Microfluidics-Based Diagnostic Technologies for Low-Resource Settings Christian E. Fabian Martinez Contents 1 2 3 Introduction .......................................................................................................................................... 2 1.1 Significance of diagnostics in low-resource settings..................................................................... 2 1.2 Role of microfluidic technologies.................................................................................................. 3 Integration challenges........................................................................................................................... 4 2.1 Identifying the gaps ...................................................................................................................... 5 2.2 Bridging research and real-world application ............................................................................... 6 Technology outlook............................................................................................................................... 6 3.1 Improving design flexibility ........................................................................................................... 7 3.2 Technology adoption .................................................................................................................... 8 4 Conclusion ............................................................................................................................................. 8 5 References ............................................................................................................................................ 8 6 Annotations......................................................................................................................................... 10 1 1 Introduction Microfluidics is the mechanical analog to microelectronics and is a subject of study that similarly has potential to empower technological advances in various fields, including analytical chemistry, biotechnology, and diagnostics. Advancement in these fields has a worldwide reach that can affect millions of individuals by helping overcome the accessibility hurdle that currently exists in low-resource settings for diagnostic testing. Specifically, the implementation of microfluidics in point-of-care (POC) diagnostic devices aims to circumvent issues related to centralized diagnostic labs in developing countries (and other resource-poor regions) by providing accurate and repeatable diagnostic tools that require less equipment, less trained personnel, are more portable, and generate faster responses. 1.1 Significance of diagnostics in low-resource settings Centralized-lab diagnostic testing thrives when it is supported by infrastructure that can accommodate sample transportation, sample storage, large high-throughput equipment, and has access to trained personnel – this is a good option for developed countries that meet the infrastructure requirements. However, developing countries and low-resource settings oftentimes lack even basic infrastructure, such as reliable power or trained technicians and healthcare professionals, and therefore centralized-lab diagnostic testing falls short in providing access to people living in those areas. 3 Decentralized diagnostic solutions, such as POC diagnostic devices, can aid in eliminating geographic and socioeconomic barriers that block certain people from accessing their closest centralized diagnostics lab; in fact, these types of barriers currently prevent the necessary healthcare service access to 69% of HIVinfected people in resource-limited settings like Sub-Saharan Africa.7 In the context of HIV infections, a major concern is the transmission of the virus to infants during childbirth. A critical parameter in reducing mortality in HIV-positive infants is the time to antiretroviral therapy (ART) initiation from the time the blood sample was taken. Guidelines from the World Health Organization (WHO) recommend that HIV diagnostic results be delivered to the infant’s caregiver no more than 28 days after sample collection; similarly, the WHO recommends ART initiation within seven days of diagnosis for HIV-positive children under 5 years of age. A study from the sub-Saharan African region found that that the median lead time for receipt of HIV diagnosis for infants was 35 days, and the median lead time for ART initiation was 39 days – both of these metrics exceeded the threshold established by the WHO.14 Diagnosis is only the first step, and subsequent steps for the treatment of HIV requires monitoring of CD4+ T cell counts to evaluate the effectiveness of ART treatment up to 3-4 times a year. 5 Monitoring for HIV disease presents yet another key challenge for resource-limited settings, where ART optimal performance is dependent on adherence to monitoring schedules; in particular, monitoring of this disease helps identify treatment failure and therefore early therapeutic switches to another ART regimen can lead to declines in mortality.15 In 2017, it was reported that there were over 219 million cases of malaria across 90 countries, with more than 435,000 related deaths. Despite the attempts to thwart malaria infections using netting, insecticides, and mass prophylactic drug administration, progress has stalled in part due to unreliable diagnostic techniques. In low-resource settings the standard diagnostic method is light microscopy; however, this method requires a trained technician, and it fails to identify the disease in asymptomatic 2 patients who have low parasite loads. Other diagnostics tools, such as malaria immunoassays know as rapid diagnostic tests have shown poor sensitivity performance between 70-75% in real-world scenarios – the WHO has recommended that the target sensitivity for diagnostic tests be a minimum of 97%. The significance of sensitive diagnostics tools is highlighted in the fact that successful malaria disease elimination programs depend on identifying populations where the disease maintains low levels and can therefore continue spreading due to not being treated.13 1.2 Role of microfluidic technologies Decentralized testing from POC devices has been shown to significantly decrease the time required for patients to receive an HIV diagnosis. The same study on HIV diagnosis for infants in the sub-Saharan Africa region discussed earlier found that within 6 months of implementing POC diagnostic tools, the median turnaround time for HIV diagnosis dropped from 35 days to 0 days, and ART initiation dropped from 39 days to 1 day.14 This study demonstrated the importance of POC devices in low-resource settings and provided objective justification for recommending the implementation of POC devices in routine government-supported public sector healthcare facilities. With this type of evidence, it’s clear why the microfluidics community has focused research efforts on health and biomedical applications, particularly applications in POC diagnostics, which represent around a third of the microfluidics overall market. 