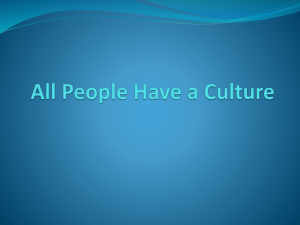
Nursing Continuing Professional Development Parent/Caregiver Perceptions of the Concept of Legacy in a Pediatric Hospital: A Qualitative Study Maile T. Jones, Jessika C. Boles, Jenna E. Dunbar, and Jessica Cook early 6 million overnight hospital stays are recorded for children each year in the United States (McDermott et al., 2017). Whether a child is admitted for a common pediatric ailment or a life-threatening and life-changing illness, pediatric hospitalization impacts entire family systems by challenging family relationships, coping mechanisms, roles, and responsibilities (Foster et al., 2016). Parents/caregivers have identified several significant stressors when their child is hospitalized, namely lack of information about the child’s condition or procedures, the unfamiliarity of the hospital environment, separation from home and family, and uncertainty about illness and treatment plans (Canga et al., 2020). If these stressors and parent/caregiver coping needs are left unaddressed, chronic health care-related stress can impair quality of life and lead to long-lasting post-traumatic stress symptoms or disorders for parents/ caregivers and their children (Price et al., 2016). Given the wealth of stressors parents/caregivers encounter during a child’s hospitalization, and the clearly documented direct relationship between parent and N Instructions for NCPD Contact Hours PNJ 2203 Nursing continuing professional development (NCPD) contact hours can be earned for completing the learning activity associated with this article. Instructions are available at pediatricnursing.net Deadline for submission: April 30, 2024 1.4 contact hour(s) Jones, M.T., Boles, J.C., Dunbar, J.E., & Cook, J. (2022). Parent/caregiver perceptions of the concept of legacy in a pediatric hospital: A qualitative study. Pediatric Nursing, 48(2), 59-67, 102. A child’s hospitalization affects the entire family system, with parents/caregivers reporting a myriad of stressors challenging family dynamics and coping efforts. Legacy-oriented interventions employ play- and arts-based techniques to promote collaboration and communication in families of hospitalized children and thereby foster resilience. Although offered in most children’s hospitals, little is known about the impact of these interventions on pediatric patients and families, or the ways pediatric health care providers, parent/caregivers, and pediatric patients understand and describe the concept of legacy. This study explored the legacy perceptions of parents/caregivers of hospitalized children on acute or critical care units in an academic medical center. Ninety-three parents/caregivers completed a semi-structured, in-depth interview regarding their perceptions of the concept of legacy. Analysis yielded four themes: 1) legacy is a transgenerational process; 2) legacies can be actions, accomplishments, and experiences; 3) legacy can be a powerful tool for education and change; and 4) a ‘good’ legacy can be left in different ways. These findings together indicate that capturing and integrating a family’s unique history, stories, strengths, and experiences appear to be a desirable and useful component of family-centered health care. Additionally, when considered along previous research and practice, it appears medical and psychosocial care providers should assess, recognize, and involve parent/caregivers’ experiences with and understandings of legacy into legacyoriented interventions or activities, as well as other aspects of care related to patient and family coping and functioning. Key Words: Pediatric, qualitative, caregivers, caretaking, health care. child coping and distress (Doupnik et al., 2017), supporting parents/ caregivers during a child’s hospitalization is a priority objective for high quality health care. Certified Child Life Specialists (CCLSs) and other health care professionals have recognized this need for parent/caregiver support during a child’s hospitalization, imple- menting a variety of family-centered interventions to promote coping and adjustment. Certified Child Life Specialists are health care professionals who capitalize on the power of play to provide education, promote coping, and reinstate a degree of normalcy for children and families in medical settings (Association of Child Life Professionals, 2020; Maile T. Jones, M.Ed, CCLS, CIMI, is a Certified Child Life Specilist, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville, TN. Jessika C. Boles, PhD, CCLS, is an Assistant Professor of Practice, Vanderbilt University, and a Certified Child Life Specialist, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville, TN. Jenna E. Dunbar, M.Ed, CCLS, CIMI, is a Certified Child Life Specilist, Johns Hopkins Children’s Center, Baltimore, MD. Jessica Cook, M.Ed, is a Doctoral Student, The University of Memphis, Memphis, TN. PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 59 Boles, Fraser et al., 2020). In addition to the psychological preparation, medical play, diagnosis education, and generalized family support they offer, CCLSs have also integrated legacy-oriented interventions as a family-centered coping support (Boles & Jones, 2021). Sometimes referred to as ‘legacy building,’ the more aptly named legacy-oriented interventions are arts- and play-based therapeutic interventions designed to help children and their families stay connected, express their thoughts and feelings, find meaning, and create lasting positive memories during difficult health care experiences (Sisk et al., 2012). Mediums, such as journaling, scrapbooking, photography, video diaries, keepsake collections, handprints, plaster hand-molds, letters, storytelling, and songwriting, are just a few of the legacy-oriented intervention techniques CCLSs use to help preserve and strengthen family bonds, promote open communication, and foster resilience (Boles, 2014; Foster et al., 2012; Ramirez et al., 2019; Sisk et al., 2012). However, amidst resource limitations, staffing constraints, and the presumptions upon which these practices are founded, legacyoriented interventions have been typically and unfortunately prioritized in those moments in which a child’s death is anticipated or imminent (Boles, Jones et al., 2020; Boles & Jones, 2021). Although 97% of children’s hospitals offer legacy-oriented interventions as standard of care for