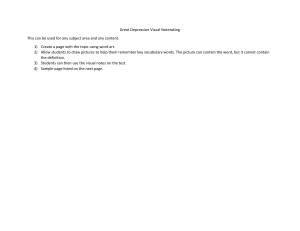
ORIGINAL ARTICLE Characteristics and correlates of poststroke depression: An Indian study Amlan Kusum Jana, Suddhendu Chakraborty1, Samir Kumar Praharaj2 Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 Department of Psychiatry, KPC Medical College and Hospital, Kolkata, 1Department of Psychiatry, Bongaon J R Dhar Sub Divisional Hospital, Bongaon, West Bengal, 2Department of Psychiatry, Kasturba Medical College, Manipal, Karnataka, India ABSTRACT Background: Post stroke depression adversely affects long term outcome of stroke and increases mortality risk. Few studies have looked into the comprehensive picture of post stroke depression in past. Aim: The current study aimed to look into the phenomenology, characteristic features and various correlates of post stroke depression. Method: 142 consecutive stroke patients aged 60 years or above, fulfilling the inclusion criteria were assessed. Sociodemographic and clinical data were gathered using a specially designed pro-forma. Depression, apathy and psychosis were assessed by Post stroke depression rating scale, Apathy Evaluation Scale, and Brief Psychiatric Rating Scale respectively. Groups (with or without major depression) were compared using Mann-Whitney U, chi square or Fisher’s exact test. One way ANOVA was conducted to see the relations of lesion location and laterality with various clinical parameters. Kaplan-Meier survival analysis was done to see the time to develop depression. The effect sizes were reported as r and partial eta squared. Results: Guilt was significantly higher (p<.05) with lesions in parietal lobe and remaining of middle cerebral artery territory. Catastrophic reaction (p<.05) and emotional dyscontrol (p<.05) were higher for diffuse lesions, periventricular lesions and lesions in frontal/occipital lobe. BPRS score, but not apathy, had a significant positive correlation with depression (Pearson’s r=.692). Mean time to develop depression after stroke was 28.34 (95% CI 22.37 to 34.31) months. Conclusions: Post stroke depression consists of various clinically important sub-components whose occurrence varies with different lesion locations. Post stroke depression is discriminable from apathy but is related to psychosis. Key words: Apathy, depression, stroke INTRODUCTION Stroke is a devastating neurological disorder with both neurological and psychiatric complications. From aphasia, hemiparesis, or other neurodeficits to depression, psychosis, Address for correspondence: Dr. Suddhendu Chakraborty, Department of Psychiatry, Bongaon J R Dhar Sub Divisional Hospital, Bongaon ‑ 743 235, 24 Paraganas (North), West Bengal, India. E‑mail: dr.suddhendu.chakraborty@gmail.com or apathy, burden of stroke can be quite heavy. Poststroke depression especially worsens the overall outcome of stroke. Patients with poststroke depression show far less recovery from functional impairments compared to nondepressed patients with stroke and are 3.4 times more likely to die during the first 10 years after stroke.[1] The role of depression in poststroke mortality has been re‑emphasized in a meta‑analysis.[2] Opposing theories exist to explain the relation between stroke and depression. Some propose a biological mechanism behind depression, according Website: This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms. www.indianjpsychiatry.org For reprints contact: reprints@medknow.com Access this article online Quick Response Code DOI: 10.4103/psychiatry.IndianJPsychiatry_421_19 How to cite this article: Jana AK, Chakraborty S, Praharaj SK. Characteristics and correlates of poststroke depression: An Indian study. Indian J Psychiatry 2019;61:605-11. © 2019 Indian Journal of Psychiatry | Published by Wolters Kluwer - Medknow 605 Jana, et al.: Characteristics of poststroke depression Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 to which vascular insults directly affect neural circuits regulating mood.[3,4] Inflammatory process, genetic and epigenetic variations, white matter disease, cerebrovascular dysregulation, altered neuroplasticity, and changes in glutamate transmission have all been thought to be giving rise to various psychiatric disorders after stroke.