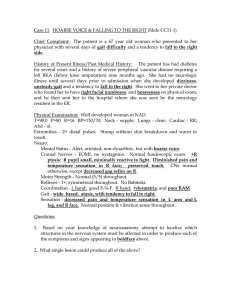
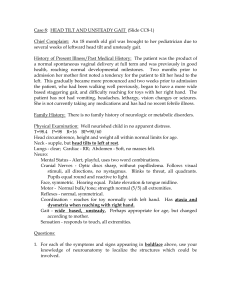
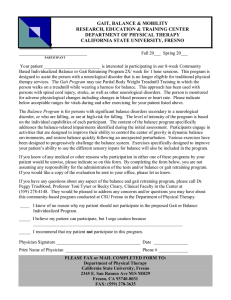
Gait Kwabena Kan–Dapaah, Ph.D. Department of Biomedical Engineering School of Engineering Sciences College of Basic and Applied Sciences University of Ghana November 21, 2023 Outline 1 Introduction 2 Normal Gait Terminologies Gait Cycle Data Energy Consumption 6th Determinants: Foot and Knee Mechanics 3 Pathological Gait Specific Gait Abnormalities Common Pathologies 4 Clinical Examination of Gait Introduction Normal Gait Pathological Gait Clinical Examination of Gait Details At the end of this lecture, you should to be to: define terminologies related to gait describe the gait data describe energy consumption of gait describe muscle activity during gait differentiate normal and pathological gait References: Introduction to Biomechanics: From Cells to Organisms, C.R. Ethier and C. A. Simmons - Chapter 10.1 − 10.2 Saunders et al., ”The major determinants in normal and pathological gait”, J. Bone Joint Surg Am, 1953, 35, 543-58 Lecture notes: KIN 201, 2007-1, Clinical Biomechanics of Gait, Stephen Robinovitch, Ph.D. Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Definitions Normal Walk or Run A method of locomotion involving the use of two legs, alternately, to provide both support and propulsion Walk: at least one leg in contact with ground at all times Normal depends on: gender, ages, body geometry Gait “The manner or style of walking”, rather than the walking process itself Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption History I Descriptive Studies Leonardo da Vinci, Galileo and Newton Borelli (1682) - De Motu Animalum measured CoG of body walking balance maintained by constant forward movement Weber Brothers Gait cycle - 1836 Timing of gait and pendulum-like swing of leg Kinematics Marey (1873) Multiple exposure on black suit with illuminated stripes on limbs pressure beneath foot Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption History II Eadweard Muybridge (1978) 24-camera triggered in suscession to capture horse movement extended study to naked human beings walking, running, etc Braune and Fischer (1895) - Der Gang des Menschen Marey’s technique but with fluorescent strip-lights 3D trajectories, velocities and accelerations of the body segments Bernstein, Moscow (1930s) Developed several photographic techniques for kinematic measurements studied 150 subjects Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption History III Force platforms Amar (1924) - described early design Elftman (1938) - improved Amar’s design Muscle activity Scherb, Switzerland, (1940s) muscle palpating during treadmill walk and EMG Verne Inman et al. - UC at San Francisco and Berkeley published Human Walking (Inman et al., 1981) Mechanical analysis Bresler & Frankel (1950) free-body calculations for the hip, knee and ankle joints Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption History IV their analytical techniques formed basis of many current methods of modeling and analysis Saunders et al. (1953) and Cavagna & Margaria (1966) Energy consumption and transfer between segments Patricia Murray (1967) research concentrated on variability of walking, development of gait in children and the deterioration of gait in old age Mathematical modeling - Joint forces Paul (1965) first detailed analysis of hip joint forces (1965) and knee (1966) during walking Clinical application - The Ultimate Goal Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption History V translation from lab to clinic began since 1960 in the beginning issues related to quality data now it s how to use it beneficially Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Gait Cycle Gait cycle - defined as the time interval between 2 successive occurrences of one of the repetitive events of walking Cycle time - duration of complete cycle stance time swing time Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Spatiotemporal Data - Terminologies Gait Cycle Data Energy Consumption Timing of Signle/Double Support Leading and trailing leg Stance: 60% and Swing: 40% Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Spatiotemporal Data - Foot Placement on Ground Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Spatiotemporal Data - Cadence, Cycle Time, Speed Cadence The number of steps per unit time, usually given in steps per minute cycle time (s) = 120/cadence(steps/min) speed (m/s) = stride length (m) × cadence(steps/min) 120 speed (m/s) = stride length (m)/cycle time (s) Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics (1) (2) (3) Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Kinematic Data - SP Hip Angle Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Kinematic Data - SP Knee Angle Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Kinematic Data - SP Ankle Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Kinematic Data - FP Pelvic Obliquity Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Kinematic Data - TP Pelvic Rotation Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Kinetic Data - Force & CoP Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Electromyography Data - Muscle activity Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Energy Consumption The energy used by a person who is walking can be divided into 3 parts: 1 2 Muscles - accelerate and decelerate the trunk and limb segments Overheads cardiac muscles respiratory muscles - the diaphragm, the rib cage and the abdominal ‘basal metabolism’ Two forms of optimization transfers of energy minimize displacement Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Energy Transfer Two types of energy transfer occur during walking: between potential and kinetic energy up/down movements of trunk twisting of the shoulder girdle and pelvis in opposite directions between one limb segment and another Movement HAT (Head, Arms and Trunk) transfered to thigh and shank Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Centre of Gravity (CoG) An abstraction concept that simplifies locomotion All forces considered to be acting at the centre of gravity (CoG) Thus, displacement of CoG considered end result of forces and motions concerned with locomotion Under static conditions, CoG of the body has been determined by Cadaver double suspensions Living subjects balanced beam and volume contours In adult fe-/males: mid-line: about 55% from ground of the total stature1 vertebral column: anterior to 2nd sacral vertebrae 1 Crosskey et al., 1922 Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Displacement Rhythmic up-/downward displacement of CoG framework for examining pathologies High point: 25 and 75 % of cycle, (mid-stance), Low point: 50 % both feets on group Functional significance: lower displacement of CoG; reduce energy expenditure Inman et al., 1981 Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Background A straight line locomotion has least expenditure of energy possible with say wheels impossible by means of bipedal gait Most economical alternative: low amplitude sinusoidal pathway with gradual deflection Newton’s second law: F = m · v · t abrupt changes compel high energy expenditure CoG translation through a smooth undulating pathway of low amplitude conserves energy body strives to achieve this it is important to analyze the factor that determines this pathway Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption Compass Gait A bipedal system consisting of lower extremities with no foot Figure 1: L: Pathway series of high amplitude arcs and R: Pelvic rotation flattens arc. Source: JBdM Saunders et al.,J. Bone Joint Surg. Am. 1953, 25:543-58 Quasi-locomotion, only flexion and extension involved Compass: CoG rise = 10 cm, ∆P.E.∼ 70 J, Normal: CoG rise = 4 − 5 cm, ∆P.E.∼ 35 J Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption 4&5th D: Human trajectory in the sagittal plane Factors that: raise the low point of the trajectory 1 pelvic rotation lower the apex of the trajectory: 2 pelvic tilt 3 knee flexion during mid-stance decrease the slope of the rise: 4 plantarflexion after heel strike decrease the slope of the dip: 5 plantarflexion after heel-off Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Terminologies Gait Cycle Data Energy Consumption 6th Determinant: Lateral displacement of pelvis Description: During stance, the pelvis shifts laterally towards the stance limb CoG closer to the stance leg, making it easier for the stance-side hip abductors to raise the swing leg and control pelvic tilt Result: horizontal (transverse plane) oscillation of the CoG with an amplitude of ∼ 5 cm, and frequency one-half that of vertical (sagittal plane) movement (∼ 1 Hz vs. 2 Hz) Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Backgorund Normal gait occurs if locomotor system accomplishes 4 things 1 Each leg in turn must be able to support the body weight without collapsing 2 Balance must be maintained, either statically or dynamically, during single leg stance 3 The swinging leg must be able to advance to a position where it can take over the supporting role 4 Sufficient power must be provided to make the necessary limb movements and to advance the trunk. Abnormal gait may result from a disorder in brain, spinal cord, nerves, muscles, joints & skeleton presence of pain Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Trendelenburg Gait Conditions for normal (middle) 1 absence of significant pain on loading 2 adequate power in the hip abductors 3 sufficiently long lever arm for the hip abductors 4 solid & stable fulcrum in or around the hip joint. Conditions for Trendelenburg gait painful hip, hip abductors weakness, abnormal hip joint, wide walking base, unequal leg length Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Trendelenburg Gait Assumptions the weight of the trunk is 452 N (46 kg) the weight of the right leg is 147 N (15 kg) Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Trendelenburg Gait Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Trunk Bending Figure 2: in normal walking, the line of force early in the stance phase passes behind the knee; anterior trunk bending brings the line of force in front of the knee, to compensate for weak knee extensors. Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Trunk Bending Figure 3: in normal walking, the line of force early in the stance phase passes in front of the hip; posterior trunk bending brings the line of force behind the hip, to compensate for weak hip extensors. Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Trunk Bending Figure 4: when there is a fixed flexion deformity of the hip (left), the whole pelvis must rotate forwards for the femur to move into a vertical position (right), with a resulting increase in lumbar lordosis. Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Ab. Gait Patterns: Functional Leg Discrepancy Figure 5: The swinging leg moves in an arc, rather than straight forwards, to increase the ground clearance for the swing foot. Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Specific Gait Abnormalities Common Pathologies Neurological Conditions Cerebral palsy Parkinsonism Spina bifida Stroke Figure 6: Sagittal plane kinematic data for the left side of a 9-year-old patient with cerebral palsy spastic diplegia Kwabena Kan–Dapaah, Ph.D. Figure 7: Cerebral Palsy BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Homework During normal gait, what variation occurs in the position of the CoG in the coronal plane? During normal gait, what variation occurs in potential energy of the body? How is this affected by the determinants of gait? What factors lower the apex of the COG during gait? What factors raise the low point of the COG during gait? What factors reduce the slope of the rising and falling portions of the CoG trajectory during gait? Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics Introduction Normal Gait Pathological Gait Clinical Examination of Gait Thank You! Kwabena Kan–Dapaah, Ph.D. BMEN 307: Biomechanics