9 Microfluidic systems have found synergy with POC applications due to their compactness, low reagent consumption, rapid result turn-around time, low environmental impact, requirement for small sample volumes, and on-chip storage of required reagents.9 Another benefit of microfluidic systems is the high surface to volume ratio, which is advantageous in many bioassays where reactions take place at surfaces and therefore there is an inherent sample efficiency that follows. 10 Other aims for microfluidic POC applications includes the concept of parallelization, sometimes referred to as multiplexing, of various tests within a single run – the method usually involves a single sample which is run through various parallel channels, each with the required chemical process steps to evaluate multiple analytes. Multiplexing is of importance when an infectious disease, such as malaria, can be caused by a variety of strains and each needs to be treated differently. Figure 1 below show a paper-based microfluidic device that enables a multiplexed test for two strains of malaria. Figure 1. Paper-based microfluidic device for a multiplexed DNA test for Plasmodium and P. falciparum (Source: Reboud et al., 2019). 3 High portability has been a major target for microfluidics since its inception and is one of the major drivers in the design of microfluidic systems for low-resource settings. These devices are commonly referred to as miniaturized total analysis systems (μTAS) or lab-on-a-chip (LoC) technologies. The miniaturization of electronics, particularly electrical sensors, have also paved way for making lab-on-achip concepts a potential reality of the not-so-distant future. An example of the miniaturization of assays and detectors can be seen in the microfluidic CD4+ T cell counter developed by Watkins et al. (2013) – the motivation for development of the T cell counter was to make this type of diagnostic test more accessible to those individuals in resource-limited regions and where incidences of HIV infection are more prevalent. A small measurement circuit was developed using impedance microcytometry principles that could achieve single-cell accuracy performance and easily rivaled the current gold standard process for cell counts, flow cytometry.10 Figure 2 shows the sensing region within the microfluidic chip, which contains the miniaturized circuit and a microchannel that is 15 µm tall x 15 µm wide – the sense volume was a mere 300 fL. Though an entire device was not developed using this T cell counter microfluidics chip, it establishes the groundwork for future developments of a POC device that integrates this technology in a hand-held form factor. Figure 2. Micrograph of the counting channel in within the sensing region of the microfluidic device developed by Watkins et al. The scale bar in the bottom right corner is 200 micrometers. (Source: Watkins et al., 2013) 2 Integration challenges While a multitude of microfluidic technologies have been described in academic papers, only a few examples of these microfluidic devices have successfully been translated into real-world applications and commercialized products. There are a large number of articles regarding microfluidic technologies with unique biological applications, including diagnostics and many lab-on-a-chip concepts, yet widespread industry integration remains a challenge.6 Adoption of microfluidics in mainstream biomedical research and biotech industry can aid in realizing many of the academic microfluidic diagnostic concepts designed specifically for low-resource settings. The integration problem that broadly affects microfluidics is partially responsible for stifling efforts on the diagnostic applications front. Ultimately, the end-users of microfluidic diagnostics in resource-poor regions cannot advocate for addressing these integration challenges so it’s up to research teams working on these diagnostic solutions to consider gaps in their work. 4 2.1 Identifying the gaps For industry to adopt microfluidic technologies, there would need to be significant operational advantage or cost reductions. Academic microfluidic research sometimes does not account for how their technology could integrate into the existing biotech infrastructure without major disruptions. Lab-on-achip platforms are sometimes developed with complex array of tubing and syringe pumps that are illsuited for scaling and cannot be used by personnel with no knowledge of microfluidics. It’s been noted that some if these microfluidic devices need expert technicians (in many cases their inventors) to set-up, and to non-stop monitor and troubleshoot running systems.10 In a similar fashion, better adoption of microfluidic technologies involves demonstrating significant improvement compared to current gold standards. Many microfluidic methods exist that simply improve or provide marginally better performance compared to macroscale standards, and in some cases might not offer fundamentally new capabilities.2 Relevant clinical application of microfluidic technologies necessitates collaboration between engineers and biomedical researchers – the reason for this is that oftentimes engineers over-extend their knowledge of biological systems to the point where they draw false conclusions about biological functions and therefore lack clinical significance. An expert bioengineer, for instance, might not take those microfluidic publications seriously and therefore an opportunity for further development may be lost. Evidence of poor communication between engineers and external fields related to diagnostics can be seen by looking at the number of publications featuring microfluidics in engineering journals compared to those in biology and medicine journals. Figure 3 below shows large difference in number of microfluidics-related publications in engineering journals compared to those in multidisciplinary journals. Figure 3. Graph showing disproportionate number of microfluidics publications in engineering journals compared to multidisciplinary journals and biology/medicine journals (Source: Sackmann et al., 2014). A criticism of microfluidic systems is lack of integration considerations and what the biotechnology community call ‘chip-in-a-lab’. This wordplay on the ‘lab-on-a-chip’ concept in microfluidics is used as a way of relaying disappointment that most microfluidic systems are not designed to integrate well into a biotechnology workflow, and that they are essentially a stand-alone process that necessitates its own individual task and analysis. This frustration stems from microfluidic systems sometimes requiring specialized equipment that is not widely available in a biotechnology lab, for instance. 