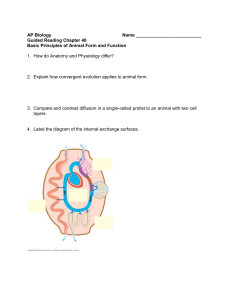
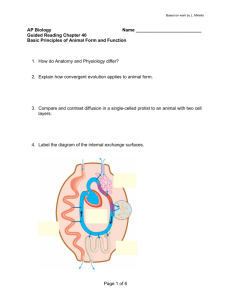
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/342155373 Metabolic Adaptation to Weight Loss: a Brief Review Preprint · June 2020 DOI: 10.13140/RG.2.2.21486.02887 CITATIONS READS 0 1,244 1 author: Mario García Martínez-Gómez Servicio de Salud de Castilla-La Mancha 1 PUBLICATION 0 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Metabolic adaptation to weight loss: a brief review View project All content following this page was uploaded by Mario García Martínez-Gómez on 14 June 2020. The user has requested enhancement of the downloaded file. Bachelor’s Degree Final Project Metabolic Adaptation to Weight Loss: a Brief Review Mario García Martínez-Gómez Abstract: As the scientific literature has continuously shown, weight loss attempts don`t always follow a linear fashion nor always go as expected even when the intervention is calculated with precise tools. One of the main reasons why this tends to happen relies on our body’s biological drive to regain the weight we lose to survive. This phenomenon has been referred to as ‘metabolic adaptation’ many times in the literature and plays a very relevant role in the management of obesity and human body weight. This review will provide insight into some of the theoretical models for the etiology of metabolic adaptation as well as a quick look into the physiological and endocrine mechanisms that underlie it. Nutritional strategies and dietetic tools are thus necessary to confront these so-called adaptations to weight loss. Among some of these strategies we can highlight increasing protein needs, opting for high-fiber foods or programming controlled dietrefeeds, and diet-breaks over a large weight loss phase. Outside the nutritional aspects, it might be wise to increase the physical activity and thus the energy flux of an individual when possible to maintain diet-induced weight loss in the long-term. This review will examine these protocols and their viability in the context of adherence and sustainability for the individual towards successful weight loss. Keywords: diet-reducing; weight loss; caloric restriction; adaptative thermogenesis; appetite control; energy balance; energy expenditure; energy intake; metabolic rate; diet refeeds; diet breaks. 1. Introduction Energy balance could be described as the subtracted difference from the number of calories consumed by an individual through food intake and the energy expended to maintain his metabolic and physiological functions and support physical activity and exercise demands (1). If we conceive the human body as a bioenergetic system, this concept would align with the first law of thermodynamics, which postures that the total energy of a system is constant, where energy can be transformed from one form to another, but cannot be created nor destroyed (2). Thus, modifications over time in energy balance would be the prime determinant of body weight variation in humans (3). Alongside this concept, successful weight loss in an individual can be achieved by creating what is known as a caloric deficit or energy deficit, which broadly speaking, consist in expending more calories or energy than those ingested through food, either by increasing physical activity or decreasing one’s caloric intake (4). Despite the promotion of Metabolic adaptation to weight loss 1 different types of diets for weight loss (5,6), the weekly application of the aforementioned principle (energy deficit) is common amongst all of them and remains the prime determinant factor for bodyweight reduction (7). Nonetheless, this process is not expected to occur linearly (8), since it is well documented that macronutrient distribution can affect the magnitude of losses in the short term (9) and that a series of homeostatic and metabolic adaptations, such as adaptative thermogenesis(10), changes in mitochondrial efficiency (11) or alterations in the levels of circulating hormones occur during periods of energy restriction (12). The severity of these changes will depend on the duration of the dieting period, where longer durations will increase adaptations; the magnitude of the energy deficit; where higher deficits will promote larger homeostatic responses; or previous body composition, where lower body fat levels before the intervention will result in more drastic metabolic adaptations (13,14). It also remains unclearly answered whether certain nutritional interventions can reduce the severity of the adaptations to weight loss since the available evidence is reduced, restricted to specific populations (overweight individuals) and many studies are performed in mice (15,16). Inferring practical applications from this data may be of relevance for both researchers and practitioners to achieve successful weight loss in populations who might struggle at manipulating body weight for various reasons (obese individuals, athletes…). Aim It is thus important to understand: (i) the dynamic nature of energy balance, (ii) how these series of ‘metabolic adaptations’ can affect weight loss and weight regain over time, and (iii) what are the possible nutritional solutions proposed to mitigate these phenomena. These will be the main aims of the present review. 2. Evolutionary origins and models to metabolic adaptation The question still arises as to why our species have been endowed with these modifications to our physiology during periods of energy restriction. Although the answer is still inconclusive and mostly dependant on multiple factors, some hypotheses related to our evolutionary past have been postulated. The ‘Thrifty gene hypothesis’ states that several thousand years back, environmental pressures and natural selection would favor those who were able to survive long periods of famine when food was scarce, and thus are the ones who prevailed and conform our genetic heritage, a heritage that when thrown in our modern ‘obesogenic environment’, lead us to chronic disease (17). In simple words, ‘Our ancient savior has become our modern issue’. While this theory is an oversimplification that takes a determinist standpoint and only provides a causal genetic factor for the development of obesity in our era, it can be used as a conceptual framework to understand why metabolic adaptation occurs and where it could have come from. Another hypothesis that aligns with this last one to explain the issue at hand is the existence of a ‘hypothalamic feeding Metabolic adaptation to weight loss 2 center’, more commonly referred as ‘adipostat’, an axis between all of our organs and our central nervous system that would tightly control food intake in the long term (18,19). This system would receive afferent signals ranging from hormones (leptin, ghrelin, insulin…) to the gut or adipose tissue that would help to establish a ‘set-point’ of energy reserves primarily in the form of adipose tissue and hepatic and muscular glycogen storage thresholds (20,21). This hypothesis has been generally accepted by the scientific community as a theoretical model to understand the selfregulation of food intake but presents several limitations to explain certain diseases like obesity (22). The focus of the theoretical models for food intake regulation, however, hasn’t only been placed on adipose tissue; Millward proposed the existence of a ‘protein-stat’ that would suggest food intake to be regulated through the needs for maintenance of lean mass (23). Nonetheless, the evidence for this mechanism is limited. Regarding adaptative thermogenesis (AT), Keys et al. were the first ones to define this event (24). AT is explained as a spontaneous decrease in energy expenditure (EE) during weight loss, potentially coming from reductions in the metabolic rate of some relevant organs (heart, kidneys, brain, liver) and tissues contained within the fat-free mass (FFM)(25). In one relevant study on this topic (26), it was reported the magnitude of the adaptation to be around 70-100 kcal/day. Although clinically significant, we must take this data with caution, since FFM is widely varied in respect to its composition (27), and adjusting for variables such as the water content of different organs and tissues might affect the previous calculation. Several methodological limitations arise when accounting for the evaluation of AT (28). Inter-individual variability was also observed in the Minnesota experiment (26), where higher baseline EE was associated with higher AT, supporting the notion that the magnitude of weight loss can be proportional to AT. Nonetheless, the energy expenditure component (which will be further explained in better detail) where this reduced EE might come from remains unclear since AT might be coming from the non-resting energy compartment of EE (non-voluntary reductions in EE through decreases in physical activity), as other models have proposed (29). Considering this, whether AT is relevant itself or even actually measurable as part of the metabolic adaptation to weight loss remains disputed (30). 