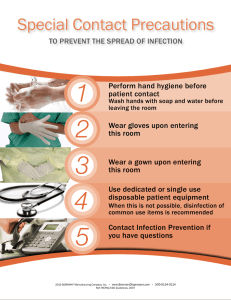
Hospital Infection Control: Basic Principles Infection Control Committee Goals for hospital infection control & prevention program 1. Protect the patients 2. Protect the HCW, visitors, and others in the healthcare environment. 3. cost effective and cost efficient. MMC Infection Control Committee • • • • • • • • • • • • • Nursing service Medicine (ICU/telemetry) Pediatrics (Nursery/PICU) Surgery (OR) OB-GYN (DR) IHC Pharmacy Laboratory Pulmonary Dietary Radiology Housekeeping Facility Management/Engineering Infection Control Committee Promote an adequate environment for the patient care program. Strives to minimize the hazards of hospital-associated infections by: prevention investigation reporting control The ICC has the following tasks: • • • • • Annual plan for infection control Infection control policies. Support the IC team & direct resources to address problems as identified Ensure availability of appropriate supplies Review epidemiological surveillance data & identify area for intervention. The ICC has the following tasks (cont): • • • • • Promote improved practice at all levels of the health care facility Training in infection control and safety. New technology & new devices Outbreak investigation Link with other committees ISOLATION PRECAUTIONS Guideline for Isolation Precautions in Hospitals Centers for Disease Control & Prevention Hospital Infection Control Practices Advisory Committee (January 1996; updated 2004) Isolation Precautions – 2-Level Approach: 1. Standard Precautions - primary strategy 2. Transmission-Based Precautions STANDARD PRECAUTIONS • reduce the risk of transmission of bloodborne pathogens • applies to all patients receiving care in hospitals, regardless of their diagnosis or presumed infection status. STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS a. Handwashing – between patient contacts – after touching blood, body fluids, secretions, excretions, and contaminated items – after gloves are removed Hand Hygiene Technique 1. Palm to Palm 4. Back of Fingers to opposing palms with fingers interlocked 2. Palm of Right hand over back of left hand & vice versa 5. Rotational rubbing of right thumb clasped in left palm and vice versa 3. Palm to Palm with fingers interlaced 6. Rotational rubbing, backwards and forwards with clasped fingers of right hand in left palm and vice versa STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS B. Clean & non-sterile gloves should be worn: – touching blood, body fluids, secretions, excretions, and contaminated items. – performing venipuncture & other vascular access procedures Wash hands after removing your gloves STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS Masks & protective eyewear, goggles or face shields should be worn during: – procedures that are likely to generate splashes/droplets of blood or other body fluids to prevent exposure of mucous membrane of the mouth, nose, & eyes. STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS D. Gowns or aprons should be worn during: – procedures that are likely to generate splashes of blood or other body fluids STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS Soiled patient-care equipment: - Wear gloves if visibly contaminated & practice routine hand hygiene Environmental Contact: - Follow procedure for routine care, cleaning & disinfection of environment surface, especially frequently touched surfaces in patient-care areas. STANDARD PRECAUTIONS Needles and other sharps: All HCW’s should take precautions to prevent injuries caused by needles, scalpel, & other sharp instruments or devices during procedures – when cleaning used sharp instruments – during disposal of used needles – when handling sharp instruments after procedures STANDARD PRECAUTIONS Sharps Injuries to prevent needle stick injuries, needles: – should not be recapped – should not be purposely bent or broken by hand – should not be manipulated by two hands (one hand scoop technique if required can be done) STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS Handling soiled or contaminated linens -Always use gloves when handling linen. -Inspect for needles, syringes, etc while stripping. -Linen should not be placed on the