those patients and families approaching the end of life (Foster et al., 2012), little is known about the impacts of these activities on parent/caregiver distress or other measures of family functioning, coping, or adaptation. As the course of history and health care research patterns continues to demonstrate, illness and treatment concepts are often explored in adult populations and settings prior to their study and integration in pediatrics. At this juncture, legacy practices in adult health care have taken a variety of clinical forms, yet empirical evaluations of legacy-oriented interventions with seriously or terminally ill adults are limited (Martinez et al., 2017; Scarton et al., 60 2018). However, the handful of interventional studies completed to date has yielded promising results in terms of feasibility, acceptability (Akard et al., 2018), and appreciable improvements in emotional wellbeing and spiritual functioning (Piderman et al., 2015), life satisfaction (Allen et al., 2014), self-efficacy (Franklin & Cheung, 2017), and feeling prepared for the end of life (Keall et al., 2013). Further, many of these effects have held true for caregivers and family members, suggesting some family-centered utility of legacy-oriented interventions in adult health care. Whether within adult or pediatric frameworks, the study of legacy has been hindered by a lack of consistent terminology for describing the concept of legacy, and those interventions designed to target legacy needs and preferences. Signified with terms ranging from legacy-building (Sisk et al., 2012) to legacy-making (Foster et al., 2012), memory making (Riegel et al., 2019), life-review (Allen et al., 2008), Dignity Therapy (Chochinov et al., 2005), spiritual life review (Piderman et al., 2017), and even legacy artwork (Schaefer et al., 2019), the only clear consistency is that legacy as concept and intervention has been defined and operationalized in a variety of ways. In gerontology, legacy is described as “the process of passing one’s self through generations, creating continuity from the past through the present to the future” (Hunter, 2008; p. 328); however, Boles and Jones (2021) define legacy as “an enduring representation of the self—its qualities, experiences, effects, and relationships—built and bestowed across generations. Whether concrete or intangible, intentional, or serendipitous, legacies are an avenue of connection, education, inspiration, or transformation” (p. 19). Conversely, Naik and colleagues (2016) describe legacy as “being understood and remembered by one’s social network” (p. 629), whereas others have asserted that “legacy is both what we leave and how we live” (Andersen et al., 2018; p. 260), or “the values or meanings of one’s life passed from one to another” (Schellinger et al., 2018; p. 161). Thus, the existing spectrum of legacy definitions and practices further complicates the current lack of research dedicated to the specific features, forms, functions, and outcomes of legacy. Despite its interventional prevalence in pediatric health care settings, the concept of legacy itself has yet to be intentionally explored and described in pediatric health care. It follows, then, that to understand the potential impacts of legacy interventions, it is necessary to first understand the ways parents/caregivers perceive and describe the concept of legacy, which will improve intervention validity. Therefore, the purpose of this study was to explore the perceptions of the concept of legacy among parents/caregivers of hospitalized children at an academic medical center. Methods Study Design Moustakas’ (1994) psychological phenomenology, defined as a methodology grounded in social constructionism and focused on understanding the underlying essence of and perceptual differences concerning a shared phenomenon, was chosen for this study to capture participants’ understandings of, experiences with, and thoughts about the concept of legacy for three reasons. First, the lack of both conceptual and experimental research regarding legacy in pediatric health care has, as of yet, failed to produce topic-specific methodologies or measures that research teams can consider and select. Second, because the purpose of this study was to understand legacy perceptions of parents/caregivers of hospitalized children and the aim to construct an evidenceinformed definition of the concept of legacy, it was necessary to select an approach that would generate diverse perspectives around a unifying phenomenon. Finally, logistical difficulties and health risks of group data collection strategies led the research team to conclude that individual, in-person interviews would be the safest, most feasible, and least disruptive option for the PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 Figure 1. Parent/Caregiver Interview Questions intended participant population (Boles, 2018; Boles & Daniels, 2019). Setting This study was conducted at a children’s hospital associated with an academic medical center in the Southeastern United States. Accredited as a Level-I trauma center, the hospital serves patients and families from a three-state and 200-mile radius at its 209-bed main campus. This site was chosen not only for the diverse patient populations it serves, but also for its reputation as a high-quality care institution and international contributions to health care research. In addition, the research team was familiar with and able to access this site due to the principal investigator’s dual employment status with the medical center and the university with which it is affiliated. Approval for this study was granted by the research site (Protocol Number 171121), though the two entities share a common Institutional Review Board with designated subcommittees. Participants Participants in this study 1) were 18 years or older at the time consent was obtained, 2) spoke English as their primary language, and 3) were parents/caregivers of pediatric patients (less than 18 years of age) who were actively being diagnosed, treated, and managed on an inpatient floor at the research site. Parents/caregivers were defined as a biological parent or a primary caregiver (e.g., grandparent) to the pediatric patient. Parents/caregivers of children in state custody were not approached for participation in this study. Potential participants were recruited from both acute and critical care pediatric inpatient units, which included hematology/oncology, infant medicine, adolescent medicine, medical acute care, surgery and trauma, pediatric critical care, cardiac intensive care, cardiology stepdown, and neonatal intensive care. Those who met eligibility criteria were pre-identified each day by the principal investigator, and a census was created to guide bedside recruit- 1. 