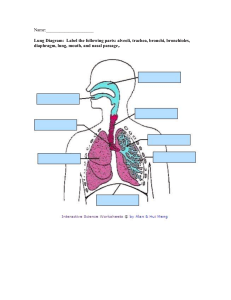
Last Name 1 ANAT in class notes/slides Anatomy and physiology of respiration -esophagus posterior to trachea -lungs consists of lobes, apeical is the apex -larynx is cap to trachea - signet ring (crico bone) - gingiva (gums) Respiration Inspiration/expiration. Primary purpose of respiratory system = “the exchange of oxygen between an organism and its environment”, tales place in alvuli Respiration is the energy supply for speech (voice production) Respiratory problems cause reduction in lung volume o Which results in reduced vital apacity o Reduced pressure generation ability o Reduced phrasing in speech o Reduced vocal intensity The respiratory system o Large airways Trachea Right bronchus Left bronchus o Smaller airways Dichotomous branches Last Name 2 Pleural membranes Outer parietal Inner visceral Brathing can be viewed in terms of cycle of respiration o This picture illustrates quiet tidal respiration o Notice that an entire cycle takes around 10 seconds o About 4 seconds for inspiration o 6 seconds for expiration o This varies based on level of activity How many cycles of breathing per minute o Avg 12 breaths per minute Respiration= echalation and inhalation = gas exchange o Occurs with minute air sacs called ”alveoli” o Active muscular process o Seeks balance and equilibrium o Cant happen without air pressure exerted on walls of a chamber ( lungs) by molecules of air o What happens if you have a punctured lung? Last Name 3 Respiration for speech o Remember The basic needs of the body will always be met before speech needs are met You breathe 12 times per minute, whether you are speaking or not The pressures for life must be maintained whether you or speaking or not. Quiet and forced inspiration o In quiet inspiration Diaphragm and external intercostals contact Compresses abdominal viscera, abdomen bulges out About 500cc flow in/out of lungs o In forced inspiration Diaphragm contracts, abdomen protrudes Thorax expands and elevates Compresses abdominal viscera, but not as much as when expire! o Diaphragm accounts for 60% of inspiratory capacity o Accessory muscles account for other 40% Tidal volume (TV): volume if air inhaled and exhaled during any single expiratory cycle o Males and females vary, based on body and thorax size o For a young adult female at rest: TV=450cc o Young adult male at rest: TV= 600cc Last Name 4 o Female + male average TV at rest = 525cc o Tidal volume during heavy work: as high as 2300cc o Functional residual capacity -how much we can take in and push out Measurement of volume o Spirometer Measures volume of air that is displaced o Pressure Manometer (cm or inches f H20 elevated) -force over area P = F/A As force increases, pressure increases As area increases, pressure decreases High heel shoes versus snowshoes Same force (weight of individual) High heel: tiny area = great pressure Snowshoe: huge area = small pressure o Pressures of the tissues Relaxation pressure Inspiratory pressure Expiratory pressure o Boyles law: pressure varies inversely with volume for a given gas On test When piston s pushed down Molecules are closer together Last Name 5 Molecular forces of repulsion increase pressure Pressure increases P=F/A (force over area= amount of force required to overcome inertia: force exerted on an area) Rib cage and diaphragm Changes of thoratic volume for inspiration o Two planes of movement when youre inspiring o Vertical (up down) From contraction of diaphragm o Transverse Transverse dimension Lateral view diaphragm o When the thorax expands in the transverse dimension the thoracic cavity increases in volume o When thethorax expands in the vertical dimension (by diaphragm contracting) the thoratic volume increases Structures of respiration o Bony thorax Vertebral column -7 cervical vertebrae Anterior view of thorax: clavical, sternum, ribs o Visceral thorax Respiratory passageway (mouth and nose; tracgea and bronchi) Lungs Last Name 6 mediastinum be able to recognize the muscles of inspiration and expiration (pg. 92 SDH) muscles of inspiration … thorax, neck, back and upper limb muscles of expiration.. thorax, back, upper, limb, abdominal muscles diaphragm = primary sterocleidomastoid (SCM) external intercostals pectoralis major and minor scalenes diapgragm o only unpaired muscle of respiration o thin o musculotendinous o separates thorax and