3. Components of energy expenditure As stated before, a sustained energy deficit over time will lead to weight loss, thus it is important to precisely describe where total daily energy expenditure (TDEE) of an individual comes from (31). We can describe at least 2 major components that determine an individual’s TDEE. The first one, resting energy expenditure (REE), refers to the basal metabolic rate (BMR) and will be the largest constituent of TDEE in most cases, with an average contribution of 70% to TDEE (32). This value will depend on many variables such as sex, height, age, physical activity, etc.(33–35) and although mostly constant through and individual’s lifetime, losses or gains in metabolically active tissue such as lean body mass (LBM) can contribute to small, though not significant (25), Metabolic adaptation to weight loss 3 variations in REE (36,37). For research purposes, it should be minded that after approximately two days of fasting, transient increases in this component (5-10%) can be observed due to an increase in gluconeogenesis rate (38). The second component is non-resting energy expenditure (NREE) which is further divided into other 3 minor contributors: exercise activity thermogenesis (EAT), Non-exercise activity thermogenesis (NEAT), and the thermic effect of food (TEF). The latter refers to the energy expended during the digestion of food, and its contribution to TDEE is estimated to be around 10%. However, it should be noted that different macronutrients as well as other variables (size of meals, processing of foods, duration) contribute separately to this effect, where bigger meals and higher carbohydrate and protein content can have a larger impact on TEF (39). This factor might be of consideration when accounting for the TDEE of specific populations, for instance, high-protein diets for some athletes (40). However, some metabolic chamber studies in overweight subjects show that even high protein feedings may not pose a significant difference in TDEE (41), contrary to what could be expected. A commonly held myth regarding TEF is that a higher frequency of meals will result in increased thermogenesis, but research does not support this claim (42). EAT would refer to the energy expended during daily, programmed exercise sessions. This value accounts for little for TDEE (5-10%) and remains unchanged for the most part unless exercise is ceased or the weight of an individual is reduced significantly (43), thus needing less energy to support the locomotion required to perform. NEAT is defined as the energy required to support non-exercise related tasks such as walking and other leisure time activities (44,45). This component has gathered a lot of attention in recent years, due to its large and variable contribution to TDEE. NEAT has also been shown to downregulate during periods of energy restriction (46) and even maintain that state afterward, potentially contributing to weight regain (47). However, a recent review on the topic (48), aimed to examine the response of NEAT to diet interventions to promote weight loss, concluding the majority of evidence, despite having relevant limitations and a high risk of bias, didn’t support a significant reduction in this components. All TDEE contributors are subjected to some degree of both inter and within-individual variability (49), where the largest variations in TDEE are dictated by changes in NEAT. If we were to take NEAT into perspective with the other components, it could represent 15% of TDEE in sedentary subjects up to 50% in more active individuals (44,50). Figure 1 visually summarizes the different components of energy expenditure. Metabolic adaptation to weight loss 4 Components of energy expenditure REE~5-8% TEF~20% EAT~1-4% NEAT~15-50% 100% 90% NEAT~15-50%. 15% 80% EAT~1-4%. 5% TEF~20%. 10% 70% %TDEE 60% 50% 40% 30% REE~5-8% 70% 20% 10% 0% TDEE Figure 1. Components of TDEE and their reported coefficients of variation. Note how daily exercise activity (EAT) is a far-less relevant contributor to TDEE than non-programmed activity (NEAT), despite the common belief. TEF reports a high variability because it might be dependent on the properties of food ingested. Adapted from various sources (13,31,49). 4. Physiological responses to weight loss and endocrine modulation of food intake The energy balance equation remains undisputed for explaining changes in an individual’s body weight. However, a series of physiological and endocrine alterations occur in response to an energy deficit that can drive the behavioral response of an individual regarding appetite, satiety, and food intake, potentially closing the gap between the prescribed energy deficit and the actual caloric intake. Some of the extreme attempts to reduce weight can be observed in sports where body weight or aesthetic appearance is relevant for performance outcomes (combat sports, gymnastics, bodybuilding…). A series of observational and case-report data show many endocrine and hormonal alterations in athletes who undergo these practices (51–53). These endocrine profile changes are generally relegated to increases in orexigenic signals and decreases in anorexigenic pathways to promote food ingestion and restoration of energy homeostasis (31,54). (Figure 2) Metabolic adaptation to weight loss 5 Figure 2. A theoretical framework of metabolic adaptation. Note how increases in hunger and slight reductions in TDEE after long periods of energy restriction exert negative feedback on the initial deficit, attenuating the degree of weight loss. Adapted from Trexler et al. (13) It was with the discovery of leptin (55) and its relation with the fat mass that a possible endocrine role on energy intake was elucidated. We can take leptin, thyroid hormone, insulin, or ghrelin as examples: Post-prandial leptin levels have been shown to vary over the course of weeks depending on adipose stores (56). These variations result in increased satiety after a meal (increased leptin levels/replete adipose stores scenario) or decreased satiety (decreased leptin levels/depleted adipose stores scenario), potentially regulating subsequential food intake beyond the conscious control of an individual (57). Leptin has also been shown to modulate hunger by other means such as inhibiting neuropeptide Y (NPY) and agouti-related protein neurons (AgRP) or stimulating pro-opiomelanocortin neurons in the hypothalamus (58,59). The thyroid gland hormones, particularly T3, are also of relevance when accounting for the energy expenditure of an individual (60). In a cohort of obese children (61), reductions in T3 and T4 levels were observed after weight losses in the long term, with no variation to TSH. It is important to note that the levels of these hormones were altered at baseline among some of the subjects included in the study (two-fold above the standard deviation for their age) and thus it could be debated if restoration of metabolic homeostasis via reductions in excessive fat-mass was attributable for that outcome instead of weight loss per-se. In another study of non-overweight subjects (62), it was reported that those who lost >5% of body weight experimented significant reductions in T3 as well as in the T3: T4 ratio. Thyroid hormone has also been shown to stimulate brown adipose tissue (63), which can make small contributions to energy expenditure (64). Insulin is similar to Metabolic adaptation to weight loss 6 leptin in the sense that both regulate body weight and/or food ingestion via negative feedback (65) and both have been reported to decrease during periods of energy restriction (66). Insulin acts in the brain as a potent anorexigenic hormone signaling ‘energy availability’, whereas peripherally lowers blood glucose levels, driving food intake (67,68). Insulin is also known for its anti-catabolic properties (69). This is relevant because reductions in FFM have also been shown to possess a strong orexigenic effect (70) and are now being considered as a potent tonic appetite signal and a strong driver of food intake after weight loss (71,72). Ghrelin was discovered in 1999 (73) in the stomach, whose main function is to regulate food intake and serve as an orexigenic signal. Ghrelin levels have been shown to increase after diet-induced weight loss (74) as well as upregulate during energy restriction (75). It is thus commonly stated that these transient orexigenic signals in response to weight loss can drive food consumption and increase appetite (76). Contrary to leptin, increases in ghrelin production underlie rises in AgRP and NPY neuropeptides, contributing to its orexigenic effect (77). Regarding ghrelin, this study (78) reported how the response