2. 3. 4. 5. The word ‘legacy’ is one that we hear used in many different ways, but it is also a word that is hard to define. How would you define the concept of ‘legacy’ for you and your family? What sorts of experiences in your life have led you to this particular definition? What other sources of information have you used when thinking about legacy in this way? When you hear the word legacy, what is your first reaction? (Prompting for emotional response rather than cognitive process.) Is there anything you’d like to share that we haven’t asked? ment. Eligible participants were approached at their child’s bedside by two members of the research team. As one team member guided the parent/caregiver through the study details, consent document, and demographic survey (participants documented written consent and survey responses using a REDCap-enabled electronic tablet), the other team member engaged in play and conversation with the child, if appropriate. When multiple parents/caregivers were present, met eligibility criteria, and were interested in participation, they were allowed to do so; however, this was a rarity given the difficulty families often face when balancing a child’s hospitalization with other needs at home, work, and school. Although parents/caregivers were asked to participate in this study during the stress and uncertainty of a child’s inpatient hospitalization, many of which were for critical illnesses or injuries, those approached by the research team rarely declined to participate. Instead, participant accrual was at times limited due to parents/caregivers not being at bedside for various reasons, concurrent medical procedures in progress or needing to begin, or medical staff other than the primary nurse providing bedside care. In these situations, the research team offered to return at another time if appropriate or made note to attempt recruitment on a different day and time, if possible. Procedures All parents/caregivers who met eligibility criteria and chose to participate were immediately enrolled PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 in the study. After digitally signing the study consent form using a REDCap-enabled electronic tablet, each participant completed a brief demographic survey on the tablet that collected information about the parent/caregiver and the nature of their child’s hospitalization. Parents/ caregivers then participated in a brief, in-person semi-structured interview about their legacy perceptions and experiences that lasted an average of 25 minutes. All participants were offered a choice of locations and accommodations for completing the interview to minimize inconvenience, maximize opportunities for empowerment and control, and respect parent/caregiver and patient privacy (Boles, 2018; Boles & Daniels, 2019); however, all but two participants chose to participate in their child’s hospital room. The semi-structured interview guide consisted of five open-ended questions, with probes added as needed to clarify participant perceptions and experiences (see Figure 1). Each participant was first asked to describe how they would define the word ‘legacy;’ follow-up questions were then asked about the legacy experiences, information sources, thoughts, and feelings they incorporated into their definition. One of the research team members conducted and audio-recorded the semi-structured interview, while the other remained available to play and interact with the patient as needed during this time. Both research team members were trained graduate student research assistants. Participation in this study concluded with completion of the semistructured interview. 61 Figure 2. Data Analysis Procedures Open coding: Each line of each transcript coded independently by two team members. Recurrent or similar codes are combined into categories. Perceptions of the Concept of Legacy Transcripts reread to check for relevance of categories. Connections between and across categories noted and used to assemble themes. Transcripts reread to ensure that themes developed reflect participants’ experiences. A group textural description is developed to detail themes as seen in participants’ words. Source. Adapted from process and figure described by Boles et al., 2017. Data Analysis Descriptive statistics were conducted in SPSS (IBM, 2019) to better characterize the study sample. All interviews were transcribed verbatim, double-checked by another member of the research team, and then independently coded by two members of the research team using an inductive, categorizing process outlined by Boles and colleagues (2017) and shown in Figure 2. An inductive, line-by-line coding approach was chosen both due to the lack of pre-existing theoretical frameworks for the concept of legacy, and to allow for diverse thoughts, experiences, and beliefs that may otherwise have been limited by a deductive coding scheme. Rather than resolving code discrepancies through consensus meetings, codes from both reviewers were entered in a comprehensive spreadsheet to maximize the diversity of perspectives and interpretations present in the findings. Through continued reviews of tran- 62 parents/caregivers were unsure how to answer this question and asked the research team members for clarity. More than half of the sample (56%) had been hospitalized for four or more days at the time of participation in this study. scripts and the individual codes, repetitive or overlapping codes were collaboratively assembled into larger categories by the research team. Related categories were then combined to comprise the four themes detailed below. Findings were discussed with all members of the research team to ensure completeness and accuracy of interpretations, resolve disagreements, and ensure that themes remained rooted in the data. Results Sample Characteristics The final sample (see Table 1) included 93 parents/caregivers of pediatric patients receiving inpatient acute or critical care. Participants were largely