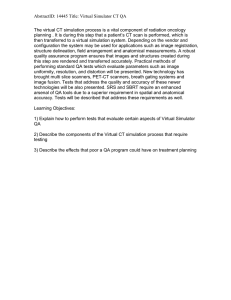
Medical Engineering & Physics 29 (2007) 367–374 Hardware-in-the-loop-simulation of the cardiovascular system, with assist device testing application B.M. Hanson a,∗ , M.C. Levesley a , K. Watterson b , P.G. Walker a a School of Mechanical Engineering, University of Leeds, Leeds LS2 9JT, UK b Yorkshire Heart Centre, Leeds General Infirmary, Leeds, UK Received 29 November 2005; received in revised form 13 March 2006; accepted 9 May 2006 Abstract This paper presents a technique for evaluating the performance of biomedical devices by combining physical (mechanical) testing with a numerical, computerised model of a biological system. This technique is developed for evaluation of a cardiac assist device prior to in vivo trials. This device will wrap around a failing heart and provide physical beating assistance (dynamic cardiac compression). In vitro, the device to be tested is placed around a simulator comprising a mechanical simulation of the beating ventricles. This hardware model interfaces with a computerised (software) model of the cardiovascular system. In real time the software model calculates the effect of the assistance on the cardiovascular system and controls the beating motion of the hardware heart simulator appropriately. The software model of the cardiovascular system can represent ventricles in various stages of heart failure, and/or hardened or congested blood vessels as required. The software displays physiological traces showing the cardiac output, depending on the natural function of the modelled heart together with the physical assist power provided. This system was used to evaluate the effectiveness of control techniques applied to the assist device. Experimental results are presented showing the efficacy of prototype assist on healthy and weakened hearts, and the effect of asynchronous assist. © 2006 IPEM. Published by Elsevier Ltd. All rights reserved. Keywords: Hardware-in-the-loop (HIL); Cardiac assist device; Modelling; Simulation; Cardiovascular system; LVAD 1. Introduction Cardiac assist devices are currently being developed with the aim of providing physical pumping assistance to a weakened or failing heart. Implantable impeller pump-based left ventricular assist devices (LVADs) are emerging. Alternatively, dynamic cardiac compression (DCC) can assist by providing compression to the surface of the ventricle(s) [1]—thereby avoiding some problems of immune-system rejection and thromboses [2]. In the early development of LVADs, numerical simulations of circulatory systems have been valuable tools when used to simulate the effect of assist devices on the cardiovascular ∗ Correspondence to: Department of Mechanical Engineering, University College London, Torrington Place, London WC1E 7JE, UK. Tel.: +44 7879 415 504. E-mail address: ben@benhanson.com (B.M. Hanson). system (CVS) [3,4]. These models have a long history of use and some are highly detailed (e.g. [5]). However, when working prototypes have been constructed purely numerical techniques become less attractive; it can be inconvenient and inaccurate to create numerical models of prototype devices, whose physical behaviour may not be fully understood yet. Physical testing is therefore required. The actual hydraulic performance of prototype LVAD systems has been tested on electro-hydraulic servo-systems [6–8]. Investigators have used simple models of the circulatory system to present a realistic hydraulic load to the LVAD, however these testing models have not shown how the mechanical performance of an LVAD directly affects the complete circulatory system. With a DCC assist device, the interaction between the assist device and the surface of the heart is crucial. This interaction is likely to depend on physical features which are particularly difficult to model, such as non-linear friction and backlash. Physical testing of DCC devices requires 1350-4533/$ – see front matter © 2006 IPEM. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.medengphy.2006.05.010 368 B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 a physical heart (or model) on which to apply compression, and a means of measuring the compressive effort applied. In vitro studies on dead hearts are unfortunately not feasible due to non-function of papillary muscles, collapse of the ventricular outflow tracts and increased myocardial stiffness (unpublished results). However, excised hearts have been sustained for in vitro tests using a blood supply from a “support” animal [1,9,10]. In these studies, a hydraulic servo pump was used to present a realistic outflow impedance using a windkessel model, as with the LVAD tests. Again, the effects on the closed-loop circulatory system were not studied. These animal studies have produced invaluable results, however they are costly in terms of time, resources and animal lives. 