[5] Others propose psychosocial mechanism which takes the social and psychological stressors associated with stroke as the causes behind depression.[6,7] However, current understanding endorses a bidirectional relation between physical and psychiatric illnesses.[8,9] There has been controversy regarding phenomenology of poststroke depression as well. Catastrophic reactions, hyperemotionality, and diurnal mood variations have been proposed to be more consistently associated with poststroke depression compared to endogenous depression.[5] However, as these features are widely seen in other neurological conditions without depression, question remains about their specificity for poststroke depression.[10] Researches have been carried out to find an association between specific location of stroke and subsequent development of depression. Robinson and Szetela[11] in their landmark research had shown a significant inverse correlation between the severity of poststroke depression and the distance of the anterior border of the lesion from the frontal pole. Since then, there have been a number of researches looking for an association of specific lesion location and depression though reaching a consensus has not yet been possible. At this juncture, a study of poststroke depression, looking for the phenomenology, and the clinical and anatomical correlates was felt necessary. There have been very few studies in this field from South Asian countries, and the single study from India[12] had a small sample size and had assessed depression through an instrument which was not specific for poststroke depression. The current study attempted to overcome these methodological flaws and present a holistic picture of poststroke depression. MATERIALS AND METHODS Participants This was a cross‑sectional study carried out in the outpatient clinic of the department of neurology in a tertiary hospital. The hospital is situated in the southern part of Kolkata, India, with a wide catchment area. Ethical clearance was obtained from the institutional ethical committee before conducting the study. The sample consisted of 142 consecutive patients, giving written informed consent, diagnosed with stroke, and fulfilling the study criteria. Inclusion criteria included patients diagnosed with stroke by qualified neurologist(s) and patients aged over 60 years. Patients with a past history of psychiatric disorder, substance use (except nicotine), family history of psychiatric disorder, poor cognitive function so as to lead to unreliable psychiatric assessment (Hindi Mental Status Examination score ≤23), and history of 606 stressful life events (excepting current illness) since the onset of stroke or in the past 6 months (whichever is earlier) were excluded from the study. Since the study was conducted in the outpatient clinic, all those stroke patients who were admitted to the hospital were automatically excluded. Assessment All the assessments were made by a single clinician. The assessments were done before looking into neuroimaging or other investigation findings. Sociodemographic and clinical data were gathered using a pro forma specially designed for the study which included all the relevant parameters as described in literature including age, sex, marital status, family type, monthly income, education, residence, current and past employment status, and past medical history among others. The details of stroke, which were filled up after the clinical assessments, included location of lesion, number, type (ischemia/hemorrhage), and the exact date of the event. Poststroke depression was assessed by the Poststroke Depression Rating Scale (PSDRS).[13] It consists of 10 sections. The first nine sections include depressed mood, guilt feelings, suicidality, vegetative (sleep and appetite) disorders, apathy/abulia/indifference, anxiety, catastrophic reactions, difficulty in emotional control, and anhedonia. The last section detects diurnal mood variation. Each section has a score range of 0–5 with a higher score meaning worse psychopathology. The assessment consists of a semi‑structured interview that follows for each section. In determining the total score, all the scores of the sections are summed up excluding the last section which does not denote depression severity.