female (69%), white (78%) mothers (68.8%) between the ages of 30 and 39 years (39%). Of the 93 participants, an acute majority reported their child had a illness (52%) rather than a chronic condition; of note, several Thematic analysis of semi-structured interview data yielded four themes: 1) legacy is a transgenerational process; 2) legacies can be actions, accomplishments, and experiences; 3) legacy can be a powerful tool used for education and change; and 4) a ‘good’ legacy can be left in different ways. Theme 1: Legacy is a transgenerational process. Parents and caregivers largely defined legacy as a transgenerational process passed across generations through “children, grandchildren, down along the line. Years and years.” As one grandmother noted: …genealogy, that’s the way I think about legacy, like what is behind you plus what is ahead of you. How your family left the legacy for you and how you’re going to leave the legacy for your kid. According to a mother of a teenager with an eating disorder, legacy could take many forms. Legacy could be passed through tangible items such as assets, possessions, “monetary gifts and land,” but more importantly, legacy was defined by the intangibles – “the values and morals passed from generation to generation.” Thus, legacy “may not be something tangible you can feel, it could just be thoughts and ideas and processes” that are passed through and across generations. Grandparents and parents are common sources of one’s knowledge of family legacy. Stories and memories provide other family members with a window into influential stories that shaped family dynamics and parenting practices. In this vein, legacy was conceptualized as something unique to each family. Additionally, legacy often brought about reminiscence and PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 Table 1. Participant Demographics N Percentage (%) Mother 64 68.8 Father 23 24.7 Other 6 6.5 20-29 20 21.5 30-39 36 38.7 40-49 23 24.7 50+ 12 12.9 Variables nostalgia of the past and reflection of how their family legacy has been carried on to the present. As one participant described: Relationship to Patient Age (Years) Race White 72 77.4 Black/African American 8 8.6 Hispanic/Latino 5 5.4 Other 7 7.6 12 12.9 $10,000-$20,000 7 7.5 $20,001-$30,000 12 12.9 $30,001-$45,000 8 8.6 $45,001-$60,000 19 20.4 Greater than $60,000 30 32.3 4 4.3 High school/GED 23 24.7 Some college 24 25.8 Annual Income Less than $10,000 Education Level Less than high school Associates 8 8.6 Bachelors 22 23.7 Graduate cegree 5 5.4 PhD, MD, terminal degree 2 2.2 Single 20 21.5 Married 57 61.3 Divorced 9 9.7 Chronic 40 43.0 Acute 48 51.6 1 13 14.0 2 11 11.8 3 13 14.0 4+ 52 56.0 Marital Status Admission Reason Length of Hospital Stay (Days) Notes. N = 93; some participants did not disclose all demographic variables. PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 Just watching family, you always have that one that kind of stands out that’s the leader that you look to what grandma did, what did grandma say. She kind of leads all the way down and you keep following what she started. Legacies were primarily defined by qualities and possessions bestowed upon the current generation and intended to carry into the future. As one father explained: If you’re a lucky enough individual to have had children, your legacy is embedded in them. It’s kind of your values, morals, and ideals that you’ve shown them throughout your life. So the things you’re interested in, they will be interested in. The values and ideals that you’ve had that you’ve bestowed in them will carry on with them. Theme 2: Legacies can be actions, accomplishments, and experiences. Legacy was identified as something both bestowed and earned. When thinking about legacy, participants took stock of their past and current possessions, inventorying who they were and what they had done in their lifetime. Legacy was conceptualized as “deeds or actions that are notable” defined by personal stories, values, principles, and beliefs. As one father shared: “I think it’s just be the best person you could be, do right by others. I don’t look at legacy as much as a family name that carries on but more of your actions.” Legacy encapsulates one’s life challenges and life journey, both where they’re from and what they’ve accomplished. Life experiences that shape one’s legacies were identified as school, business legacies, occupation, and personal or familial health challenges. According to participants, past experiences help shape actions, principles, and beliefs. For some, legacy is a 63 reminder to keep fighting; for others, it is a reminder to live the best life and reach their full potential in daily actions. As reflected by one father: “It is not necessarily what you leave; it’s about what you’re doing.” To have good morals, donate to charity, volunteer, and be thoughtful and compassionate with others are all ways participants describe legacy as being intentional. According to participants, hard work and perseverance are also ways people make a name for themselves. In this sense, legacy was reported as a choice – a choice of life philosophy, beliefs, and actions. Participants highlighted one’s character, influence, impact, and impression on others, whether through family name, achievements, or research, as defining “what one is known for” and “what they stood for.” Theme 3: Legacy can be a powerful tool used for education and change. According to the mother of a teenage patient with a neurological condition, people learn from and teach through legacy. Many learn from others’ successes and strive to “live [their] life like they [elders] lived theirs.” However, legacy was also used to learn about what not to do – from stories to historical events and contexts. In other words, legacy acted as an opportunity to avoid repeating history and past mistakes, as described by a mother of a patient with leukemia: My dad had a difficult childhood and family history. Kind of in one generation, he sort of turned it all around and was this phenomenal father and husband… he kind of changed his whole legacy that was passed to him. His legacy was able to be turned around in one generation for the rest of us. In this sense, legacy was reported as a time for growth and positive change in the future – an opportunity to rise above a difficult childhood, overcome adversity, and avoid parents’ mistakes. According to another participant: “You don’t have to take what 64 your family gave you,” but instead you can “enhance it, modify it and make it better.” One father described legacy as an opportunity to provide children with opportunities they did not have growing up: My legacy for him [patient] is to accomplish what I couldn’t in life. For him to go to college and be all that he can be … It [legacy] makes me feel good because I know I will be able to give him what I didn’t have growing up. I will be able to push him as far as he can go. I want him to…become something in life and achieve something. Legacy was also defined by pushing children to accomplish things and “helping them be happy and strong in the process.” Cultivating “patience, understanding, acceptance, and love of differently abled people” were important lessons to be learned from and taught to others, both generationally and through friends, communities, and work. Thus, legacy was referred to as a powerful tool that provided an avenue for change and a teaching model for the future. Theme 4: A ‘good’ legacy can be left in different ways. Legacy was symbolic of “what you leave behind for them [children],” which can take various forms. One mother said legacy was “what you stood for and what you accomplished and kind of what you want them [children] to stand for and accomplish in their lifetime.” On the other hand, some participants described legacy as “the way [someone] was remembered. Not necessarily while they were alive but definitely after they’ve passed away,” so they stressed the importance of leaving a ‘good’ legacy for people to remember them by and for others to follow. For some, leaving a ‘good’ legacy was about building and purchasing things, such as businesses and land, to make a name for oneself for others to remember them by. For others, legacy was defined by one’s behavior – doing good things, doing right, and having good morals. As described by another mother of a pediatric cardiology patient, “…when you leave something behind, an inheritance, that’s always good. But what’s more important is the character traits and attitudes that you leave for them and how to live their life.” In this sense, legacy was something to work towards with the intent of “leaving the earth and the people you know on earth better than it was when you were there.” One mother of a child with acute peritonitis shared an understanding of legacy as: What you leave behind when you go… the life you lived, if you lived a good life. People are going to talk about that, you know. If you did great things, you donated to charities, or you did this to support this group of people, or things like that. That would be a legacy you leave behind. So trying to leave the world a better place than you came into it. The definitions and expectations of what encompassed a ‘good’ legacy were a product of one’s surroundings – experiences, stories, communities, friendships, books, news, or research. Although there were various definitions of what a good legacy meant, participants were “hopeful that there’s some good things to be left” and fostered a personal hope that “I’ve done some good, somewhere.” Discussion Health care experiences, especially those expected to, or likely to result in, terminal illness or death are significant sources of stress for individual patients, their caregivers, and the families that support them (Doupnik et al., 2017). Not only can these events engender immediate coping challenges and threats to psychosocial wellbeing, but if unrecognized and unaddressed, persistent distress can impair psychological health and functioning throughout the lifespan (Price et al., 2016). Thus, CCLSs and other health care professionals frequently offer legacy-oriented interventions PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 to help patients and families make meaning of their experiences and promote the adaptive coping efforts that characterize resilience (Boles, Fraser et al., 2020). However, the forms, features, and functions of legacy that underlie these practices have not yet been systematically addressed, rendering the concept of legacy itself an untouched undertaking from the perspective of parent/caregiver stakeholders. Therefore, this study explored the legacy perceptions of parents/caregivers of hospitalized pediatric patients to help professional design interventions that are truly family-centered and evidence-informed. Using a phenomenological qualitative design (Moustakas, 1994) and inductive categorizing analysis as per Boles and colleagues (2017), this study revealed that parents/ caregivers of hospitalized children describe legacy as 1) a transgenerational process; 2) actions, accomplishments, and experiences for which one is remembered; 3) a powerful tool that can be used for education and change; and 4) a ‘good’ legacy can be left in different ways. Some of these understandings closely mirror what has been described in previous work regarding perceptions of the concept of legacy and legacy-oriented interventions in adult and geriatric health care, as described by Scarton and colleagues (2018), Franklin and Cheung (2017), and Allen and colleagues (2008). However, some key differences emerged, reinforcing the need for additional education about and interventional research on legacy-oriented needs and interventions for hospitalized children and their families. Legacy as a Transgenerational Process Parent/caregiver descriptions of legacy as a transgenerational process echo previous research defining legacy as the transmission of one’s self across generations (Hunter, 2008). However, participants in this study especially emphasized the contributions of their child’s illness or hospitalization to their beliefs about legacy. Rather than remaining focused on legacy as remnants of the past, parents/caregivers acknowledged the impact of the present hospitalization on their perceptions of their child’s legacy as well as their own. Health care providers, when serving parents/caregivers of hospitalized children, should acknowledge multiple generations of legacy as a contextual factor in a family’s experiences, communication, and decision-making. It is important to understand the values and preferences parents/caregivers relay in their child’s care may be related to not only their own experiences in the present, but also those of the people before