5 2.2 Bridging research and real-world application Bridging the gaps in microfluidic technology from research to real-world application is a step towards development of microfluidic POC devices that solve real issues, specifically those in resourcelimited settings. An important gap to close, specifically for POC diagnostic applications, is one that minimizes the use of external equipment. Limiting the use of equipment makes microfluidic diagnostic systems more accessible to resource-poor regions where maintaining low cost and portability for tests is paramount. Paper-microfluidics (a type of μTAS device) is a powerful tool that is already under development that aims to meets those low-cost and portability goals, while maintaining comparable performance to diagnostic gold standard tests. In fact, the malaria diagnostic paper device discussed in the introduction is estimated to cost approximately $0.50 per assay to manufacture yet achieves 98% sensitivity to Plasmodium pan infection (exceeding the WHO guideline for sensitivity).13 The biotechnology community demands a ‘chip-in-a-box’ concept from microfluidics systems, which means that microfluidic chips should come in a plug-and-play system so that there is no ambiguity on how the microfluidic should be set-up to perform efficiently.10 This ‘box’ would have all the necessary equipment already on-board, as well as software for simple analysis and interpretation of data. This idea of complete systems can be extended to microfluidic POC diagnostics, where it is definitely expected to have as much of the critical processing performed within the microfluidic chip. Having external equipment and manual chemical processing only opens up the possibility for user error, which in turn would lead to a system with poor reproducibility and sensitivity. Lastly, collaboration between academic engineers and industry research scientists is a method to better develop technologies that can be easily integrated and scaled-up. Industry research scientists usually have better visibility into end-user needs and therefore this information can be shared with academic engineers during collaboration sessions. An industry research scientist might also be able to provide information regarding throughput, price, and manufacturing time targets that will give microfluidic technologies the best chance of being adopted. This is particularly important for microfluidic POC applications since the development of a fully integrated POC device is likely going to be launched by industry leaders in diagnostics, such as Abbot Laboratories or Becton Dickenson (BD). 3 Technology outlook Microfluidics has the potential to improve POC diagnostics and can even widen its scope if the shortcomings discussed in the previous section are addressed. Many of the authors of microfluidics research papers encouraged other teams to take their technology and modify certain steps to fit their application. In the context of diagnostics, an already-developed microfluidic chip could be modified to identify a different analyte or count another cell type, for instance. With this in mind, the following sections discuss how microfluidics can grow as a discipline that serves diagnostics and its wide range of needs. 6 3.1 Improving design flexibility One of the current issues with microfluidic systems is having poor design flexibility – most are designed with a very specific application and operating parameters in mind and would likely require a major re-design to be used in other, relevant applications. A way that this problem can be addressed is by making use of modular unit operation chips that have a single purpose and can be assembled into a full system in a LEGO-like fashion. Building blocks, such as a fluid handling, mixing, dilution, sample concentration, filtration, sorting, samples amplification, and detection, can be developed and subsequently be fully characterized. The characterization of unit operation chips can even be extended to include mathematical models and software tools for simulation – this type of characterization can enable researchers and other user to quickly put a semi-custom microfluidic platform to serve a unique application. Figure 4 shows a concept for a modular-based microfluidic device and how a hydraulic schematic might be developed to analyze flow resistances. Figure 4. Concept for a modular microfluidics system that is comprised of various building blocks. The schematic on the left shows how these systems could be specified to calculate hydraulic resistances for all building blocks. (Source: Fernandes et al., 2018) Another aspect of microfluidics that is expected to develop is the standardization of features to improve connectivity. These connectors would minimize dead volume and would be fully specified so that multiple microfluidic chips can be connected. This type of standardization would improve the way researchers collaborate when developing microfluidic solutions for new applications. Connectivity would not only be limited to connecting microchannels; in fact, this concept could be expanded to connectivity of electrical connections.9 The standardization of connections would also allow better integration with other non-microfluidic systems, and therefore further improve the odds of technology adoption. 7 3.2 Technology adoption Recent microfluidics publications are increasingly co-authored by engineers, biologist, and clinicians. 2 This type of multidisciplinary collaboration is conducive to successful implementation of microfluidic technology in diagnostics. Similarly, some of the microfluidic articles reviewed performed end-user evaluations and field testing, which proved the robustness of the diagnostic tools that the authors developed – this is particularly important in low-resource setting applications because field testing might reveal shortcomings related to unforeseen environmental conditions, user errors, or workflow issues. In essence, collaboration between the microfluidic community and other medical and biotechnology disciplines is expected to grow in an effort to further advance the field and bring microfluidics one step closer to widespread adoption. 