in Graves’ ophthalmopathy: reliability of a photographic technique and comparison with a clinical technique. Ophthalmology. 2004;111:1029–1034. Ettorre G, Weber M, Schaaf H, Lowry JC, Mommaerts MY, Howaldt HP. Standards for digital photography in cranio-maxillo-facial surgery—part I: basic views and guidelines. J Craniomaxillofac Surg. 2006;34:65–73. Ferrario VF, Sforza C, Miani A, Tartaglia G. Craniofacial morphometry by photographic evaluations. Am J Orthod Dentofacial Orthop. 1993;103:327–337. Glat PM, Freund RM, Spector JA, Levine J, Noz M, Bookstein FL, McCarthy JG, Cutting CB. A classification of plagiocephaly utilizing a three-dimensional computer analysis of cranial base landmarks. Ann Plast Surg. 1996;36:469–474. Guyot L, Dubuc M, Richard O, Philip N, Dutour O. Comparison between direct clinical and digital photogrammetric measurements in patients with 22q11 microdeletion. Int J Oral Maxillofac Surg. 2003;32:246–252. Hamer RM. Compute six intraclass correlation measures. Available at http://support.sas.com/kb/25/031.html 1990. Accessed September 28, 2009. Hovis CL, Butler MG. Photoanthropometric study of craniofacial traits in individuals with Williams syndrome. Clin Genet. 1997;51:379–387. Hutchison BL, Hutchison LA, Thompson JM, Mitchell EA. Plagiocephaly and brachycephaly in the first two years of life: a prospective cohort study. Pediatrics. 2004;114:970–980. Hutchison BL, Hutchison LA, Thompson JM, Mitchell EA. Quantification of plagiocephaly and brachycephaly in infants using a digital photographic technique. Cleft Palate Craniofac J. 2005;42:539–547. Kelly KM, Littlefield TR, Pomatto JK, Ripley CE, Beals SP, Joganic EF. Importance of early recognition and treatment of deformational plagiocephaly with orthotic cranioplasty. Cleft Palate Craniofac J. 1999;36:127–130. Littlefield TR, Beals SP, Manwaring KH, Pomatto JK, Joganic EF, Golden KA, Ripley CE. Treatment of craniofacial asymmetry with dynamic orthotic cranioplasty. J Craniofac Surg. 1998;9:11–17, discussion 18–19. Loveday BP, de Chalain TB. Active counterpositioning or orthotic device to treat positional plagiocephaly? J Craniofac Surg. 2001;12:308–313. McGarry A, Dixon MT, Greig RJ, Hamilton DR, Sexton S, Smart H. Head shape measurement standards and cranial orthoses in the treatment of infants with deformational plagiocephaly: a systematic review. Devel Med Child Neurol. 2008. Mortenson PA, Steinbok P. Quantifying positional plagiocephaly: reliability and validity of anthropometric measurements. J Craniofac Surg. 2006;17:413–419. Mulliken JB, Vander Woude DL, Hansen M, LaBrie RA, Scott RM. Analysis of posterior plagiocephaly: deformational versus synostotic. Plast Reconstr Surg. 1999;103:371–380. O’Broin ES, Allcutt D, Earley MJ. Posterior plagiocephaly: proactive conservative management. Br J Plast Surg. 1999;52:18–23. Schaaf H, Streckbein P, Ettorre G, Lowry JC, Mommaerts MY, Howaldt HP. Standards for digital photography in cranio-maxillo-facial surgery—part II: additional picture sets and avoiding common mistakes. J Craniomaxillofac Surg. 2006;34:444–455. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–428. Schaaf et al., PHOTOGRAPHIC VERSUS STANDARD ANTHROPOMETRIC MEASUREMENTS IN CRANIAL DEFORMITIES 453 St John D, Mulliken JB, Kaban LB, Padwa BL. Anthropometric analysis of mandibular asymmetry in infants with deformational posterior plagiocephaly. J Oral Maxillofac Surg. 2002;60:873–877. van Vlimmeren LA, Takken T, van Adrichem LN, van der Graaf Y, Helders PJ, Engelbert RH. Plagiocephalometry: a non-invasive method to quantify asymmetry of the skull; a reliability study. Eur J Pediatr. 2006;165:149–157. Zhang X, Hans MG, Graham G, Kirchner HL, Redline S. Correlations between cephalometric and facial photographic measurements of craniofacial form. Am J Orthod Dentofacial Orthop. 2007;131: 67–71. Zonenshayn M, Kronberg E, Souweidane MM. Cranial index of symmetry: an objective semiautomated measure of plagiocephaly. Technical note. J Neurosurg. 2004;100:537–540.