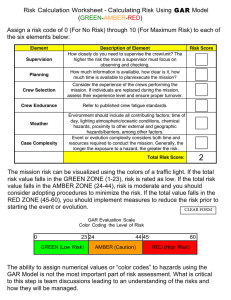
Pre-Job Briefing/Job Safety Analysis (JSA) Form Date________________ Person Completing Form______________________________Supervisor________________________________ Work Location/Address:________________________________City/Town:_________________Time:___________□ AM □ PM GPS Coordinates:_____________________ Nearest Intersection: Landmark: If you were to call 911,what landmark information would be helpful to provide Enter Temperature for applicable Conditions:_____________________ Weather Conditions:____Sunny____Cloudy____Rain____Snow____Ice____Wind Are weather conditions appropriate for the work to be conducted? Yes No; if no, find appropriate job site or task or suspend operations. 1.) Emergency Information: Area 911 Yes/No If No, EMS/Fire Phone number_____________________________________ Emergency Action Plan: How will we conduct a rescue?_______________________________________________________ __________________________________________________________________________________________________ First Aid Supplies Onsite:_______________________________________________________________________________ Closest Medical Facility: Name:____________________________________________________Contact#________________________________ Address____________________________________________________________________________________ Do I have crew members who are CPR and First Aid Trained? Yes/No Work or Training Task: 2.) Is this a training? or work related?(Please Circle one) Job Tasks: _____Driving_____Inspection/Auditing_____Traffic Control____Bucket Trim____Ground Cutting ____Climbing____Brush Chipping____Tree Removal____Stump Grinding____Crane ____Heavy Equipment Operation (Please Identify Equipment_________________________) Other Describe:__________________________________________________________________________________________ 3.) NATS’ MODEL: Applying the NIOSH Hierarchy of Controls When Dealing With COVID-19 Job Site Hazard Control (Describe how you are going to control hazards, risks, and potential impacts)___________________________ _________________________________ _________________________________ _________________________________ _________________________________ _________________________________ _________________________________ _________________________________ Proper Personal Protective Equipment (PPE) while responding to COVID-19 ____N95 Respiratory Protection (Face Mask) ____Medical Gloves ____Eye Protection (goggles or a disposable face shield that covers the front and sides of the face) Remove all PPE once contaminated and after being exposed to other individuals or potential hazard. 4.) Electrical Safety Are electric utilities present in or near your work area?_____Yes_____No Is the work taking place for a utility contractor or subcontractor? _____Yes_____No Are the students/attendees QLCA Trained? _____Yes_____No Utility Company___________________________________________ Utility & Contact Number Line kV MAD Pole or Structure # Verification of Di-Electric test date (MM/YY): Insulated Tool _________Insulated Pole Saw__________Insulated Pole Pruner__________Insulated Boom_______Other (Solid Core Only) (Solid Core Only) 5.) Topics of Discussion (Hazards, Risks and Potential Impacts) Gravity Falling Objects/Tools □ □ □ □ Falling from a Height Falling Trees/Branches Drop Zone Electrical □ Energized Equipment □ □ □ □ Chemical □ Flammable or Explosive □ Toxic or Poisonous □ Corrosive or Reactive □ Acids or Caustics Hazard Control Measures Backfeed/Induction Energized Trees Vertical to Horizontal Conductors Mechanical □ Equipment Failure □ □ □ Climbing Hazards Tension Loads Moving Parts/Sharp Objects Vehicular □ Traffic Conditions □ □ □ Driving Conditions Moving Loads Vehicle Stability Step Potential Body Mechanics □ □ □ □ Hazard Identification List – Check all that apply Slips or Trips Lifting/Twisting Repetitive Motion Awkward Positions Noise □ □ □ Other Continuous Loud Noise Explosive Noise Distractive Noise □ □ □ □ Insect Bites/Stings Wildlife Blood/Body Fluids Heat/Cold Exposure Is Drop zone sufficient to drop debris away from obstacles?___Yes___No; If no, select other means of controlling debris/drop zone. Job Site Hazard Control (Describe how you are going to control hazards, risks, and potential impacts)_____________________________ __________________________________ __________________________________ __________________________________ __________________________________ __________________________________ Identify type & # of Signs & Cones: _______________________Signs _____________Cones in place to ID work site Traffic Control Flagger Initials: 1_________2________ Radios______Yes_______No Dig Safe Required? 1-800-DIG-SAFE ______Yes_______No 6.) Personal Protective Equipment Required Has every employee inspected their Personal Protective Equipment?_____Yes_____No Head Protection ____Hard Hat/ Helmet (ANSI Z89) ____Face Shield (When Required) Eye Protection Leg Protection ____Chainsaw Pants OR ____Chainsaw Chaps Foot Protection ____Safety Glasses Or Eye shield (ANSI Z87.1) Hearing Protection ___Hearing Protection Hand Protection _____Gloves/Cutresistant gloves (ANSI 105) ____Class 2 Hi Vis ____Other ____Boots ____CutResistant Boots Fall Protection ____Fall Restraint ____Work Position ____Fall Suspension ____Fall Arrest In an effort to reduce the potential spread of COVID-19, please designate one person on your crew to capture all required information. Through verbal responses from crew members, the transcriber will report all opinions and positions utilizing the GAR model and will document each individual's response in the chart above next to the appropriate name. Employee# Name Verbal Status (GAR) The Green, Amber, Red (GAR )Model The Green, Amber, Red or (G.A.R.) Model is a work risk management model that includes and values the opinions and positions of all workers involved on a work project/site. There is no allowance for hierarchy or anyone to force another to proceed until discussion and/or explanation results in all workers involved being Green. All workers must have indicated their status in the above chart as Green. If any worker has indicated that they are an Amber or Red, then discussion and/or measures must take place to address concerns to alleviate risks until all individuals are Green. Person Transcribing: Print Name:___________________________Signature :______________________________ Job Site Visit: Supervisor:____________________Manager:_____________________Safety:_________________