4 Conclusion Microfluidics-based technologies have the potential to offer diagnostic testing accessibility to people that live in resource-limited settings. The importance of POC testing in resource-poor regions was discussed, as well as how microfluidics fits within the paradigm of POC testing. Benefits that are inherent with microfluidic diagnostic systems compared to current macroscale systems were analyzed, in addition to considering the hurdles that microfluidics must still overcome to see the widespread adoption. Lastly, a microfluidics technology outlook was presented to prepare the reader on what to potentially expect next in this growing field. 5 References [1] Nguyen, N.-T., Wereley, S. T., & Mousavi, S. S. A. (2019). Fundamentals and Applications of Microfluidics (3rd Ed.). Artech House. [2] Sackmann, E. K., Fulton, A. L., & Beebe, D. J. (2014). The present and future role of microfluidics in biomedical research. Nature, 507(7491), 181–189. https://doi.org/10.1038/nature13118 [3] Martinez, A. W., Phillips, S. T., Whitesides, G. M., & Carrilho, E. (2009). Diagnostics for the developing world: Microfluidic paper-based analytical devices. Analytical Chemistry, 82(1), 3–10. https://doi.org/10.1021/ac9013989 [4] Chin, Laksanasopin, T., Cheung, Y. K., Steinmiller, D., Linder, V., Parsa, H., Wang, J., Moore, H., Rouse, R., Umviligihozo, G., Karita, E., Mwambarangwe, L., Braunstein, S. L., van de Wijgert, J., Sahabo, R., Justman, J. E., El-Sa, W., & Sia, S. K. (2011). Microfluidics-based diagnostics of infectious diseases in the developing world. Nature Medicine, 17(8), 1015–1019. https://doi.org/10.1038/nm.2408 8 [5] Moon, Keles, H. O., Ozcan, A., Khademhosseini, A., Hæggstrom, E., Kuritzkes, D., & Demirci, U. (2009). Integrating microfluidics and lensless imaging for point-of-care testing. Biosensors & Bioelectronics, 24(11), 3208–3214. https://doi.org/10.1016/j.bios.2009.03.037 [6] Caicedo, & Brady, S. T. (2015). Microfluidics: The Challenge Is to Bridge the Gap Instead of Looking for a “Killer App.” Trends in Biotechnology (Regular Ed.), 34(1), 1–3. https://doi.org/10.1016/j.tibtech.2015.10.003 [7] Watkins, N. N., Hassan, U., Damhorst, G., Ni, H. K., Vaid, A., Rodriguez, W., & Bashir, R. (2013). Microfluidic CD4+ and CD8+ T lymphocyte counters for point-of-care HIV diagnostics using whole blood. Science Translational Medicine, 5(214). https://doi.org/10.1126/scitranslmed.3006870 [8] Fu, Liang, T., Spicar-Mihalic, P., Houghtaling, J., Ramachandran, S., & Yager, P. (2012). TwoDimensional Paper Network Format That Enables Simple Multistep Assays for Use in LowResource Settings in the Context of Malaria Antigen Detection. Analytical Chemistry (Washington), 84(10), 4574–4579. https://doi.org/10.1021/ac300689s [9] Fernandes, Gernaey, K. V., & Krühne, U. (2018). Connecting worlds – a view on microfluidics for a wider application. Biotechnology Advances, 36(4), 1341–1366. https://doi.org/10.1016/j.biotechadv.2018.05.001 [10] Ortseifen, Viefhues, M., Wobbe, L., & Grünberger, A. (2020). Microfluidics for Biotechnology: Bridging Gaps to Foster Microfluidic Applications. Frontiers in Bioengineering and Biotechnology, 8, 589074–589074. https://doi.org/10.3389/fbioe.2020.589074 [11] Ahmed, Bui, M.-P. N., & Abbas, A. (2016). Paper-based chemical and biological sensors: Engineering aspects. Biosensors & Bioelectronics, 77, 249–263. https://doi.org/10.1016/j.bios.2015.09.038 [12] Xia, Si, J., & Li, Z. (2016). Fabrication techniques for microfluidic paper-based analytical devices and their applications for biological testing: A review. Biosensors & Bioelectronics, 77, 774–789. https://doi.org/10.1016/j.bios.2015.10.032 [13] Reboud, Xu, G., Garrett, A., Adriko, M., Yang, Z., Tukahebwa, E. M., Rowell, C., & Cooper, J. M. (2019). Paper-based microfluidics for DNA diagnostics of malaria in low resource underserved rural communities. Proceedings of the National Academy of Sciences - PNAS, 116(11), 4834– 4842. https://doi.org/10.1073/pnas.1812296116 [14] Boeke, C. E., Joseph, J., Wang, M., Abate, Z. M., Atem, C., Coulibaly, K. D., Kebede, A., Kiernan, B., Kingwara, L., Mangwendeza, P., Maparo, T., Mbaye, R. N., Mukungunugwa, S., Ngugi, C., Nzuobontane, D., Okomo Assoumou, M. C., Reta, Y., Wambugu, B., Rioja, M. R., Peter, T., Doi, N., Vojnov, L., Khan, S. and Sacks, J. A. Point-of-care testing can achieve same-day diagnosis for 9 infants and rapid ART initiation: results from government programmes across six African countries. J Int AIDS Soc. 2021; 24(3):e25677 [15] Bélec, & Bonn, J.-P. (2011). Challenges in implementing HIV laboratory monitoring in resourceconstrained settings: how to do more with less. Future Microbiology, 6(11), 1251–1260. https://doi.org/10.2217/fmb.11.121 6 Annotations [1] Nguyen, N.-T., Wereley, S. T., & Mousavi, S. S. A. (2019). Fundamentals and Applications of Microfluidics (3rd Ed.). Artech House. This textbook hopes to introduce the reader to the fundamentals of microfluidics, as well as to showcase the various applications of the technology, such as providing design rules for microvalves, micropumps and microflow sensors. I used this resource as an entry into the field of microfluidics and to better understand the possible applications that may deserve further study. Additionally, I felt the need to understand the fundamentals of microfluidics, which may be lightly touched on (or even excluded) from many scholarly articles in an effort to put more focus on the study at-hand. For this annotation I put more focus on the impact of the authors and therefore I reviewed the number of times the Mousavi, Wereley, and Nguyen were cited (4623, 21098, and 31120, respectively). The citations number gave me confidence in the influence of the authors and the content of the textbook. [2] Sackmann, E. K., Fulton, A. L., & Beebe, D. J. (2014). The present and future role of microfluidics in biomedical research. Nature, 507(7491), 181–189. https://doi.org/10.1038/nature13118 This was a citation from the textbook reference above and was selected based on my interest of biomedical applications of microfluidics. This paper provides a concise review of microfluidic technology in the biomedical field. First, the article argues that the technology is still looking for a ‘killer application’ in the biomedical field and goes on to analyze the discrepancy between the number of articles written about microfluidics and its use in the biomedical field – most were written for technical/engineering journals and not biology or medical journals. Additionally, the adoption of the technology has been limited due competing macroscale techniques advancing to the point where microfluidic techniques are only marginally better than traditional methods. Lastly, the paper urges researchers to find the ‘right problems to solve’ and to choose those where macroscale processes are at a major disadvantage compared to microfluidic methods, such as the portable, scalable, low-cost design of microfluidic paper diagnostic devices. This article is reputable due its publication on the Nature journal, which is a high-impact journal (69.5 in 2021). 