in circulating levels of ghrelin to meals with different calories wasn´t equal between obese and lean subjects. Whereas ghrelin levels decreased after high-calorie meals in the lean group and responsively increased after low-calorie meals (as expected), obese subjects experimented no significant variation at all (78). This finding highlights how persistent endocrine alterations (obesity, in this case) can influence the outcomes of studies examining metabolic adaptation (79). Mechanisms for both leptin and ghrelin resistance in obesity have been reported elsewhere (80,81). Multiple additional alterations can be observed in the endocrine profile of other hormones related to appetite and satiety such as gastric-inhibitory polypeptide (GIP) (54) or amylin (54,82) with weight loss. Peptide YY (PYY) and cholecystokinin (CKK) are gastrointestinal (GI) peptides that can have an anorexigenic role regarding appetite (83).Their production is sensitive to size, caloric content, and macronutrient composition of meals (84). Intervention studies in obese humans report reductions in their respective circulating levels after a weight loss intervention (85–87), suggesting the notion that these hormones might play a role in weight regain. Glucagon-like peptide 1 (GLP-1) is secreted in the small intestine in response to a nutrient load and has direct implications in the regulation of appetite (88). In one study by De Luis et al. (89) who aimed to examine the effect of weight loss on GLP-1 levels, a positive relationship between the degree of weight loss and reductions in GLP-1 was observed. In a different study (90), similar results were observed, where GLP-1 levels decreased after weight loss compared to baseline. To sum up the information displayed in this section; evidence has been presented to suggest that reductions in the circulating levels of hormones who might possess an anorexigenic effect and increments in the ones whose role is mostly orexigenic have been reported in weight loss intervention trials, both in the short-term and the long-term. This might be reflective of the body’s attempt to restore energy homeostasis. We must not forget that the sample of the studies available is not always representative of the general population, let it be the clinically Metabolic adaptation to weight loss 7 obese or athletes. Thus, effect size and significance cannot be always reliably assessed. The psychological, behavioral, and environmental aspects regarding weight loss and metabolic adaptation are out of the scope of this review, however, a proper understanding and management of these variables is of high relevance (91–93) to achieve successful weight loss. Figure 3 visually presents an integrative model of the endocrine regulation of appetite and the feedback regulatory mechanisms that play a role in the dynamic nature of energy balance. Figure 3. Schematic representation of the endocrine control of energy balance. TDEE: total daily energy expenditure; EAT: exercise-activity thermogenesis; REE/BMR: Resting energy expenditure/basal metabolic rate; NEAT: non-exercise activity thermogenesis; TEF: Thermic effect of food; FM: fat mass; FFM: fat-free mass; CCK: cholecystokinin; PYY; peptide YY; GLP-1: glucagon-like peptide 1. Adapted from various sources (31,72,94–96). 5. Nutritional strategies to reduce metabolic adaptation to weight loss. In order to determine the most adequate nutritional interventions to reduce the deleterious effects of metabolic adaptation to weight loss we must target the main issues responsible for this phenomenon, which are increased hunger coupled with decreased energy expenditure (13,94,97). Figure 4 summarizes the ‘energy gap concept’, which explains why hunger and energy expenditure are the key drivers to design interventions to reduce metabolic adaptation to weight loss. Higher protein diets, fiber, and intermittent energy restriction protocols (diet refeeds & breaks) have been proposed as nutritional strategies to have either direct or a non-direct effect on sustained and successful weight loss. Other factors such as increasing physical activity to maintain diet-induced weight loss are of utmost importance to reduce our body’s compensatory responses (98), though this review will focus on the dietetic interventions. Metabolic adaptation to weight loss 8 Protein One of the main contributors to the increase in appetite and hunger during energy restriction is FFM tissue losses, which increases central signaling for food intake (70). Protein is the most important macronutrient when accounting for the maintenance of FFM and overall health during lifespan (99,100) and our optimal needs might be increased during periods of dietary restriction (101,102). To either maintain or increase lean body mass (a component of FFM) the rates of muscle protein synthesis (MPS) must exceed muscle protein breakdown (MPB) rates (103). A deeper understanding of protein turnover is out of the scope of this review; the reader is redirected to other reviews on the topic (104,105). Given the fact that protein might possess a satiating effect (106,107) and has a higher thermic effect after consumption (108), theory supports increasing protein intake over usual consumption patterns to mitigate potential increases in hunger and appetite. In this trial with a randomized parallel design (109) in obese subjects who lost 5-10% of their total body weight in three months, those who consumed 48g of protein over their usual intake regained less weight after the follow-up and mainly in the form of FFM. In another study (110), adding 30g/day of protein to the diet during 7 months resulted in less body weight regained in overweight subjects. To the author’s criteria, both these studies were well conducted and showed no important limitations, however, is it important to note the studies were carried out by the same research group and although the results may be extrapolated with ease, further replication of the findings is warranted. In the DIOGENES study (111), a randomized controlled trial performed in Europe with obese and overweight subjects on ad libitum diets, it was reported that after the initial weight loss, those who consumed a higher amount of protein regained significantly less weight than those with a lower intake. These results add up to the idea that increased protein might promote satiety and better weight loss outcomes than a usual intake (112). Several meta-analyses involving overweight and obese individuals suggest that 1.2–1.5 g/kg is an appropriate daily protein intake range to maximize fat loss (113–115). It should be reminded that, alongside protein, exercise plays a relevant role in the maintenance of FFM and the maintenance of energy expenditure during weight loss. In a randomized controlled trial by Verreijen et al. (116) 100 overweight subjects on hypocaloric conditions underwent either a 10-week program with a high protein (1,3g/kg) or a low protein diet (0,8g/kg) with or without resistance-type exercise. The results show how only the group with the combined intervention (high protein & resistance exercise) preserved a significant amount of FFM. Following this idea, a recent meta-analysis (117) aimed to determine the effect of different types of exercise on energy expenditure, concluding that resistance exercise was slightly superior than endurance and aerobic exercise in increasing energy expenditure. It would also appear that in athletic populations, where the FFM component is generally larger than that of overweight and sedentary individuals, protein needs during weight loss might be even higher and of more relevance (118,119) ranging from 1,2g/Kg Metabolic adaptation to weight loss 9 to 2g/kg of body weight. Mettler et al. (120) found a better retention of lean body mass (skeletal muscle component of FFM) in individuals who consumed 2,3g of protein/kg/day versus those who consumed 1g/kg/day during a weight loss protocol. Intakes up to 3,4-4,4g/kg have been studied before in this population (121–123) with no deleterious health effects and improvements in body composition reported. However, in the author’s view, such high intakes shouldn’t be generally recommended since food choices to meet those goals may become unsustainable and adherence will be compromised. For a more personalized approach, it might be wise to estimate optimal protein needs based on FFM or lean body mass (124–126) instead of total body weight, since adipose tissue demands for protein are lower than those of FFM (127). To conclude, increasing protein intake over usual values might be wise to offset the negatives of dieting over long periods of time. It is important to understand that recommended dietary allowances (RDA) establish a minimum, not an optimal intake (128) and thus shouldn`t be taken as a one-size-fitsall recommendation, especially during a caloric