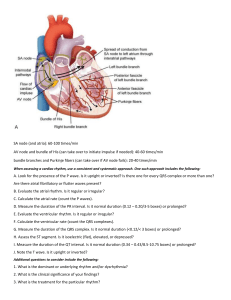
ECG NORMAL ECG WAVE FORMS BASIC INTERVALS ABNORMAL WAVEFORMS ST ELEVATION ST DEPRESSION • Myocardial ischaemia/ • Myocardial ischaemia/ • • • • infarction Acute pericarditis, myocarditis LVH/LBBB Brugada pattern (RBBB with ST elevation in right precordial leads ) Hyperkalemia • • • • • • infarction LVH (strain pattern ) LBBB,RBBB, WPW Drugs ( digitalis ) Hypokalemia Cardiomyopathies Normal variant TALL T WAVES T WAVE INVERSION • Hyperacute phase of AMI • Myocardial • Prinzmetal angina ischaemia/infarction • LVH/RVH • LBBB/RBBB,WPW • Hyperkalemia • CVA • LVH/LBBB • Acute pericarditis WIDE QRS • Normal variant • LBBB/RBBB, WPW, VPC’s • Hyperkalemia QT PROLONGATION • Electrolyte disturbances- hypokalemia, hypocalcemia, • • • • hypomagnesemia Drugs- classI and III antiarrhythmic agents, phenothiazines, TCA, antibiotics (erythromycin, pentamidine), terfinadine, cisapride Myocardial ischaemia/ infarction CVA Congenital – Romano-Ward syndrome, Jervell and Lange –Nielsen syndrome (AR with congenital deafness ) LOW VOLTAGE QRS • Defines as QRS <5 mm in all the limb leads and less than 10 mm in all the chest leads • CAUSES Normal variant Obesity Pleural/ pericardial effusion COPD, Constrictive pericarditis Cardiomyopathies CALCULATION OF RATE If rate is regular ➢ No of large boxes (0.2 sec ) between 2 successive QRS complexes (R-R interval ) and divide 300 by this number Or ➢ 1500 divided by the number of small boxes (0.04 sec ) If rate is irregular ➢ Count the number of QRS complexes in 6 second interval and multiply by 10 QRS AXIS • Direction of ventricular • • • • depolarisation Normal axis is down and to the left Normal axis varies from -30 ° to +110° Axis > -30 ° or more negative is LAD Axis >+110° 0r more positive is RAD CAUSES OF AXIS DEVIATION RAD • Spurious • Normal variant • Dextrocardia • Right ventricular overload ( acute- pulmonary embolism, severe asthma ; chronic- COPD, pulmonary stenosis, pulmonary hypertension ) • Lateral wall MI LAD • Normal variant • LVH • LBBB • Left anterior hemiblock • Ostium primum ASD, tricuspid atresia ATRIAL ENLARGEMENT • Normal P wave in every lead is ≤ 2.5mm (0.25 mV) in amplitude and less than 0.12 sec ( 3 small squares ) in width • P wave exceeding any of these dimensions in any lead is abnormal • Normal P wave is positive in lead II and negative in avR RIGHT ATRIAL ENLARGEMENT • Also known as P- pulmonale • Abnormally tall P wave ( height >2.5mm ) • No effect on the total duration of atrial depolarisation , so width remains normal • Best seen in leads II,III, aVf and V1 LEFT ATRIAL ENLARGEMENT • Also known as P-mitrale • Because left atrium depolarises after the right atrium LAE prolongs the total duration of atrial depolarisation so width increases • Classically, LAE produces a wide P wave ( > 0.12 sec ), amplitude may be normal or increased • Best seen in leads II and V1. • In V1 a biphasic p wave may be seen, with a small initial positive deflection followed by a wide negative deflection. The negative component is longer than 0.04 sec in CAUSES OF ATRIAL ENLARGEMENT RAE • Pulmonary disease- BA, pulmonary embolism, emphysema, bronchitis • Congenital heart diseasepulmonary stenosis, ASD, tetralogy of Fallot, Ebstein’s anomaly LAE • Valvular heart diseaseMS,MR,AS,AR • Hypertensive heart disease • CAD • Cardiomyopathies