10 [3] Martinez, A. W., Phillips, S. T., Whitesides, G. M., & Carrilho, E. (2009). Diagnostics for the developing world: Microfluidic paper-based analytical devices. Analytical Chemistry, 82(1), 3–10. https://doi.org/10.1021/ac9013989 Martinez et al. presented microfluidic paper-based analytical devices (µPADs) as a potential diagnostic solution for the developing world. The authors argue that other diagnostic technologies require expensive tests, established infrastructure, and trained personnel; µPADs on the other hand are inexpensive, easy to transport, easy to manufacture, have low environmental impact, and can be analyzed using basic equipment (e.g., cell phone camera or a home desktop scanner). Various methods of fabrication and analysis are presented, as well as results from an application in urinalysis (specifically the creation of calibration plots for glucose and BSA protein). Lastly, the article discusses other potential uses for paper-based microfluidics including paper microzone plates, use in the military, home healthcare, and agriculture. The Analytical Chemistry journal is a reputable source because it was published by a well-known institution, American Chemical Society, and this journal had 170,464 citations in 2021. I paid particular attention to one of the authors, namely George M. Whitesides, because he has a large amount of citations (380,659 all-time) and has a large h-index (282). [4] Chin, Laksanasopin, T., Cheung, Y. K., Steinmiller, D., Linder, V., Parsa, H., Wang, J., Moore, H., Rouse, R., Umviligihozo, G., Karita, E., Mwambarangwe, L., Braunstein, S. L., van de Wijgert, J., Sahabo, R., Justman, J. E., El-Sa, W., & Sia, S. K. (2011). Microfluidics-based diagnostics of infectious diseases in the developing world. Nature Medicine, 17(8), 1015–1019. https://doi.org/10.1038/nm.2408 Chin et al. showcased a microfluidic point-of-care (POC) device, called mChip, that was able to rival the performance of current lab-based ELISA immunoassays (the gold standard) in detecting HIV and syphilis; more importantly, the mChip achieved those comparable results while being easily deployable in remote locations, requiring simple detection equipment, completes within 20 minutes, and only needs a few microliters of blood sample. The authors focused on developing a device that is easy to manufacture, and thus results in a low-cost device – the cassettes are injection molded in polystyrene and cyclic olefin copolymer. Another innovation that the authors developed is the reagent delivery, which can introduce multiple reagents and washings sequentially (14 in total) in a single syringe; this method avoids the need to have bulky pipetting robots that are typically used in the lab-based ELISA. Lastly, a signal amplification method, using reduction of silver ions onto gold nanoparticles, was used to avoid the need for expensive detection equipment (e.g., microscopes, bulky sensitive detectors); instead, a lowcomplexity, low-cost device that uses LED’s and photodetectors was sufficient. This source is reputable given its publication in Nature Medicine journal (impact factor of 87.24 in 2021) [5] Moon, Keles, H. O., Ozcan, A., Khademhosseini, A., Hæggstrom, E., Kuritzkes, D., & Demirci, U. (2009). Integrating microfluidics and lensless imaging for point-of-care testing. Biosensors & Bioelectronics, 24(11), 3208–3214. https://doi.org/10.1016/j.bios.2009.03.037 11 The article focuses on the HIV public health challenge that resource-limited settings face. CD4+ T-lymphocyte and viral load counts are used to monitor the progress and treatment of HIV disease. Proven CD4+ T-lymphocyte isolating methods, CCD image sensor, microfluidics, and cell counting software are integrated to develop a system that could be used in the developed and developing world. A microfluidic chip, made of plastic and glass, is surface treated to separate CD4+ T-lymphocyte from whole blood, then is followed by a wash step to remove unbounded red blood cells and CD4+ monocytes. Subsequently, the chip is placed on the CCD image sensor and cell counts are performed with software within seconds. The test method was compared to flow cytometry and manual fluorescent imaging count to evaluate the specificity and efficiency of the proposed microfluidic solution. Compared to FACSCount (Becton Dickinson, CA, USA), which encompasses $27,000 equipment cost, $5-20 reagent cost, limited throughput 30-50 samples/day), the microfluidic technology met the need of a low-cost, low-resource, sufficiently accurate solution. While the authors aimed for a low-complexity device, there are still several pieces of equipment needed for the systems, such as microfluidics pumps, moderately expensive CCD sensor, computer to run the cell counting software, and cleaning supplies. The Biosensors and Bioelectronics journal had an impact factor of 12.54 in 2021. [6] Caicedo, & Brady, S. T. (2015). Microfluidics: The Challenge Is to Bridge the Gap Instead of Looking for a “Killer App.” Trends in Biotechnology (Regular Ed.), 34(1), 1–3. https://doi.org/10.1016/j.tibtech.2015.10.003 While reading other articles in microfluidics I was left wondering about the commercial viability of the ideas presented in those articles. I stumbled across this article that settled my question as to why I have not read about widespread translation of microfluidic technologies to commercial applications. The authors of this article make 3 major conclusions as to why microfluidic technologies are not widely commercialized despite the myriad of useful biological applications (e.g., protein crystallization and lymphocyte counters for point-of-care diagnostics). The first is that for industry to adopt microfluidic technologies, there would need to be significant operational advantage/cost reductions, and academic microfluidic research does not account for how their technology could integrate into the existing biotech infrastructure without major disruptions. Lab-on-a-chip platforms are sometimes developed with complex array of tubing and syringe pumps that are ill-suited for scaling and to be used by personnel with no knowledge of microfluidics. Second, relevant clinical application of microfluidic technologies necessitates collaboration between engineers and biomedical researchers – the reason for this is that oftentimes engineers over-extend their knowledge of biological systems to the point where they draw false conclusions about biological functions and therefore lack clinical significance. An expert bioengineer (or even biotech companies) might not take those microfluidic publications seriously and therefore an opportunity for further development may be lost. Lastly, the authors encourage the collaboration between academic engineers and industry research scientists to better develop technologies that can be easily integrated and scaled-up. This journal, Trends in Biotechnology, had an impact factor of 21.942 in 2022. Hector Hugo Caicedo has been cited 364 times, while the co-author, Scott T. Brady, has been has 17,309 citations. 