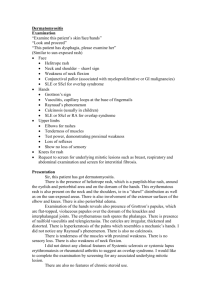
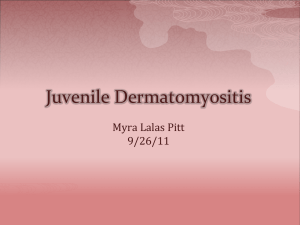
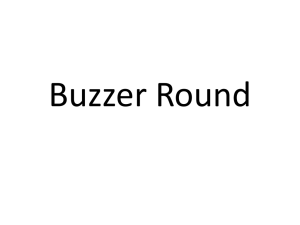
Search Home Rheumatology International Article Download PDF Case Based Review Published: 23 December 2019 Dilemma in management of hemorrhagic myositis in dermatomyositis Julia M. Chandler Irene L. Wapnir , Yoo Jung Kim, Justin L. Bauer & Rheumatology International 40, 331–336 (2020) 616 Accesses Metrics 6 Citations 7 Altmetric Abstract Dermatomyositis (DM) is a rare inflammatory disorder affecting the muscle and skin. DM patients can present with spontaneous muscle hemorrhage, a potentially fatal complication. The best practice for management of hemorrhagic myositis in these patients remains unclear. Here we discuss the case of a patient who presented with progressive muscle weakness and intermittent rash that was diagnosed with dermatomyositis. During admission, she developed spontaneous hemorrhagic myositis of the right pectoralis Log in major treated with surgical evacuation. She also developed a spontaneous left anterior thigh hematoma which was treated conservatively. She recovered and showed no evidence of recurrent bleeding at either location. We performed a literature review and identified ten cases of spontaneous hemorrhage in DM patients, with a 60% mortality rate among reported cases. Given the high mortality rate associated with spontaneous hemorrhage in DM patients, it is important for physicians to be aware of the diagnosis, workup, and management strategies. Access provided by Specialized Presidential Council for Educ and Scientific Research Portal Working on a manuscript? Avoid the common mistakes Introduction Dermatomyositis (DM) is a rare systemic autoimmune disease of skin and muscle inflammation that affects 3 to 23 in 100,000 people [1, 2]. Patients present with weakness of the proximal muscles, pink papules overlying the dorsal interphalangeal joints (Gottron’s papules), periorbital rash (Heliotrope sign), and nailfold telangiectasias. DM is associated with an increased incidence of cancer, esophageal motility disorders, calcinosis, and interstitial lung disease [3]. Spontaneous hemorrhagic myositis is a rare complication of DM that can be fatal [4,5,6,7,8]. The pathophysiology has not been clearly elucidated; previous case reports describe a possible association with deep vein thrombosis (DVT) prophylaxis medications such as heparin and dalteparin, although cases of idiopathic hemorrhagic myositis also exist [5, 9]. We describe a case of recurrent hemorrhage in a patient with DM. A review of the literature of DM-related spontaneous muscular hematomas and their management and prognosis is included. Case presentation A 64-year-old female with no significant past medical history and no current medications presented to the emergency department with a 2-month history of progressive weakness, a 5-month history of intermittent rash of the face and hands, and a 1-week history of progressive hoarseness and dysphagia. The generalized muscle weakness was severe as she was unable to stand from a chair or lift her head while supine. Other notable features of the physical exam were Gottron's papules on the bilateral fingers, violaceous rash or Holster sign on the thighs, and non-pitting edema in both legs. Muscle strength was 3/5 in the proximal upper extremities, hip flexors, and hip extensors. Labs were consistent with DM, including elevated aspartate aminotransferase (337 U/L; reference: < 40 U/L), alanine aminotransferase (276 U/L; reference: < 60 U/L), creatinine kinase (4812 ng/mL; reference: < 60 ng/mL), c-reactive protein (1.9; reference: < 0.9 mg/dL), and lactate dehydrogenase (2268 U/L; reference: < 340 U/L). Coagulation labs were notable for an elevated activated partial thromboplastic time (54.1 s; reference: 25.1–36.6 s); however, these labs were drawn after initiation of routine prophylactic subcutaneous heparin, and a subsequent PTT inhibitor screen had indeterminate results due to the presence of anticoagulant in the sample. She tested weakly positive for anti-Mi-2, but other DM- associated antibodies were negative. Skin biopsy showed “vacuolar interface dermatitis with mucin,” compatible with