RIGHT VENTRICULAR HYPERTROPHY • R>S in V1 • Often associated with RAD and T wave inversion in right to mid precordial leads • Affects both depolarisation and repolarisation , so inverted T waves in rightmid precordial leads (RV strain ) • Causes- congenital heart disease (PS, TOF, ASD, eisenmenger’s syndrome), LEFT VENTRICULAR HYPERTROPHY • Voltage of S in V1 + R in V5 or V6 >35mm • R wave in aVl ( 11to 13 mm ) • ST depression with inverted T waves in leads with tall R waves ( LV strain ) • LAD or LAE, LV conduction delay (wide QRS ) may be seen ATRIAL FIBRILLATION • AF is one of the most common arryhthmias encountered in clinical practice • Classified into - paroxysmal (stops spontaneously within 7 days, usually within 48 hrs ), persistant (lasts for >7 days and usually requires cardioversion ) and permanent (lasts indefinitely or fails to terminate or recurs even after cardioversion ) • Causes- alcohol abuse ( holiday heart ), autonomic , congenital/coronary/hypertensive / valvular heart disease, cardiomyopathy, cardiothoracic surgery, idiopathic, thyrotoxicosis, pulmonary disease ECG IN AF • Irregular wavy baseline produced by rapid f waves • An irregular ventricular rate HEART BLOCK Degree AV conduction pattern First degree block Uniformly prolonged PR interval 2nd degree (intermittant conduction failure ) Mobitz type I: progressive PR prolongation 3rd degree block No AV conduction Mobitz type II: sudden conduction failure MOBITZ TYPE I vs MOBITZ TYPE II COMPLETE HEART BLOCK • P waves are present with a regular atrial rate faster than the ventricular rate • QRS complexes are present with a slow (usually fixed ) ventricular rate • The P waves have no relation with the QRS complexes and PR intervals are completely variable because the atria and the ventricles are completely disconnected MYOCARDIAL INFARCTION • Localisation of infarction • Anterior – leads V3, V4 ( septal V1-V2) Reciprocal changes- II, III, avf • Lateral wall- I, aVl, V5, V6 Reciprocal changes – III, aVf, V1 • Inferior wall- II, III, aVf Reciprocal changes- I, aVl • Posterior wall - V1-V3 (depression) reciprocal changes SEQUENCE OF CHANGES • The ST segment elevations and the reciprocal changes can be seen within minutes of the infarct . Tall positive T waves ( hyperacute ) are also seen at this time and may sometimes preceede the ST elevation . Sometimes new Q waves may also appear( acute phase) • After hours to days ST segments come back to baseline and at the same time T waves become inverted in the leads that showed ST elevation (evolving phase ) • Resolving plase- partial or complete regression of ST-T changes and sometimes of Q waves PATTERN OF ST ELEVATION AND DEPRESSION STEMI NSTEMI ECG IN SPECIAL SITUATIONS HYPERKALEMIA HYPOKALEMIA • Tall and peaked T waves • ST elevation • Prolongation of PR, QRS and • Appearance of U wave • ST depression QT • Loss of P waves • Sine-wave pattern and asystole CARDIAC DIGITALIS TOXICITY NON CARDIAC • Weakness • Anorexia • Nausea and vomiting • Altered colour perception • Mental status changes Bradycardia • Sinus bradycardia including sinoatrial block • Junctional (escape ) rhythm • AV block including mobitz type 1 and CHB Tachycardia • Accelerated / junctional rhythm like nonparoxysmal/junctional tachycardia • Atrial tachycardia with block • Ventricular ectopy including premature beats,