floor. -Soiled linen should be placed directly in the cloth hamper. -Contaminated linen should be placed in a yellow doubled plastic bag sealed by a knot. STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement h. Occupational Health & Bloodborne Pathogens To prevent injuries when using needles, scalpels, & other sharp instruments or devices Never recap used needles Place used disposable syringes & needles, scalpel blades, & other sharp items in appropriate puncture-resistant containers for transport to reprocessing area. Use mouthpieces, resuscitation bags as an alternative to mouth-to-mouth resuscitation methods in areas where the need for resuscitation is predictable. STANDARD PRECAUTIONS a. b. c. d. e. f. g. h. i. Handwashing Gloves Mask, Eye Protection, Face Shield Gown Patient Care Equipment Environmental Control Linen Occupational Health & Bloodborne Pathogens Patient Placement STANDARD PRECAUTIONS Patient Placement: - Prioritize for single-patient room if at increase risk of transmission of infection - Likely to contaminate the environment STANDARD PRECAUTIONS Respiratory Hygiene / Cough Etiquette (new TB guideline) - Instruct symptomatic person to cover mouth/nose when sneezing/coughing - Use tissue and dispose properly and avoid touching the receptacle bin - Observe hand hygiene after soiling of hands with respiratory secretions RESPIRATORY ETIQUETTE Isolation Precautions – 2-Level Approach: 1. Standard Precautions 2. Transmission-Based Precautions - Applied to selected patients based on suspected or confirmed diagnosis - Always implemented in conjunction with Standard Precautions Transmission- based precautions Based on 3 major modes of transmission: – Airborne Precaution – Droplet Precaution – Contact Precaution Some diseases may require more than one isolation category Indications for Transmission-based Precautions Known or Suspected Diseases or Pathogens Airborne – Measles – Tuberculosis, pulmonary or laryngeal – Varicella – Zoster (disseminated or immunocompromised patient) – SARS – Viral hemorrhagic fever Scenarios Requiring Airborne Precautions – Vesicular rash – Maculopapular rash + coryza + fever – Cough, fever, upper lobe pulmonary infiltrate – Cough, fever, any pulmonary infiltrate in an HIV patient (or patient at risk for HIV) Airborne Precautions Private room, keep door closed at all times Negative air-pressure ventilation, externally exhausted or HEPA filtered air if recirculated Fitted respirator masks (N95 respirator) worn by susceptible HCW Susceptible HCW should wear mask or avoid entering room Patient should wear mask when transported out of isolation room DROPLET PRECAUTIONS Use for patients known or suspected to be infected with organisms transmitted by respiratory droplet (large particle >5um in size) that can be generated by the patient during coughing, sneezing and talking on the performance of cough inducing procedures. Known or Suspected Diseases or Pathogens Droplet – Diphtheria (pharyngeal), Pertussis – Meningococcal infections – HI meningitis, epiglottitis, pneumonia – Influenza – Mumps, Rubella (postnatal) – Mycoplasma pneumonia – Parvovirus B19 – Adenovirus (infants, children) – Streptococcal (group A) pharyngitis, pneumonia, scarlet fever Scenarios Requiring Droplet Precautions – Meningitis – Petechial or ecchymotic rash with fever – Paroxysmal or severe persistent cough (periods of pertussis activity) Droplet Precautions Private Room, may cohort patients with same diseases; if not possible have a distance of 3 feet between patients and visitors Patient should leave the room only when necessary; If patient required to leave the room, must wear a surgical mask Use mask (standard surgical mask) if within 3 feet of patient Contact Transmission Two Modes: – Direct- body surface to body contact and physical transfer of micro-organisms; when doing physical exam, turning patients, giving the patient a bath, etc – Indirect- contact of a susceptible host with a contaminated intermediate object (needles, instruments, dressings, hands) Scenarios Requiring Contact Precautions – Acute diarrhea – Vesicular rash – Respiratory infections in infants & young children – History of infection/colonization with MDR organisms – Skin, wound or UT