2. Hardware-in-the-loop concept This paper describes the use of hardware-in-the-loop (HIL) simulation to test a DCC assist device in vitro. This HIL simulation combines a realistic numerical model of the heart and cardiovascular system with a controllable physical heart simulator, and this interacts in real time with a prototype DCC assist device. The nature of these interactions is shown in Fig. 1. Hardware-in-the-loop-simulation has been developing in industrial control for testing of systems comprising some physical and some simulated components [11–13]. Simulation is used to represent processes that are physically unavailable, or whose use would be too costly, dangerous, or time-consuming. Proven benefits of HIL include: • Reproducibility of experiments. • The ability to perform tests which would otherwise be impossible, impractical or unsafe: ◦ testing a component under extreme or dangerous operating or environmental conditions (e.g. extremes of temperature, pressure, acceleration); ◦ testing effects of sensor and/or actuator faults; ◦ long-term durability testing—until failure. In this investigation, the cardiovascular system is the simulated component, and the benefits described above apply equally to the biomedical field. Using HIL simulation for biological systems could provide: • The possibility to test on a wide range of simulated patient geometries and pathologies. • Repeated testing on a consistent model. • Facilitated numerical quantification of performance by recording simulated physiological parameters. • Replacement of human and/or animal subjects: ◦ sterile, clinical environment is not required; ◦ ethical issues are removed; ◦ cost and development time are reduced. 3. Hardware-in-the-loop simulation Fig. 1 shows the overall structure of the HIL simulation for the assist device application. The system involves a position control loop (indicated) whereby the diameter of the heart simulator is controlled by computer, such that it is a real-time physical “display” of the diameter of the simulated heart. The assist device contracts around this simulator and a sensor records the assist force at the physical interface between assist device and simulator. The HIL aspect is that this physical force signal forms part of the control loop: the force signal is fed into the CVS model, which calculates its effect on pressure within the heart and therefore blood Fig. 1. Structure of the hardware-in-the-loop-simulation of the cardiovascular system. B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 flow into and out of the heart, therefore the diameter of the simulated heart. Thus, the motion of the hardware simulator depends on the effect that hardware interaction with the assist device has on the software CVS model. From the point of view of the assist band, the heart’s physical motion and response to assistance appear realistic, as governed by the software CVS model. The components of the HIL cardiovascular simulation will now be described, with reference to Fig. 1. 3.1. Numerical model of cardiovascular system The human cardiovascular system has been modelled many times at various levels of complexity (for a review see, e.g. [14], and the state-of-the-art [15,16]). This particular model is based on some elements of previously-reported models, selected as appropriate to the requirements of the DCC assist device application. The structure of the model is shown in Fig. 2; it is an important feature that the model is haemodynamically closed-loop in order to assess the effects of applying assistance. The function of the software model is described in detail in [17], however an overview of the model is provided here. In a HIL simulation, the interface between hardware and software is crucial—in this case that is the heart. The model is therefore biased with more detail being used to describe the heart than the rest of the circulatory system. The four heart chambers are modelled separately, allowing assessment of the effect of disease or incompetence in any or all of the chambers. Two further passive, compliant compartments represent the aorta and pulmonary artery. The equation relating flow and pressure in each compartment is of the form: Px = Zx φx + Px additional (1) Fig. 2. Representation of the circulatory system model using an electrical equivalent, indicating six compartments in which blood can be stored (vertical branches). 369 where Padditional is applied to the heart chambers only and represents the sum of pressures generated by passive stretching of the pericardium, natural systolic function, and assist pressure, where appropriate. For the atria we apply a pressure–time curve; this is not dependent on atrial volume. For the ventricles we use a function, f(t), to generate a time-varying myocardial wall stress; the instantaneous active systolic pressure within the ventricles is then calculated from the wall stress and ventricle dimensions. This stress, σ, depends on the volume, V, to give a representation of the Frank–Starling relationship, and is also rate-dependent [5]: dV σ(t) = σmax f (t)KV (V (t) − V0 ) 1 − DV (2) dt Since research has concentrated on modelling the primary mechanical effects of assistance, the model does not include hormonal effects, vasomotor control, orthostatic stress or breathing, although these could of course be added at a later stage. The model has been implemented using LabVIEWTM to produce not only the software/hardware interface but also the numerical circulatory model itself, in LabVIEWTM ’s visual programming language. The use of a graphical programming environment makes it easy to incorporate physiological data into the model, and to manipulate it into a suitable form. Non-linear circulatory elements and functions are shown graphically and can therefore be consulted, verified, and manipulated more easily than tabulated data. As an example Fig. 3 shows the shape of a typical activation function for myocardial stress generation. This is scaled in the X and Y directions and used in the heart chamber models to create the function f(t) which is a stress, Y, acting over a time, X. The graphical code is compiled efficiently to take advantage of the hardware computation processes available on a Fig. 3. A normalised activation function curve: used to generate myocardial pressures within the CVS model. 