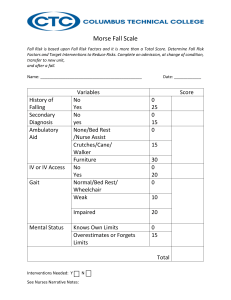
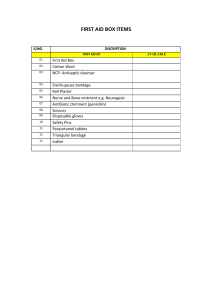
RLE MODULE 1F: Interventions for Common Signs and Symptoms DEFINITION OF TERMS; Related to Signs and Symptoms ● Intervention - act of interfering with a condition or process's result or course, to prevent harm or improve functioning. ● Sign - any objective signs that is directly observed by a physician or a nurse and can be measured with an equipment; pulse rate, body temperature, oxygen level, vital signs, blood pressure, heart rate, respiratory rate QUESTION: Would pain be under the category of sign since there are scales and charts used to measure a person’s pain level? ■ If she says 8/10 and there are observable actions then it would be sign ■ It should also be detailed and evidential for it to be considered as a sign ● Symptom – subjective, only patients can verify; chest pain, headache, loss of taste or smell, fatigue ● Syndrome - a group of signs and symptoms linked to any afflictive process that collectively characterize the disease's overall image. ○ Group of traits or conditions that occur together and characterize a recognizable disease ● Fever - increase in body temperature higher than the normal body temperature 98.6 F. or (37 C). ○ 99 F (37.2 C) or above – armpit ○ 100 F (37.8 C) or above – oral temperature ○ 100.4 F (38 C) or above – rectal, ear, temporal artery CHECK THE BOOK FOR THE NORMAL BODY TEMP RANGE ● Tepid Sponge Bath - therapeutic bath by washing all around the body using a sponge to dilate superficial blood vessels, thus releasing heat and lowering down body temperature. ● Cough - this is the body’s response to irritants (mucus, dust, smoke) in your airways. ● Chest Physiotherapy - it is an airway clearance technique to empty the lungs that includes the use of: ○ percussion (clapping), ○ vibration, ○ postural drainage – expel mucus or airway clearance with the use of gravity ○ Best determinant is body weight ● Rehydration - the process of replenishing the body's fluids and tissues with lost water. ● Oral Rehydration Solution (ORESOL) - an aqueous mixture of glucose and electrolytes having rehydrating properties and dehydration prevention properties: such as ■ sodium, potassium, chloride, magnesium, and phosphorus. ● Oral Rehydration Therapy - consists of providing a dehydrated patient a drink that is a combination of water, glucose, and salts to restore the body's normal amounts of fluids, carbohydrates, and electrolytes. IMPORTANCE: ● Chest tapping “thoracentesis” – excess fluids in the pleural space between lungs and chest wall is removed by tapping the areas ● Expectorant - a type of cough medicine used to assist removal of mucus (phlegm) from your airways. ● Diarrhea - refers to a more-frequent bowel movements with loose and watery fecal characteristics; if it happens at least bathroom call for just a day ● Dehydration - body lacks sufficient water and other fluids to perform its regular functions because you expend or lose more fluid than you consume. ❖ Importance of Tepid Sponge Bath: • reduces fever by dilating superficial blood vessels, thus releasing heat and lowering body temperature. o effectiveness is just equivalent to taking a Paracetamol, study shows that tepid sponge bath lowers the temperature faster within 30 and even more effective at lowering body temperature when combined. • lower systemic temperature when routine fever treatments fail, particularly for infants and children, whose temperatures tend to rise very high, very quickly. • What type of water will you be using for tepid sponge bath? o Utilize lukewarm water o Cold water shouldn’t be used because there will be an abrupt change in the client’s temperature ❖ Importance of Chest tapping: • get rid of extra mucus in his or her lungs. This is important because too much mucus can block the airways in the lungs. If the airways are blocked, the air cannot move in and out like it should. • essential in the airway clearance of acute and chronic respiratory disorders with retained airway secretions. 1 • • improve and maintain the well-being of the patients within the limitations imposed by the impaired lung function. Regular Chest physiotherapy plays a significant role in reducing the morbidity in children with chronic lung diseases like cystic fibrosis. ❖ Importance of ORESOL (oral rehydration solution) preparation: • replenish the body’s fluid levels. o treat moderate dehydration due to diarrhea, vomiting, or other conditions. ▪ To assess baby’s dehydration (baby: check the fontanelle if less than 12 months, if there is a depression → dehydrated) • ORESOL contains specific amounts of glucose and electrolytes. The electrolytes are potassium and sodium. That is why such solutions are given to babies suffering from diarrhea. The use of ORESOL is not only limited to babies as elders are also prescribed it for staying hydrated. Intermittent - Remittent - DIFFERENT TYPES OF FEVER, COUGH, DIARRHEA - TYPES OF FEVER Research different types of fever not limited to this; continuous, hectic temperature rise lasts for a short time before returning to normal. Causes: focal bacterial infections (canals; urinary or biliary ducts or the colon) and infections caused by foreign material. Temperature remains higher than usual throughout the day and swings by more than 1 degree celsius in 24 hours, indicating infective endocarditis. Causes: viral upper respiratory tract, legionella, and mycoplasma infections. Relapsing Constant Temperature returns to normal for a few days before rising again. Causes: borrelia bacteria species, Tick-borne relapsing fever (TBRF) (ornithodoros tick) The temperature remains above normal throughout the day and fluctuates by no more than 1 degree celsius in 24 hours. 2 TYPES OF COUGHS RESEARCH DIFF TYPES OF COUGHS; Paroxysmal, croup and others Productive Non-productive - when it pulls up or generates - produces no mucus or other mucus or any type of fluid, discharges. including blood, from the lungs or - dry cough nasal sinuses. - Many people describe the irritability - assists in the removal of mucus as “tickling” or “scratchy.” (sputum) and foreign particles from - Causes: throat irritation the airways. - Postnasal drainage occurs when a cold or allergy causes mucus to leak down the back of the throat. - Causes: Bronchitis, pneumonia, or chronic obstructive pulmonary diseases (COPD). TYPES OF DIARRHEAS Acute - three or more loose stools per day that lasts no more than 14 days. - Causes: Viruses (viral gastroenteritis - Diarrhea is frequently self-limiting. - sometimes early use of oral rehydration therapy is the best option for treating acute diarrhea. Chronic - lasts more than 14 days. - fatty or malabsorption diarrhea, inflammatory diarrhea, or watery diarrhea. - Cause: Inflammatory bowel illness (IBD) ❖ Types of Fever Interventions: ● To assess causative/ contributing factor - Identifying underlying cause. - Note chronological and developmental age of client. ● To evaluate effects/ degree of fever - Monitor core temperature by appropriate route (e.g., tympanic, rectal). Note the presence of temperature elevation (>98.6 degrees fahrenheit [37 degree celsius]) or fever (100.4 degree fahrenheit [38 degree celsius]). - Assess whether body temperature reflects heat stroke. 3 - Assess neurological responses, noting the level of consciousness and orientation, reaction to stimuli, reaction of pupils, and presence of posturing or seizures. - Monitor blood pressure and invasive hemodynamic parameters if available (e.g., mean arterial pressure [MAP], central pulmonary capillary wedge pressure [PCWP]). - Monitor heart rate and rhythm. - Monitor respirations. - Auscultate breath sounds, noting adventitious sounds such as crackles (rales). - Monitor and record all sources of fluid loss such as urine and diarrhea, wounds, fistulas, and insensible losses. - Note the presence or absence of sweating as the body attempts to increase heat loss by evaporation, conduction, and diffusion. - Monitor laboratory studies, such as arterial blood gas levels (ABGs), electrolytes, and cardiac and liver enzymes; glucose; urinalysis; and coagulation profile. ● To assist with measures to reduce body temperature/ restore normal body/organ function - Administer antipyretics, orally or rectally (e.g., ibuprofen, acetaminophen), as ordered. Refrain from use of aspirin products in children or individuals with a clotting disorder or receiving anticoagulant therapy. - Promote surface cooling by means of undressing; cool environment and/or fans; cool, tepid sponge baths or immersion; or local ice packs, especially in groin and axilla. In pediatric clients, tepid water is preferred. - Monitor used of hypothermia blanket and wrap extremities with bath towels. Turn off hypothermia blanket when core temperature is within 1 to 3 degrees of desired temperature. - Administer medications (e.g., chlorpromazine or diazepam), as ordered. - Assist with internal cooling methods to treat malignant hyperthermia. Promote client safety (e.g., maintain patent airway; padded side rails; quiet environmental; mouth chare for dry mucous membranes; skin protection from cold, when hypothermia blanket is used; observation of equipment safety measures). - Provide supplemental oxygen. - Administer medications, as indicated such as antibiotics, dantrolene, or beta-adrenergic blockers. - Administer replacement fluids and electrolytes. - Maintain bedrest. - Provide high-calorie diet, enteral nutrition, or parenteral nutrition. ● To promote wellness (teaching/ discharge considerations) - Instruct the parents in how to measure the child’s temperature, at what body temperature to give antipyretic medications, and what symptoms to report to the physician. - Review specific risk factor or cause, such as (1) underlying conditions (hyperthyroidism, dehydration, neurological diseases, nausea, vomiting, sepsis); (2) use of certain medications (diuretics, blood pressure medications, alcohol or other drugs [cocaine, amphetamines]); (3) environmental factors (exercise or labor in hot environment, lack of air conditioning, lack of acclimatization); (4) reaction to anesthesia (malignant hyperthermia); or (5) other risk factors (salt or water depletion, elderly living alone). - Identify those factors that the client can control (if any), such as (1) treating underlying disease process (e.g., thyroid control medication), (2) protecting oneself from excessive exposure to environmental heat (e.g., proper clothing, restriction of activity, scheduling outings during cooler part of day, use of fans/airconditioning where possible), and (3) understanding family traits (e.g., malignant hyperthermia reaction to anesthesia is often familial). 4 - - - - Instruct families/caregivers (of young children, persons who are outdoors in very hot climate, elderly living alone) in the dangers of heat exhaustion and heatstroke and ways to manage hot environments. Caution parents to avoid leaving young children in an unattended car, emphasizing the extreme hazard to the child in a very short period of time. Discuss importance of adequate fl uid intake at all times and ways to improve hydration status when ill or when under stress (e.g., exercise, hot environment) Review signs/symptoms of hyperthermia (e.g., fl ushed skin, increased body temperature, increased respiratory and heart rate, fainting, loss of consciousness, seizures). Recommended avoidance of hot tubs and sauna, as appropriate. Identify community resources, especially for elderly clients, to address specific needs. ❖ Types of Cough Interventions: ● To maintain adequate, patent airway: - Identify client populations at risk. - Assess level of consciousness/ cognition and ability to protect own airway. - Monitor respirations and breath sounds, noting rate and sounds (e.g., tachypnea, stridor, crackles, or wheezes). - Evaluate client’s cough/ gag reflex, amount and type of secretions, and swallowing ability. - Position head appropriately for age and condition. - Suction nose, mouth, and trachea prn using correct-size catheter and suction timing for child or adult. - Insert oral airway (using correct size for adult or child) when needed. - Elevate head of bed, encourage early ambulation, or change client’s position every 2 hr. - Exercise diligence in providing oral hygiene and keeping oral mucosa hydrated. - Monitor infant/ child for feeding intolerance, abdominal distension, and emotional stressors. - Assist with appropriate testing (e.g., pulmonary function or sleep studies). - Instruct in/ review postoperative breathing exercises, effective coughing, and use of adjunct devices (e.g., intermittent positive pressure breathing or incentive spirometer) in preoperative teaching. - Assist with procedures (e.g., dust, feather pillows, or smoke) according to individual situation. ● To mobilize secretions: - Mobilize the client as soon as possible. - Encourage deep-breathing and coughing exercises or splint chest/ incision. - Administer analgesics. - Administer medications (e.gexpectorants, anti-inflammatory agents, bronchodilators, and mucolytic agents), as indicated. - Increase fluid intake to at least 2000 mL/day within cardiac tolerance (may require IV in acutely ill, hospitalized client). Encourage/ provide warm versus cold liquids as appropriate. Provide supplemental humidification, if needed (ultrasonic nebulizer or room humidifier). Monitor for signs/symptoms of congestive heart failure (crackles, edema, or weight gain) when the client is at risk. - Perform or assist the client in learning airway clearance techniques, such as postural drainage and percussion (chest physical therapy [CPT]), fluter devices, high-frequency chest compression with an inflatable vest, intrapulmonary percussive ventilation (IPV), and active cycle breathing technique (ACBT). (Refer to NDs ineffective Breathing Pattern; impaired Gas Exchange, impaired spontaneous Ventilation.) - Support reduction/cessation of smoking 5 - Position appropriately (e.g., head of bed elevated, side lying) and discourage use of oil-based products around nose. (Refers to NDs risk for Aspiration; impareid swallowing.) ● To assess