DM. The patient had no known risk factors for malignancy, and an extensive screening workup for cancer was performed with studies for breast, colon, and cervical cancers all negative. On admission, the patient was started on methylprednisolone 1 g for 3 days, intravenous immunoglobulin 2 g/kg over 2 days, and mycophenolate mofetil 500 mg twice daily, resulting in prompt improvement in strength and swallowing (Fig. 1). Subcutaneous heparin for DVT prophylaxis was also initiated. Fig. 1 Timeline of significant events and medication regimen for a case of hemorrhagic myositis in a dermatomyositis patient Two days after admission, she developed rapid enlargement of the right breast (Fig. 2) associated with hypotension of 60/36 and a drop in hemoglobin from 12.0 to 9.7 g/dL. Two units of fresh frozen plasma were administered, and a computed tomography (CT) angiogram of the chest revealed active arterial extravasation within a 13 cm hematoma located in the right pectoralis major muscle (Fig. 3). Given the hemodynamic instability and further decrease in hemoglobin to 7.9 g/dL over the ensuing hours, the patient was taken to the operating room for hematoma evacuation and exploration for the source of bleeding. The muscle fibers were splayed, containing a 400 mL hematoma that extended medially to the sternal border, superiorly to the clavicle, and laterally along the mid-axillary line down to the inframammary fold. However, no significant arterial or venous bleeding vessels were identified. Numerous bleeding small intramuscular vessels were cauterized or ligated. Two units of packed red blood cells and one unit of cryoprecipitate were administered intraoperatively, and a JacksonPratt drain was placed. A muscle biopsy was sent as part of the surgical pathology and was notable for “extensive hemorrhage” in the setting of a “chronic myopathic process.” Fig. 2 Top–down comparison between the normal left breast and the swollen right breast in a dermatomyositis patient with hemorrhagic myositis of the right pectoralis major. The right breast demonstrates tense fullness superiorly and laterally Fig. 3 Computed tomography (CT) angiogram demonstrating large right pectoralis major hematoma in a dermatomyositis patient with hemorrhagic myositis. There is active extravasation within the hematoma, surrounding fat stranding, and edema involving the serratus anterior. a Arterial phase CT with black arrow pointing to a focus of active extravasation within the hematoma, b venous phase CT with a black arrow pointing to further pooling of extravasated contrast The postoperative recovery was uneventful. However, on the second day, the patient experienced increasing pain and swelling in the anterior left thigh. An ultrasound showed a massive 30.5 cm hematoma occupying the area. This represented a second episode of hemorrhagic myositis. A decision was made to treat this event conservatively with a pressure dressing, because the patient was otherwise asymptomatic and blood counts remained stable. There was minimal drainage from the chest wall drain, and she was discharged to a skilled nursing facility on oral prednisone 60 mg daily and mycophenolate mofetil 1500 mg twice daily. Ten months after discharge, the patient’s overall muscle strength has improved except for the left lower extremity where the hematoma was not drained. Bilateral manual muscle testing 8 (MMT8) scores have been largely stable to improving, with scores of 128 when first performed 6 months after admission and 133 another 6 months later (maximum score possible: 150). Significantly, the characteristic skin findings, including Holster sign and pink erythema of face, neck, hands, elbows, arms, and knees, have persisted, but with gradual improvement over time; scores on the Cutaneous Dermatomyositis Disease Area and Severity Index (CDASI) decreased from 16 to 9 in the 3 months following admission. She remains compliant with a regimen of mycophenolate mofetil 1500 mg twice daily and prednisone 5 mg daily, which is being tapered. Search strategy We used MEDLINE, EMBASE, Scopus, and Web of Science to find studies describing patients with spontaneous hemorrhagic myositis in the context of a previous or concurrent DM