370 B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 typical modern processor, thus in practice may be computed as fast as code written in, e.g. C. 3.2. Heart simulator An interface is required to communicate between the physical (hardware) assist device and the software cardiovascular model. The requirements of the physical simulator of the heart for this assist device application are: • it must be possible to wrap a contractile band-type heart assist device around the simulator, and • sense the assist pressure produced, • the device must represent the motion of one “slice” through the ventricles—the volume of the heart encircled by one assist belt, • the device must be able to simulate normal and pathological heart motion at rates of up to 150 bpm. In use, when combined with the software model and controller, the device is required to “beat” in a real-time display of the changing volume of the ventricles. The combined system must respond to assistance compression in a physically realistic manner. This interface takes the form of a heart simulator, as illustrated in Fig. 4. The simulator was constructed using electromagnetic swing-arm actuators that can be controlled by computer easily and accurately. These are arranged in a circular array as shown in Fig. 4—the swing arms are shown, but the actuation method is omitted for clarity. On the end of each of the six arms is mounted a vertical post; these form a hexagon around which to wrap the assist device. With the configuration used, external diameters from 24 to 96 mm (vertex to vertex) can be simulated. Though independently actuated, the six actuators are currently all linked with coupling rods, giving the sim- ulator just one degree of freedom: the diameter. Therefore, it is just the gross change in ventricle volume that is represented; this is sufficient since the assist band to be tested also has just one degree of freedom (circumferential contraction). 3.3. Assist device The prototype DCC assist device being tested consists of several contractile belts which are to be placed around both ventricles of the heart to form a contractile blanket. One band was tested in isolation on the heart simulator as indicated in Fig. 4. The circumference of these flexible belts is controlled using direct-drive, miniature dc motors. Compared to pneumatic actuation used in other DCC devices, the torque and position of these motors are easily controlled by computer, and are suitable for use with an implantable battery power supply. Long-term device life is being determined by endurance trials. If necessary, brushless commutation could be used to increase motor life; brushless motors are currently in use within implanted LVADs. Further details of the form and control of the device can be found in [18]. 3.4. Interfacing between hardware and software The key factor in an HIL simulation is the interfacing; this must be designed to suit both the hardware and software systems. A custom-made force sensor was used to record the force produced by the assist device. This comprises a thin aluminium cantilever beam structure (dimensions: 5.5 mm × 12 mm) with strain gauges on both beam surfaces. The force signal from this sensor is read into the software via analogue-to-digital conversion using an interfacing card (National Instruments PCI-MIO-16E). The increase in ventricular pressure created by this force was calculated using a simple model, Eq. (3), and added to the ventricular pressures within the software model. Passist = Fig. 4. Plan view diagram of the heart simulator, constructed from six swingarm actuators. Key: , 6× pivot points of swing-arm actuators; posts, around which is wrapped; sensor; , flexible belt of assist device; , monitor unit of assist device. , 6× , force T rh (3) where T is the circumferential tension in the assist belt (= force recorded, with the current geometry), r the external radius of the ventricles, and h is the effective width of the assist band. The same assist pressure was added to both ventricles. A servo-potentiometer is used to measure the position of one swing-arm actuator, and from this, the diameter of the heart simulator is calculated. This is the feedback used to control the instantaneous diameter of the simulator. The model is paced using an ex-planted pacemaker interfaced to the computerised model. This allows synchronous in vitro/in vivo comparison to be performed in future, where B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 Fig. 5. Position tracking performance of the heart simulator at 50, 100, and 150 beats per minute (bpm). a pacemaker would relay real physiological pacing signals to the computer model. For the data presented herein, the pacemaker was set to a constant rate and the model could equally have been paced numerically. 