changes, note complications: - Auscultate breath sounds and assess air movements. - Monitor vital signs, noting changes in blood pressure and heart rate. - Observe for signs of respiratory distress (increased rate, restlessness/ anxiety, or use of accessory muscles for breathing). - Evaluate changes in sleep pattern, noting insomnia or daytime somnolence. (Refer to NDs Insomnia, Sleep Deprivation.) - Document response to drug therapy and/or development of adverse side effects or interactions with antimicrobials, steroids, expectorants, and bronchodilators. - Observe for signs/symptoms of infection (e.g., increased dyspnea with onset of fever or change in sputum color, amount, or character) - Obtain sputum specimen, preferably before antimicrobial therapy is initiated. - Monitor/ document serial chest x-rays, arterial blood gasses or pulse oximetry readings. ● To promote wellness (Teaching/ Discharge Considerations): - Assess client’s/ significant other’s (SO) knowledge of contributing causes, treatment plan, specific medications, and therapeutic procedures. - Provide information about the necessity of raising and expectorating secretions versus swallowing them. - Demonstrate/ assist client/SO in performing specific airway clearance techniques (e.g., forced expiratory breathing [also called huffing] or respiratory muscle strength training, chest percussion, or use of a best), as indicated. - Instruct client/SO/caregiver in use of inhalers and other respiratory drugs. Include expected effects and information regarding possible side effects and interactions of respiratory drugs with other - - medications, over-the-counter medications, and herbals. Discuss symptoms requiring medical follow-up. Encourage/provide opportunities for rest; limit activities to level of respiratory tolerance. Urge reduction or cessation of smoking. Refer to appropriate support groups (e.g., stop smoking clinic, COPD exercise group, weight reduction, the American Lung Association, the Cystic Fibrosis Foundation, or the Muscular Dystrophy Association). Determine that the client has equipment and is informed in the use of nocturnal continuous positive airway pressure (CPAP). (Refer to NDs Insomnia, Sleep Deprivation.) ❖ Types of Diarrhea Interventions: ● To assess causative factors/ etiology. - Ascertain onset and pattern of diarrhea, noting whether acute or chronic. - Obtain history and observe stools for volume, frequency (e.g., more than normal number of stools per day), characteristics (e.g., travel, recent antibiotic use, day care center attendance) related to occurrence of diarrhea. - Note the client's age. - Determine if incontinence is present. (Refer to ND bowel Incontinence.) - Note reports of abdominal or rectal pain associated with episodes. - Auscultate abdomen. - Observe for the presence of associated factors, such as fever or chills, abdominal pain and cramping, bloody stools, emotional upset, physical exertion, and so fort. - Evaluate diet history, noting food allergies or intolerances and food and water safety issues, and not general nutritional intake and fluid and electrolyte status. 6 - Review medications, noting side effects and possible interactions. Determine recent exposure to different or foreign environments, change in drinking water or food intake/ consumption of unsafe food, swimming in untreated surface water, and similar illness of family members/ others close to client. - Note history of recent gastrointestinal surgery, concurrent or chronic illness and treatment, food or dug allergies, and lactose intolerance. - Review results of laboratory testing. ● To eliminate causative factors. - Restrict solid food intake, as indicated. - Provide for changes in dietary intake - Limit caffeine and high-fiber foods; avoid milk and fruits, as appropriate. - Adjust strength or rate of enteral tube feedings; change formula, as indicated. - Assess for and remove fecal impaction, especially in an elrdly client. (Refer to NDs Constipation; bowel Incontinence.) - Recommend change in drug therapy, as appropriate (e.g., choice of antibiotic). - Assist in treatment of underlying conditions (e.g., infections, malabsorption syndrome, cancer) and complications of diarrhea. - Promote use of relaxation techniques (e.g., progressive relaxation exercise, visualization techniques) ● To maintain hydration/ electrolyte balance. - Note reports of thirst, less frequent or absent urination, dry mouth and skin, weakness, light-headedness, and headaches. - Monitor total intake and output, including stool output as possible. - Observe for or question parents about young child crying with no tears, fever, decreased urination, or no wet diapers for 6 to 8 hr; listlessness or irritability; sunken eyes; dry mouth and tongue; and suspected or documented weight loss. - Asses for the presence of postural hypotension, tachycardia, skin hydration/ turgor, and condition of mucous membranes. - Weigh infant’s diapers - Review laboratory studies for abnormalities. - Administer antidiarrheal medications, as indicated. - Encourage oral intake of fluids containing electrolytes, such as Gatorade, Pedialyte, Infalyte and Smart Water, as appropriate. - Administer IV fluids, electrolytes, enteral and parenteral fluids, as indicated. ● To maintain skin integrity. - Assist, as needed, with pericare after each bowel movement. - Provide prompt diaper/ incontinence brief change and gentle cleansing. - Use appropriate padding and pressure-reducing devices, where indicated. - Apply lotion or ointment as skin barrier, as needed. - Provide wrinkle-free dry linen, as necessary. - Refer to NDs impaired Skin Integrity, and risk for impaired Skin Integrity. ● To promote return to normal bowel functioning - Increased oral fluid intake and return to normal diet, as tolerated. - Encourage intake of nonirritating liquids. - Discuss possible change in infant formula. - Recommend products such as natural fiber, plain natural yogurt, and Lactinex. - Administer medications, as ordered. - Provide privacy during defecation and psychological support, as necessary. ● To promote wellness (Teaching/ Discharge Considerations) - Review causative factors and appropriate interventions. - Discuss individual stress factors and coping behaviors. 7 - Review food preparation, emphasizing adequate cooking time and proper refrigeration or storage. Emphasize importance of hand hygiene Discuss the possibility of dehydration and the importance of proper fluid replacement. Suggest the use of incontinence pads (depending on the severity of the problem). SIGNS AND SYMPTOMS OF: fever, cough and diarrhea Signs Symptoms Fever ● A temperature higher than: ● Body aches and headaches. ○ 100.4 °F or 38°C ● Fatigue (tiredness) (rectally) ● Loss of appetite ○ 99.5°F or 37.5°C ● Intermittent or constant (orally) sweating. ○ 99.5°F or 37.5°C ● Unwell (measured under the arm / in armpit) ● Increased pulse and heart rate (When the temperature rose by 1 degree C, the heart rate increased on the average by 8.5 beats per minute.) ● Increased BP ● Shivering, chills and shaking ● Flushed skin – warm to touch Cough ● Presence of phlegm or sputum ● A feeling of liquid running (for wet cough) down the back of the throat ● Rarely, coughing up blood (postnasal drip) ● Runny nose ● stuffy nose ● Wheezing ● Frequent throat clearing ● Hoarseness of voice and sore throat (observable) ● shortness of breath ● Heartburn or a sour taste in the mouth. Diarrhea ● Dry skin and sunken eyes due ● Abdominal cramps to dehydration ● Abdominal pain ● Rapid and deep respiration ● Bloating ● Rapid pulse rate ● Fatigue ● Low Blood Pressure (BP) ● Nausea ● Vomiting ● Frequent, loose, watery stools ● Weight loss QUESTION: cold skin or hot skin be considered a symptom since there’s no temperature indicated? • Cold skin or hot skin is considered a SIGN because it is observable and can be verified PRINCIPLES AND GUIDELINES of tepid sponge bath, chest tapping, oresol preparation Tepid Sponge Bath ● Anatomy and Physiology - Knowing both anatomy and physiology is essential for delivering tepid sponge baths because the nurse must note which bodily parts need sponges. ● Microbiology - Tepid sponge bath is done to eliminate pathogenic microorganisms. To prevent the spread of bacteria, all objects that will be used for the sponge bath should be well cleansed and washed. ● Psychology - Tepid Sponge Bath promotes a state of well-being. It is effective in relieving fever by reducing high temperature. It is also helpful in alleviating pain and providing comfort and relaxation. The procedure must be explained to the patient in order for him or her to mentally prepare for the procedure, reducing anxiety and encouraging cooperation. 8 ● Physics - Tepid sponging is the application of water to the patient's skin surface to promote dispersal of body heat when the body temperature is 39.5°C and over. The procedure is based on the principles of evaporation and conduction. Chest Tapping ● Anatomy and Physiology - As the procedure is carried out, the nurse should be aware of the landmarks in relation to respiratory assessment, proper positioning, or percussion of the client. ● Body Mechanics - With conventional CPT, you get into various positions to drain the excess mucus from the different lobes of your lungs. Each position is specifically designed so that one of the five lobes of the lungs is facing downward. The nurse must assist the client in assuming the appropriate position. To avoid unintended injury, the nurse should periodically check the client's position. ● Microbiology - To avoid the transmission of microorganisms, all materials used for chest tapping should be thoroughly cleaned and washed. Maintain cleanliness throughout the procedure when handling the drained pulmonary secretions. ● Psychology - Chest tapping helps you access your body's energy and send signals to the part of the brain that controls stress. They claim that stimulating the meridian points through EFT tapping can reduce the stress or negative emotion you feel from your issue, ultimately restoring balance to your disrupted energy. The procedure must be explained to the patient in order for him or her to mentally prepare for the procedure, reducing anxiety and encouraging cooperation. ● Physics - This enables gravity, power and pressure applied through percussion or tapping, as well as vibration, to aid in the removal of bronchial secretions from various lung segments. ● Chemistry - It results in release of energizing chemicals such as epinephrine. Oresol Preparation ● Anatomy and Physiology - The body part - small intestine plays an important role in the regulation of water and electrolyte balance between plasma and intestinal lumen. ● Microbiology - Oral rehydration therapy is used for treating the more serious dehydration that is caused by viral gastroenteritis, also known as stomach flu. This virus can cause a child to vomit repeatedly or have prolonged diarrhea, which can result in dehydration. To avoid the transmission of microorganisms, all materials used for chest tapping should be thoroughly cleaned and washed. Maintain cleanliness throughout the procedure when handling the drained pulmonary secretions. ● Psychology - Restoring a potassium deficit promotes a feeling of well-being and stimulates appetite and activity. ● Chemistry - Modest amounts of sodium and potassium-rich salts and sugar are to be added to the water for therapeutic purposes. GENERAL GUIDELINES AND NURSING management of: fever, cough and diarrhea INTERVENTIONS in the ❖ General guidelines involved in Tepid Sponge Bath 9 Tepid sponging (cold sponging); application of a moist, cold liquid to the skin in order to reduce body heat absorption and evaporation. ● Using cold sponges, a patient with hyperpyrexia can lower their temperature. ● The body's heat can pass to the cooler solution on the surface of the body because large regions of the body are sponged at once. ● Where blood circulation is close to the skin's surface, such as the neck, axillae, groin, and ankles, damp towels are frequently used. ● The vital signs are monitored often to look for potential issues early on. ● Vaso-constriction, decreased blood flow, capillary permeability, lowered metabolism, decreased blood viscosity, etc. are some physiological effects of cold treatments. ● Because the wetness spreads the cold across a wide and deep area, applying moist cold is more effective than applying dry cold. ● To obtain a tepid sponge or a cold sponge, a written order is required. ● When sponging, use long strokes and stay away from friction or circular motions. ● Maintain the hot water bag at the foot of the bed ready. ❖ General guidelines involved in Chest tapping employs one or more methods to enhance the effects of gravity and external thoracic manipulation, such as postural drainage, percussion, vibration, and coughing. Additionally, vibrations can be sent to the lung tissues via a mechanical percussor. ● In postural drainage, the patient lays or sits in various positions to elevate the area of the lung that has to be drained. ● Next, percussion, vibration, and gravity are used to drain that portion of the lung. ● The caregiver can clap on the patient's chest wall while they are in one of the positions for people with CF. ● This often lasts three to five minutes, and then there may be a brief tremor over the same area for around 15 seconds (or during five exhalations). ● The individual is then prompted to cough or puff vigorously to expel the mucus from the lungs. ❖ General guidelines in ORESOL preparation An oral powder known as oral rehydration solution (ORS) contains a mixture of sodium citrate, potassium chloride, and glucose sodium chloride. They are designed for the prevention and treatment of dehydration caused by diarrhea, including maintenance therapy, after being dissolved in the necessary amount of water. ● Use oral rehydration salts that are sold commercially. It is not advised to use homemade ORS to cure dehydration. When commercial oral rehydration salts are unavailable, these should only be taken to help avoid or delay the onset of dehydration while traveling to get medical help. ● An oral rehydration solution is created by combining water and salts for oral rehydration, which are commercially available. It is important to properly follow the dosage and ORS preparation instructions. To make the ORS, always use boiling or treated water. ● Oral rehydration salt packets are sold in most nations' pharmacies, but it is advised to buy them before leaving Canada and pack them in your travel health kit. ● If maintained at room temperature, ORS must be consumed or discarded within 12 hours, or 24 hours if kept at a cooler temperature. Nursing intervention for fever Tepid Sponge Bath Before ● Assess your patient's condition. This information will be used as a starting point to assess how well the patients responded to the therapy. 