[14] Hence, the PSDRS score ranges from 0 to 45. This scale is specifically designed to detect poststroke depression, emphasizing on those symptoms such as catastrophic reaction and emotional dyscontrol which are common in poststroke depression but not in functional depression. Besides, it is the only scale to provide a holistic picture of poststroke depression, beyond just depressive symptoms. Apathy was separately assessed by the clinician‑rated version of the Apathy Evaluation Scale.[15] It is an 18‑item scale with each item generating a score from 1 (“not at all characteristic”) to 4 (“a lot characteristic) on a Likert scale. The maximum total score is thus 72. This is a widely used scale for assessing apathy, especially in patients with neurological illnesses. For screening of cognitive impairment, the Hindi Mental Status Examination[16] was used as all the participants in the study could speak and understand Hindi. This is a modified version of the Mini Mental Status Examination (MMSE).[17] In this scale the main advantage over MMSE is that it can be used in illiterate persons as well. The maximum score is 30, and the cutoff for cognitive dysfunction is 23. Indian Journal of Psychiatry Volume 61, Issue 6, November-December 2019 Jana, et al.: Characteristics of poststroke depression To screen stressful live events, the Presumptive Stressful Life Events Scale[18] was used which is an Indian adaptation of the Social Readjustment Rating Questionnaire.[19] A total of 51 life events are included in the scale which are subclassified according to whether they are personal or impersonal (not dependent on the individual’s action) and according to whether they are desirable, undesirable, or ambiguous. Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 Psychosis was assessed by the Brief Psychiatric Rating Scale (BPRS).[20] The Global Assessment of Functioning (GAF)[21] scale was employed to assess patients’ functioning in the past 1 month. Patients were also assessed by the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM‑IV)[22] to detect whether or not they had major depression. Windows (SPSS Inc., Chicago, Ill, USA). One‑way analysis of variance (ANOVA) was conducted to see the relations of lesion laterality (left‑hemispheric lesion, right‑hemispheric lesion, and bilateral lesion) as well as lesion location with various clinical profiles including apathy, scores in the subscales of PSDRS, BPRS score, and GAF score. Lesion location was divided into four subgroups according to predominant source of blood supply: Area A (74 patients): basal ganglia (supplied mainly by the middle cerebral artery [MCA]); Area B (28 patients): parietal lobe and rest of the MCA territory; Area C (23 patients): brain stem, cerebellum, and thalamus (supplied mainly by the posterior cerebral, vertebral, and basilar arteries); and Area D (17 patients): the remaining locations including diffuse lesions, periventricular region, frontal lobe, occipital lobe, and other locations. Statistical analysis The collected data were statistically analyzed using the Statistical Package for the Social Sciences (SPSS) 16.0 for According to the DSM‑IV, patients were grouped as with or without major depression. The groups were compared using the Mann–Whitney U‑test for continuous variables and the Table 1: Group differences in clinical and demographic profile Age, mean (SD) Years of education, mean (SD) Time since stroke (months), mean (SD) GAF, mean (SD) AES (C), mean (SD) BPRS, mean (SD) Sex (male), n (%) Marital status (married), n (%) Family type (nonnuclear), n (%) Lesion location, n (%) Basal ganglia Parietal lobe + MCA territory Brain stem + cerebellum + thalamus Others Lesion laterality (n=141), n (%) Left Right Bilateral Current lesion number, n (%) 1 2 Multiple Lesion type (ischemia), n (%) Religion (Hindu), n (%) Income (middle), n (%) Occupation, n (%) Employed Unemployed Others Residence, n (%) Urban Rural Semi‑urban Family diagnosis (n=40), n (%) Medical Stroke/related Family history (absent), n (%) Past medical history (absent), n (%) With major depression (n=55) Without major depression (n=87) P 67.42 (7.073) 9.16 (5.711) 14.75 (10.261) 71.42 (6.682) 34.11 (8.728) 15.91 (5.093) 30 (54.54) 51 (92.73) 45 (81.82) 68.02 (7.251) 9.71 (5.521) 13.94 (8.677) 74.74 (6.355) 34.89 (9.257) 12.47 (4.948) 48 (55.17) 83 (95.40) 59 (67.82) 0.591 0.619 0.766 0.007 0.753 0.000* 0.942 0.501 0.066 26 (47.27) 13 (23.64) 8 (14.54) 8 (14.54) 48 (55.17) 15 (17.24) 15 (17.24) 9 (10.34) 0.626 23 (42.59) 18 (33.33) 13 (24.07) 44 (50.57) 33 (37.93) 10 (11.49) 0.144 40 (72.73) 3 (5.45) 12 (21.82) 40 (72.73) 41 (74.54) 32 (58.18) 70 (80.46) 6 (6.89) 11 (12.64) 68 (78.16) 72 (82.76) 56 (64.37) 0.334† 4 (7.27) 19 (34.54) 32 (58.18) 5 (5.75) 30 (34.48) 52 (59.77) 0.961† 9 (16.36) 33 (60.00) 13 (23.64) 16 (18.39) 59 (67.82) 12 (13.79) 0.325 12 (75.00) 4 (25.00) 39 (70.91) 43 (78.18) 15 (62.50) 9 (37.50) 63 (72.41) 68 (78.16) 0.408 0.460 0.237 0.459 0.846 0.998 Fischer’s exact test conducted for these variables; *P<0.001. MCA – Middle cerebral artery; AES (C) – Apathy Evaluation Scale (clinician version); GAF – Global Assessment of Functioning Scale; BPRS – Brief Psychiatric Rating Scale; SD – Standard deviation † Indian Journal of Psychiatry Volume 61, Issue 6, November-December 2019 607 Jana, et al.: Characteristics of poststroke depression Chi‑square test or Fisher’s exact test (whichever is applicable) for categorical variables. Finally, Kaplan–Meier survival analysis was done to see the time to develop depression after stroke. The effect sizes were reported as r (calculated from z value of the Mann–Whitney U‑test) and partial eta squared. The level of significance was set at P < 0.05 (two‑tailed). Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 RESULTS Group comparison As shown in Table 1, patients with major depression had lower mean age, years of education, GAF score, and apathy and higher mean time since stroke, but the differences did not reach statistical significance. However, depressed patients had a significantly higher BPRS score (P < 0.001; r = 0.34) compared to their nondepressed counterparts. In the distribution of sex, marital status, family type (nuclear vs. nonnuclear), lesion location, laterality (right/left hemispheric or bilateral), number (one/two/multiple) and type (ischemia vs. hemorrhage), religion (Hindu vs. Muslim and others), income (middle vs. low), occupation (employed, unemployed, and others including students and homemakers), residence (urban, rural, and semi‑urban), family history (present vs. absent), past medical history (present vs. absent), and family diagnoses (medical vs. stroke/related history), patients with major depression were comparable to those without. Relations of lesion laterality with other clinical parameters One‑way ANOVA [Table 2] between various clinical parameters and lesion laterality did not show left‑hemispheric lesions to be associated with a higher value of guilt in PSDRS, but the association was not statistically significant. Likewise, for the subscale of anxiety in the PSDRS, left‑hemispheric lesions showed a higher value compared to right‑hemispheric or bilateral lesion, but the difference failed to reach statistical significance. Relations of lesion location with other clinical parameters One‑way ANOVA [Table 3] showed significant group differences in apathy (P = 0.036; df: 3, 138) where patients with lesions in Area C (brain stem, cerebellum, and thalamus) had the highest value among different lesion locations. For the subscale of guilt in the PSDRS, Area B, i.e., parietal lobe and the remaining MCA territory lesions, produced a significantly higher (P = 0.025; df: 3, 138) score compared to other locations. BPRS score (P = 0.001; df: 3, 138; partial eta squared = 0.112), catastrophic reaction (P = 0.039; df: 3, 138), and emotional dyscontrol (P = 0.013; df: 3, 138) were significantly higher in patients with lesions in Area D (diffuse lesions, frontal lobe, occipital lobe, periventricular region, etc.) compared to other lesion location areas. Area D also registered a higher value than other areas, for total PSDRS score (P = 0.070; df: 3, 138) and the subscale of sleep (P = 0.089; df: 3, 138). The differences, however, did not reach statistical significance. Similarly, a higher mean suicidality score (another subscale of PSDRS) was seen with lesions in Area B which failed to achieve statistical significance (P = 0.057; df: 3, 138). Other