3.5. Position control loop The physical simulator’s task is to display the exact timevarying dimensions of the modelled “slice” through the heart, as shown in Fig. 4. The instantaneous position of the simulator is controlled in a feedback loop operating concurrently with the circulatory system model—data is passed along each arrow in Fig. 1 at a loop rate of 500 Hz. This rate provides a high resolution of the CVS simulation that allows detailed identification of the effects that assistance might have. A fast rate is also desirable to reduce the delay associated with digital filters that are used to remove high-frequency electrical noise from analogue input signals. The upper limit on loop rate is in practice governed by the time required for analogue interfacing rather than model computation. A non-linear PID control algorithm is used for feedback position control of the hexagonal array of swing-arm actuators. This gives good positional accuracy in the presence of unpredictable disturbance forces from the assist device. The tracking performance of the heart simulator is shown in Fig. 5, where the simulator replicated the motion of a heart beating at 50, 100, and 150 bpm. The actual position of the simulator followed the desired position to within 0.5 mm diameter, and this was deemed sufficient accuracy for the application. 4. Experimental methods The HIL simulator allows quantification of the circulatory effects of real, physical assist. In this paper we present results that demonstrate the efficacy of the HIL testing environment, and its specific benefits. 371 The HIL simulator was used to evaluate the performance of a prototype assist band, demonstrating the direct effect of its assistance on a model of a weakened cardiovascular system. A study of assist synchronisation was performed to attempt to determine the effect of assistance that is poorly synchronised with the heart’s own efforts: when used in vivo, the device will use the heart’s natural pacing signal, if available, sensed from a pacemaker. This will be exhibit beat-to-beat timing variations, and without careful control it is possible that an assist device may lose synchronisation with the natural heart. To assess this effect, a delay of up to 200 ms was imposed between the pacing signal at the start of natural systole and the onset of assist compression. The assist band was mounted to the heart simulator, as shown in Fig. 4. A weakened heart model was used, as described below. With the model operating in a steady haemodynamic state, the assist device was switched on, applying compression every beat. The CVS reached a new steady operating state after approximately 8–10 beats. Simulated physiological traces were recorded from the model over this period; the pressure within ventricles and main arteries was studied in each case, along with the ventricle volumes and cardiac output. The energy efficiency of the assist device was measured: instantaneous electrical power in to the assist device was calculated as the product of voltage and current, and mechanical power applied to the simulated ventricle was measured by multiplying the applied belt tension by the rate of change of circumference. The energy efficiency of the assist device was measured in each delayed case as the ratio of total mechanical energy (out) to electrical energy (in). This was averaged over a period of three cardiac cycles, once the CVS had reached a steady state. To simulate acute ischaemic heart disease, the contractility of both left and right ventricles was scaled down to 50% of their nominal healthy values [4]. Although autonomous nervous system (ANS) control of peripheral resistance is not included in this current model, the model’s values of vascular resistances were increased manually to maintain blood pressure in the weakened condition (values in Appendix A). Other parameters, including heart rate, were unchanged; use of a software model ensures that the experimental conditions are identical for each repeated test—something that would be impossible on a biological model. 5. Results Fig. 6 shows some traces from the numerical CVS simulation while undergoing testing. The assistance in this example was synchronised with the natural systolic effort. The closed-loop CVS model has shown that when one compression band is applied around both ventricles, assistance affects the systemic (left heart) and pulmonary (right heart) circulation in different ways. These effects are dis- 372 B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 Fig. 6. Simulated physiological traces from HIL simulation. Healthy CVS shown, and weakened CVS with effect of direct compression from a prototype assist device: LV, left ventricle; RV, right ventricle; PA, pulmonary artery. cussed in more detail in [17]. The model suggests that the assistance acts to empty the right ventricle, and the increased pulmonary pressure would then tend to increase the operating volume of the left ventricle. These effects would be reduced in vivo by the body’s ANS applying compensatory mechanisms. Therefore, this model is valuable