deficit. Combining high protein intakes with a prescribed resistance exercise program appears to be a more interesting intervention to avoid FFM losses than protein alone (129), and the negative consequences of metabolic adaptation overall. Fiber The idea that dietary fiber might help control appetite is still controversial. As a public health strategy, it is indicated to increase fiber intake (130), since requirements are generally not met. Evidence from epidemiological studies reports higher fiber intakes to be associated with improved weight control, higher satiety, and overall lower food intake (131–133). High-fiber foods generally possess a higher satiety index (134). Possible explanatory mechanisms to this relation might reside in longer chewing periods to consume high fiber foods as well as its low energy density (2kcal/g) (135,136). A review with meta-analysis (137) who examined the relation between acute satiety and consumption of fiber, found no clear relationship between these two variables in interventional studies. However, there is tremendous variability in the design and methodology of fiber trials, where different types of fiber may yield different outcomes (138). High fiber meals can also modulate postprandial concentrations of anorexigenic gastrointestinal peptides like GLP-1 and PYY (139) thus contributing to increased satiety after a meal. Gastric emptying rate (GER) is also affected by fiber ingestion as demonstrated by Geliebter et al. (140). In their study it was reported how oatmeal significantly lowered GER compared to corn flakes (less fiber than oatmeal) and contributed to greater satiety after the meal. Different and varied fiber consumption might also contribute to a remodeling of the gut microbiota (141,142) which present numerous implications in the regulation of food intake and overall health, yet further investigation is needed about it at the moment. Overall, research on the satiating effects of fiber has been reported to present numerous methodological limitations and a lack of external validity (143). Randomized trials with subjects on hypocaloric conditions, with high fiber intakes through Metabolic adaptation to weight loss 10 a whole-food approach are lacking. Thereby, designing and approach towards increasing fiber in order to attenuate the effects of metabolic adaptation is complex. Since high-fiber intakes have been reported to reduce the energy density of the diet (144) as well as allowing for larger volumes of food without drastically increasing calories (145), fiber could be a useful dietetic tool to attain an energy deficit. Diet refeeds and diet breaks The current US and European (146,147) guidelines recommend continuous energy restriction (CER) as an effective tool to lose weight. On the other hand, intermittent energy restriction (IER) includes a series of nutritional protocols that differ from the traditional approach of dieting in a CER (14), in the sense that they alternate periods of overfeeding with periods of undereating, which still follow the principles of energy balance (1). The most common IER protocols used are diet breaks and refeeds. Diet refeeds could be defined as a specific dietetic strategy where calories and macronutrients are increased at energy maintenance levels or slightly above on specific days (1-2 days) over the course of a weekly deficit, predominantly achieved by increasing carbohydrate consumption (13,148). There are several hypotheses to why increasing carbohydrate periodically could lead to improved weight loss outcomes and better FFM retention; Firstly, since circulating insulin levels have a role in the maintenance of FFM (69) responses in secretion to acute carbohydrate refeeds could help reduce muscle protein breakdown (149,150) as well promote a more pronounced muscle protein synthesis response through the activation of the mTORC1 pathway (151). Secondly, leptin has been demonstrated to be especially responsive to carbohydrate intake(152). To test if overfeeding alone was solely responsible for the rise in leptin, this study (153) on lean healthy female subjects, aimed to compare fat versus carbohydrate refeeds. Plasma leptin levels were elevated after a carbohydrate overfeed but not a fat overfeed, suggesting carbohydrate to have a major impact on leptin levels. Overweight and obese subjects may benefit from this strategy since a series of hormonal alterations like leptin resistance have been reported in this population (154). In this study (155), obese and overweight subjects were randomly allocated in either an IER restriction group with refeeding every 5 days, a CER group, or a control group with no advice to restrict calories for 1 year. No significant differences were observed between the ICR and CER group in regards to weight loss and multiple other biomarkers, concluding that both protocols were equally effective in weight reduction and disease prevention(155). In another trial on obese and overweight subjects (156) similar results were observed, however, reported feelings of hunger were more common among the IER group after 1 year. One key aspect to consider when evaluating different dietary protocols is reported adherence (157,158). In both studies, the drop-out rate from the participants was reported to be less than 10%, suggesting adherence to IER is similar to CER. Lastly, athletes might benefit more from intermittent refeeds than overweight subjects as this population has reported favorable results Metabolic adaptation to weight loss 11 following this protocol (159). This might be due to carbohydrate being pertinent for sports performance outcomes (160,161). Though not all kinds of sports may require high amounts of carbohydrate to improve performance (162,163), they are undoubtedly needed for high-intensity efforts (164,165). In a very recent study by Campbell et al. (166), resistance-trained subjects followed either a 21% CER or a 26% IER for 7 weeks. Results showed similar reductions in body weight but higher retention in FFM on the IER group. There are, nonetheless, several methodological considerations to address when inferring conclusions from the evidence presented. Adherence was low (27 participants completed the trial from the 58 that were instructed at baseline), the caloric restriction was different between groups (21% vs 26%) and results were highly heterogeneous, with subjects losing 3,5Kg of FFM and others gaining 2,5Kg within the IER group (potentially due to the body assessment methods used). These variables alone might shift the results of this study towards the null, thus conclusions should be interpreted cautiously. Diet breaks are similar to refeeds, but differ in the amount of time where energy balance conditions are met (from 1-2 days up to weeks). Since metabolic adaptations have been shown to persist even after years after initial weight loss (54), diet breaks are used on the premise that compensatory responses to weight loss require longer periods in energy balance conditions to partially or completely return to baseline (167,168). However, evidence for diet breaks is also mixed: In the MATADOR study (169), 51 obese subjects followed a CER or an IER alternating weeks of energy balance (14 weeks) with periods of energy restriction (16 weeks) during a total 30 weeks. The results reported greater weight loss among the participants of the IER compared to the CER group, as other studies have also replicated (170). In contrast, another study (171) found no difference between diet break protocols over a traditional caloric restriction after 14 weeks. An important consideration to mind about the methodology of the previous study is that the CER group performed a 2-week break (wasn’t strictly continuous) whereas the IER followed a 6-week diet break. Since it is not well understood how much time of a break is needed to revert the compensatory adaptations to weight loss, this factor could have played in favor of the CER group, thus resembling the outcome. To forge a more solid answer to the question, two recent meta-analysis (172,173) compared the effects IER to CER regarding weight loss outcomes, concluding that there was no significant difference between both protocols. It was also reported how the number of studies included was small and presented huge heterogeneity. Besides, most of them were at an unclear risk of bias. Metabolic adaptation to weight loss 12 Figure 4. Visual representation of the energy gap concept. Lowering hunger and increasing energy expenditure potentially narrows the difference between what’s ingested and what’s expended, thus reducing the relative magnitude of the energy deficit, ensuring less metabolic adaptation overall while still losing weight. Taken from Melby et al. (97). Discussion, practical applications, and concluding remarks. The postulation of energy balance is a mathematically