diagnosis. The search was conducted using the following terms: “dermatomyositis” and “spontaneous hematoma” or “spontaneous hemorrhage” or “spontaneous hemorrhagic myositis.” The search was performed from inception of each database through August 2019. The references in each selected study were reviewed to identify other relevant articles. We excluded non-English articles, conference abstracts, and articles describing hemorrhagic myositis in patients not previously or concurrently diagnosed with DM. Two authors reviewed the search results and agreed on the included articles. From each article selected, data were collected on age, gender, location of the hematoma(s), presence of DM-associated antibodies, the use of DVT prophylaxis prior to identification of the spontaneous hematoma, the treatment for the spontaneous hematoma, the listed complications, and the case outcome. Results We identified eight reports describing ten cases of spontaneous hemorrhage in patients with DM (Table 1) [4,5,6,7,8,9,10,11]. The cases occurred most commonly in adults older than 50, with roughly equal rates in males and females [10]. The sites of hemorrhage were varied, including the deltoid and trapezius muscles, rectus abdominus, retroperitoneum, and psoas muscles; five out of ten patients experienced involvement of the iliacus and psoas [5, 7, 8, 11]. Six out of ten patients presented with at least two hematomas in distinct anatomical locations [5,6,7, 11]. Treatment strategies included observation, conservative treatment with blood transfusion, and embolization. There was a 60% mortality rate among reported cases. Table 1 Reported cases of spontaneous hemorrhagic myositis in dermatomyositis patients Discussion Hemorrhagic myositis is a rare complication of DM, with only ten prior cases reported in the literature. It occurs most commonly in adults over 50 years of age with roughly equal rates in males and females, and various muscle groups can be affected. In the majority of reported cases, DM-associated hemorrhagic myositis is fatal. There is no consensus on treatment strategies for hemodynamically significant hemorrhagic myositis in patients with DM. Three management strategies have been previously described: observation, conservative treatment with transfusions, and arterial embolization. Orrell et al. described two patients treated successfully without procedural intervention, one of whom was observed and the other who was supported with blood transfusions [10]. Three patients underwent arterial embolization, all of whom eventually died. In one patient, arterial embolization initially achieved hemostasis; however, bleeding recurred at the same site 1 week later, and the patient subsequently expired [4]. In one case, interventional radiologists were unable to isolate the source of a patient’s hemorrhage, and the patient died from multiorgan failure [7]. These findings are consistent with the diffuse muscle hemorrhage seen in our patient, which would not have been amenable to treatment with embolization due to lack of a single identifiable bleeding vessel. In non-DM patients, spontaneous hematomas most commonly occur within the rectus sheath or iliopsoas muscle and with use of anticoagulant or antiplatelet therapies [12,13,14]. It is worth noting that the latter occurs due to bleeding from a single blood vessel, in contrast to DM-associated hematomas which occur due to diffuse bleeding from multiple small vessels. As such, non-DM hematomas are typically treated conservatively or, in cases of continued expansion or hemodynamic instability, with catheter embolization of the affected vessel. Risk factors for DM-associated hemorrhagic myositis leading to hematoma remain poorly understood. The use of prophylactic anticoagulation has been linked as an exacerbating factor increasing the risk of bleeding in DM patients, a factor that may have contributed to or exacerbated the rapid evolution of pectoral hematoma in our case [5, 9]. However, at least two patients developed spontaneous hemorrhage without prophylactic anticoagulation [10]. Furthermore, among the eight patients who developed a hematoma after anticoagulation, two had normal activated partial thromboplastin