12 [7] Watkins, N. N., Hassan, U., Damhorst, G., Ni, H. K., Vaid, A., Rodriguez, W., & Bashir, R. (2013). Microfluidic CD4+ and CD8+ T lymphocyte counters for point-of-care HIV diagnostics using whole blood. Science Translational Medicine, 5(214). https://doi.org/10.1126/scitranslmed.3006870 This research group tackled a part of the global HIV epidemic issue with the specific motivation to take part in the solution to give HIV diagnostics access to people in resource-limited settings, such as Sub-Saharan Africa. Both diagnosis and treatment of HIV infection require the monitoring of CD4+ and CD8+ T lymphocyte levels. The ‘gold standard’ for CD4+ and CD8+ T cell counts is flow cytometry, which requires centralized lab facilities and trained personnel – both of which are not always found in low-resource settings. The authors propose a point-of-care (POC) device that houses a microfluidic lab-chip that utilizes electrical impedance measurements to achieve single-cell counting accuracy. The PDMS microfluidic chip is comprised of 4 regions that are connected via microfluidic channels, and each has a purpose in getting CD4+ or CD8+ T cell counts from 10 μL of undiluted, unprocessed human blood samples. The first two regions essentially help selectively dissolve red-blood cells so that they don’t interfere with the counts downstream. The third region is a capture chamber that contains immobilized CD4 or CD8 antibodies that capture the CD4+ or CD8+ T cells. The last region is the counter used dualfrequency electrical interrogation method, which is the major technological breakthrough in this paper. An interesting aspect is how the authors used COMSOL (a CFD software package) to optimize the shear stresses in the cell capture chamber to optimize the capture efficiency of both CD4+ and CD8+ T cell. Another important result was that the microfluidic chip achieved similar performance to the flow cytometry standards (both high accuracy and high repeatability) and better performance compared to the Alere Pima bench-top system (another CD4+ T cell counter that has been successful in resource-poor regions. This microfluidic chip is not the end solution, but rather a platform that needs further development and integration in a small POC device. The journal, Science Translational Medicine, had an impact factor of 19.32 in 2021. Nicholas Watkins has 1179 citations, Umer Hassan has 907 citations, and Gregory Damhorst has 788 citations to-date. These metrics give me confidence that the article is reputable and can be used for my research. [8] Fu, Liang, T., Spicar-Mihalic, P., Houghtaling, J., Ramachandran, S., & Yager, P. (2012). TwoDimensional Paper Network Format That Enables Simple Multistep Assays for Use in LowResource Settings in the Context of Malaria Antigen Detection. Analytical Chemistry (Washington), 84(10), 4574–4579. https://doi.org/10.1021/ac300689s This paper was a continuation in my research of paper microfluidic applications. The paper device, called two-dimensional paper networks (2DPNs), demonstrated in this article is a lateral flow assay that has the capability to perform multistep chemical processing. Lateral flow assay tests currently have applications in drug testing, pregnancy tests, and disease detection, however, many of those applications only perform a single chemical process. The authors 13 proved that a lateral flow test does not need to be limited to a single chemical processing step, and in fact, could be modified to perform a variety of bioassays. The motivation for trying to expand the use of lateral flow assays is that they already have applications in low-resource settings, so it is a tried-and-proven technology. The 2dPNs can be implemented in low-cost ‘cards’ that require minimal user steps, that already contain all reagents stored within the card in dried form, and that only need water to start the test. The authors characterized the fluid flow in the multi-inlet paper network and the performance in detecting recombinant malaria protein PfHRP2. The 2DPN system presented was able to have a comparable limit-of-detection (LOD) to an ELISA test (the standard lab test). This article proposes a modified version of current lateral flow assays but is clearly still in the early stages of development and does not have a particular application that has gained traction. The mock assay consisted of lab-prepared samples with known concentration only to prove that the 2DPN will deliver reagents sequentially and in proper timing to not affect the performance of the biochemistry assay. The article does not show performance of the 2DPN with whole blood samples, which inevitable will introduce many variables that are not accounted for with the mock assay where the recombinant malaria protein PfHRP2 was simply diluted in fetal bovine serum. The Analytical Chemistry journal is a reputable source because it was published by a well-known institution, American Chemical Society, and this journal had 170,464 citations in 2021. Elain Fu has 7148 citations, Paul Yager has 26641 citations, Sujatha Ramachandran has 1955 citations, and Jared Houghtaling has 1454 citations to-date. These metrics give me confidence that the article is reputable and can be used for my research. [9] Fernandes, Gernaey, K. V., & Krühne, U. (2018). Connecting worlds – a view on microfluidics for a wider application. Biotechnology Advances, 36(4), 1341–1366. https://doi.org/10.1016/j.biotechadv.2018.05.001 I chose to read this paper to explore some of the hurdles in microfluidic technologies that might not have been discussed in other papers that I’ve read thus far. In agreement with the article by Caicedo & Brady, this article discusses the reason why only a select few microfluidic applications have been successfully commercialized. This article also introduces several more reasons for the discrepancy between the number of academic applications of microfluidics and commercially successful microfluidic systems, namely repeatability issues, low application flexibility, short lifetime, restrictive intellectual property (IP) licensing agreements, lack of standardization of connections between microfluidic systems/modules, reliance on external systems (micropumps), and need for a holistic understanding of the entire microfluidic system. I found an interesting piece of information in this article, which is the following: “Health and biomedical applications have been in the focus of many research efforts in microfluidics, especially for applications in point-of- care (POC) diagnostics which represent around a third of the microfluidics overall market”. This indicates that the outlook for microfluidic technology POC diagnostic applications is bright and likely will become more prevalent so long as the issues that the authors mentioned are addressed. 