abdomen o dome shaped higher than left o “inverted dome” Sternal Costal Vertbral portions of diaphragm o Innervation : phrenic nerve o Function: expand thorax in vertical dimension Diaphragmatic hiatuses o Aortic hiatus Descending abdominal aorta from thorax to abdomen Last Name 7 Esophogeal hiatus Passageway for esophageus Foramen vena cava o For inferior vena ceva (vein from lower body) Action of diaphragm Contraction pulls central tendon down o Increases vertical dimension of thorax (up-down dimension) o Compresses abdominal viscera Muscles of expiration o Expiration o Two ways to exhale o Passive and active o Function: compress abdominal viscera Transversus thoracis o Inncervation: intercostal nerves o Function: pulls ribs down RInternal intercostals: o FUNCTION: depress/pull down rib cage for expiration o Internal intercostals are muscles of expiration except the chondral portion which is used in inspiration> Last Name 8 Pathologies that affect speech o Any physical pathology or trauma that causes a deficit have an impact o speech production! A few problems o Acute/Suddent conditions E.g., Aspiration (a type of bacterial pneumonia) Punctured lung = pneumothorax o Chronic/Continuing conditions When the serious fluid between the pleural linings is lost or reduced, a person is said to have pleurisy COPD, sleep apnea, pulmonary fibrosis, asthma, lung cancer o Neurological: progressive neuromuscular, brain and/or nerve damage. Chronic Obstructive Pulmonary disease (COPD) Has two major subtypes Chronic bronchitis o Most often caused by tobacco smoking o Affect about 5% of adults and 6% of children in world- = about 2.9 million deaths world -wide annually o Definition: productive cough that lasts for 3 months or longer, twice in one year for 2 years o Caused by inflammation of bronchial passageways o Results in excessive musus, cough, wheezing, shortness of breath May lead to rib fractures, consciousness loss Last Name 9 o Diagnostic indicators: poor lung function, including reduced capacity o Treatments: bronchodilators, steroids to reduce inflammation, long term oxygen therapy, lung transplant o Effect on speech: reduced vocal intensity, short phrasing, fatigue during speech Emphysema o Second type of COPD o Results from loss of continuity of alveoli o Inner alveolar walls break down so that alveolar surface area declines Walls weaken and rupture Reduces oxygen transfer Symptoms: shortness of breath, fatigue Most often caused by tobacco smoke, second-hand smoke, or environmental polutions Symptoms can develop between 40 and 60 years Complications Pneumothorax Heart problems: increases workload of heart Physical changes Barrel chest Paradoxical respiration Diaphragm cant descend further, contraction actuallu shortens fibers horizontally and pulls lower thorax in Last Name 10 Emphysema and speech: short phrasing, limited phonotary ability, significant fatigue Asthma o Physical changes: narrowing of bronchial passageway, extra mucus, inflammation of bronchi o May be life-threatening o Signs and symptoms Shortness of breath Chest pain or tightness Sleep disturbance Wheezing, coughing o May arise form exercise, occupational irritants, cold air, some medications, emotional stress, gastroesophageal reflux, or allergy (spores, cat dander, etc.) o Emergency treatment for rapidly increasing difficulty o Long-term treatment: bronchial dilator (inhaler) o Effects on speech: Paradoxical vocal fold movement Can result in paradoxical vocal fold movement (PVFM) Involuntary adduction of vocal folds during inspiration PVFM can co-occur with asthma, or occur separate from asthma o Reduced vocal intensity, short phrasing, physical weakness and fatigue Last Name 11 Lung cancer o Leading cause of cancer deaths in US o Risk factor: smoking tobacco The longer you smoke, the greater the risk Smoke contains carcinogens Radon: can cause cancer and also increase risk in smokers Symptoms: o Persistent cough o Coughing blood o Chest pain, hoarseness, unanticipated weight loss Treatment: surgical, chemotherapy, radiation therapy o Surgical: from wedge resection (small section) to lobectomy (lobe) or pneumonectomy (whole lung) o New therapies: targeted drug therapies, immunotherapy Effects on speech o Pretreatment: short phrasing, shortness of breath, fatigue o Post-treatment: chemotherapy issues and cognition, shortness of breath, fatigue Last Name 12