10 ● To the patient or observer, describe the procedure. It will be much simpler for them to cooperate if you tell them a little bit about the procedure. ● Bring all the necessary materials and place them next to the bed. Verify each item in your materials to make sure it is there. - Bath basin - Tepid water (37ºC; 98.6ºF) 4 Washcloths Bath thermometer Bath blanket Patient thermometer During ● Before beginning the treatment, carefully wash your hands. ● For privacy, close the door or the partition sheets (if at the ward). ● Set the height of the patients' beds so that it is convenient for working. As a result, you won't have to worry about hurting your back. ● To protect the bed linens, place a bed protector or rubber sheet on the patient's bed. ● Grab a pair of work gloves. This stops the spread of pollutants. ● To ensure privacy, carefully undress the patient, then cover him with the bath towel. ● Pour cold water into your basin and mix it with hot water. Keep an eye on its temperature. Ideally, the temperature should be just right. The ideal range is between 27 and 37 degrees Celsius. ● Small towels should be submerged or dipped in the warm water. Apply it gently to the forehead, the axilla or armpits, and the groin area while squeezing it to prevent leakage. Repeat, if necessary, after 20 to 30 minutes of doing this. Applying compresses to areas with big superficial blood vessels, such as the axillary and groin regions, greatly improves heat transfer. ● For around five minutes, gently wipe the patients' extremities. then spend the next 5 to 10 minutes working on your back and buttocks. Typically, the chest and abdomen are excluded. ● By taking his temperature, keep track of how the patient is responding to the treatment. If it is just a little bit higher than average, stop the process. After ● The patient's attire should be changed, and a light covering should be placed over him. As far as possible, refrain from allowing your patient to wear bulky clothing or additional bedding, as these things will only make him feel hotter. ● Change the linens on the patient's bed and move any equipment away from it to prevent the spread of bacteria. Next, lower the patient's bed back to a safe height. Remove your gloves and give your hands a good, thorough wash. ● Record the procedure that was performed, the patient's vital signs, their reaction to the treatment, and whether any complications arose. Nursing interventions for Cough Chest tapping Before ● Check for patency of the airway. ● To promote comfort, instruct the client to remove tight clothing, jewelry, buttons, and zippers around the neck, chest and waist. Light, soft clothing, such as a T-shirt, may be worn. Do not do CPT on bare skin. ● Keep a supply of tissues or a place to cough out the mucus nearby. During ● The nurse clapping (percussion) on the chest wall over the area of the emptied lung facilitates the passage of mucus into the bigger airways. 1. With postural drainage, the patient shifts their position while lying or sitting in order to empty as much of the lung as feasible. 11 2. The caregiver can clap on the patient's chest wall while they are in one of the positions for people with CF. This often lasts three to five minutes, and then there may be a brief tremor over the same area for around 15 seconds (or during five exhalations). The individual is then prompted to cough or puff vigorously to expel the mucus from the lungs. 3. The hand is cupped as if to hold water but with the palm facing down (as shown in the figure below) 4. A firm beat and forceful percussion are used. Every rhythm ought to sound hollow. Because the arm is relaxed and most of the action is in the wrist, percussion is less demanding to perform. When the hand is appropriately cupped, drumming shouldn't hurt or sting. ● Vibration is a technique that gently shakes the mucus so it can move into the larger airways. 1. In order to create a delicate shaking motion, the caregiver tenses the muscles in the arm and shoulder and places a strong touch on the chest wall over the area of the lung being drained. The caregiver then lightly presses the part that is vibrating. 2. The flattened hand is used for vibration, not the cupped hand (see the figure below). Exhalation ought to be as gradual and thorough as feasible. After ● Perform aftercare ● Identify the patient's lung sounds ● Inquire if the person feels any relief. Nursing interventions for Diarrhea Making homemade ORESOL Before ● Prepare the necessary material (below is the ratio of oresol) ○ FOR GLASS ̶ 1 teaspoons of sugar ̶ Glass with 240 mL boiled water ̶ Pinch of salt ○ FOR LITER ̶ 8 teaspoons of sugar ̶ A liter of water ̶ 1 teaspoon of salt ● Then do medical handwashing During ● One liter of water should contain six tablespoons of sugar. 12 ● Add water to ½ teaspoon of salt. ● Combine each component. Wait until all of the components of the two mixtures have dissolved into the water solution. ● The ORS mixture prepared is now ready for consumption. After ● Apply aftercare ● Any salts for rehydration that have dissolved in water but haven't been used ought to be discarded after one hour in room temp (unless stored in a fridge, where they may be kept for 24 hours but beyond that throw). ● Record the results and the patient's reaction. BEGINNING SKILLS in: tepid sponge bath, chest tapping and ORESOL preparation Tepid sponge bath 1. Prepare the necessary materials for the procedure. 2. Perform Medical Handwashing. 3. Don the necessary Personal Protective Equipment (PPE). 4. Identify the client. 5. Explain the purpose, process, and their role in the procedure. 6. Measure the client’s body temperature and record/document the result. 7. Adjust the client’s bed, as well as the client’s position, for comfortability and for efficient execution of the procedure. 8. Place a rubber sheet on the client's bed to protect the underlying linens. 9. Request the client to take off layers of clothing, if possible, so as to expose the body for the sponge bathing. 10. Prepare the tepid water in a basin and make sure to keep it at an appropriate temperature for the client. 11. Moderately soak the washcloth so as to provide comfort for the client during the sponge bathing. 12. Once the washcloth is soaked, gently apply the wash cloth to the client’s forehead. 13. Afterwards, soak another washcloth and gently apply to the axilla/armpits of the client. a. Note: Once axilla/armpit should each have a washcloth. 14. Then, soak another washcloth that is to be gently applied to the groin area of the client. 15. The washcloths should be applied for about 20-30 minutes. 16. Afterwards, remove the washcloths and gently dry the areas with a dry towel. 17. Replace the client’s clothing and cover the client with a light sheet/blanket. 18. Monitor the client’s temperature and document the results. 19. Perform aftercare: complete and proper collection of used materials, medical handwashing, return the client’s bed back to its original form, reposition client to a comfortable position, and dispose of waste materials if any. Armpit, inguinal and chest have a lot of blood vessels that is why it emits the most heat Chest tapping 1. Perform Medical Handwashing. 2. Identify the client. 3. Explain the purpose, process, and their role in the procedure. 4. Auscultate the client's lungs to determine the capability of the client to undergo the procedure. 5. Position the client depending on the section of the lungs to undergo the procedure. a. Note: The procedure usually begins with the lower lobes and ends with the upper lobes. 13 6. Then perform percussion with hands in a cupped shape, with fingers flexed and thumbs pressed against the index fingers. 7. Afterwards, request the client to expectorate any secretions loosened by the procedure. 8. Monitor clients for any observations that indicate immediate attention. 9. Properly and safely dispose of secretions and waste. 10. Auscultate the client’s lungs for any indications of respiratory issues. 11. Record/document the results of the procedure. ORESOL preparation a.) Made at home 1. Prepare a clean container that can hold 1 liter of water. 2. Fill the container with clean water up to 1 liter. 3. Add six (6) teaspoons of sugar. 4. Add half (1/2) a teaspoon of salt. 5. Stir the mixture until the contents have dissolved. b.) Pre-packed formula 6. Prepare a clean container according to the serving size mentioned on the packaging. 7. Fill the container with clean water up to the mentioned amount. 8. Pour the contents of the packaging into the container. 9. Stir the mixture until the contents have dissolved. 3. Oresol/oral rehydration solution – aqueous solution composed of glucose and electrolytes with dehydration prevention and rehydration activities 4. Remittent – fever that remains above normal throughout the day and fluctuates more than 1 C in 24 hours 5. Relapsing – type of fever that returns to normal for days before rising again 6. All statements are correct – In performing Chest Physiotherapy, the hand should be cupped as if to hold water with the palm facing down. The cupped hand curves to the chest wall and traps a cushion of air to soften the clapping. 7. True – one importance of chest tapping is for airway clearance technique 8. Physics – Prior to performing Chest Tapping, Nurse Jeremy, makes sure to cupped her hands and have the client position correctly. 9. Anatomy and Physiology – Nurse Anna is performing a tepid sponge bath for a pediatric client. She knows that the procedure's goal is to lower the body's temperature. The hypothalamus is the center of the body's temperature regulation. This describes the principle of: 10. True SELF ASSESSMENTS: MODULE 1F: 1. Chest tapping/chest percussion – technique used to loosen secretions in the lungs and respiratory tract 2. Postural drainage – type of chest physiotherapy shown in the illustration above 14 RLE MODULE 2F: FIRST AID (BANDAGING AND SPLINTING) Terms A situation or incident that is unanticipated and unplanned. 125.2 bandaging It is when you cover a skin injury in order to help stop the bleeding and prevent infection. 125.4 burns 125.5 dislocation A condition in which the bone ends are displaced from their natural locations. 125.6 emergency care Refers to the initial care you should administer to an injured or ill individual until complete medical treatment is available. Definition 125.1 accidents 125.3 bites tendons, life threatening Includes most medical services required for immediate diagnosis and treatment of medical condition which it not addressed immediately may lead to death 125.7 fainting “syncope” Wounds where the skin is only slightly damaged or when the bite is from a human (e.g., a child) or a domestic animal that is vaccinated/unvaccinated against rabies. A temporary loss of consciousness caused by a reduction in blood supply to the brain. 125.8 first aid Tissue damage caused by fires, extended exposure to sunlight or other types of radiation, or contact with hot surfaces or chemicals. The initial and urgent care given to anyone with a mild or serious disease or injury, with the goal of preserving life, preventing the condition from worsening, or promoting recovery. 125.9 frostbite It occurs when the skin and underlying tissues freeze as a result of being exposed to extremely cold temperatures. 125.10 hematoma It is a collection of blood that has accumulated outside the blood arteries. A blood clot that occurs in an organ, tissue, or bodily area. 125.11 hemorrhage A blood loss caused by damaged blood vessels. A hemorrhage can be internal or external, and it usually involves a large amount of bleeding in a short period of time. First degree burn: superficial, minor and nonthreatening Second degree burn: affects epidermis and parts of dermis; most painful and may cause blisters, scarring Third degree burn: nerves and changes color of skin, up to subcu Fourth degree burn: affects muscle, bone, 15 • • MASSIVE BLEEDING 125.12 infarction An injury or death of tissue (as in the heart or lungs) caused by insufficient blood flow, particularly as a result of thrombus or embolus obstruction of the local circulation. TYPES • Focal onset: aware and impaired awareness • Generalized onset: impaired awareness • Unknown onset May result to necrosis – death of body tissue 125.13 125.14 125.15 125.16 injuries joints poisoning seizure It is characterized as physical harm to your body. It is a general term that relates to injuries caused by accidents, falls, hits, weapons, and other factors. two or more bones come together to allow movement. 