times [4, 6]. Patients with DM may have increased risk of DVT, complicating the decision of whether to initiate anticoagulant or antiplatelet therapy [15]. The inflammatory nature of DM is thought to cause hypercoagulability through alterations to the coagulation cascade, including an imbalance of procoagulants and anticoagulants and suppression of fibrinolysis [16]. Furthermore, DM patients have a number of other risk factors for DVT, including concomitant malignancies and immobilization secondary to disease activity. Despite this increased risk of DVT, DM patients are not routinely maintained on outpatient antiplatelet or anticoagulant therapy, and recent attempts at consensus guidelines for management of DM have yet to address the issue [17]. The case presented herein describes the occurrence of two hematomas in the same patient, one treated by surgical evacuation and the other non-operatively. This case is unique as it is the first report of DM involving the pectoralis major muscle. Diffuse bleeding from many small intramuscular vessels was encountered with pathology showing a chronic myopathic process, consistent with the suspected pathophysiology of DM-associated microangiopathy. The bleeding may have been exacerbated by administration of prophylactic heparin at the time of admission. Weakness in the left thigh has persisted where the hematoma was managed conservatively. Physicians lack specific recommendations regarding management of hemorrhagic myositis in DM patients. We suggest the risk of hemorrhagic myositis be remembered when starting prophylactic anticoagulation. Our case suggests that in addition to aggressive clinical management, operative intervention is warranted when active extravasation is identified. Successful treatment modalities have included conservative therapy with transfusions and surgical evacuation. Although rare, the presence of a spontaneous hematoma should take into consideration the possibility of DM as an underlying cause. Conclusion Spontaneous hemorrhagic myositis in the setting of DM is rare but can be fatal. When admitting patients with DM symptoms, physicians should be cognizant that multiple sites may be involved and should consider the risk of exacerbating hemorrhagic myositis when starting DVT prophylaxis. Embolization as a means of treating diffuse extravasation has not been shown to be effective. More research remains to be done to elucidate the risk factors and pathophysiology of spontaneous hemorrhagic myositis in dermatomyositis. References 1. Bernatsky S, Joseph L, Pineau CA, Belisle P, Boivin JF, Banerjee D, Clarke AE (2009) Estimating the prevalence of polymyositis and dermatomyositis from administrative data: age, sex and regional differences. Ann Rheum Dis 68(7):1192–1196. https://doi.org/10.1136/ard.2008.093161 2. Bendewald MJ, Wetter DA, Li X, Davis MD (2010) Incidence of dermatomyositis and clinically amyopathic dermatomyositis: a population-based study in Olmsted County Minnesota. Arch Dermatol 146(1):26–30. https://doi.org/10.1001/archdermatol.2009.328 3. Krathen MS, Fiorentino D, Werth VP (2008) Dermatomyositis. Curr Dir Autoimmun 10:313–332. https://doi.org/10.1159/000131751 4. Yamagishi M, Tajima S, Suetake A, Kawakami H, Watanabe T, Kuriyama H, Takada T, Suzuki E, Gejyo F (2009) Dermatomyositis with hemorrhagic myositis. Rheumatol Int 29(11):1363–1366. https://doi.org/10.1007/s00296-0080821-3 5. Higashi Y, Mera K, Kanzaki T, Kanekura T (2009) Fatal muscle haemorrhage attributable to heparin administration in a patient with dermatomyositis. Clin Exp Dermatol 34(3):448–449. https://doi.org/10.1111/j.13652230.2008.02952.x 6. Hanawa F, Inozume T, Harada K, Andou N, Kawamura T, Shibagaki N, Shimada S (2013) A case of dermatomyositis accompanied by spontaneous intramuscular hemorrhage despite normal coagulability. Rheumatol Int 33(11):2949 –2950. https://doi.org/10.1007/s00296012-2492-3 7. Van Gelder H, Wu KM, Gharibian N, Patel DB, Clements PJ, Heinze ER, Morris RI, Wong AL (2014) Acute hemorrhagic myositis in inflammatory myopathy and review of the literature. Case Rep Rheumatol 2014:639756. https://doi.org/10.1155/2014/639756 8. Chen YH, Wu PC, Ko PY, Lin YN (2015) Retroperitoneal