in showing the direct, mechanical effects, as this allows the development of a control scheme to maintain both ventricle volumes without relying on ANS control. Assistance is seen to immediately increase the modelled blood pressure within ventricles and major arteries. Again, in vivo, ANS control would act to reduce vascular resistance to decrease the aortic blood pressure and increase the cardiac output. This model only shows the direct, mechanical effects of compression, which is sufficient for evaluating prototype assist devices. The increase in cardiac output (C.O.) as a result of assistance is shown in Table 1. The C.O. of the simulated weakened state is dramatically reduced in comparison to the healthy state, however the C.O. was then increased with assistance. The beneficial increase in C.O. is highest for synchronous assist, however a delay of up to 50 ms in assist action did not indicate a significant effect on performance. Fig. 7 shows a comparison between synchronous and asynchronous assist. In Fig. 7(a), assist is applied at beginning of systole, and a positive assist force is recorded over the period of ventricle contraction. In Fig. 7(b), the assist is delayed (by 150 ms), and a force is only recorded over part of the contraction period. The assist force continues into the isovolumetric relaxation period, which is extended as a result—diastole only begins once the assist pressure has been removed. Fig. 7(b) also shows a significant peak in force during the isovolumetric period, which could be clinically important—the increased contact force in diastole could restrict blood flow over the surface of the myocardium and increase the risk of further ischaemia. The efficiency of the device in converting electrical power into mechanical power is indicated by the relative magnitudes Table 1 Effects of prototype assist device with delayed onset on HIL simulation of the CVS Condition Assist Healthy Weak Weak Weak Weak Weak Weak None None Assisted Assisted Assisted Assisted Assisted Delay (ms) L.V. (E.D.V.) C.O. (l/min) Assist efficiency (%) 0 50 100 150 200 140 142 158 158 154 152 144 5.02 2.45 3.08 3.08 3.01 2.87 2.59 9.0 9.0 6.7 4.0 1.5 B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 373 Fig. 7. Force and power traces recorded from heart simulator, shown with ventricle diameter: (a) synchronous assist and (b) asynchronous assist. of the electrical and mechanical traces in Fig. 7. With no delay, the efficiency recorded was approximately 9%. This is below the theoretical maximum efficiency of dc electric motors (up to 70%), however that occurs at much higher rotational speeds than used in this application. Friction in the belt and the motor’s pulley system will have reduced the potential efficiency of the device. The electrical power used by the device does not change very significantly between Fig. 7(a and b), however the useful mechanical power out from the device is reduced if the assistance is applied to ventricles that have finished contracting. Table 1 shows how the efficiency reduces with increasingly asynchronous assist. Further investigation of the conversion of mechanical assist power into fluid power is recommended, taking into account the work done by the myocardium (in simulation). Preliminary investigations, as yet unpublished, have indicated that when assisted through systolic contraction, the myocardium generates a lower active component of stress. It is hoped that this could promote remodelling of the muscle. 6. Discussion and conclusions The results of HIL testing have demonstrated that applying mechanical assistance in the form of direct cardiac compression can increase blood pressure and cardiac output from a weakened heart. The experimental testing described in Sections 4 and 5 has demonstrated several of the benefits of HIL simulation identified in Section 2: compared to testing on an animal model, it would not have been possible to perform these repeated experiments, all on an identical patient model, in a short space of time, in a non-clinical setting. The HIL environment also facilitated numerical evaluation of the experiments and assessment of the device’s efficiency. Compared with a purely numerical simulation, HIL simulation enabled evaluation of the effect of the real, physical performance of the prototype assist device. This included the electromechanical properties of the motor and the mechanics of tension transmission via the flexible band to the heart surface. The efficacy of the prototype assist device was assessed as the dimensions of the ventricles changed over the cardiac cycle. The numerical CVS model used in HIL simulation can be further developed as required by future investigations. The short computational time required for the current model did not suggest that future models will have to be greatly simplified, especially given the increasingly available computing power. Ferrari et al. [4] found that LabVIEW running under Microsoft Windows provided limited time for computation, and suggested LabVIEW Real Time. For this apparatus we are also investigating LabVIEW Real Time, installed on a conventional PC. The assist device bands each have one degree of freedom – to contract circumferentially – however, this form of assist has been shown to