125.17 shock A serious condition brought on by an abrupt decrease in blood flow. 125.18 splinting Stabilizes a broken bone while injured person is taken to hospital for advanced treatment 125.19 sprain A ligament damage caused by tearing of the ligament's fibers. An injury or death caused by ingesting, inhaling, touching, or injecting medications, chemicals, venoms, or gases. Changes in behavior and sudden, uncontrollable physical movements are brought on by aberrant electrical activity in the brain. Wrench or twist in the ligaments violently causing pain and swelling but not to the point of dislocation 125.20 strain Sudden uncontrollable electrical activity in the brain STAGES OF SEIZURE: • Prodromal phase: starts a few hours before the seizure • Aura: last a few seconds Ictal: body stiffens, actual seizure Post-ictal: tiredness, irritability, vomiting, and balance problems injuries brought on by overstretching of the muscles or tendons, which attach the muscles to the bones. Injury to muscle or tendon from overuse or trauma 125.21 tourniquet Tight bands that are used to block blood flow to a wound in order to control bleeding. Limits blood flow 16 125.22 trauma A bodily injury or an event that produces longterm mental or emotional harm. 125.23 wound care Wound care is an important process that includes all stages of wound management in order to avoid serious consequences. This includes determining the type of wound, factors that influence wound healing, and the appropriate wound management therapy. Ensures wound healing and prevents more serious complications from occurring Importance of First Aid ● It affords people with the ability to provide help during various emergency situations. If someone ingests hazardous substances, or suffers health-related issues like a heart attack, or if a natural disaster occurs, a person knowledgeable in first aid becomes more than just another bystander. Instead, they become an invaluable support not only to victims, but also to professional emergency responders and medical practitioners. ● First aid helps ensure that the right methods of administering medical assistance are provided. Knowing how to help a person is just as important in emergency situations. It only takes six minutes for the human brain to expire due to lack of oxygen. As such, ineptitude and misinformation will not be of much help to a person in need of medical assistance. ● Knowledge in first aid also benefits the individuals themselves. Whether the emergency affects themselves directly, or involves people they live and work with, first aid stems the severity of an emergency in a given time and place. Aims of First Aid ● Preserve Life As a first responder to any situation, your first priority should be to preserve life. You may need to perform CPR, stop bleeding or take other action to preserve the victim’s life. Start with ABC – airway, breathing and circulation Assess the quality of the victim’s circulation, adjust if needed. Ensure that the victim has no blocks to their airway and that they are breathing. The goal is to prevent the condition from worsening in any way. ● Prevent Deterioration This is all about keeping the patient’s condition stable so it does not worsen in the time spent waiting for medical professionals to arrive. The goal is to prevent the condition from worsening and prevent any potential further injury. This may mean moving the victim to a safer location, applying first aid, stabilizing them, or just staying with the victim and providing comfort. To do this, the first responder would provide first aid treatment and reassurance. Further injury would be guarded against and the casualty would be positioned safely and comfortably. ● Promote Recovery The first responder, in providing first aid treatment, would aim to relieve pain and encourage confidence in the patient. These are important steps in helping the recovery process. These 3 Ps help prioritize a first responder’s actions and play an important role in emergency treatment for victims. Hindrances in First Aid ● Unfavorable surroundings - Night time - Crowded City streets 17 - Busy Highways Cold and rainy weather Lack of necessary materials or helpers ● Presence of crowds - Crowds curiously watch, sometimes heckle, sometimes offer incorrect advice - They may demand haste in transportation or attempt other improper procedures ● Pressure from friends or relatives - High expectations - Afraid of failure Roles, Characteristics, and Responsibilities of a First Aider ● Being a First Aider - Provides immediate lifesaving care before the arrival of further medical care - Places an unconscious casualty into the recovery position - Performs cardiopulmonary resuscitation (CPR) - Adult: 30 compressions; 2 breaths - Children: 15 compressions: 2 breaths - Uses automated external defibrillators (AED) - In cases of cardiac arrest - Stops bleeding using pressure and elevation - Keeps fractured part still - Keep it as immobile as much as possible - Performs emergency first aid at the site - Takes universal precautions or observes Standard Operation Procedure (SOP) - Helps an individual who is injured or ill to keep them safe and to cause no harm ● Characteristics - REGORT - Respectable - Empathetic - Gentle - Observant - Resourceful - Tactful ● Responsibilities - Manages the incident and ensures the continuing safety of themselves, bystanders, and the casualty - Assesses the casualties and find out the nature and cause of injuries - Prioritizes casualties based upon medical need - Prevents infection or cross-contamination by wearing Personal Protective Equipment (PPE) - Arranges for further medical help - Arranges other emergency services such as fire/security/ambulance/evacuation - Provides detailed information while handing over the patient to hospital doctor - Maintains first aid boxes - Reports all injuries to appropriate authorities - Shares immediate information of event with OHC/Plant in charge/Department authorities Principles involved in First Aid ● Anatomy and Physiology - It is important to have a basic understanding of the structures and functions of the human body. This knowledge can help with patient assessment, patient care, and emergency communication and reporting. An example where this principle can be applied is when using the triangular 18 bandage. It is especially important to be familiar with basic body parts in order to recognize different landmarks when applying the bandage. ● Body Mechanics - Proper body mechanics enables individuals to carry out activities without expending excessive energy, and it aids in the prevention of injuries for both patients and health care providers. ● Microbiology - Knowledge of microbiology is important in first aid because one may be dealing with patients who may become infected due to microorganisms and improper wound care. Rinsing the wound thoroughly, covering it properly, changing the dressing frequently, and using antiseptics as needed all help to prevent infection by reducing bacteria. ● Pharmacology- First responders must have sufficient knowledge of the different medications they need to give the patient in order to provide temporary relief while waiting for help or other healthcare team. Having knowledge about different drugs will also contribute to helping the patient who is experiencing drug or substance overdose. ● Sociology - In first aid, it is important to have the patient cooperate and follow what needs to be done in order to help them effectively. There are some procedures in first aid that require the help of the patient so establishing rapport for their cooperation and trust is important. This is also observable as first raiders communicate with the other healthcare members in order to provide the best course of treatment possible. ● Chemistry - The principle of chemistry is applied when dealing with chemical hazards. If a chemical comes into contact with the skin, immediately flush it with water. If a chemical penetrates the clothing, remove it immediately and flush the skin with water. This principle is also applied when using antiseptic solutions to prevent infections. ● Physics - When creating various slings, splinting, or bandaging, ensure that the bandage is tightly placed and that there is pressure to stop bleeding in wounds or to avoid moving fractures or injuries. Applying too much pressure, however, may affect the casualty's circulation. Proper positioning of materials in the right parts is critical in ensuring no further damage will be caused. ● Time and Energy - The preserving life principle requires immediate action. A quick response to an accident can save lives and reduce the possibility of things worsening. If someone requires assistance due to an injury or illness, one should not hesitate to assist. ● Safety and Security - This principle is applied when one makes sure that the bandages are securely fastened to prevent them from becoming loose and not supporting the injury causing other risks of injury. Making sure that the place is safe enough to help the patient will help avoid causing more harm to the patient, especially during natural calamities. Bandaging ● Psychology - First responders must be able to remain calm under pressure and contribute to lowering the overall stress levels of the injured person as well as other people who may be concerned. In an emergency, reassurance can provide more support than you might expect and help people make the right decisions. Explaining the procedures to be done will also help in easing the patient’s stress and concerns and can provide assurance to the patient of the competency of the first aider. 19 Applying a Bandage ● Dress the wound ○ Wear gloves or other protective gear to avoid coming into touch with the blood. ○ Use gentle soap and water to clean the wound. ○ If desired, apply a thin layer of topical antibiotic. ○ Cover the entire wound with a fresh dressing. Air can enter gauze dressings to speed up healing. The surface of non-stick dressings is unique and won't stick to the wound. ○ If the dressing becomes soaked with blood, cover it with another one. ● Cover the bandage ○ Roll up some cloth or gauze strips, and wrap them around the wound many times. ○ Extend the bandage at least an inch past the dressing on both sides. ○ Avoid wrapping the bandage too tightly to prevent healthy tissue from receiving blood flow. ● Secure the bandage ○ Attach the bandage with tape or a tie. ○ Avoid wrapping the bandage too firmly to prevent your fingers or toes from turning pale or blue. ● Check circulation ○ Check circulation in the area below the bandage after several minutes and again after several hours. If circulation is poor, the skin may look pale or blue or feel cold. Signs of poor circulation also include numbness and tingling. ○ If circulation is impaired, remove the bandage as soon as possible. If symptoms persist, seek medical attention. The Triangle of Forehead Bandage ● Place middle of base of triangle so that edge is just above the eyebrows and bring apex backward, allowing it to drop over back of head (occiput). Bring ends of triangle backward above ears. ● Cross ends over apex at occiput, carry ends around forehead, and tie them in a square knot ● Turn up apex of bandage toward top of head. Pin with safety pin or tuck in behind crossed part of bandage Splinting Applying Splints ● A splint should be long enough to extend beyond the injured joint or bone. It should extend above and below the fracture point. ● Any firm or rigid material can be used for splinting, such as wood, tongue depressor, cardboard, folded magazines or newspaper. ● Use towels, clothing, or other soft material to cushion the area to prevent further injury. 20 ● Support and fasten the splints with bandages or cloths at a minimum of three areas: ○ Below the joint; below the break. ○ Above the joint; above the break. ○ At the level of the break; but not directly on the injury ● Broken bones in the hands or feet can be immobilized by gently wrapping a pillow or blanket around them to protect from further injury. ● Apply pressure with a sterile dressing to control any serious bleeding. 3. Until more durable splints can be used, an injured finger can be splinted using small pieces of wood or cardboard or buddy-taped to the nearby, unaffected fingers. Lower Extremities Upper Extremities 1. For immobilizing collarbone, shoulder, and upper arm injuries reaching down to the elbow, bandages can be used to make a sling. A thick bandage covering the person's chest is stretched around the person's body to secure the arm sling. 2. A straight, supporting splint that secures and aligns both sides of the injury is necessary for forearm and wrist injuries. Open hardcover books provide an effective, quick, and portable temporary immobilizer. 1. Evaluate the foot ○ Check the temperature thoroughly ○ Check for sensation ○ Check for movement ○ Check for bruising 2. Create a cardboard splint that is broad enough along with the different panels. 3. Pad the splint with a towel in order to bolster the foot. 4. Position the splint so that the center panel is directly under the back of the leg and foot. 5. Secure the splint with tape after folding up the side panels. 6. Place an ice pack on the injury to help reduce the swelling and pain. 7. Reassess and go to the hospital by rechecking the circulation, sensation, motion, and bruising after the splint has been secured 21 Slinging Triangular Arm Sling ● Bend arm at elbow so that the little finger is about a handbreadth above level of elbow. ● Drape upper end of triangle over uninjured shoulder. ● Slip bandage between body and arm. ● Carry lower end up over flexed forearm (ends of fingers should extend slightly beyond base of triangle). ● Slide lower end of bandage under injured shoulder between arm and body and secure the two ends with a square knot. ● Draw apex toward elbow until snug, and secure with safety pin or adhesive tape. 3. Ask the casualty to let go of his injured arm. Tuck the base of the bandage under his hand, forearm, and elbow. 4. Bring the lower end of the bandage up diagonally across his back, to meet the other end at his shoulder. 5. Tie the ends in a reef knot at the hollow above the casualty’s collar bone. Tuck the ends under the knot to pad it. 6. Twist the point until the bandage fits closely around the casualty’s elbow. Tuck the point in just above his elbow to secure it. If you have a safety pin, fold the fabric over the elbow, and fasten the point at the corner. 7. Regularly check the circulation in the thumb. If necessary, loosen and reapply the bandage and sling. Nursing Interventions for the following medical emergencies Epistaxis Interventions: • • • Elevation Sling 1. Ask the casualty to support his injured arm cross his chest, with the fingers resting on the opposite shoulder. 