14 The second half of this paper is really focused on a call to the microfluidics community to making systems that are modular, and therefore this technology would be flexible and could have a wider range of applications. Namely, the authors make the argument that making modular microfluidic systems would lead to better acceptance among non-microfluidics experts – this would require standardization for connectivity between microfluidic chips, and even establishing mathematical models for all ‘unit operation’ microfluidics chips so that the enddesigner of the microfluidic technology can put all these modular microfluidic blocks together for a semi-custom microfluidic solution. This journal that published this article, Biotechnology Advances, has an impact factor of 14.23 in 2020. This particular article has been cited 29 times. The work of Fernandes, Gernaey, and Krühne have been cited 165, 10771, and 834 times, respectively. Given this information, it’s fair to assume that this source is reputable. [10] Ortseifen, Viefhues, M., Wobbe, L., & Grünberger, A. (2020). Microfluidics for Biotechnology: Bridging Gaps to Foster Microfluidic Applications. Frontiers in Bioengineering and Biotechnology, 8, 589074–589074. https://doi.org/10.3389/fbioe.2020.589074 This paper was chosen as another take on what can be done to make microfluidic technologies more accessible and relatable, specifically from the biotechnology standpoint. The authors begin the article by compiling all the benefits that microfluidics can bring to biotechnology, but then end the first quarter of the article by saying that most of the microfluidic systems meant for biotechnology can be better referred to as “chip-in-a-lab”. This wordplay on the ‘lab-on-a-chip’ concept in microfluidics, and it was said as a way of relaying the disappointment that most microfluidic systems are not designed to integrate well into a biotechnology workflow, and that they are essentially a stand-alone process that necessitates its own individual task and analysis. The authors call for ‘chip-in-a-box’ concept for designing microfluidics, which means that these microfluidic chips should come in a plug-and-play system so that there is no ambiguity on how the microfluidic should be set-up to perform efficiently. This box would have all the necessary equipment already on-board, as well as software for simple analysis. There are case studies presented that demonstrate the usefulness of microfluidics, and at the same time show the shortcomings. One example is that ultra-high throughput cell screening capacity, where droplet-based microfluidics show that the systems successfully meet the demand for high-throughput screening, but the scale in biotechnology (ultrahigh) is even larger and further technological advances need to be made to achieve that scale of throughput with microfluidic technology. The same problem of integration into work routine and need for plugand-play solution is highlighted. This journal that published this article, Biotechnology Advances, has an impact factor of 5.89 in 2021. The work of Ortseifen, Wobbe, and Grünberger have been cited 217, 1339, and 2925 times, respectively. Given this information, it’s fair to assume that this source is reputable 15 [11] Ahmed, Bui, M.-P. N., & Abbas, A. (2016). Paper-based chemical and biological sensors: Engineering aspects. Biosensors & Bioelectronics, 77, 249–263. https://doi.org/10.1016/j.bios.2015.09.038 This article begins with detailing the history and working physics of paper-based biosensors (which are considered microfluidic devices due to the small pores within the fibers of the paper). The authors explain that the flow in these types of devices is the Reynolds number less than 1 and therefore flows in this devices is laminar. The next section discusses all that fabrication methods for hydrophobic and hydrophilic regions of a microfluidic device, including wax printing and wax transfer methods. From this section in fabrication methods, it’s apparent that very basic equipment is required to manufacture these types of devices, and therefore this translates to low manufacturing costs – only some instances there is requirement for more expensive equipment, such as laser beam cutters and plasma treatment. An important note was mentioned that relates to citation #13, which is that origami style microfluidic devices have received negative feedback from the diagnostics industry due to reproducibility issues and manual fabrication procedure. The middle sections of the article talk about how paper can be modified to have better properties (e.g., immobilization of molecules for sample separation) that are conducive to achieving better diagnostic performance, namely by adsorbing materials, covalent modification of the cellulose paper to include functional groups, and entrapment of biomolecules within the paper structure. The authors also discuss transduction systems – the first two that are mentioned are the most common (i.e., colorimetric and electrochemical). Lastly, the authors have a really interesting section on challenges and outlook for these challenges that can be reference for the final section of my review (see Section 4 of the paper). The Biosensors and Bioelectronics journal had an impact factor of 12.54 in 2021. This particular article has been cited 178 times. Given this information, it’s reasonable to say that the source is reputable. [12] Xia, Si, J., & Li, Z. (2016). Fabrication techniques for microfluidic paper-based analytical devices and their applications for biological testing: A review. Biosensors & Bioelectronics, 77, 774–789. https://doi.org/10.1016/j.bios.2015.10.032 [13] Reboud, Xu, G., Garrett, A., Adriko, M., Yang, Z., Tukahebwa, E. M., Rowell, C., & Cooper, J. M. (2019). Paper-based microfluidics for DNA diagnostics of malaria in low resource underserved rural communities. Proceedings of the National Academy of Sciences - PNAS, 116(11), 4834– 4842. https://doi.org/10.1073/pnas.1812296116 This article presents a paper-based microfluidics solution for a malaria diagnostic tool that can be used in resource-limited regions. The article begins by presenting the case that there are over 219 million cases of malaria across 90 countries. Further, the current diagnostic tools are either non sensitive enough (rapid diagnostic tests) or