and scientifically objective concept to explain changes in human body weight but sometimes incomplete to accurately measure human energy intake and behavior towards food. Models such as the ‘thrifty gene hypothesis’, the ‘adipostat’ or changes in expenditure compartments during weight loss referred to as ‘adaptative thermogenesis’ aim to explain those inaccuracies, but all present their respective limitations. Changes in energy expenditure during weight loss indeed occur but are largely explained by involuntary changes in the non-exercise activity compartment (NEAT). Alongside changes in energy expenditure, endocrine and physiological alterations underlying the modulation of appetite during weight loss comprise reductions in leptin, insulin or FFM, and increases of ghrelin and gastric orexigenic peptides among many, which represents our organism’s homeostatic drive to restore balance. Athletes and overweight subjects have shown to respond differently to weight loss protocols. Where obese subjects might present previous alterations related to energy homeostasis, leaner athletes usually don’t and thus, slightly different nutritional approaches should be taken. For example, the higher the previous level of body fat is, the bigger the energy deficit can be without implying drastic homeostatic adaptations (96), which is the case for obese subjects. Whereas in lean individuals, faster rates of weight loss are both associated with larger FFM losses (174) and with an increased risk of fat regain (175,176). Another potential difference between these two population groups is exercise, since a lack of it, especially resistance-type exercise, during weight loss results in more pronounced FFM losses (116,177). In regards to preserving FFM and avoiding negative consequences, high-protein diets ranging from 1,21,5g/Kg in overweight individuals, and up to 2g/kg in leaner ones, have been presented as effective and secure solutions to aid in the reduction of metabolic adaptation and weight loss. High fiber foods such as whole grains, fruits, and vegetables are also recommended due to their ability to generate early satiation and allow for large volumes of food to be consumed while maintaining an individual on an energy deficit, though more experimental evidence is needed in Metabolic adaptation to weight loss 13 ad-libitum conditions (143). Concerning diet refeeds and diet breaks, the evidence is mixed and scarce. However, some positive results for IER have been reported in certain scenarios (166,169) where both athletes and overweight subjects might benefit from it as a part of a periodized weight loss program. The disparity of refeeding and diet break protocols used in interventions makes it harder to establish the superiority of one intervention to the other. However, ensuring proper adherence, prioritizing carbohydrate over any other macronutrient on refeed days, and establishing an adequate refeed duration are likely the key factors to consider when implementing these strategies, yet their direct usefulness as a tool to minimize unwanted compensatory adaptations to weight loss is still unknown. Non-dietary interventions such as increasing physical activity energy expenditure and engaging in programmed resistance-training are also advised to be combined with the aforementioned to further minimize the deleterious effects of metabolic adaptation to weight loss. As a final remark, the strength and magnitude of the compensatory responses to dieting appears to be of relevance, at best, in most subjects. Even so and with all the characterized adaptations that have been described in this review, high individual variability is observed in studies targeting metabolic adaptation. This might be due to many of the studies on this topic adopting a biological reductionism perspective. The big picture of metabolic adaptation engulfs behavioral and psychological aspects related to the subjects many trials fail to properly address. The accountability of these variables might grant a more solid view of the problem and therefore its solution. Thus, a proper acknowledgment of the context of the subject, both overweight and lean, followed by personalized nutritional and exercise advice is the key to consequently choosing the best possible approach to achieve successful weight loss avoiding the potential drawbacks associated with it. References 4. Bowden RG, Schwarz NA, Rigby BR, La Bounty P, Shelmadine B. A review of 1. Hall KD, Heymsfield SB, Kemnitz JW, weight control strategies and their effects on Klein S, Schoeller DA, Speakman JR. the regulation of hormonal balance. J Nutr Energy balance and its components: Metab. 2011;2011. Implications for body weight regulation. Am J Clin Nutr. 2012;95(4):989–94. 5. Malik VS, Hu FB. Popular weight-loss diets: From evidence to practice. Nature Clinical 2. Zohuri B, Mcdaniel P. First Law of Practice Cardiovascular Medicine. 2007. Thermodynamics. In 2015. p. 99–149. 6. 3. Hall KD. Predicting metabolic adaptation, Freire R. Scientific evidence of diets for weight loss: Different macronutrient body weight change, and energy intake in composition, intermittent fasting, and humans. Am J Physiol - Endocrinol Metab. popular diets. Nutrition. 2020; 2010;298(3). 7. Metabolic adaptation to weight loss Strasser B, Spreitzer A, Haber P. Fat loss 14 depends on energy deficit only, independently of the method for weight loss. Ann Nutr Metab. 2007;51(5):428–32. 8. PLoS One. 2011; 17. genetic basis of human obesity. Ann Surg. Hopkins M, Blundell JE. Energy balance, body composition, sedentariness and appetite regulation: Pathways to obesity. 2014;259(4):642–8. 18. 11. hypothalamic paraventricular nucleus: T. Effect of Macronutrient Composition on Evidence of a cellular basis for the adipostat. Short-Term Food Intake and Weight Loss. Neuron. 1999; thermogenesis in humans. Int J Obes. al. Obesity pathogenesis: An endocrine 2010;34(0 1):S47–55. society scientific statement. Endocr Rev. 2017; Bevilacqua L, Ramsey JJ, Hagopian K, 20. hypothalamic control of food intake in the muscle mitochondrial proton leak and rat. Proc R Soc London Ser B, Biol Sci. reactive oxygen species production. Am J 1953; 21. Brzozowki T. Brain-gut axis and its role in Trindade MRM, Friedman R, Leitão CB. the control of food intake. Journal of Determinants of body weight regulation in Physiology and Pharmacology. 2004. 22. Cannon B, Nedergaard J. Thermogenesis challenges the adipostat hypothesis for body- Trexler ET, Smith-Ryan AE, Norton LE. weight control. Proc Nutr Soc. Metabolic adaptation to weight loss: 2009;68(4):401–7. Implications for the athlete. J Int Soc Sports Nutr. 2014;11(1):1–7. 23. Considerations for the Athlete. Sports. the Lean Body Mass. Nutr Res Rev. 1995; 24. BJ. Hepatic adaptations to maintain of Human Starvation. Am J Psychol. 1951; 25. in Clinical Nutrition and Metabolic Care. and refeeding in mice. Nutr Metab. 2016; weight, body fat, energy expenditure and metabolic fuel selection in C57BL/6 mice. Metabolic adaptation to weight loss McClave SA, Snider HL. Dissecting the energy needs of the body. Current Opinion metabolic homeostasis in response to fasting Guo J, Hall KD. Predicting changes of body Fuhrman FA, B. M, Keys A, Brozek J, Henschel A, Mickelsen O, et al. The Biology 2019;7(1):22. Geisler CE, Hepler C, Higgins MR, Renquist Millward DJ. A Protein-Stat Mechanism for Regulation of Growth and Maintenance of Peos J, Norton L, Helms E, Galpin A, Fournier P. Intermittent Dieting: Theoretical 16. Konturek SJ, Konturek JW, Pawlik T, Moehlecke M, Canani LH, e Silva LOJ, 2016;60(2):152–62. 15. KENNEDY GC. The role of depot fat in the and medium-term calorie restriction on humans. Arch Endocrinol Metab. 14. Schwartz MW, Seeley RJ, Zeltser LM, Drewnowski A, Ravussin E, Redman LM, et Physiol - Endocrinol Metab. 2004; 13. 19. Rosenbaum M, Leibel RL. Adaptive Weindruch R, Harper ME. Effects of short- 12. npy, agrp, and melanocortin signals in the Intake SF, Loss W, Bellissimo N, Akhavan 2015; 10. Cowley MA, Pronchuk N, Fan W, Dinulescu DM, Colmers WF, Cone RD. Integration of Clin Sci. 2016;130(18):1615–28. 9. O’Rourke RW. Metabolic thrift and the 2001. 26. Müller MJ, Enderle J, Pourhassan M, Braun W, Eggeling B, Lagerpusch M, et al. Metabolic adaptation to caloric restriction 15 and subsequent refeeding: The Minnesota 27. Changes in Energy Expenditure with Weight Nutr. 2015; Gain and Weight Loss in Humans. Curr Obes Rep. 2016;5(4):413–23. Toomey CM, Cremona A, Hughes K, 38. Splanchnic metabolism of amino acids in of health. Topics in Clinical Nutrition. 2015. healthy subjects: Effect of 60 hours of fasting. Metabolism. 