2. Place the bandage over his body, with one end over the uninjured shoulder. Hold the point just beyond his elbow. • Have the patient sit in an upright position and lean forward. Keeping an upright position will reduce blood pressure in the veins of the nose. This discourages further bleeding. Sitting forward will also prevent the patient from swallowing blood which can irritate the stomach. Apply continuous pressure by pinching nares together for 5-10 minutes. Direct external digital pressure to the nares with the use of index finger and thumb must be applied. Pinching sends pressure to the bleeding point on the nasal septum and often stops the flow of blood. Tell the patient to breathe through the mouth. To prevent re-bleeding, tell the patient to not pick or blow his/her nose and don't bend down for several hours while keeping the head higher than the level of the heart. Petroleum jelly can also be applied to the inside of the nose using a cotton swab or finger. If bleeding persists, cotton pledgets soaked in a vasoconstrictor and anesthetic will be placed in the anterior nasal cavity, and direct pressure should be applied at both sides of the nose. 22 • Animal Bites (Snakes, dogs, or any rabid animal) Interventions: • • • • Stop the wound from bleeding by applying direct pressure with a clean, dry cloth. Wash the wound. Use mild soap and warm, running water. Thoroughly clean the wound by washing with soap and tap water as soon as possible. A light scrubbing should occur during the wash. After drying, the wound should not be closed if it is a puncture wound, but it may be covered with a dry dressing if there is a cut or laceration. Patient should be taken to the doctor immediately. Since there is a chance of being infected with tetanus, the doctor will administer an injection containing tetanus vaccine. It is better to take the course of anti-rabies treatment to provide immunity against the disease. Wounds (Open and Closed) Interventions: • • • • • • First, wash your hands. This helps avoid infection. Stop the bleeding. Minor cuts and scrapes usually stop bleeding on their own. If needed, use direct pressure with a clean bandage or cloth and elevate the wound to control bleeding and swelling. Wash and disinfect the wound to remove all dirt and debris. Rinse the wound with water. Keeping the wound under running tap water will reduce the risk of infection. Wash around the wound with soap. But don't get soap in the wound. See a doctor if you can't remove all debris. When wrapping the wound, always use a sterile dressing or bandage. Covering the wound keeps it clean. o Very minor wounds may heal without a bandage. Change the dressing. Disinfect and dry the wound thoroughly before dressing it again. Dispose of old dressings and bandages in plastic bags. Let the patient get a tetanus shot if he/she hasn't had one in the past five years and the wound is deep or dirty. Watch for signs of infection. The patient must seek a doctor if there are signs of infection on the skin or near the wound, such as redness, increasing pain, drainage, warmth or swelling. Burns Interventions: ● For minor burns: ○ Cool down the burn. After holding the burn under cool, running water, apply cool, wet compresses until the pain subsides. ○ Remove tight items, such as rings, from the burned area. Be gentle, but move quickly before swelling starts. ○ Avoid breaking blisters. Blisters with fluid protect the area from infection. If a blister breaks, clean the area and gently apply an antibiotic ointment. ○ Apply a moisturizing lotion, such as one with aloe vera. After the burned area has been cooled, apply a lotion to provide relief and to keep the area from drying out. ○ Loosely bandage the burn. Use sterile gauze. Avoid fluffy cotton that could shed and get stuck to the healing area. Also avoid putting too much pressure on the burned skin. ○ Administer over-the-counter pain reliever to the patient if necessary. Consider acetaminophen (Tylenol), ibuprofen (Advil), or naproxen (Aleve). ● For major burns: ○ Make sure that the patient is safe and out of harm’s way. Move the patient away from the source of the burn. If it’s an electrical burn, turn off the power source before touching the patient. ○ Check to see if the patient is breathing. If needed, start rescue breathing if you’ve been trained. 23 ○ Remove restrictive items from their body, such as belts and jewelry in or near the burned areas. Burned areas typically swell quickly. ○ Cover the burned area. Use a clean cloth or bandage that’s moistened with cool, clean water. ○ Avoid immersing the burned patient in water. Hypothermia (severe loss of body heat) can occur if you immerse large, severe burns in water. ○ Raise the burned area. If possible, elevate the burned area above their heart. ○ Watch for shock. Signs and symptoms of shock include shallow breathing, pale complexion, and fainting. • • • • • Give orals fluids to assist vomiting, if directed by a physician. If the person vomits, turn his or her head to the side to prevent choking and aspiration of vomitus and assist in keeping the airway open. Poison on the skin. Remove any contaminated clothing using gloves. Rinse the skin for 15 to 20 minutes in a shower or with a hose. Poison in the eye. Gently flush the eye with cool or lukewarm water for 20 minutes or until the physician arrives. Inhaled poison. Get the person into fresh air as soon as possible. Choking (Partial or complete obstruction) Interventions: • Partial Obstruction o Ask patient to cough and expel the foreign body. o Let the patient spit out the object if it's in his/her mouth. • Complete Obstruction: o Stand behind the patient and slightly to one side. Support the chest with 1 hand. Lean the patient forward so the object blocking the airway will come out of the mouth, rather than moving further down. o Give up to 5 sharp blows between the patient’s shoulder blades with the heel of your hand. The heel is between the palm of your hand and your wrist. o Check if the blockage has cleared. If not, give up to 5 abdominal thrusts. Don't give abdominal thrusts to babies under 1 year old or pregnant women. o If the person's airway is still blocked after trying back blows and abdominal thrusts, get help immediately. o If the patient loses consciousness and is not breathing, begin cardiopulmonary resuscitation (CPR) with chest compressions. Frostbite Interventions: • • • • Rewarming of the skin. If the skin hasn't been rewarmed already, rewarm the area using a warm-water bath for 15 to 30 minutes. The skin may turn soft and gently move the affected area as it rewarms. Administer oral pain medicine, if advised by the doctor as the rewarming process can be painful and the patient will likely need a drug to ease the pain. Wound care. A variety of wound care techniques may be used, depending on the extent of injury. Whirlpool therapy or physical therapy. Soaking in a whirlpool bath (hydrotherapy) can aid healing by keeping skin clean and naturally removing dead tissue. Poisoning (Irritant, narcotics, and corrosives) Interventions: • Swallowed poison. Remove anything remaining in the person's mouth. If the suspected poison is a household cleaner or other chemical, read the container's label and follow instructions for accidental poisoning. 24 Dislocation • Interventions: ● Don't delay medical care. Get medical help immediately. ● Don't move the joint. Until the patient receives medical help, splint the affected joint into its fixed position. Don't try to move a dislocated joint or force it back into place. Attempting to move or jam a dislocated bone back in can damage blood vessels, muscles, ligaments, and nerves. ● Put ice on the injured joint. This can ease swelling and pain in and around the joint by controlling internal bleeding and the buildup of fluids in and around the injured joint. Strain Interventions: • • • • • The main treatment is RICE (rest, ice, compression, and elevation). o Rest, to give the injured limb a break o Put ice to affected area to dull the pain o Apply compression to reduce the swelling o Elevate the injury to reduce swelling and pain Elevate or immobilize the affected joint, and apply ice packs immediately. Assist with tape, splint or cast application, as necessary To manage the pain, over-the-counter pain relievers may be helpful. Physical therapy rehabilitation may be required to some strain injuries to help the tissue heal and to retain and strengthen the muscles and tendons. A more severe strain may require evaluation by a doctor if the symptoms or pain don't improve while treating the injury. Sprain • • • After the acute inflammatory stage (24 to 48 hours after injury), heat may be applied intermittently (for 15 to 30 minutes four times a day) to relieve spasm and to promote vasodilation, absorption and repair. If the sprain is severe such as torn muscle fibers and disrupted ligaments, surgical repair or cast immobilization may be necessary so that the joint will not lose its stability. Instruct the client to allow the muscle or tendon to rest and repair itself by avoiding use for approximately a week and then by progressing activity gradually until healing is complete. Administer prescribed medications, which may include nonopioid analgesics. Fractures Interventions: ● Immediately after injury, if a fracture is suspected, it is important to immobilize the body part before the patient is moved. ● Adequate splinting is essential to prevent the movement of fracture fragments. ○ In an open fracture, the wound should be covered with a sterile dressing to prevent contamination of the deeper tissues. ● Maintain bed rest or limb rest as indicated. Provide support of joints above and below the fracture site, especially when moving and turning. ● Position the patient, so that appropriate pull is maintained on the long axis of the bone. This promotes bone alignment and reduces the risk of complications (delayed healing and nonunion). ● Elevate extremity. The affected extremity is elevated to minimize edema. Interventions: • Elevate or immobilize the affected joint, and apply ice packs immediately o Assist with tape, splint or cast application, as necessary 25 Shock • Interventions: • • • • • • • • Let the patient lie down. This is the most comfortable position. If the patient is in pain, letting him or her rest is crucial. Pain may further intensify stress and accelerate the progression of shock. Call for medical help. Shock can’t be managed by first aid alone. The patient still needs emergency medical care. Maintain the patient’s normal body temperature. Keep him or her warm if the body is getting cold. If the patient is vomiting or bleeding from the mouth, turn the patient on his or her side to prevent choking or aspiration. If you suspect a spinal cord injury, let him lie flat on the floor. If the patient stops breathing, open the airway and check for breathing. Begin cardiopulmonary resuscitation (CPR). Continue until help arrives or the patient starts breathing again. Symptoms: sudden decrease in blood pressure • Promote airway clearance. Maintain a lying position, flat surface. Loosen clothing from neck or chest and abdominal areas. Clear away dangerous objects, if the person is moving. Don't try to restrain someone having a seizure. Avoid putting your fingers or other objects in the person's mouth. Stay with the person until medical personnel arrive. Observe the person closely so that you can provide details of the happening. Picture Material Description Cravat / Triangular bandage Used as an arm sling to support the injury. Fainting Interventions: • • • • Position the person on his or her back. If there are no injuries and the person is breathing, raise the person's legs above heart level. Loosen constrictive clothing such as belts and collars. Check for breathing. If the person isn't breathing, begin CPR. Continue CPR until help arrives or the person begins to breathe. To reduce the chance of fainting again, don't get the person up too quickly. If the person doesn't regain consciousness within one minute, call for help. Seizure Interventions: • Ease the patient to the floor. Turn him/her gently onto one side, this will help the person breathe and place something soft under his or her head. Hard splint I. A supportive device used to keep in place any suspected fracture in one’s limbs. Bandaging - The application of a strip or roll of cloth or other material that may be wound around a part of the body in a variety of ways to secure a dressing, maintain pressure over a compress, or immobilize a limb or other part of the body. 26 Materials needed for Bandaging: Cravats Procedure Guide for Bandaging PROCEDURE RATIONALE Triangular Bandages Making a broad-fold bandage Making a narrow-fold bandage 1. Fold a triangular bandage to make a This is a necessary step as the semi broad-fold bandage. narrow fold bandage requires 3 folds unlike the semi broad-fold which requires 2. 1. Open out a triangular bandage and Opening it on a clean surface would fold the bandage in half horizontally, prevent contamination and makes so that the point of the triangle it easier to fold the bandage. touches the center of the base. 2. Fold the bandage horizontally in half Folding it once more created a again. It should form a long, narrow bandage used to apply on narrow, thick strip of material. smaller body parts. 2. Fold the triangular bandage in half The apex should be folded down to again, in the same direction, so that the base twice to create a broadthe first folded edge touches the fold bandage ready for application. base. The bandage should now form a broad strip Scalp Injury 1. Fold a hem along the base of the bandage. Place the bandage on the casualty’s head with the hem underneath and the center of the base just above his eyebrows. Folding along the base creates a cushion to support the head. Placing the hem just above the eyebrows ensures that the patient’s eyes are not covered. 