findings Poststroke depression total score was not significantly correlated with age, years of education, time since stroke, or apathy. However, a significant positive correlation (P < 0.001) was seen with BPRS (Pearson’s r = 0.692). This significance was maintained (P < 0.001) even when partial correlation between them was calculated after age, years of education, time since stroke, and apathy were controlled (Pearson’s r = 0.731). The prevalence of poststroke depression (major) in the current study was 38.73% (55 patients out of 142). Table 2: Relation of lesion laterality with various clinical profiles Laterality, mean (SD) PSDRS total PSDRS mood PSDRS guilt PSDRS suicidality PSDRS sleep PSDRS appetite PSDRS apathy‑indifference PSDRS anxiety PSDRS catastrophic reaction PSDRS emotional dyscontrol PSDRS anhedonia PSDRS diurnal variation GAF AES (C) BPRS Time since stroke (months) ANOVA Left (n=67) Right (n=51) Bilateral (n=23) F P 18.10 (5.745) 2.12 (0.616) 1.48 (0.841) 0.99 (0.639) 1.43 (0.633) 1.04 (0.614) 2.76 (1.615) 2.34 (1.175) 1.04 (0.638) 1.15 (0.530) 3.75 (1.119) 1.78 (0.850) 73.67 (6.609) 35.18 (9.326) 14.24 (5.027) 14.57 (11.187) 16.90 (5.766) 1.98 (0.616) 1.12 (0.739) 0.98 (0.678) 1.31 (0.616) 0.96 (0.599) 2.75 (1.468) 1.94 (1.333) 1.06 (0.858) 1.16 (0.612) 3.65 (1.110) 1.69 (0.860) 73.94 (6.373) 33.35 (8.054) 13.10 (5.711) 13.04 (7.403) 16.39 (4.755) 1.91 (0.733) 1.39 (0.839) 1.09 (0.668) 1.35 (0.647) 0.91 (0.417) 2.83 (1.497) 1.74 (0.810) 0.78 (0.422) 1.04 (0.475) 3.35 (1.613) 1.87 (0.757) 72.52 (6.625) 35.65 (10.421) 13.78 (4.843) 15.74 (6.635) 1.102 1.200 2.694 0.241 0.546 0.562 0.022 2.928 1.419 0.377 0.931 0.405 0.387 0.772 0.682 0.722 0.335 0.304 0.055 0.787 0.580 0.571 0.978 0.057 0.245 0.687 0.397 0.668 0.680 0.464 0.507 0.488 PSDRS – Poststroke Depression Rating Scale; AES (C) – Apathy Evaluation Scale (clinician version); GAF – Global Assessment of Functioning Scale; BPRS – Brief Psychiatric Rating Scale; ANOVA – Analysis of variance; SD – Standard deviation 608 Indian Journal of Psychiatry Volume 61, Issue 6, November-December 2019 Jana, et al.: Characteristics of poststroke depression Table 3: Relation of lesion location with various clinical profiles Lesion location, mean (SD) Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 Age (years) Years of education Time since stroke (months) GAF AES (C) BPRS PSDRS total PSDRS mood PSDRS guilt PSDRS suicidality PSDRS sleep PSDRS appetite PSDRS apathy PSDRS anxiety PSDRS catastrophic reaction PSDRS emotional dyscontrol PSDRS anhedonia PSDRS diurnal variation ANOVA Area A (n=74) Area B (n=28) Area C (n=23) Area D (n=17) F P 68.46 (7.753) 9.64 (5.877) 13.31 (8.158) 74.42 (6.857) 32.85 (8.551) 12.70 (4.742) 16.84 (5.075) 2.00 (0.549) 1.24 (0.824) 0.88 (0.618) 1.27 (0.556) 0.97 (0.596) 2.74 (1.481) 2.04 (1.091) 0.95 (0.639) 1.05 (0.402) 3.69 (1.146) 1.74 (0.812) 66.79 (6.641) 8.86 (5.407) 15.62 (10.171) 73.32 (7.318) 34.50 (10.423) 15.64 (4.490) 19.25 (6.108) 2.21 (0.833) 1.75 (1.076) 1.25 (0.752) 1.57 (0.690) 1.07 (0.604) 3.07 (1.609) 2.18 (1.188) 1.11 (0.832) 1.14 (0.591) 3.89 (1.315) 1.64 (0.826) 67.35 (7.030) 9.70 (5.764) 14.23 (12.356) 72.57 (5.017) 38.70 (7.945) 12.48 (5.125) 16.09 (6.338) 1.91 (0.733) 1.13 (0.757) 1.04 (0.638) 1.39 (0.656) 0.87 (0.548) 2.52 (1.620) 1.83 (1.114) 0.87 (0.626) 1.09 (0.515) 3.43 (1.273) 1.91 (0.793) 67.12 (5.566) 9.71 (4.593) 15.71 (7.389) 70.65 (6.133) 36.71 (8.498) 17.35 (6.623) 19.53 (6.663) 2.24 (.831) 1.53 (.624) 1.18 (.728) 1.59 (.795) 1.18 (.529) 2.71 (1.532) 2.71 (1.687) 1.47 (1.007) 1.53 (.874) 3.41 (1.228) 1.76 (1.033) 0.473 0.153 0.547 1.689 2.925 5.827 2.403 1.410 3.214 2.573 2.214 1.097 0.578 1.948 2.875 3.729 0.862 0.443 0.702 0.928 0.651 0.172 0.036* 0.001* 0.070 0.242 0.025* 0.057 0.089 0.353 0.631 0.125 0.039* 0.013* 0.462 0.723 *P<0.05. Area A – Basal ganglia; Area B – Parietal lobe and rest of the MCA territory; Area – Brain stem, cerebellum, and thalamus; Area D – Others (diffuse lesions, frontal lobe, occipital lobe, periventricular region, etc.). PSDRS – Poststroke Depression Rating Scale; AES (C) – Apathy Evaluation Scale (clinician version); GAF – Global Assessment of Functioning Scale; BPRS – Brief Psychiatric Rating Scale; ANOVA – Analysis of variance; SD – Standard deviation with current or past substance use and stressful life events (excepting the current stroke) in a relevant time period. Hence, the depression seen in the study population was biologically and/or psychosocially related to stroke only, and the confounding variables were taken care of. The sample size was robust, and the instrument for detecting depression was specific for poststroke depression only. Figure 1: Kaplan–Meyer survival analysis showing time to depression after stroke. Mean survival time – 28.34 (95% confidence interval: 22.37–34.31) months Kaplan–Meier survival analysis showed [Figure 1] mean time to develop depression (as diagnosed by the DSM‑IV) after stroke was 28.34 (95% confidence interval: 22.37–34.31) months. DISCUSSION A major strength of the current study lied in elimination of rater bias. The rater was blind to investigation reports (including neuroimaging findings) or current treatment regimen as ratings were done before looking into them. Sample selection was another area of strength. All the predisposing factors for depression, apart from the stroke itself, were eliminated by excluding patients with a past history or family history of psychiatric illness and patients The highlight of the current study finding is that though the depression score (PSDRS total) was not significantly different across lesion locations and did not change significantly according to lesion laterality, its components did. Guilt, catastrophic reaction, and emotional dyscontrol significantly varied across lesion locations. Again guilt and anxiety, though not statistically significant, did vary according to lesion laterality. These findings probably justified the selection of PSDRS over the other rating scales to detect functional depression. It produces a comprehensive picture of poststroke depression beyond the depressive symptoms. It also helped in looking into the relation of symptoms more specific to poststroke depression (as compared to functional depression, e.g., catastrophic reaction), with lesion location and laterality. Guilt and anxiety were more (though not statistically significant) in left‑hemispheric lesions. Left‑hemispheric lesions have been reported to be more consistently associated with depression,[23] though the importance of laterality is diluted with passage of time after stroke. By 3–6 months poststroke, proximity to the frontal lobe in both hemispheres influences the occurrence of poststroke depression.[24] Guilt also showed significantly different values across lesion locations with the highest mean value for lesions in the parietal lobe and the remaining of the MCA territory. However, relations of components of poststroke Indian Journal of Psychiatry Volume 61, Issue 6, November-December 2019 609 Jana, et al.: Characteristics of poststroke depression depression‑like guilt with lesion laterality or location have not been reported previously. Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 Apathy, abulia, and indifference, as a subscale of PSDRS, did not produce significantly different values across lesion locations, but a composite measure of apathy through the Apathy Evaluation Scale showed the highest value for lesions in the thalamus, cerebellum, or brain stem. Apathy is more commonly seen in lesions of cortico-subcortical circuits[25] and basal ganglia which lead to dysfunctions of frontal subcortical system.[26] However association of apathy with thalamic lesions has also been seen.[27-29] Catastrophic reaction and emotional dyscontrol had significantly higher mean values for diffuse lesions, periventricular lesions, and lesions in the frontal and occipital lobes. This was in comparison with lesions in the parietal lobe, basal ganglia, cerebellum, brain stem, and thalamus. The current study population had a disproportionately little number of patients with lesion in the frontal and occipital lobes, and the group with lesions in Area D (the “others” group) which included these locations contained only 17 patients. Hence, this particular finding should be cautiously generalized. Depression, as assessed by total score of PSDRS, did not have any significant correlation with apathy. Apathy has been reported to be related to but discriminable from depression.