1988; Browning MG. Methodologic considerations 39. Burgess NN, Flores RA, Busta ML, et al. 2016. The Thermic Effect of Food: A Review. J Am Coll Nutr. 2019;38(6):547–51. Rosenbaum M, Leibel RL. Models of energy 40. M. Protein, weight management, and satiety. Dulloo AG, Jacquet J, Montani JP, Schutz In: American Journal of Clinical Nutrition. Y. Adaptive thermogenesis in human body 2008. weight regulation: More of a concept than a measurable entity? Obes Rev. 2012; 41. of protein overfeeding on energy expenditure measured in a metabolic The impetus for weight regain. Am J Physiol chamber. Am J Clin Nutr. 2015; - Regul Integr Comp Physiol. 2011;301(3). Levine JA. Measurement of energy 42. International Society of Sports Nutrition Curtis V, Henry CJK, Birch E, Ghusain‐ position stand: Meal frequency. J Int Soc Choueiri A. Intraindividual variation in the Sports Nutr. 2011;8:1–12. basal metabolic rate of women: Effect of the menstrual cycle. Am J Hum Biol. 1996; 34. 43. N, Mauriège P, Després JP, et al. Greater than predicted decrease in energy KR. Intra-individual variation of basal expenditure during exercise after body metabolic rate and the influence of daily weight loss in obese men. Clin Sci. 2003; 44. Nutr. 2003; 36. Doucet E, Imbeault P, St-Pierre S, Alméras Adriaens MPE, Schoffelen PFM, Westerterp habitual physical activity before testing. Br J 35. La Bounty PM, Campbell BI, Wilson J, Galvan E, Berardi J, Kleiner SM, et al. expenditure. Public Health Nutr. 2005; 33. Bray GA, Redman LM, De Jonge L, Covington J, Rood J, Brock C, et al. Effect MacLean PS, Bergouignan A, Cornier MA, Jackman MR. Biology’s response to dieting: 32. Paddon-Jones D, Westman E, Mattes RD, Wolfe RR, Astrup A, Westerterp-Plantenga reduced body weight. Obesity. 2016; 31. Calcagno M, Kahleova H, Alwarith J, American Journal of Clinical Nutrition. homeostasis in response to maintenance of 30. Siw Eriksson L, Olsson M, Björkman O. composition measurement in the assessment in the evaluation of adaptive thermogenesis. 29. Müller MJ, Enderle J, Bosy-Westphal A. Starvation Experiment revisited. Am J Clin Norton C, Jakeman P. A review of body 28. 37. Levine JA, Vander Weg MW, Hill JO, Klesges RC. Non-exercise activity Henry CJK. Mechanisms of changes in basal thermogenesis: The crouching tiger hidden metabolism during ageing. Eur J Clin Nutr. dragon of societal weight gain. Arterioscler 2000; Thromb Vasc Biol. 2006;26(4):729–36. Leibel RL, Rosenbaum M, Hirsch J. 45. Chung N, Park M-Y, Kim J, Park H-Y, Changes in energy expenditure resulting Hwang H, Lee C-H, et al. Non-exercise from altered body weight. N Engl J Med. activity thermogenesis (NEAT): a 1995; component of total daily energy expenditure. Metabolic adaptation to weight loss 16 J Exerc Nutr Biochem. 2018; 46. 54. Purcell K, Shulkes A, Kriketos A, et al. Levine JA. Non-exercise activity Long-term persistence of hormonal thermogenesis (NEAT). Best Pract Res Clin adaptations to weight loss. N Engl J Med. Endocrinol Metab. 2002 Dec;16(4):679–702. 47. Weyer C, Walford RL, Harper IT, Milner M, MacCallum T, Tataranni PA, et al. Energy 2011; 55. of the mouse obese gene and its human The Biosphere 2 experiment. Am J Clin homologue. Nature. 1994; Nutr. 2000; Silva AM, Júdice PB, Carraça E V., King N, 56. physical activity and related energy and interactions. International Journal of expenditure of free-living adults? A Obesity. 2002. 58. Ahima RS, Bjorbæk C, et al. Leptin differentially regulates NPY and POMC Variability in energy expenditure and its neurons projecting to the lateral components. Current Opinion in Clinical hypothalamic area. Neuron. 1999; 59. Cerdán MG, Diano S, Horvath TL, et al. of nonexercise activity thermogenesis in Leptin activates anorexigenic POMC resistance to fat gain in humans. Science neurons through a neural network in the (80- ). 1999; arcuate nucleus. Nature. 2001; Hulmi JJ, Isola V, Suonpää M, Järvinen NJ, 60. Kim B. Thyroid hormone as a determinant Kokkonen M, Wennerström A, et al. The of energy expenditure and the basal effects of intensive weight reduction on metabolic rate. Thyroid. 2008. female fitness competitors. Front Physiol. 61. Pardue A, Trexler ET, Sprod LK. Case study: Unfavorable but transient Dis Child. 2002; 62. Moderate weight loss is sufficient to affect preparation in a drug-free male bodybuilder. thyroid hormone homeostasis and inhibit its Int J Sport Nutr Exerc Metab. 2017; Loenneke JP, Stout JR. Natural bodybuilding competition preparation and recovery: A 12-month case study. Int J Sports Physiol Perform. 2013; Metabolic adaptation to weight loss Agnihothri R V., Courville AB, Linderman JD, Smith S, Brychta R, Remaley A, et al. physiological changes during contest Rossow LM, Fukuda DH, Fahs CA, Reinehr T, Andler W. Thyroid hormones before and after weight loss in obesity. Arch 2017; 53. Cowley MA, Smart JL, Rubinstein M, Levine JA, Eberhardt NL, Jensen MD. Role body composition and serum hormones in 52. Elias CF, Aschkenasi C, Lee C, Kelly J, Donahoo WT, Levine JA, Melanson EL. Nutrition and Metabolic Care. 2004. 51. Margetic S, Gazzola C, Pegg GG, Hill RA. Leptin: A review of its peripheral actions 2018;119(12):1327–45. 50. 57. behavioural compensation in non-exercise systematic review. Br J Nutr. 49. Friedman JM. Leptin and the endocrine control of energy balance. Nat Metab. 2019; Teixeira PJ, Sardinha LB. What is the effect of diet and/or exercise interventions on Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloning metabolism after 2 y of energy restriction: 48. Sumithran P, Prendergast LA, Delbridge E, peripheral conversion. Thyroid. 2014; 63. Broeders EPM, Vijgen GHEJ, Havekes B, Bouvy ND, Mottaghy FM, Kars M, et al. Thyroid Hormone Activates Brown Adipose Tissue and Increases Non-Shivering 17 64. 65. Thermogenesis - A Cohort Study in a Group advances and practical implications. Expert of Thyroid Carcinoma Patients. PLoS One. Rev Endocrinol Metab 2017;12(6):401–15. 2016; 3 Cannon B, Nedergaard J. Brown Adipose Matsuo H, Kangawa K. Ghrelin is a growth- Significance. Physiological Reviews. 2004. hormone-releasing acylated peptide from stomach. Nature. 1999; Cummings DE, Overduin J, Foster-Schubert 74. Breen PA, Ma MK, Patchen Dellinger E, et in Endocrinology and Diabetes. 2005. al. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Mars M, De Graaf C, De Groot LCPGM, insulin concentrations after acute energy 68. Engl J Med. 2002; 75. regulates ghrelin function on energy food intake. Am J Clin Nutr. 2005; homeostasis. Neuroendocrinology. 2011; Lenard NR, Berthoud HR. Central and 76. Frost GS, Murphy KG, et al. Ghrelin physical activity: Pathways and genes. enhances appetite and increases food intake Obesity. 2008; in humans. J Clin Endocrinol Metab. 2001; Austin J, Marks D. Hormonal Regulators of 77. UCP2 mediates ghrelin’s action on Rooyackers OE, Nair KS. HORMONAL 1997; NPY/AgRP neurons by lowering free radicals. Nature. 2008; 78. Postprandial plasma ghrelin is suppressed Collateral fattening in body composition proportional to meal calorie content in autoregulation: Its determinants and normal-weight but not obese subjects. J Clin significance for obesity predisposition. In: Endocrinol Metab. 2005; European Journal of Clinical Nutrition. 79. narrative review. Clin Obes. 2017; Hopkins M, Naslund E, King N, et al. Role 72. Poddar M, Chetty Y, Chetty VT. How does obesity affect the endocrine system? A Blundell JE, Caudwell P, Gibbons C, of resting metabolic rate and energy Le Roux CW, Patterson M, Vincent RP, Hunt C, Ghatei MA, Bloom SR. Dulloo AG, Miles-Chan JL, Schutz Y. 2018. Andrews ZB, Liu ZW, Walllingford N, Erion DM, Borok E, Friedman JM, et al. PROTEIN METABOLISM. Annu Rev Nutr. 71. Wren AM, Seal LJ, Cohen MA, Brynes AE, peripheral regulation of food intake and REGULATION OF HUMAN MUSCLE 70. Briggs DI, Andrews ZB. Metabolic status restriction and subsequent compensation in Appetite. Int J Pediatr Endocrinol. 2009; 69. Cummings DE, Weigle DS, Scott Frayo R, appetite and body weight. Current Opinion Kok FJ. Decreases in fasting leptin and 67. Kojima M, Hosoda H, Date Y, Nakazato M, Tissue: Function and Physiological KE. Roles for ghrelin in the regulation of 66. 73. 80. Cui H, López M, Rahmouni K. The cellular expenditure in hunger and appetite control: and molecular bases of leptin and ghrelin A new formulation. DMM Disease Models resistance in obesity. Nature Reviews and Mechanisms. 2012. Endocrinology. 2017. Hopkins M, Beaulieu K, Myers A, Gibbons 81. Crujeiras AB, Goyenechea E, Abete I, Lage C, Blundell JE. Mechanisms responsible for M, Carreira MC, Martínez JA, et al. Weight homeostatic appetite control: theoretical regain after a diet-induced loss is predicted Metabolic adaptation to weight loss 18 by higher baseline leptin and lower ghrelin 82. 91. plasma levels. J Clin Endocrinol Metab. RM, Gorin AA, Powell-Wiley TM, et al. 2010; Accumulating Data to Optimally Predict Obesity Treatment (ADOPT) Core Reinehr T, De Sousa G, Niklowitz P, Roth Measures: Environmental Domain. Obesity. CL. Amylin and its relation to insulin and 2018; lipids in obese children before and after weight loss. Obesity. 