27 2. Wrap the ends of the bandage securely around the casualty’s head,tucking the hem just above his ears. Cross the two ends at the nape of the casualty’s neck, over the point of the bandage. Proper wrapping will thoroughly secure the bandage on the patient’s head. Ensure that the crossed ends are not too tight and not too loose. of the casualty’s head. Tie ends in a reef knot (opposite) at the centre of the forehead, positioning it over the hem of the bandage. Tuck the free part of each end under the knot. against the patient’s head. Using this type ensures that the knot is secure and will not slip. The tucking is done to ensure no complications from a stray cloth and will display neatness. 4. Steady the casualty’s head with one hand and draw the point down to tighten the bandage. Then fold the point up over the ends and pin it at the crown of his head. If you do not have a pin, tuck the point over the ends. Tightening thoroughly secures the bandage and it also ensures compression in order to stop the bleeding of the injury and pinning or tucking secures the bandage. 3. Bring the crossed-ends to the front The reef knot secures the bandage 28 2. Fold the lower end of the bandage This ensures a neat and secure up over the forearm and bring it to sling so no complications arise. meet the upper end at the shoulder. Arm Sling 1. Ensure that the injured arm is supported with the hand slightly higher than the elbow. Fold the base of the bandage under to form a hem. Place the bandage with the base parallel to the casualty’s body and level with his little fingernail. Slide the upper end under the injured arm and pull it around the neck to the opposite shoulder. The injured arm should be given proper support and elevation to prevent further harm. Positioning the injured arm on teh bandage and sliding the upper ends around the neck anchors the bandage in place. 3. Tie a reef knot on the injured side, at the hollow above the casualty's collarbone. Tuck both free ends of the bandage under the knot to pad it. A reef (square) knot is secure and will not slip. Directing the knot in that position prevents pressure on the back of the neck. 29 necessary, loosen and reapply the tight, can restrict blood circulation bandages and sling. to teh area beyond it. If this occurs, the bandage must be reapplied more loosely. Elevation Sling 4. Fold the point forward at the To hold the arm securely and to casualty's elbow. Tuck any loose display neatness. fabric around the elbow, and secure the point to the front with a safety pin. If you do not have a pin, twist the point until the fabric fits the elbow snugly; tuck it into the sling at the back of the arm. 1. Ask the casualty to support his To support the injured area before injured arm cross his chest, with the bandages are applied and to fingers resting on the opposite prevent further injury. shoulder. 2. Place the bandage over his body, To restrict and immoblize the with one end over the uninjured injured shoulder. shoulder. Hold the point just beyond his elbow. 5. As soon as you have finished, check Checking circulation is important the circulation in the fingers. because limbs can swell after an Recheck every 10 minutes. If injury, and a bandage, if done too 30 to pad it. 3. Ask the casualty to let go of his To allow the nurse to start the injured arm. Tuck the base of the process of supporting and bandage under his hand, forearm, stabilizing the injury. and elbow. 6. Twist the point until the bandage fits closely around the casualty’s elbow. Tuck the point in just above his elbow to secure it. If you have safety pin, fold the fabric over the elbow, and fasten the point at the corner. prevents any complication that a stray cloth may bring. Twisting the point is to hold the elbow securely, avoid any injury, and display neatness. Circulation must be checked to know whether nerves are damaged, and if so, the bandage must be redone to be not too tight. 4. Bring the lower end of the bandage To allow the sling to raise the up diagonally across his back, to injured arm and bring it closer to meet the other end at his shoulder. the body. 5. Tie the ends in a reef knot at the A reef (square) knot is secure and hollow above the casualty’s collar will not slip. Tucking the excess bone. Tuck the ends under the knot fabric ensures neatness and it also 7. Regularly check the circulation in To check circulation is important the thumb. If necessary, loosen and because limbs can swell after an reapply the bandage and sling. injury, and a bandage, if done too tight, can restrict blood circulation to teh area beyond it. If this occurs, the bandage must be reapplied more loosely. 31 II. Splinting - The process of immobilizing, restraining or supporting a body part; stabilization, immobilization and/ or protection of an injured body part with a supportive appliance. Materials needed for Splinting: Hard Splints 2. Position the arm on a rigid splint The rigid splint will immobilise the arm. 3. Secure the splint A bandage is used to secure the splint in place. Procedure Guide for Splinting PROCEDURE RATIONALE Triangular Bandages Arm Sling and Binder 1. Support the arm To ensure that no further harm will happen. 32 4. Check circulation Circulation must be checked to prevent injury to the nerves and other tissues. This can be checked through the patient’s fingernails. If circulation is poor, the bandage must be adjusted, making sure it is not too tight. 5. Position the triangular bandage. To use for the arm sling the patient will use. 6. Bring the lower end of the To have both ends ready to be tied bandage to the opposite side of around the patient’s neck. the neck. 7. Tie the ends using a square knot A square knot is secure and will not slip. 33 8. Secure the point of the bandage To ensure that it fits the elbow snugly at the elbow. and secure the bandage. Splinting the Leg 9. Tie a binder bandage over the To secure the arm of the patient. sling around the chest. 1. Gently slide 4 or 5 bandages or To secure the splint in place. strips of cloth under both legs. 34 2. Put padding between the legs. To use as a cushion for both legs so that they will not come in contact. 4. Tie the bandages To securely fasten the splint and bandages in place. 3. Gently slide the uninjured leg next This must be gently done to not cause to the injured leg. further injury to the injured leg. 35 RLE MODULE 3F: TRANSFER AND AMBULATION DEFINITION OF TERMS 1.1 Transfer - The act of moving a person with limited function from one location to another. 1.4 Non-ambulatory - An individual physically or mentally unable to walk or traverse a normal path to safety without the physical assistance of another. 1.2 Ambulation - The capacity to move independently from one location to another while using or without a mobility aid. 1.5 Alignment - Refers to how the head, shoulders, spine, hips, knees and ankles relate and line up with each other. 1.3 Ambulatory - Promotion and assistance with walking to maintain or restore autonomic and voluntary body functions during treatment and recovery from illness or injury 36 1.6 Braces - A medical device used in orthopedics to retain, align, or support a body part in the proper position 1.7 Canes - Canes or walking canes are one of several devices available to assist in ambulation, or walking. 1.8 Carry - To hold or support while moving 1.9 Crutches - Is a wooden or metal staff used to aid a patient’s mobility impairment or an injury that limits walking ability. 1.10 Gait - The way or manner in which you walk. Depends on how well a person can balance and support their weight. 1.11 Hydraulic lift - A tool that can help transfer an immobile or obese patient safely from the bed to a chair. 37 1.14 Movement - The act or process of moving. 1.12 Lift sheet - The medical field uses this sheet to get immobile patients out of bed. It is around the size of a typical sheet and is available in cotton, plastic, or rubber. When lifting, it provides support for the body from the upper back to the mid-thigh. 1.13 Mobility - The quality or state of being mobile. 1.15 Orthostatic hypotension - A client's blood pressure that drops when they stand or sit suddenly. It typically results from peripheral vasodilatation, in which blood departs from central body organs, particularly the brain, and flows to the periphery, frequently making the person feel dizzy. 38 1.16 Stretcher - A device used for carrying a sick, injured, or dead person. 1.19 Weight - A measure of the heaviness of an object. 1.20 Wheelchair - Is a device used for mobility by people for whom walking is difficult or impossible, due to illness or disability. 1.17 Transfer belt - A device used primarily to help a patient to transfer between bed and wheelchair or wheelchair and toilet or car. 1.18 Walker - An enclosing framework of lightweight metal tubing, sometimes with wheels, for patients who need more support in walking. CLO#2: discuss the importance, indications and contraindications, and factors affecting transfer and ambulation Importance of Transfer and Ambulation Transfer ● Permits a patient to function in different environments ● Increases the level of independence of the patient 39 ● Maximizes the ability to encompass a task with minimal effort and maximum safety ● Mobilizes client without causing injury and falls ● Prevents systematic hazards of immobilization Ambulation ● Stimulates blood circulation throughout the body, preventing inflammation in the veins and the development of stroke-causing clots ● Improves joint flexibility, especially that of the hips, knees, and ankles ● Assures fast healing; helps the patients in building strength and muscle tone, which eventually leads to improvement of oxygen delivery into the blood tissues ● Enhances the movement of their abdominal muscles; gradually helps in stimulating the intestinal tract and therefore prevents constipation ● Prevents urinary tract incontinence and infection; clients are able to go to the bathroom on their own ● Relieves pressure on the body and skin, which helps prevent ulcers ● Feelings of independence helps improve client’s self-esteem Indications of Transfer and Ambulation Transfer ● Client needs to be transported to another room or unit ● Client has a treatment or diagnostic test ● Client who is permitted out of the bed Ambulation ● Client's need for mobility ● Elderly person ● Pregnant women ● Post-surgery clients ● Continued bed exercise for muscle strengthening Contraindications for Transfer and Mobility Transfer ● Clients who have spinal injury ● Clients who have undergone spinal surgery ● Clients that have severe wounds or burns Ambulation ● Spinal injury ● Paralyzed legs ● Contraindicated by the doctors Factors Affecting Transfer and Ambulation Transfer ● Postoperative clients ● Existing injuries or wounds ● Unfamiliarity with equipment ● Inexperienced provider ● Poor communication with the receiving facility Ambulation ● Postoperative clients ● Severe trauma clients ● Patients on complex medications and/or infusion regimes ● Insufficient preparation of the client ● Poor communication with the receiving facility CLO#3: explain the principle involved in transfer and ambulation 3.1 Body Mechanics - Body mechanics involves standing and moving one's body so as to prevent injury, avoid fatigue, and make the best use of strength. You can safely control and move another person if you learn to control and balance your own body. 3.2 Safety and Security - This procedure involves safety and security to prevent and reduce risks, errors, and harm to patients and health providers while providing health care. 3.3 Microbiology - Maintaining a clean surrounding and of course doing hand washing before getting contact with the client is a must to avoid possible infections. 3.4 Psychology - Proper approach to the patient and administration in transferring the patient will let the patient feel safe and away from worrying 40 that anything bad will happen. 3.5 Physics - Physics is involved in the procedure in terms of the energy and force in transferring the patient and the friction between the patient and the board. Also when the health providers keep the heaviest part of the patient near the health providers center of gravity for stability. 3.6 Anatomy and Physiology - Having enough knowledge about the Anatomy and Physiology will allow the care provider to easily determine which part of the body would be the heaviest or the lightest or which part of the patient should be taking care of. 3.7 Time and Energy - Preparing the materials needed in transferring the patient and ambulation requires enough time and energy. Also when they are transferring the patient they need sufficient energy to position and transfer the client to the stretcher. - Patient-handling tools mostly utilized in pre-hospital trauma care. Purpose: to give a person with suspected spinal or limb damage stiff support while they are moving. 4.1.3 Wheel chair - a wheeled chair that is used when walking is difficult or impossible because of an illness, injury, age- or disability-related issues. Purpose: specifically made to be used for indoor or both indoor and outdoor locomotion by a person with a mobility impairment. CLO#4: describe the mechanical devices used in transferring and ambulating patients as to its description and purpose. 4.1 Mechanical devices used in transferring patients: 4.1.1 Stretcher - a tool or equipment that stretches or expands material. Purpose: to lift a person who must lie flat and is unable to move independently. 4.1.4 Transfer belt - equipment that a caregiver places on a patient with mobility problems before transporting the patient. Purpose: to help a patient safely transition from a standing position to a wheelchair 4.1.2 Spine board 41 4.1.5 Hydraulic lift - Devices for transferring patients from beds to wheelchairs, commodes by the bed, and bathtubs Purpose: utilized with patients who are too heavy to be properly moved by members of the healthcare team, have physical restrictions such amputations or quadriplegia, or who are unable to bear weight at all. 4.2.2 Walkers - a four-point walking assistance that makes contact with the ground. Purpose: help stabilize patients who have lower extremity disability or poor balance and mobility. 4.2.3 Crutches - Medical devices that shift bodily weight from the legs to the torso and arms to help with ambulation. Purpose: utilized to help people who have neurological disability or lower extremity injuries. 