[15] The current finding thus is in accordance with that. However, poststroke depression was significantly positively correlated with psychosis (BPRS score), and the significance was maintained in partial correlation between them after the possible confounding variables were controlled. This was reflected in comparison of groups as well. Patients with depression (diagnosed by the DSM‑IV) had a significantly higher BPRS score than those without. This relation between poststroke depression and psychosis has not been reported in the past. Poststroke depression and psychosis are two distinguishable entities, but BPRS might not be the best instrument to detect poststroke psychosis. Probably, this finding should encourage researchers to device an instrument to specifically detect poststroke psychosis. The prevalence of major depression (as per the DSM‑IV) was seen to be 38.73% which falls in the range described in literature.[10] Mean time to develop major depression was 28.34 months. This is longer than what is described in literature so far,[30] which reports the peak prevalence of depression to be around 3–6 months following stroke, declining by about 50% in 1 year time. However, in the current study, survival analysis was done only for major depression (as per the DSM‑IV) and not minor depression or dysthymia which also are common after stroke. This might explain the longer mean time to develop depression. 610 CONCLUSION It can be said that poststroke depression consists of various clinically important subcomponents apart from depressed mood, and their occurrence varies according to lesion locations. Poststroke depression is discriminable from apathy but is related to poststroke psychosis. The current study had certain limitations. First, the cross‑sectional design failed to detect the relation of stroke and depression over a longer time period. It also could not throw any light on the course and long term outcome of poststroke depression. Second, since the study was hospital based, many patients in community who were not obtaining the services of this hospital were missed. Finally, to eliminate confounding variables for depression, patients with a past or family history of depression and patients with current or past substance use were excluded from the study. This elimination was achieved against a cost as it made the current study unable to detect the association between these factors and poststroke depression. In the future, community‑based prospective studies from these parts of the world might shed more light in this interesting field. Financial support and sponsorship Nil. Conflicts of interest There are no conflicts of interest. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Morris PL, Robinson RG, Andrzejewski P, Samuels J, Price TR. Association of depression with 10‑year poststroke mortality. Am J Psychiatry 1993;150:124‑9. Bartoli F, Lillia N, Lax A, Crocamo C, Mantero V, Carrà G, et al. Depression after stroke and risk of mortality: A systematic review and meta‑analysis. Stroke Res Treat 2013;2013:862978. Starkstein SE, Bryer JB, Berthier ML, Cohen B, Price TR, Robinson RG. Depression after stroke: The importance of cerebral hemisphere asymmetries. J Neuropsychiatry Clin Neurosci 1991;3:276‑85. Robinson RG, Kubos KL, Starr LB, Rao K, Price TR. Mood disorders in stroke patients. Importance of location of lesion. Brain 1984;107 (Pt 1):81‑93. Robinson RG, Jorge RE. Post‑stroke depression: A Review. Am J Psychiatry 2016;173:221‑31. Gainotti G, Azzoni A, Marra C. Frequency, phenomenology and anatomical‑clinical correlates of major post‑stroke depression. Br J Psychiatry 1999;175:163‑7. House A. Depression associated with stroke. J Neuropsychiatry Clin Neurosci 1996;8:453‑7. Katz IR. On the inseparability of mental and physical health in aged persons: Lessons from depression and medical comorbidity. Am J Geriatr Psychiatry 1996;4:1‑6. Villa RF, Ferrari F, Moretti A. Post‑stroke depression: Mechanisms and pharmacological treatment. Pharmacol Ther 2018;184:131‑44. Robinson RG, Price TR. Post‑stroke depressive disorders: A follow‑up study of 103 patients. Stroke 1982;13:635‑41. Robinson RG, Szetela B. Mood change following left hemispheric brain injury. Ann Neurol 1981;9:447‑53. Srivastava A, Taly AB, Gupta A, Murali T. Post‑stroke depression: Prevalence and relationship with disability in chronic stroke survivors. Ann Indian Acad Neurol 2010;13:123‑7. Gainotti G, Azzoni A, Razzano C, Lanzillotta M, Marra C, Gasparini F. hThe post‑stroke depression rating scale: A test specifically devised to investigate affective disorders of stroke patients. J Clin Exp Neuropsychol 1997;19:340‑56. Indian Journal of Psychiatry Volume 61, Issue 6, November-December 2019 Jana, et al.: Characteristics of poststroke depression 14. 