them that were central to their development. Given this cross-generational and multitemporal feature of legacy, it is essential for health care providers to allow parents/caregivers to involve multi-level familial supports and perspectives in their child’s health care experience. Whether inquiring about a family’s preferences or designing hospital visitation policies, health care staff should prioritize opportunities for parents, grandparents, and other generations of caregivers to provide the invaluable psychosocial support that pediatric patients and family members need when hospitalized. Representation of One’s Actions, Experiences, Effects, and Accomplishments Operationalized as “legacy-building” activities or enacted as “dignity therapy” or “life-review” protocols, the concept of legacy has been diversely applied to health care, especially for those patients and families anticipating loss or approaching the end of life. Like previous reports with terminally ill adult patients (Allen et al., 2008; Hunter, 2008), participants in this study ascribed both tangible and intangible qualities to legacy, from genetic and monetary inheritances to social roles, character traits, values, and perceived impacts on others. Notably different in this study population was the proportion of intangible descriptions to those that involved physical items; parents/caregivers in this study more frequently reported and emphasized one’s actions, beliefs, relationships, and personal experiences, PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 describing these as more important than physical assets or artifacts. This focus on the intangible components of legacy starkly contrasts with current legacy-oriented intervention practices in children’s hospitals, as described by Foster and colleagues (2012), as well as those employed in adult health care settings (Allen et al., 2008; Riegel et al., 2019; Scarton et al., 2018). As the 2012 study by Foster and colleagues highlights, most children’s hospitals provide standardized, tangible, legacy-making activities or items, such as painted handprints, plaster hand-molds, or collections of the child’s hospital belongings – primarily offered at the end of a child’s life. However, because longitudinal research about the impact of these interventions is currently limited, it is possible these items do not sufficiently embrace the immaterial aspects of legacy that parents/caregivers of hospitalized children appear to prioritize. Additionally, the study by Foster and colleagues (2012) revealed that most children’s hospitals offer these legacy-making activities at certain intervals, namely when cure is no longer being sought, at the time of death, or after time of death. Similarly, in adult care, the majority of legacy-oriented interventions are offered to older adults or those with terminal illness in anticipation of the end of life (Allen et al., 2008; Chochinov et al., 2005; Naik et al., 2016; Piderman et al., 2017). Not only does providing interventions in this way associate the concept of legacy with death in a way that directly contradicts the perceptions of participants in this study, but this limited schedule of support also depersonalizes and limits what these interventions can convey about the unique relationships and experiences of a child’s life. It is imperative, then, that CCLSs and other health care providers assist families in recognizing and describing the intangible components of their child’s legacy, regardless of expected illness outcome, throughout the child’s hospital experience. Encouraging families to engage in favorite activities, memory-making opportunities, and collaborative experiences can be done by CCLSs 65 at any point in a child’s care trajectory. Partnering with CCLSs, social workers, creative arts therapists, hospital activity coordinators, and nursing staff can help families access memorable opportunities to play, connect, and build legacy with one another throughout their care experience. Acknowledging developmental milestones by recreating important routines and rituals, interacting with special events or visitors, or helping families connect with wish-granting or other nonprofit organizations are all ways to help families create unique experiences and build memories together. In addition, engaging in individualized discussions or activities – rather than relying on standardized legacy practices – can help children and families strengthen their relationships, honor their history, anticipate their future, and support their coping efforts in the face of medical stress (Boles, Fraser et al., 2020). Educational Value of a Legacy Unlike previous research with adult patient populations, parents/ caregivers of hospitalized children in this study focused on the educational value of legacy, frequently describing lessons they felt they had learned from their child’s illness or injury. Witnessing their child in this environment seemed to serve as an inspiration to live life with renewed perspective, work hard for their family, and strive to succeed as a parent and individual. Additionally, parents/caregivers in this study expressed perceptions of legacy as an avenue for change, sharing that they intentionally selected aspects of their own experiences and those of the family members before them to mimic, discard, or transform while raising and supporting their children. Honoring family relationships by aligning hospital practices and services with the tenets of patient- and family-centered care (Institute for Patient-and-Family-Centered Care, 2017), CCLSs create opportunities for improved assessment of a child and family’s health care needs, which also includes their current legacy-oriented needs and preferences. By taking the time to learn about family histories and motiva66 tions, and the ways in which families apply these sentiments to their child’s treatment trajectory, CCLSs and other multidisciplinary health care providers can better meet patients and families “where they are” in their hospitalization experience (The Beryl Institute, 2019). Thus, it is essential for health care providers to support families as they share, reject, or change their legacies during their child’s inpatient hospitalization. Leaving a ‘Good’ Legacy Many participants reflected on the importance of leaving a ‘good’ legacy for people to remember them by and for their children