4.2 Mechanical devices used in ambulating patients: 4.2.1 Canes - a device that offers a little balance and support for walking and standing. Purpose: to help people who are weak, unsteady, in pain, or have lost their balance during ambulation and transfers. CLO#5: explain the guidelines in the measurement of crutches and proper use of crutches 42 5.1 Measurement of Crutches The handgrips of the crutches should be at a height which allow elbows to be bent at about 30°. Adult and children – measure from position of hand by side when elbow is 30° bent, with patient standing upright, to ground 4 inches away from side of foot. 5.2 Measurement of Axillary Crutch MEASUREMENT OF AUXILIARY CRUTCHES With patients’ shoes on, stand tall. Put their arms below the crutches. Let their arms swing down over the crutches with ease. With their hands hanging loosely, there should be two inches between their armpit and the top of the crutch. When holding the hand grips, they should be level with patients’ wrist. Their elbows should be slightly bent at a 30-degree angle. 5.3 Measurement of Elbow Crutch MEASUREMENT OF ELBOW CRUTCHES If the patient is standing up straight, measure from the side of the hand where the elbow is bent by 30 degrees to the distance of the ground, which should be 4 inches. Height should be adjusted to allow for 20–30 degrees of elbow flexion while keeping shoulders relaxed. 5.4 Guidelines in proper use of crutches Proper Use of Crutches Stand upright. Put the crutches' tops under their arms. Place the ends 5 to 8 inches (or 12 to 20 cm) to the side of your feet. If there is 2 to 3 fingers between the top of the crutch pad and the patient's armpit, the crutches are the right length. When their arm is hanging by their side, the hand grasp should be at wrist level. As the patient presses down on the hand grips, their elbows are slightly bent. Remember: The weight should be supported with the hand grips, not the crutch pads under your armpits. 5.4.1 Proper positioning ● When standing up straight, the top of your crutches should be about 1-2 inches below your armpits. ● The handgrips of the crutches should be even with the top of patients’ hip line. ● Patients’ elbows should be slightly bent when holding the handgrips. ● To avoid damage to the nerves and blood vessels in patients’ armpits, their weight should rest on your hands, not on the underarm supports. 5.4.2 Proper walking ● Lean forward slightly and put your crutches about one foot in front of you. ● Begin your step as if you were going to use the injured foot or leg but, instead, shift your weight to the crutches. ● Bring your body forward slowly between the crutches. Finish the step normally with your good leg. When your good leg is on the ground, move your crutches ahead in preparation for your next step. Always look forward, not down at your feet. 5.4.3 Proper sitting ● The patient positions himself or herself at the center front of the chair with the posterior aspect of the legs touching the chair. ● Then the patient holds both crutches in the hand opposite the affected weight-supporting braces. ● The patient holds the crutches in the hand on his or her stronger side. 43 5.4.4 Proper standing up ● Patient should inch themselves to the front of the chair. ● Hold both crutches in the hand of the injured side. ● Patient should push up and stand on their good leg. 5.5.5 Using the stairs with crutches ● (Ascending stairs) ○ The patient usually uses a modified three-point gait. ○ He/she stands at the bottom of the stairs and transfers body weight to the crutches . ○ He/she advances the unaffected leg between the crutches to the stairs. ○ The patient then shifts weight from the crutches to the unaffected leg. ○ Finally he/she aligns both crutches on the stairs. ○ The patient repeats this sequence until he or she reaches the top of the stairs. ● (Descending stairs) ○ A three-phase sequence is also used to descend the stairs ○ The patient transfers body weight to the unaffected leg. ○ He/she places the crutches on the stairs and begins to transfer body weight to them, moving the affected leg forward. ○ Finally the patient moves the unaffected leg to the stairs with the crutches. ○ The patient repeats the sequence until reaching the bottom of the stairs. CLO#6: explore safety points or issues when a patient is on a stretcher and wheelchair and the basic guidelines in transferring and ambulating patients 6.1 Safety points to consider when using a Stretcher Properly Place the Stretcher - Properly placing a stretcher into an ambulance is a part of proper stretcher handling. If a stretcher is in the ambulance, make sure that it is firmly fastened to prevent movement while the patient is being transported to the hospital. Look at the Stretcher’s Legs - Inspection of the Stretcher’s leg is very advisable since some screws or nuts may be loosened and it must be tightened due to usage. To avoid any accidents, the stretcher must be examined and made sure it is fastened in place. Check the Wheels on the Stretcher - Checking the wheels of a stretcher ensures the safety of the patients. Some stretcher brakes are not functioning well due to usage of which. Assess the Weight of the Patient - Stretchers are designed to be durable. Stretchers must be able to support the patient's weight even though they are made to be sturdy. Stretchers must be able to support the patient's weight even though they are made to be sturdy. Opt for Level Ground When Possible - A stretcher should be placed on flat ground for the safety of both the transporter and the patients. This is advised to avoid an accident where one of the EMS personnel loses their balance or footing. Hold the Handles During Transfers - The handles must be grasped as the stretcher is pushed into the location where it will be put when patients are transferred into or out of an ambulance. Medical workers should release their grip on the handles only after the stretcher is in position. During transfers from stretcher to bed or the other way around, the stretcher's handles should be tightly grasped. 44 6.2 Safety points to consider when using a wheelchair in both LE. ● Provides best balance & stability for person but must be able to weight bear on both legs with your right foot. The pattern is right crutchleft foot and left crutchright foot. This gait pattern is used when one of the lower extremities (LE) is unable to fully bear weight (due to fracture, amputation, joint replacement, etc). ● Allows the individual to eliminate all the weightbearing on the affected leg There are three points of contact with the floor. The crutches serve as one point, the involved leg as the second point, and the uninvolved leg as the third point. Both crutches move forward, the affected limb then steps up to the crutches. This is followed by the weight-bearing limb which steps through, beyond the crutches. There are always three points of contact with the floor at any given time. Make sure the patient's seat belts are securely fastened - Being buckled in any type of device or vehicle helps you keep safe and secure. If you don't buckled up with seat belt this might throw you rapidly and can cause accident. Patients feet are on the footplate - The stability of a patient's fully loaded feet on the proper footplate can lower the chance of slipping and falling out of the chair and helps maintain excellent posture while seated. Always lock the brakes before getting in and out of the wheelchair - Before a patient will sit in a wheelchair we must first check and lock the brakes for a sudden stop or if not, it will lead you to an accident. Regular Maintenance is very important - Providing regular check up for the wheelchair is a must, thus this will help prolong the life of the device. Also this will help you know what to repair when it is broken. Avoid putting heavy loads on the back of a wheelchair - Avoid placing any kind of things which are heavy thus this will cause the wheelchair to tip backwards in transferring the patients. Only attach useful and light items for your safety. CLO#7: Discuss the different type of gaits and carry including its indications, advantages and guidelines 7.1 Types of gait Type of gait Indications 1. Four-point gait This gait pattern is most commonly used when there is a lack of coordination, poor balance and muscle weakness Advantages ● It provides a slow and stable gait pattern with four points of support. Guidelines To use this gait, put the right crutch out and step with the left foot. Then put the left crutch out and step 2. Three-point gait 45 3. Two-point gait 4. Swing-To gait This gait pattern is used when the patient can bear some weight on both lower extremities. ● Faster than a Four point gait. Place the patient in the tripod position and instruct him to do the following: 1. Move the right leg and left crutch forward together. 2. Move the left leg and the right crutch forward together. 3. Repeat this sequence for the desired ambulation. Also known as "step-to", this gait type is common with individuals with limited use of both lower extremities and/or trunk instability (one or both feet make contact with the floor). ● Provides stability ● Can use this gait with a walker. Place the patient in the tripod position and instruct him to do the following: 1. Advance both crutches 2. Lift both feet/Swing forward/land feet next to crutches 3. Repeat the sequence in rhythm for desired ambulation. 5. Swing-Through This gait pattern is used for patients with lower extremities that are paralyzed and/or in braces. ● Faster, but requires more energy Place the patient in the tripod position and instruct him to do the following: 1. Move both crutches forward together about 6 inches. 2. Move both legs forward together about 6 inches. 3. Repeat the sequence in rhythm for desired ambulation. 7.2 Types of Carry Type of carry Indications Advantages Guidelines One-Person help 1. One-Person Walk Assist This type of carry is used when the victim can selfextricate with ● The oneperson walk assist offers the least 1. Place victim's arm around your neck and hold their wrist 46 2. Firefighter Carry 3. Pack Strap Carry little or no assistance as walking wounded. chance for injury to both rescuer and victim. 2. Place your arm nearest to them around their waist and walk with them to safety This type of carry should only be conducted by a very strong rescuer and a smaller victim. ● It allows the rescuer to move the victim across significant distances, quickly, the technique is used to carry injured people away from danger. 1. With victim lying down, hook your elbows under their armpits 2. Raise them to a standing position 3. Place your right leg between the victim's legs 4. Grab the victim's right hand with your left 5. Squat and wrap your right arm around the victim's right knee 6. Stand and raise the victim's right thigh over your right shoulder ● It is a quick, down-and- 1. Facing away from the victim, place their arms The pack-strap carry is generally used to carry a conscious or unconscious casualty for a moderate distance. This carry is not used if the casualty has a broken arm or wrist. dirty way to over your move a shoulders. victim 2. Cross the quickly. victim's arms grasping the opposite wrist and pull close to your chest. 3. Squat, lean slightly forward, and drive your hips into the victim as you stand. Two-Person help 1. Two-Person Extremity Carry This type of carry is best suited for moving a victim over even terrain, such as along a paved path or within a building. ● It is easily performed ● Both conscious and unconscious victims can be carried in this manner. 1. Help the victim to a seated position. 2. First rescuer kneels behind the victim, reaches under their arms, and grabs their wrists. 3. Second rescuer backs between the victim's legs, squats down, and grabs behind the knees. 4. Stand at the command of the rescuer at the head, focusing on 47 using your legs rather than your back. 2. Chair Carry 3. Two-Handed Seat Carry This is a particularly good method to use when you must carry a person up or down stairs or through narrow, winding passageways. ● This makes the transport of a victim significantly easier on the rescuers. 1. Place victim in a sturdy chair 2. First rescuer stands behind, grabs the back of the chair, and leans it back on its hind legs 3. Second rescuer backs to the chair, squats down, and grabs the front legs of the chair 4. Stand at the command of the rescuer at the head The two-handed seat carry should only be conducted on conscious victims. ● This technique is for carrying a victim longer distances. 1. Each rescuer should kneel on either side of the seated victim. 2. Link arms behind the victim's back. 3. Place your free arms under the victim's knees and link arms. 4. Place victim's arms around the shoulders of rescuers and stand together. Three-Person help 1. Hammock carry This type of carry is helpful when the patient is unconscious or cannot move and needs to be moved. ● Efficient for patients that are heavier than the average person. 1. Reach under the victim and grasp one wrist on the opposite rescuer. 2. The rescuers on the ends will only be able to grasp one wrist on the opposite rescuer. 3. The rescuers with only one wrist grasped will use their free hands to support the victim's head and feet/legs. 4. The rescuers will then squat and lift the victim on the command of the person nearest the head, remembering to use proper lifting techniques. 48 2. Three-person carry or Stretcher lift This technique is for lifting patients onto a bed or stretcher, or for transporting them short distances. ● Help protect victims from further injuries and provide greater stability for patients. 1. Each person kneels on the knee nearest the victim's feet. 2. On the command of the person at the head, the rescuers lift the victim up and rest the victim on their knees. If the patient is being placed on a low stretcher or litter basket: 3. On the command of the person at the head, the patient is placed down on the litter/stretcher. If the victim is to be placed on a high gurney/bed or to be carried: At this point, the rescuers will rotate the victim so that the victim is facing the rescuers, resting against the rescuers' chests. 