15. 16. 17. Downloaded from http://journals.lww.com/indianjpsychiatry by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4 XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 07/22/2023 18. 19. 20. 21. 22. Quaranta D, Marra C, Gainotti G. Mood disorders after stroke: Diagnostic validation of the poststroke depression rating scale. Cerebrovasc Dis 2008;26:237‑43. Marin RS, Biedrzycki RC, Firinciogullari S. Reliability and validity of the apathy evaluation scale. Psychiatry Res 1991;38:143‑62. Ganguli M, Ratcliff G, Chandra V, Sharma S, Gilby J, Pandav R, et al. A Hindi version of the MMSE: The development of a cognitive screening instrument for a largely illiterate rural elderly population in India. Int J Geriatr Psychiatry 1995;10:367‑77. Folstein MF, Folstein SE, McHugh PR. “Mini‑mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189‑98. Singh G, Kaur D, Kaur H. Presumptive Stressful Life Event Scale. Agra: National Psychological Corporation; 1983. Holmes TH, Rahe RH. The social readjustment rating scale. J Psychosom Res 1967;11:213‑8. Overall JE, Gorham DR. Brief psychiatric rating scale. Psychol Rep 1962;10:799‑812. Patterson DA, Lee MS. Field trial of the global assessment of functioning scale – modified. Am J Psychiatry 1995;152:1386‑8. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994. 23. 24. 25. 26. 27. 28. 29. 30. Robinson RG, Kubos KL, Starr LB, Rao K, Price TR. Mood changes in stroke patients: Relationship to lesion location. Compr Psychiatry 1983;24:555‑66. Shimoda K, Robinson RG. The relationship between poststroke depression and lesion location in long‑term follow‑up. Biol Psychiatry 1999;45:187‑92. Jorge RE, Starkstein SE, Robinson RG. Apathy following stroke. Can J Psychiatry 2010;55:350‑4. Onoda K, Kuroda Y, Yamamoto Y, Abe S, Oguro H, Nagai A, et al. Post‑stroke apathy and hypoperfusion in basal ganglia: SPECT study. Cerebrovasc Dis 2011;31:6‑11. Robinson RG, Jorge RE, Clarence‑Smith K, Starkstein S. Double‑blind treatment of apathy in patients with poststroke depression using nefiracetam. J Neuropsychiatry Clin Neurosci 2009;21:144‑51. Nishio Y, Hashimoto M, Ishii K, Mori E. Neuroanatomy of a neurobehavioral disturbance in the left anterior thalamic infarction. J Neurol Neurosurg Psychiatry 2011;82:1195‑200. Ghika‑Schmid F, Bogousslavsky J. The acute behavioral syndrome of anterior thalamic infarction: A prospective study of 12 cases. Ann Neurol 2000;48:220‑7. Whyte EM, Mulsant BH. Post stroke depression: Epidemiology, pathophysiology, and biological treatment. Biol Psychiatry 2002;52:253‑64. New features on the journal’s website Optimized content for mobile and hand-held devices HTML pages have been optimized of mobile and other hand-held devices (such as iPad, Kindle, iPod) for faster browsing speed. Click on [Mobile Full text] from Table of Contents page. This is simple HTML version for faster download on mobiles (if viewed on desktop, it will be automatically redirected to full HTML version) E-Pub for hand-held devices EPUB is an open e-book standard recommended by The International Digital Publishing Forum which is designed for reflowable content i.e. the text display can be optimized for a particular display device. Click on [EPub] from Table of Contents page. There are various e-Pub readers such as for Windows: Digital Editions, OS X: Calibre/Bookworm, iPhone/iPod Touch/iPad: Stanza, and Linux: Calibre/Bookworm. E-Book for desktop One can also see the entire issue as printed here in a ‘flip book’ version on desktops. Links are available from Current Issue as well as Archives pages. Click on View as eBook Indian Journal of Psychiatry Volume 61, Issue 6, November-December 2019 611