produce differing effects on the two ventricles. Future work will consider ventricle-specific assist. The simulator can be enhanced by removing the mechanical links between the swing-arms, and providing separate position controllers for each of the six actuators. Then the different compliances of the right and left ventricles can be represented, as can regional wall motion abnormalities. Given the proven benefits of this technique, it is likely that this hardware-in-the-loop technique will be suitable for evaluation of prostheses and interaction with other biological systems. In such applications, it is the interface between hardware and software that will require the most attention. In this instance that interface took the form of a heart simulator; taking the example of an LVAD, the interface would necessarily involve fluid and may take the form of a precision servo-controlled displacement pump, with pressure transducers to measure the instantaneous pressure rise over the LVAD. This pressure would be fed into a circulation model similar to that of Fig. 2, with the addition of a branch through the LVAD. That flow would then be presented physically to the LVAD via the servo-controlled displacement pump. Arterial 374 B.M. Hanson et al. / Medical Engineering & Physics 29 (2007) 367–374 grafts, stents, and valves could be evaluated in a very similar manner, and the HIL technique may also be applied to musculoskeletal prostheses using software models of muscle function. Appendix A Some cardiovascular system (CVS) parameters used: Parameter Healthy condition Ischaemic heart disease Peripheral venous resistance (mmHg/ml/s) Pulmonary resistance (mmHg/ml/s) LV contractility scaling (dimensionless) RV contractility scaling (dimensionless) Heart rate (bpm) 1.0 0.07 28 4 70 2.4 0.15 14 2 70 References [1] Oz MC, Artrip JH, Burkhoff D. Direct cardiac compression devices. J Heart Lung Transplant 2002;21(10):1049–55. [2] Macnair R, Underwood MJ, Angelini GD. Biomaterials and cardiovascular devices. Proc Inst Mech Eng 1998;212(Part II):465–71. [3] Wu Y, Allaire P, Tao G, Wood H, Olsen D, Tribble C. An advanced physiological controller design for a left ventricular assist device to prevent left ventricular collapse. Artif Organs 2003;27:926–30. [4] Ferrari G, Kozarski M, De Lazzari C, Gorczynska K, Mimmo R, Guaragno M, et al. Modelling of cardiovascular system: development of a hybrid (numerical-physical) model. Int J Artif Organs 2003;26(12):1104–14. [5] Urbaszek A, Schaldach M. A numerical heart and circulation model to simulate hemodynamics for rate-responsive pacing. In: Power H, editor. Bio-fluid mechanics. Southampton/Boston: Computational Mechanics Publications; 1995. p. 129–60. [6] Pillon M, Duffour H, Jufer M. In vitro experiments: circulatory assist device interaction with a virtual cardiovascular system. In: Proceedings of Annual International Conference IEEE-EMBS, vol. 14. 1992. p. 740–1. [7] Wu Y, Allaire P, Tao G, Liu Y. In-vitro test of an adaptive flow controller for a continuous flow LVAD. In: Proceedings of American control conference. 2004. p. 1647–8. [8] Kozarski M, Ferrari G, Clemente F, Gorczynska K, De Lazzari C, Darowski M, et al. A hybrid mock circulatory system: development and testing of an electro-hydraulic impedance simulator. Int J Artif Organs 2003;26(1):53–63. [9] Kawaguchi O, Goto Y, Ohgoshi Y, Yaku H, Murase M, Suga H. Dynamic cardiac compression improves contractile efficiency of the heart. J Thorac Cardiovasc Surg 1997;113(5):923–31. [10] Sunagawa K, Burkhoff D, Lim KO, Sagawa K. Impedance loading servo pump system for excised canine ventricle. Am J Physiol 1982;243(2):H346–50. [11] Isermann R, Schaffnit J, Sinsel S. Hardware-in-the-loop simulation for the design and testing of engine-control systems. Control Eng Pract 1999;7:643–53. [12] Ferreira JA, Gomes Almeida F, Quintas MR, Estima de Oliveira JP. Hybrid models for hardware-in-the-loop simulation of hydraulic systems. Proc Instn Mech Engrs Part 1: J Syst Control Eng 2004;218:465–74. [13] Hanselmann H. Hardware-in-the-loop simulation testing and its integration into a CACSD toolset. In: IEEE international symposium of computer-aided control system design. 1996. [14] Melchior FM, Srinivasan RS, Charles JB. Mathematical modelling of human cardiovascular system for simulation of orthostatic response. Am J Physiol (Heart Circ Physiol) 1992;262(31):1920– 33. [15] Ha R, Qian J, Wang D, Zwischenberger JB, Bidani A, Clark JW. A closed-loop model of the ovine cardiovascular system. In: Proceedings of 26th annual international conference of the IEEE EMBS. 2004. p. 3781–4. [16] Olansen JB, Clark JW, Khoury D, Ghorbel F, Bidani A. A closed-loop model of the canine cardiovascular system that includes ventricular interaction. Comput Biomed Res 2000;33:260– 95. [17] Hanson BM, Levesley MC, Watterson K, Walker PG. Simulation of the human cardiovascular system for real-time interaction with an assist device. In: Proceedings of 27th annual international conference of the IEEE EMBS, (EMBC ’05). 2005. [18] Hanson BM, Richardson RC, Davies GLJ, Watterson K, Levesley MC, Walker PG. Control of a non-blood contacting cardiac assist device. In: Proceedings of IASTED international conference on biomedical engineering BioMED2005. 2005. p. 679–84.