3. On the command of the person at the head, all the rescuers will stand. 4. To walk, all rescuers will start out on the same foot, walking in a line abreast. CLO#8: discuss nursing responsibilities before, during and after ambulating and transferring patients. CLO#9: demonstrate the beginning skills. 9.1 Transferring patients from bed to chair to wheelchair Safety considerations: ● Check rooms for additional precautions ● Introduce yourself to patient ● Confirm patient ID using two patient identifiers (e.g., name and date of birth) ● Listen and attend to patient cues ● Ensure patient’s privacy and dignity ● Assess ABCCS(airway, breathing, circulation, consciousness, safety)/suctions/oxygen/safety ● Ensure tubes and attachments are properly placed prior to the procedure to prevent accidental removal 49 ● A gait belt and wheelchair are required PROCEDURE RATIONALE a patient has weakness on one side, place the wheelchair on the strong side. 1. One health care provider is required. The patient should be assessed as a 1person assist. 2. Perform hand hygiene. Explain what This step provides the patient with an will happen during the transfer and opportunity to ask questions and help how the patient can help. with the positioning. Apply proper ambulation footwear prior to Wheelchair with one leg rest removed 4. Sit patient on the side of the bed The patient’s feet should be in between with his or her feet on the floor. Apply the health care provider’s feet. the gait belt snugly around the waist (if required). Explain procedure to patient Proper footwear Place hands on waist to assist into a standing position Patient position prior to standing 3. Lower the bed and ensure that Ensure brakes are applied on the brakes are applied. wheelchair. Place the wheelchair next to the bed at a 45-degree angle and apply brakes. If 50 5. As the patient leans forward, grasp the gait belt (if required) on the side the patient, with your arms outside the patient’s arms. Position your legs on the outside of the patient’s legs. The patient’s feet should be flat on the floor. Assist to a standing position using a gait belt 6. Count to three and, using a rocking motion, help the patient stand by shifting weight from the front foot to the back foot, keeping elbows in and back straight. Assist into the wheelchair 8. As the patient sits down, shift your This allows the patient to be properly weight from back to front with bent positioned in the chair and prevents knees, with trunk straight and elbows back injury to health care providers. slightly bent. Allow patient to sit in wheelchair slowly, using armrests for support. Weight shift to back leg by health care provider 7. Once standing, have the patient take Ensure the patient can feel the a few steps back until they can feel the wheelchair on the back of the legs prior wheelchair on the back of their legs. to sitting down. Have the patient grasp the arm of the wheelchair and lean forward slightly. Transfer to wheelchair 9.2 Transferring from bed to stretcher and vice versa 51 ● ● ● ● ● ● ● ● ● Safety considerations: Perform hand hygiene Check room for additional precautions Introduce yourself to patient Confirm patient ID using two patient identifiers (e.g., name and date of birth) Listen and attend to patient cues Ensure patient’s privacy and dignity Assess ABCCS (airway, breathing, circulation, consciousness, safety)/suctions/oxygen/safety Ensure tubes and attachments are properly placed prior to the procedure to prevent accidental removal A slider board and full-size sheet or friction-reducing sheet is required for the transfer PROCEDURE Chin tucked in and arms across chest 3. Raise bed to safe working height. Safe working height is at waist level for Lower head of the bed and side rails. the shortest health care provider. Position the patient closest to the side The patient must be positioned of the bed where the stretcher will be correctly prior to the transfer to avoid placed. straining and reaching. RATIONALE 1. Always predetermine the number of Three to four health care providers are staff required to safely transfer a required for the transfer. patient horizontally. 2. Explain what will happen and how This step provides the patient with an the patient can help (tuck the chin in, opportunity to ask questions and help keep hands on chest). with the transfer. Collect supplies. May need additional health care providers to move the patient to the side of the bed. 4. Roll patient over and place slider The slider board must be positioned as board halfway under the patient, a bridge between both surfaces. forming a bridge between the bed and the stretcher. The sheet must be between the patient and the slider board to decrease Place sheet on top of the slider board. friction between patient and board. The sheet is used to slide patient over to the stretcher. The patient is returned to the supine position. Patient’s feet are positioned on the slider board. Stretcher and slider board Place slider board 52 Ensure all tubes and attachments are out of the way. 5. Position stretcher beside the bed on The position of the health care the side closest to the patient, with providers keeps the heaviest part of stretcher slightly lower. Apply brakes. the patient near the health care providers’ centre of gravity for stability. Two health care providers climb onto the stretcher and grasp the sheet. The lead person is at the head of the bed and will grasp the pillow and sheet. The other health care provider is positioned on the far side of the bed, between the chest and hips of the patient, and will grasp the sheet with palms facing up. Caregiver at the head of the bed The two caregivers on the stretcher grasp the draw sheet using a palms up technique, sitting up tall, and keeping their elbows close to their body and backs straight. The caregiver on the other side of the bed places his or her hands under the patient’s hip and shoulder area with forearms resting on bed. 7. The designated leader will count 1, Coordinating the move between health 2, 3, and start the move. care providers prevents injury while transferring patients. The person on the far side of the bed will push patient just to arm’s length Using a weight shift from front to back using a back-to-front weight shift. uses the legs to minimize effort when moving a patient. At the same time, the two caregivers on the stretcher will move from a sitting-up-tall position to sitting on their heels, shifting their weight from the front leg to the back, bringing the patient with them using the sheet. 8. The two caregivers will climb off the stretcher and stand at the side and grasp the sheet, keeping elbows tucked in. The step allows the patient to be properly positioned in the bed and prevents back injury to health care providers. One of the two caregivers should be in line with the patient’s shoulders and the other should be at the hip area. On the count of three, with back straight and knees bent, the two caregivers use a front-to-back weight shift and slide the patient into the middle of the bed. Caregiver at the head of the bed Weight on front leg Shift weight to back foot 53 9. At the same time, the caregiver on This step allows the patient to lie flat the other side slides the slider board on the bed. out from under the patient. 10. Replace pillow under head, ensure This promotes comfort and prevents patient is comfortable, and cover the harm to patient. patient with sheets. 11. Lower bed and lock brakes, raise Placing bed and side rails in a safe side rails as required, and ensure call position reduces the likelihood of injury bell is within reach. to patient. Proper placement of call bell facilitates patient’s ability to ask for Perform hand hygiene. assistance. Bed in lowest position, side rail up, call bell within reach Hand hygiene reduces the spread of microorganisms. Hand hygiene with ABHR (AlcoholBased Hand Rub) 9.3 Proper transport of patient using: stretcher and wheelchair (flat or level surface, ramps or inclined surfaces, through doors and elevators), canes, crutches, and walkersa 9.3.1 Stretcher ● Use hall ceiling mirrors at intersections before turning corners. ● Lock stretcher brakes when standing still. ● Always push a stretcher from the end where the client’s head is positioned as this position protects the client’s head in the event of a collision. ● Fasten safety straps across the client on a stretcher and raise the side rails. ● Ramps or inclined surfaces: - Stand at the head of the stretcher to push the stretcher up a ramp. - Back down a steep ramp while positioned at the head of the stretcher ● Doors and elevators: - Lock elevator door open when entering or exiting. - Maneuver the stretcher when entering the elevator so that the client’s head goes in first 9.3.2 Wheelchair ● Flat or level surfaces: - Lock brakes when the wheelchair is standing still. - Intravenous infusion bags can be placed on portable IV poles attached to the wheelchair during transport. - Ensure the client is positioned well back in the seat of a wheelchair. - Use seat belts that fasten behind the wheelchair to protect confused patients from falls. 54 ● Ramps or inclined surfaces - Back slowly down wheelchair ramps. - Push the wheelchair ahead of you when going up ramps or inclined surfaces. - Place your body between the wheelchair and the bottom of an incline. ● Doors and elevators: - If going through a self-closing door, back the wheelchair out of the room. You can keep the door open by backing against the door. The wheelchair can then be guided out of the room. - When pushing a wheelchair, back into and out of elevators. Rear large wheels first. 9.3.3 Canes Proper positioning ● When standing up straight, the top of the cane should reach to the crease in the patient’s wrist. ● The elbow should be slightly bent when holding the cane. ● The cane should be held in the hand opposite the side that needs support. For example, if the patient’s right leg is injured, the cane should be held in the left hand. Walking ● To start, assist the client to set the cane about one small stride ahead of the patient and step off on the injured leg. ● Inform the client to finish the step with the patient’s functional leg. Stairs ● To climb stairs: - Place the cane in the hand opposite the patient’s injured leg. - With their free hand, assist the patient to grasp the handrail. - Instruct the client to step up on their good leg first, then step up on the injured leg. ● To come down stairs: - Put the cane on the step first - Then, inform the patient to put their injured leg on the step. - Finally, put the good leg, which carries their body weight, on the step. 9.3.4 Crutches Proper positioning ● In assisting the patient with the use of crutches, make sure that the top of the crutches are about 1-2 inches below the patient’s armpits. ● Handgrips of the crutches should be even with the top of the patient’s hip line. ● When holding the handgrips, elbows must be slightly bent ● The patient’s weight should rest on their hands and not on the underarm supports to avoid damage to the nerve and blood vessels in the armpit area. Walking ● Assist the patient in slightly leaning forward and place the crutches about one foot in front of them. ● Instruct the patient to begin taking a step as if they were to use the injured foot/leg by shifting their weight onto the crutches. ● Allow them to bring their body forward in a slow manner between the crutches making sure not to stay too far from the client. Help the client in finishing the step normally with their functional leg. ● When the functional leg is on the ground, instruct the client to move the crutches in preparation for their next step. ● Advice the client to always look forward when walking and not down at their feet. Sitting ● To sit: - Make sure the client is situated in front of a sturdy chair. - Instruct the client to place their injured foot in front of them and hold both crutches in one hand. - Assist the client’s positioning making sure they are in line with the seat of the chair then slowly lower them into the chair. - Once seated, inform the patient to lean their crutches in a nearby spot making sure to lean them upside down as crutches tend to fall over when leaned on the tips. ● To stand up: - Assist the client in moving forward to the front of their chair. - Both crutches must be held by the hand on their injured side. - Assist the client in pushing them up to let them stand on their 55 functional leg. 9.3.5 Walkers Positioning ● When standing up straight, the top of the walker should reach to the crease of the patient’s wrist. ● The elbows should be slightly bent when holding the handgrips of the walker. ● Observe client making sure their is back straight not hunching over the walker. ● Check to be sure the rubber tips on the walker's legs are in good shape. If they become uneven or worn, new tips may be purchased at a drug store or medical supply store. Walking ● First, assist the client in positioning the walker about one step ahead of them, making sure that all four legs of the walker are on even ground. ● With both hands, the patient should grip the top of the walker for support and move their injured leg into the middle area of the walker. Not letting the client step all the way to the front. ● The patient should push straight down on the handgrips of the walker as they bring their good leg up so it is even with the injured leg. Assist the patient as needed making sure the patient always takes small steps when turning and moving slowly. Sitting ● To sit: - Back up until the patient’s legs touch the chair. - Assist the client’s positioning making sure they are in line with the seat of the chair then slowly lower them into the chair. - Slowly lower the patient into the chair. ● To stand up: - Assist the client in pushing themselves up using the strength of their arms and grasp the walker's handgrips. - Inform the client not to pull on or tilt the walker to help them stand up. 56