2007; 83. 92. Accumulating Data to Optimally Predict Obesity Treatment (ADOPT) Core Clinical Endocrinology and Metabolism. Measures: Psychosocial Domain. Obesity. 2008. Spiller RC, Trotman IF, Higgins BE, Ghatei MA, Grimble GK, Lee YC, et al. The ileal 2018; 93. Accumulating Data to Optimally Predict ileal fat perfusion in man. Gut. 1984; Obesity Treatment (ADOPT) Core Essah PA, Levy JR, Sistrun SN, Kelly SM, Measures: Behavioral Domain. Obesity. Nestler JE. Effect of weight loss by a low-fat 2018; diet and a low-carbohydrate diet on peptide 94. YY levels. Int J Obes. 2010; 86. Lytle LA, Nicastro HL, Roberts SB, Evans M, Jakicic JM, Laposky AD, et al. brake - inhibition of jejunal motility after 85. Sutin AR, Boutelle K, Czajkowski SM, Epel ES, Green PA, Hunter CM, et al. Woods SC, D’Alessio DA. Central control of body weight and appetite. Journal of 84. Saelens BE, Arteaga SS, Berrigan D, Ballard Casanova N, Beaulieu K, Finlayson G, Hopkins M. Metabolic adaptations during Chearskul S, Delbridge E, Shulkes A, negative energy balance and their potential Proietto J, Kriketos A. Effect of weight loss impact on appetite and food intake and ketosis on postprandial cholecystokinin Conference on ‘ Getting energy balance and free fatty acid concentrations. Am J Clin right ’ Symposium 1 : Regulation of energy Nutr. 2008; balance and whole body metabolism Metabolic adaptations during ne. 87. Pfluger PT, Kampe J, Castaneda TR, Vahl T, 2019;(February). D’Alessio DA, Kruthaupt T, et al. Effect of human body weight changes on circulating 88. 95. MacLean PS, Blundell JE, Mennella JA, levels of peptide YY and peptide YY3-36. J Batterham RL. Biological control of Clin Endocrinol Metab. 2007; appetite: A daunting complexity. Obesity. 2017; Shah M, Vella A. Effects of GLP-1 on appetite and weight. Reviews in Endocrine 96. Greenway FL. Physiological adaptations to weight loss and factors favouring weight and Metabolic Disorders. 2014. regain. Int J Obes [Internet]. 89. De Luis DA, Gonzalez Sagrado M, Conde 2015;39(8):1188–96. Available from: R, Aller R, Izaola O. Decreased basal levels http://dx.doi.org/10.1038/ijo.2015.59 of glucagon-like peptide-1 after weight loss in obese subjects. Ann Nutr Metab. 2007; 97. Melby CL, Paris HL, Foright RM, Peth J. Attenuating the biologic drive for weight 90. Adam TCM, Jochan J, Westerterp-Plantenga MS. Decreased glucagon-like peptide 1 release after weight loss in overweight/obese regain following weight loss: Must what goes down always go back up? Nutrients. 2017;9(5). subjects. Obes Res. 2005; Metabolic adaptation to weight loss 19 98. 99. 100. 101. 102. 103. Melby CL, Paris HL, Drew Sayer R, Bell C, CB, Campbell WW. The effects of Hill JO. Increasing energy flux to maintain consuming frequent, higher protein meals on diet-induced weight loss. Nutrients. appetite and satiety during weight loss in 2019;11(10). overweight/obese men. Obesity. 2011; Carbone JW, Pasiakos SM. Dietary protein the sympathetic nervous system and its application and health benefit. Nutrients. cardiovascular and thermogenic effects in 2019;11(5):1–13. man. Physiol Behav. 2008; Jäger R, Kerksick CM, Campbell BI, Cribb 109. Nijs I, Van Ooijen M, Kovacs EMR. High International Society of Sports Nutrition protein intake sustains weight maintenance Position Stand: Protein and exercise. J Int after body weight loss in humans. Int J Obes. Soc Sports Nutr. 2017;14(1):1–25. 2004; Carbone JW, McClung JP, Pasiakos SM. 110. Plantenga MS. Additional protein intake Energy Balance: Effects of Dietary Protein. limits weight regain after weight loss in Adv Nutr. 2012; humans. Br J Nutr. 2005; Carbone JW, McClung JP, Pasiakos SM. 111. Aller EEJG, Larsen TM, Claus H, Lindroos Recent Advances in the Characterization of AK, Kafatos A, Pfeiffer A, et al. Weight loss Skeletal Muscle and Whole-Body Protein maintenance in overweight subjects on ad Responses to Dietary Protein and Exercise libitum diets with high or low protein during Negative Energy Balance. Advances content and glycemic index: The in Nutrition. 2019. DIOGENES trial 12-month results. Int J Obes. 2014; Moore DR. Maximizing Post-exercise 112. Leidy HJ, Clifton PM, Astrup A, Wycherley Intakes. Front Nutr. 2019;6(September):1– TP, Westerterp-Plantenga MS, Luscombe- 13. Marsh ND, et al. The role of protein in weight loss and maintenance. American Hinkson I V., Elias JE. The dynamic state of Journal of Clinical Nutrition. 2015. 113. protein and carbohydrate intake on body mass and composition during energy requirements and recommendations for restriction: a meta-regression 1. Am J Clin athletes and active populations. Brazilian J Nutr. 2006 Feb;83(2):260–74. Med Biol Res. 2012; Leidy HJ, Mattes RD, Campbell WW. Effects of acute and chronic protein intake on metabolism, appetite, and ghrelin during weight loss. Obesity. 2007; Leidy HJ, Tang M, Armstrong CLH, Martin Metabolic adaptation to weight loss Krieger JW, Sitren HS, Daniels MJ, Langkamp-Henken B. Effects of variation in Poortmans JR, Carpentier A, Pereira-Lancha LO, Lancha A. Protein turnover, amino acid 107. Lejeune MPGM, Kovacs EMR, Westerterp- Skeletal Muscle Responses to Negative Cell Biology. 2011. 106. Westerterp-Plantenga MS, Lejeune MPGM, PJ, Wells SD, Skwiat TM, et al. protein turnover: It’s about time. Trends in 105. van Baak MA. Meal-induced activation of and muscle mass: Translating science to Anabolism: The Case for Relative Protein 104. 108. 114. Kim JE, O’Connor LE, Sands LP, Slebodnik MB, Campbell WW. Effects of dietary protein intake on body composition changes after weight loss in older adults: a systematic review and meta-analysis. Nutr Rev. 2016 Mar;74(3):210–24. 20 115. 116. Wycherley TP, Moran LJ, Clifton PM, Scheiner M, Gonzalez A, et al. A high energy-restricted high-protein, low-fat protein diet (3.4 g/kg/d) combined with a compared with standard-protein, low-fat heavy resistance training program improves diets: a meta-analysis of randomized body composition in healthy trained men controlled trials. Am J Clin Nutr. 2012 and women - a follow-up investigation. J Int Dec;96(6):1281–98. Soc Sports Nutr. 2015; Verreijen AM, Engberink MF, Memelink 123. Fromhoff B, Silver T. The effects of Effect of a high protein diet and/or resistance consuming a high protein diet (4.4 g/kg/d) exercise on the preservation of fat free mass on body composition in resistance-trained during weight loss in overweight and obese individuals. J Int Soc Sports Nutr. 2014; 124. SR. A systematic review of dietary protein during caloric restriction in resistance Coffey VG, Byrne NM. The effect of trained lean athletes: A case for higher exercise interventions on resting metabolic intakes. International Journal of Sport rate: A systematic review and meta-analysis. Nutrition and Exercise Metabolism. 2014. Available from: 125. natural bodybuilding contest preparation: 716 Nutrition and supplementation. J Int Soc Kerksick CM, Wilborn CD, Roberts MD, Smith-Ryan A, Kleiner SM, Jäger R, et al. ISSN exercise & sports nutrition review Sports Nutr. 2014;11(1):1–20. 126. managing weight loss in athletes. Eur J Sport Soc Sports Nutr. 2018;15(1):1–57. “requirements” beyond the RDA: Sci. 2015; 127. energy metabolism and metabolic disorders. physiology, nutrition, and metabolism = Frontiers in Endocrinology. 2016. Physiologie appliquee, nutrition et 128. misunderstood concept. JAMA - Journal of protein intake reduces lean body mass loss the American Medical Association. 2008. during weight loss in athletes. Med Sci 121. Antonio J, Ellerbroek A, Silver T, Vargas L, Peacock C. The effects of a high protein diet on indices of health and body composition a crossover trial in resistance-trained men. J Int Soc Sports Nutr. 2016; Metabolic adaptation to weight loss Wolfe RR, Miller SL. The recommended dietary allowance of protein: A Mettler S, Mitchell N, Tipton KD. Increased Sports Exerc. 2010; Choe SS, Huh JY, Hwang IJ, Kim JI, Kim JB. Adipose tissue remodeling: Its role in implications for optimizing health. Applied metabolisme. 2016. Murphy CH, Hector AJ, Phillips SM. Considerations for protein intake in update: Research & recommendations. J Int Phillips SM, Chevalier S, Leidy HJ. Protein Helms ER, Aragon AA, Fitschen PJ. Evidence-based recommendations for https://doi.org/10.1080/02640414.2020.1754 120. Helms ER, Zinn C, Rowlands DS, Brown MacKenzie-Shalders K, Kelly JT, So D, J Sports Sci [Internet]. 2020 May 12;1–15. 119. Antonio J, Peacock CA, Ellerbroek A, RG, Van der Plas SE, Visser M, Weijs PJM. Nutr J. 2017; 118. Antonio J, Ellerbroek A, Silver T, Orris S, Noakes M, Brinkworth GD. Effects of older adults: a randomized controlled trial. 117. 122. 