fail to detect low levels of infection (light microscopy). In fact, the sensitivity measured for the RDT was 82% and 85% for light microscopy 16 compared to the proposed microfluidic solution with a sensitivity of 98%. The method proposed in this article still requires trained personnel to do two steps of fluid handling, however, the steps appear to be simple and can be done with minimal training. Some of the reagents used, particularly the enzymes that amplify the signal, are sensitive to environmental conditions and required refrigeration. Low-resource settings will often lack the infrastructure to support reagent storage that is at -20 °C and this is why the authors decided to test the performance of this particular reagent at room temperature. It was found that the enzyme to withstand room temperature condition for 3 days without significant decrease in performance. This is unfortunately an obstacle for the technology since that means that mass storage of this type of reagent is not possible in low-resource settings – instead this reagent would have to be delivered and used within that 3-day time window. Nevertheless, the results are promising given the high sensitivity for two of the most abundant strains of the malaria parasites. Another benefit is the low cost of the device due to being manufactured with thermoplastics, acetate film, printed wax, and paper – it was mentioned that the cost of the entire device with a single assay would be approximately $0.50. Additionally, this cost could be reduced even further if it was manufactured at scale. The journal, Proceedings of the National Academy of Sciences, had an impact factor of 12.779 in 2021. Also, this particular article was cited 135 times. Given this information, it’s reasonable to say that the source is reputable. [14] Boeke, C. E., Joseph, J., Wang, M., Abate, Z. M., Atem, C., Coulibaly, K. D., Kebede, A., Kiernan, B., Kingwara, L., Mangwendeza, P., Maparo, T., Mbaye, R. N., Mukungunugwa, S., Ngugi, C., Nzuobontane, D., Okomo Assoumou, M. C., Reta, Y., Wambugu, B., Rioja, M. R., Peter, T., Doi, N., Vojnov, L., Khan, S. and Sacks, J. A. Point-of-care testing can achieve same-day diagnosis for infants and rapid ART initiation: results from government programmes across six African countries. J Int AIDS Soc. 2021; 24(3):e25677 This article was picked for it’s content to support the idea of implementing point-of-care (POC) devices in low-resource settings. Specifically, this article discusses the needed for rapid diagnosis and antiretroviral therapy (ART) initiation for infants diagnosed with HIV. The authors start the article by reminding the reader of the World Health Organization (WHO) guidelines related to the desired timing for diagnosing (specifically receipt of diagnosis to the caregiver) and starting treatment of HIV infections in infants, namely 28 days after sample collection and ART initiation within 7 days of diagnosis. The goal of the articles is to investigate the lead times for diagnosis between POC devices and centralized labs in 6 countries (Cameroon, Democratic Republic of Congo (DRC), Ethiopia, Kenya, Senegal and Zimbabwe). The study took place across 52 public sector health facilities over a year period – 6 months of observation study using centralized labs, and another 6 months after implementing POC devices in the health facilities. For the implementation of the POC devices, the research team provided training on all aspects of the POC device (procedures + maintenance), quality control (documentation), and they also provided supportive supervision visits throughout the monitor period. 17 The results show that 4610 POC and 2892 centralized-based test were conducted throughout the study. While not discussed in the article, the higher number of POC test during the monitoring period may be suggestive that patients were more willing to undergo HIV testing due to the rapid results. The researchers observed a dramatic improvement in median turnaround time from sample collection for diagnosis receipt in the POC group over centralized testing (same day vs 35 days, respectively). Further, the median time from sample collection to ART initiation was 1 day for the POC group, compared to 39 days for centralized testing. This article is reputable, and the study can be trusted to make the conclusion that POC devices can drastically reduce the time from sample collection to HIV diagnosis for infants, which would help in lowering morbidity and mortality rates. The Journal of the International AIDS Society has an impact factor of 5.396 (2020) and the article has been cited 7 times according to the journal’s website. [15] Bélec, & Bonn, J.-P. (2011). Challenges in implementing HIV laboratory monitoring in resourceconstrained settings: how to do more with less. Future Microbiology, 6(11), 1251–1260. https://doi.org/10.2217/fmb.11.121 I chose to read this article to get a better understanding of the challenges that resource-limited settings face when it comes to centralized-lab models for diagnostic testing, specifically for HIV disease monitoring. This paper introduced me to the concept of virological failure, which means that ART treatment is not always effective and can in fact have therapeutic failure – worst is that this is prevalent is resource-poor regions, such as sub-Saharan Africa where the failure of treatment can be as high as 33%. This type of failure then requires that the ART treatment be stopped, and another type of regimen begin. These facts highlight the need to HIV monitoring, which cannot always be fulfilled by centralized-lab testing. The authors also mention that current rapid HIV antibody tests are not sensitive enough, and this can lead to up to 10.5% false-positive – this is an unnecessary economic burden for ART programs and inconvenience patients. Also, the article discusses CD4 T cell counts, which is a bridge to the paper by Watkins et al. (reference 7), and is agreement that this type of diagnostic test is critical for the monitoring the HIV in patients. It is also mentioned that the effort to decentralize CD4 T cell count testing has created platforms that require major maintenance, and therefore have not been successful. It’s therefore imperative that POC solutions are robust in the face of untrained users and poor infrastructure. The journal, Future Microbiology, had an impact factor of 3.553 in 2021. Also, this particular article was cited 28 times. The work of Laurent Bélec has been cited 11, 831 times and has 282 publications. Given this information, it’s reasonable to say that the source is reputable. 18
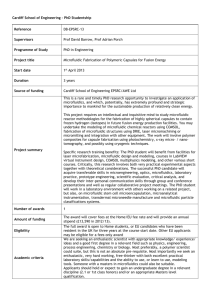
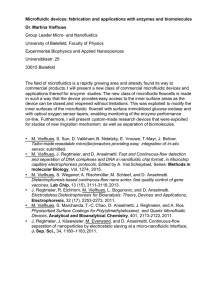
 0
0
advertisement


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users