to learn from or emulate. Like previous research, parent/caregivers in this study shared that regardless of the medium or intentionality of one’s legacy, they believe everyone wants to leave a meaningful legacy (Boles, 2014). For the parents/caregivers in this study, many aspects of a ‘good’ legacy were related to how each participant interpreted the meaning of being a ‘good’ parent. A good legacy would, as they reported, pass along values and ideals associated with positive aspects of their parental identity, which is consistent with previous research (Hunter, 2008; Naik et al., 2016; Schellinger, 2018). In response to this finding, CCLSs and other health care providers should help parents/caregivers identify ways they can safely and effectively be involved in their hospitalized child’s care, whether the child is alert and playful or intubated and sedated. Whether they connect with their child through play activities, reading books, massaging hands and feet, or bringing comfort items from home, parents/caregivers need opportunities to enact their parent role in a time when it is challenged by the limitations of illness or injury. Additionally, as in other social service contexts, health care is optimized when it is provided in accordance with patient and family preferences and experiences; thus, it is possible parents/caregivers will not only draw upon their legacy experiences in making health care decisions, but the legacy of these decisions may be a weighty factor in their considerations. Therefore, it is important for providers to recognize legacy as a medium for facilitating parent-child connection, involvement in the child’s care, and promoting parent/caregiver and patient engagement in their health care experiences. Toward a Standardized Definition Overall, parents/caregivers described their perceptions of the concept of legacy as transgenerational – something passed to, from, and across families. Stories, possessions, values, and assets were all ways in which legacy could be passed through and across generations overtime. As such, it appears that legacy, for this population aligns with Boles and Jones’ (2021) definition of legacy as “as an enduring representation of the self—its qualities, experiences, effects, and relationships—built and bestowed across generations. Whether concrete or intangible, intentional, or serendipitous, legacies are avenues of connection, education, inspiration, or transformation” (p. 19) Grounded in the words and experiences of parents/caregivers of hospitalized children, articulating legacy across these dimensions provide a variety of perspectives and elements for clinical application and research. When legacy is understood in this way, many new possibilities emerge for capturing and integrating a family’s unique history, stories, strengths, and experiences, whether during a child’s hospitalization or other health care contexts, such as clinics, emergency departments, or home-based health and hospice care. Thus, CCLSs and other medical and psychosocial care providers should assess, recognize, and involve parent/caregivers’ experiences with and understandings of legacy into legacy-oriented interventions or activities, as well as other aspects of care related to patient and family coping and functioning. Future research should investigate how hospitalized children, non-parental family members, and health care providers define the concept of legacy to PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 assess for similarities and differences that may impact medical and psychosocial care activities or approaches. Additionally, further research should focus on the child and family’s experiences with and the outcomes associated with legacy interventions or activities during a child’s hospitalization. Limitations and Conclusion This was a single-site study, which might limit the transferability of findings, especially given the cultural and individual variables that appear to shape the legacy perceptions of parents/caregivers. Further, the study sample was limited to English-speaking participants due to the composition and resources of the research team; given that language is a culturally laden phenomenon, it is possible that the term ‘legacy’ may not transfer across languages and cultural traditions, therefore limiting the scope of this study’s results. More work is needed to expand cross-cultural definitions of legacy according to caregivers of hospitalized children to inform best practices across health care settings. References Akard, T.F., Duffy, M., Hord, A., Randall, A., Sanders, A., Adelstein, K., Anani, U.E., & Gilmer, M.J. (2018). Bereaved mothers’ and fathers’ perceptions of a legacy intervention for parents of infants in the NICU. Journal of Neonatal-Perinatal Medicine, 11(1), 21-28. Allen, R.S., Harris, G.M., Burgio, L.D., Azuero, C.B., Miller, L.A., Shin, H.J., Eichorst, M.K., Csikai, E.L., DeCoster, J., Dunn, L.L., Kvale, E., & Parmelee, P. (2014). Can senior volunteers deliver reminiscence and creative activity interventions? Results of the legacy intervention family enactment randomized controlled trial. Journal of Pain and Symptom Management, 48(4), 590601. Allen, R.S., Hilgeman, M.M., Ege, M.A., Shuster, J.L., Jr., & Burgio, L.D. (2008). Legacy activities as interventions approaching the end of life. Journal of Palliative Medicine, 11(7), 1029-1038. Andersen, E.W., Frazer, M.S., & Schellinger, S.E. (2018). Expanding the palliative care domains to meet the needs of a community-based supportive care model. American Journal of Hospice and Palliative Medicine, 35(2), 258-265. Association of Child Life Professionals. (2020). ACLP official documents. https:// education.childlife.org/aclp Boles, J.C. (2014). Creating a legacy for and with hospitalized children. Pediatric Nursing, 40(1), 43-44. Boles, J.C. (2018). Treading carefully: Conducting qualitative research with children who have cancer. Journal of Ethnographic & Qualitative Research, 13, 6277. Boles, J.C., & Daniels, S. (2019). Researching the experiences of children with cancer: Considerations for practice. Children, 6(8), 93-104. Boles, J.C., Fraser, C., Bennett, K., Jones, M., Dunbar, J., Woodburn, A., Gill, M.A., Duplechain, A., Munn, E., & Hoskins, K. (2020). The value of Certified Child Life Specialists: Direct and downstream optimization of pediatric patient and family outcomes. Executive summary. Association of Child Life Professionals. https://www.childlife.org/docs/defaultsource/the-child-life-profession/valueof-cclss-executive-summary.pdf Boles, J.C., & Jones, M.T. (2021). Legacy perceptions and interventions for adults and children receiving palliative care: A systematic review. Palliative Medicine, 35(3), 529-551. https://doi.org/10.1177/ 0269216321989565 Boles, J.C., Jones, M., Dunbar, J., & Cook, J. (2020). Defining legacy: The perceptions of pediatric healthcare providers. Clinical Pediatrics, 59(11), 1004-1010. Boles, J.C., Winsor, D.L., Mandrell, B., Gattuso, J., West, N., Leigh, L., & Grissom, S.M. (2017). Student/patient: The school perceptions of children with cancer. Educational Studies, 43, 549566. Canga, M., Malagnino, I., Malagnino, G., & Malagnino, V.A. (2020). Evaluating different stressors among parents with hospitalized children. Journal of Education and Health Promotion. 