129. Morton RW, Murphy KT, McKellar SR, Schoenfeld BJ, Henselmans M, Helms E, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance traininginduced gains in muscle mass and strength in 21 breakfasts on perceived appetite and gut healthy adults. Br J Sports Med. 2018; 130. hormones in overweight women. Nutrients. Howarth NC, Saltzman E, Roberts SB. 2015; Dietary Fiber and Weight Regulation. Nutr Rev. 2009; 131. 140. R, Haq S, Yahav E, Hashim SA. Effects of Veronese N, Solmi M, Caruso MG, oatmeal and corn flakes cereal breakfasts on Giannelli G, Osella AR, Evangelou E, et al. satiety, gastric emptying, glucose, and Dietary fiber and health outcomes: An appetite-related hormones. Ann Nutr Metab. umbrella review of systematic reviews and 2015; meta-analyses. Am J Clin Nutr. 2018;107(3):436–44. 132. 141. microbiome: Profound implications for diet Normal-Weight Adults Consume More Fiber and disease. Nutrients. 2019;11(7):1–40. and Fruit than Their Age- and Height142. Microbiota in Host Health and Disease. Cell Liu S, Willett WC, Manson JAE, Hu FB, Host Microbe. 2018;23(6):705–15. Rosner B, Colditz G. Relation between changes in intakes of dietary fiber and grain 134. 143. S, Karnik K, Kristensen M, et al. A review development of obesity among middle-aged of the characteristics of dietary fibers women. Am J Clin Nutr. 2003; relevant to appetite and energy intake outcomes in human intervention trials. Am J Holt SHA, Brand Miller JC, Petocz P, foods. Eur J Clin Nutr. 1995;49(9):675–90. Clin Nutr. 2017;106(3):747–54. 144. on satiety, energy intake, and eating time of obese and nonobese subjects. Am J Clin promotion of satiety and prevention of Nutr. 1983; rebound hypoglycemia. Am J Clin Nutr. 1978; 145. Clark MJ, Slavin JL. The effect of fiber on Review. Sports Medicine. 2015. 146. Guidelines for Obesity Management in J Am Coll Nutr. 2013; Slavin JL. Position of the American Dietetic Association: health implications of dietary fiber. J Am Diet Assoc. 2008; 139. Yumuk V, Tsigos C, Fried M, Schindler K, Busetto L, Micic D, et al. European satiety and food intake: A systematic review. 138. Manore MM. Weight Management for Athletes and Active Individuals: A Brief Yao M, Roberts SB. Dietary Energy Density and Weight Regulation. Nutr Rev. 2009; 137. Duncan KH, Bacon JA, Weinsier RL. The effects of high and low energy density diets Heaton KW, Haber GB, Burroughs L, Murphy D. How fiber may prevent obesity: 136. Poutanen KS, Dussort P, Erkner A, Fiszman products and changes in weight and Farmakalidis E. A satiety index of common 135. Makki K, Deehan EC, Walter J, Bäckhed F. The Impact of Dietary Fiber on Gut Am Diet Assoc. 2006; 133. Hills RD, Pontefract BA, Mishcon HR, Black CA, Sutton SC, Theberge CR. Gut Davis JN, Hodges VA, Gillham MB. Matched Overweight/Obese Counterparts. J Geliebter A, Grillot CL, Aviram-Friedman Adults. Obes Facts. 2015; 147. Jensen MD, Ryan DH, Donato KA, Apovian CM, Ard JD, Comuzzie AG, et al. Executive summary: Guidelines (2013) for the Lafond DW, Greaves KA, Maki KC, Leidy management of overweight and obesity in HJ, Romsos DR. Effects of two dietary adults. Obesity. 2014; fibers as part of ready-to-eat cereal (RTEC) Metabolic adaptation to weight loss 22 148. 149. Escalante G, Campbell BI, Norton L. 151. 152. of intermittent versus continuous energy Breaks as a Precontest Strategy. Strength restriction on weight loss, maintenance and Cond J. 2020;(March):1. cardiometabolic risk: A randomized 1-year trial. Nutr Metab Cardiovasc Dis. 2018; Halberg N, Henriksen M, Söderhamn N, 157. Gower BA, Hunter GR. Dietary adherence on insulin action in healthy men. J Appl during weight loss predicts weight regain. Physiol. 2005; Obesity. 2011; Bird SP, Tarpenning KM, Marino FE. 158. Légaré F, Turcotte S. Interventions to carbohydrate/essential amino acid ingestion enhance adherence to dietary advice for on hormonal and muscular adaptations preventing and managing chronic diseases in following resistance training in untrained adults. Cochrane Database of Systematic men. Eur J Appl Physiol. 2006; Reviews. 2013. Wang L, Rhodes CJ, Lawrence JC. 159. Campbell B, Aguilar D, Wong V, Rogers G, Activation of mammalian target of Fox C, Hosey T, et al. The effects of rapamycin (mTOR) by insulin is associated intermittent carbohydrate re-feeds vs. with stimulation of 4EBP1 binding to continuous dieting on resting metabolic rate dimeric mTOR complex 1. J Biol Chem. in resistance trained individuals: A flexible 2006; dieting study. Proc Fifteenth Int Soc Sport Nutr Conf Expo. 2018; Jenkins AB, Markovic TP, Fleury A, 160. Burke LM, Hawley JA, Jeukendrup A, short-term regulation of leptin in humans. Morton JP, Stellingwerff T, Maughan RJ. Diabetologia. 1997; Toward a common understanding of dietexercise strategies to manipulate fuel Dirlewanger M, Di Vetta V, Guenat E, availability for training and competition preparation in endurance sport. Int J Sport Effects of short-term carbohydrate or fat Nutr Exerc Metab. 2018;28(5):451–63. overfeeding on energy expenditure and plasma leptin concentrations in healthy 161. exercise performance. Sports Medicine. Havel PJ. Role of adipose tissue in body- 1997. weight regulation: Mechanisms regulating leptin production and energy balance. In: 162. Cholewa JM, Newmire DE, Zanchi NE. Carbohydrate restriction: Friend or foe of Proceedings of the Nutrition Society. 2000. resistance-based exercise performance? Schübel R, Nattenmüller J, Sookthai D, Nutrition. 2019;60:136–46. Nonnenmacher T, Graf ME, Riedl L, et al. Effects of intermittent and continuous Hawley JA, Schabort EJ, Noakes TD, Dennis SC. Carbohydrate-loading and female subjects. Int J Obes. 2000; 155. Desroches S, Lapointe A, Ratté S, Gravel K, Independent and combined effects of liquid Battilana P, Seematter G, Schneiter P, et al. 154. Del Corral P, Bryan DR, Garvey WT, Effect of intermittent fasting and refeeding Campbell L V. Carbohydrate intake and 153. Sundfør TM, Svendsen M, Tonstad S. Effect Effectiveness of Diet Refeeds and Diet Stallknecht B, Ploug T, Schjerling P, et al. 150. 156. 163. Escobar KA, Vandusseldorp TA, Kerksick calorie restriction on body weight and CM. Carbohydrate intake and resistance- metabolism over 50 wk: A randomized based exercise: Are current controlled trial. Am J Clin Nutr. 2018; recommendations reflective of actual need? Metabolic adaptation to weight loss 23 as a means to disrupt weight control efforts. Br J Nutr. 2016;116(12):2053–65. 164. Obes Res. 2003; M. H, L.L. S. Exercise metabolism: Fuels for the fire. Cold Spring Harb Perspect Med. 172. JB. Weight-loss outcomes: A systematic 2018;8(8):1–16. 165. review and meta-analysis of intermittent Hearris MA, Hammond KM, Fell JM, energy restriction trials lasting a minimum Morton JP. Regulation of muscle glycogen of 6 months. Nutrients. 2016. metabolism during exercise: Implications for endurance performance and training 173. restriction interventions for weight Campbell BI, Aguilar D, Colenso-semple management: a systematic review and meta- LM, Hartke K, Fleming AR, Fox CD, et al. analysis. Obesity Reviews. 2018. Intermittent Energy Restriction Attenuates the Loss of Fat Free Mass in Resistance 167. 174. Sundgot-Borgen J. Effect of two different Controlled Trial. 2020;1–12. weight-loss rates on body composition and strength and power-related performance in Henry RR, Scheaffer L, Olefsky JM. elite athletes. Int J Sport Nutr Exerc Metab. 2011; restriction and isocaloric refeeding in noninsulin-dependent diabetes mellitus. J 175. perspective of human body composition Byrne NM, Hills AP. Biology or Behavior: autoregulation. In: Proceedings of the Which Is the Strongest Contributor to Nutrition Society. 2012. Weight Gain? Curr Obes Rep. 2013; Byrne NM, Sainsbury A, King NA, Hills 176. overshooting in humans: A role for feedback restriction improves weight loss efficiency in signals from lean and fat tissues. Am J Clin obese men: The MATADOR study. Int J Nutr. 1997; Obes. 2018; Davoodi SH, Ajami M, Ayatollahi SA, Dowlatshahi K, Javedan G, Pazoki-Toroudi HR. Calorie shifting diet versus calorie restriction diet: A comparative clinical trial study. Int J Prev Med. 2014; 171. Wing RR, Jeffery RW. Prescribed “breaks” Metabolic adaptation to weight loss View publication stats Dulloo AG, Jacquet J, Girardier L. Poststarvation hyperphagia and body fat AP, Wood RE. Intermittent energy 170. Dulloo AG, Jacquet J, Montani JP. How dieting makes some fatter: From a Clin Endocrinol Metab. 1985; 169. Garthe I, Raastad T, Refsnes PE, Koivisto A, Trained Individuals . A Randomized Glycemic effects of intensive caloric 168. Harris L, McGarty A, Hutchison L, Ells L, Hankey C. Short-term intermittent energy adaptations. Nutrients. 2018;10(3):1–21. 166. Headland M, Clifton PM, Carter S, Keogh 177. Hector AJ, McGlory C, Damas F, Mazara N, Baker SK, Phillips SM. Pronounced energy restriction with elevated protein intake results in no change in proteolysis and reductions in skeletal muscle protein synthesis that are mitigated by resistance exercise. FASEB J. 2018; 24