hematoma mimicking exacerbation of dermatomyositis. Intern Med 54 (8):995–996. https://doi.org/10.2169/internalmedicine.54.3195 9. Langguth DM, Wong RC, Archibald C, Hogan PG (2004) Haemorrhagic myositis associated with prophylactic heparin use in dermatomyositis. Ann Rheum Dis 63 (4):464–465. https://doi.org/10.1136/ard.2003.010272 10. Orrell RW, Johnston HM, Gibson C, Cass RM, Griggs RC (1998) Spontaneous abdominal hematoma in dermatomyositis. Muscle Nerve 21 (12):1800–1803. https://doi.org/10.1002/(sici)1097-4598 (199812)21:12%3c1800:aidmus29%3e3.0.co;2-z 11. Miwa Y, Muramatsu M, Takahashi R, Wakabayashi K, Odai T, Isozaki T, Yajima N, Kasama T (2010) Dermatomyositis complicated with hemorrhagic shock of the iliopsoas muscle on both sides and the thigh muscle. Mod Rheumatol 20(4):420 –422. https://doi.org/10.1007/s10165010-0296-4 12. Touma L, Cohen S, Cassinotto C, Reinhold C, Barkun A, Tran VT, Banon O, Valenti D, Gallix B, Dohan A (2019) Transcatheter arterial embolization of spontaneous soft tissue hematomas: a systematic review. Cardiovasc Interv Radiol 42(3):335–343. https://doi.org/10.1007/s00270-0182086-x 13. Karapolat B, Tasdelen HA, Korkmaz HAA (2019) Conservative treatment of spontaneous rectus sheath hematomas: single center experience and literature review. Emerg Med Int 2019:2406873. https://doi.org/10.1155/2019/2406873 14. Dohan A, Darnige L, Sapoval M, Pellerin O (2015) Spontaneous soft tissue hematomas. Diagn Interv Imaging 96(7–8):789–796. https://doi.org/10.1016/j.diii.2015.03.014 15. Li Y, Wang P, Li L, Wang F, Liu Y (2018) Increased risk of venous thromboembolism associated with polymyositis and dermatomyositis: a meta-analysis. Ther Clin Risk Manag 14:157–165. https://doi.org/10.2147/TCRM.S157085 16. Wagner DD, Burger PC (2003) Platelets in inflammation and thrombosis. Arterioscler Thromb Vasc Biol 23(12):2131–2137. https://doi.org/10.1161/01.ATV.0000095974.95122.EC 17. Kohsaka H, Mimori T, Kanda T, Shimizu J, Sunada Y, Fujimoto M, Kawaguchi Y, Jinnin M, Muro Y, Ishihara S, Tomimitsu H, Ohta A, Sumida T (2019) Treatment consensus for management of polymyositis and dermatomyositis among rheumatologists, neurologists and dermatologists. Mod Rheumatol 29(1):1–19. https://doi.org/10.1080/14397595.2018.1521185 Acknowledgements The authors would like to thank Dr. Matthew Lewis for his review of the manuscript. Funding There was no funding provided for this report. Author information Authors and Affiliations Department of Surgery, Stanford University School of Medicine, 300 Pasteur Drive, Rm H3591, Stanford, CA, 94305, USA Julia M. Chandler & Irene L. Wapnir Stanford University School of Medicine, Stanford, CA, 94305, USA Yoo Jung Kim Department of Radiology, Stanford University School of Medicine, Stanford, CA, 94305, USA Justin L. Bauer Contributions JC conceived the study and drafted and critically revised the manuscript. YK performed the literature search and drafted and critically revised the manuscript. JB critically revised the manuscript and provided guidance on radiologic findings. IW critically revised the manuscript and provided overall guidance for the project. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work. Corresponding author Correspondence to Julia M. Chandler. Ethics declarations Conflict of interest The authors report no conflicts of interest. Informed consent Informed consent was obtained from the patient described in the study, including permission for release of photographs. Additional information Publisher's Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Rights and permissions Reprints and Permissions About this article Cite this article Chandler, J.M., Kim, Y.J., Bauer, J.L. et al. Dilemma in management of hemorrhagic myositis in dermatomyositis. Rheumatol Int 40, 331–336 (2020). https://doi.org/10.1007/s00296-019-04501-7 Received Accepted Published 2019 2019 2019 16 September Issue Date 11 December 23 December Keywords Dermatomyositis complications Hemorrhage Myositis Hematoma Not logged in - 197.60.211.224 Specialized Presidential Council for Educ and Scientific Research Portal (3002076174) Egyptian Knowledge Bank (3000142857) © 2023 Springer Nature Switzerland AG. Part of Springer Nature.