9(9), 1-6. Chochinov, H.M., Hack, T., Hassard, T., Kristijanson, L.J., McClement, S., & Harlos, M. (2005). Dignity therapy: A novel psychotherapeutic intervention for patients near the end of life. Journal of Clinical Oncology, 23(24), 5520-5525. Doupnik, S.K., Hill, D., Palakshappa, D., Worsley, D., Bae, H., Shaik, A., Qiu, M.K., Marsac, M., & Feudtner, C. (2017). Parent coping support interventions during acute pediatric hospitalizations: A meta-analysis. Pediatrics, 140(3), e20164171. https://doi.org/10. 1542/peds.2016-4171 Foster, T.L., Dietrich, M.S., Friedman, D.L., Gordon, J.E., & Gilmer, M.J. (2012). National survey of children’s hospitals on legacy-making activities. Journal of Palliative Medicine, 15(5), 573-578. Foster, M., Whitehead, L., & Maybee, P. (2016). The parents’, hospitalized child’s, and health care providers’ perceptions and experiences of family-centered care within a pediatric critical care setting: A synthesis of quantitative research. Journal of Family Nursing, 22(1), 6-73. Franklin, F.C., & Cheung, M. (2017). Legacy interventions with patients with cooccurring disorders: Legacy definitions, life satisfaction, and self-efficacy. Sub- PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 stance Use & Misuse, 52(14), 18401849. Hunter, E.G. (2008). Beyond death: Inheriting the past and giving to the future, transmitting the legacy of one’s self. OMEGA-Journal of Death and Dying, 56(4), 313-329. Institute for Patient- and Family-Centered Care. (2017). Advancing the practice of patient- and family-centered care in hospitals. Author. https://www.ipfcc.org/ resources/getting_started.pdf Keall, R.M., Butow, P.N., Steinhauser, K.E., & Clayton, J.M. (2013). Nurse-facilitated preparation and life completion interventions are acceptable and feasible in the Australian palliative care setting: Results from a phase 2 trial. Cancer Nursing, 36(3), E39-E46. Martínez, M., Arantzamendi, M., Belar, A., Carrasco, J.M., Carvajal, A., Rullán, M., & Centeno, C. (2017). ‘Dignity therapy’, a promising intervention in palliative care: A comprehensive systematic literature review. Palliative Medicine, 31(6), 492-509. McDermott, K.W., Elixhauser, A., & Sun, R. (2017). Trends in hospital inpatient stays in the United States, 2005-2014 (Statistical Brief #225). Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality. https://www.hcup-us.ahrq.gov/reports/ statbriefs/sb225-Inpatient-US-StaysTrends.pdf Moustakas, C. (1994). Phenomenological research methods. Sage. Naik, A.D., Martin, L.A., Moye, J., & Karel, M.J. (2016). Health values and treatment goals of older, multimorbid adults facing life‐threatening illness. Journal of the American Geriatrics Society, 64(3), 625-631. Piderman, K.M., Breitkopf, C.R., Jenkins, S.M., Lovejoy, L.A., Dulohery, Y.M., Marek, D.V., Durland, H.L., Head, D.L., Swanson, S.W., Hogg, J.T., Evans, J.L., Jorgenson, S.E., Bunkowski, L.J., Jones, K.L., Euerle, T.T., Kwete, G.M., Miller, K.A., Morris, J.R., Yoder, T.J., Lapid, M.I., … Jatoi, A. (2015). The feasibility and educational value of “hear my voice,” a chaplain-led spiritual life review process for patients with brain cancers and progressive neurologic conditions. Journal of Cancer Education, 30(2), 209-212. Piderman, K.M., Radecki Breitkopf, C., Jenkins, S.M., Lapid, M.I., Kwete, G.M., Sytsma, T.T., Lovejoy, L.A., Yoder, T.J., & Jatoi, A. (2017). The impact of a spiritual legacy intervention in patients with brain cancers and other neurologic illnesses and their support persons. Psycho‐ oncology, 26(3), 346-353. Price, J., Kassam-Adams, N., Alderfer, M., Christopherson, J., & Kazak, A. (2016). Systematic review: A reevaluation and update of the integrative (trajectory) model of pediatric medical traumatic stress. Journal of Pediatric Psychology, 41(1), 86-97. continued on page 102 67 Parent/Caregiver Perceptions continued from page 67 Ramirez, F.D., Bogetz., J.F., Kufeld, M., & Yee, L.M. (2019). Professional bereavement photography in the setting of perinatal loss: A qualitative analysis. Global Pediatric Health, 6, 1-12. Riegel, M., Randall, S., & Buckley, T. (2019). Memory making in end-oflife care in the adult intensive care unit: A scoping review of the research literature. Australian Critical Care, 32(5), 442-447. Scarton, L.J., Boyken, L., Lucero, R.J., Fitchett, G., Handzo, G., Emanuel, L., & Wilkie, D.J. (2018). Effects of dignity therapy on family members: A systematic review. Journal of Hospice & Palliative Nursing, 20(6), 542-547. Schaefer, M.R., Spencer, S.K., Barnett, M., Reynolds, N.C., & MadanSwain, A. (2019). Legacy artwork in pediatric oncology: The impact on bereaved caregivers’ psychological functioning and grief. Journal of Palliative Medicine, 22(9), 1124-1128. Schellinger, S.E., Anderson, E.W., Frazer, M.S., & Cain, C.L. (2018). Patient self-defined goals: Essentials of person-centered care for serious illness. American Journal of Hospice and Palliative Medicine, 35(1), 159-165. Sisk, C., Walker, E., Gardner, C., Mandrell, B., & Grissom, S. (2012). Building a legacy for children and adolescents with chronic disease. Journal of Pediatric Nursing, 27, e71-e76. The Beryl Institute. (2019). What patient experience can learn from child life professionals. https://www.theberylinstitute.org/store/ ViewProduct.aspx?id=11084124 102 PEDIATRIC NURSING/March-April 2022/Vol. 48/No. 2 Copyright of Pediatric Nursing is the property of Jannetti Publications, Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.