infection in patient with recent hospital or nursing home stay – Abscess or draining wound that cannot be covered Known or Suspected Diseases or Pathogens Contact 1. Abscess (drainage not contained) 2. Adenovirus (infants, children) 3. Clostridium difficile intercolitis 4. Conjunctivitis, acute viral 5. Escherichia coli 0157:h7 colitis 6. Furunculosis (infants, children) 7. Grp A Streptococcal major skin, burn or wound infection 8. Hepatitis A Known or Suspected Diseases or Pathogens Contact 9. HSV (neonatal, disseminated, severe primary mucocutaneous) 10. Impetigo 11. MDR bacteria (e.g. MRSA, VRE, GISA, GRSA) infection or colonization 12. Parainfluenza infection (infants, children) 13. Rotavirus 14. Rubella, congenital 15. Shigella (diapered/incontinent patients) 16. Varicella 17. Zoster (disseminated/immunocompromised) Contact Precautions Private room; cohorting permissible (Ensure that the patient are physically separated (>3 feet) from each other and provide curtain) Clean, nonsterile gloves at all times Handwashing after glove removal Gowns at all times, unless patient is continent and contact of clothing with patient or environmental surfaces is not anticipated Remove gloves and gowns before leaving room Essential Elements of Isolation Precautions Airborne Room -Negative pressure Private room w/ air exhausted to outdoors or thru high-efficiency filtration -Door kept closed Droplet -Private room -Door may remain open Contact -Private room - Dedicate use of non-critical patient-care items to a single patient Essential Elements of Isolation Precautions Airborne Mask -N95 Mask/ Portable Respirator for those entering room -Surgical mask on patient for transport outside room Droplet Contact -For entering room surgical mask on patient for transport outside room X Essential Elements of Isolation Precautions Gloves Airborne Droplet X X Contact -when entering room *When touching blood, body fluids, secretions, excretions, contaminated items, mucous membranes, non-intact skin, remove promptly after use or before touching non-contaminated items & before next patient. Essential Elements of Isolation Precautions Airborne Droplet Gown X X Contact -if clothing will contact patient, surfaces, items in room -if patient has diarrhea, ileostomy, colostomy, uncontained wound drainage -remove gown before leaving the room Essential Elements of Isolation Precautions Face Shield/ Eye Protection -For procedures/activities likely to generate splashes/sprays of blood, body fluids, secretions/excretions Transmission-Based Precautions for Hospitalized Patients Category Single Room Mask Gown Gloves AIRBORNE Yes, neg. air P vent Yes No No DROPLET Yes* No No CONTACT Yes* Yes, for close contact No Yes Yes *Cohorting acceptable 1 A 20-yr old employee was admitted for blood-streaked sputum & weight loss. Chest-xray showed Cavitary Pulmonary Tuberculosis. Facts about Tuberculosis etiologic agent: mycobacterium tuberculosis mode of transmission: respiratory droplet nuclei <5um or dust particles containing infectious agent how transmitted: inhalation of infectious particles which remain suspended in air and travel long distances duration of infectiousness: until 3 consecutive sputum smears are afb (-) or until 2-4 weeks after anti-tb drugs with good response 2 A 60-yr old woman was brought to the emergency room with the following pertinent PE findings: fever (T=39OC), shallow respiration with petechial and violaceous purpuric skin lesions on her lower extremities. The physician immediately suspected Meningococcemia. The patient became apneic and hypotensive and went into cardio-pulmonary arrest. Facts about Meningococcemia Etiologic agent: Neisseria meningitidis Mode of transmission: DROPLET How transmitted: Droplets containing organisms propelled short distances (<3ft), deposited on host’s conjunctivae, nasal mucosa, mouth Duration of infectiousness: until 24 hours after initiation of effective antibiotic therapy 3 A 15-yr old student was admitted for fever, loss of appetite, nausea and generalized body weakness. On physical examination, he had icteric sclerae and enlarged tender liver. He was diagnosed to have Hepatitis A infection. Facts about Hepatitis A Etiologic agent: Hepatitis A virus Mode of transmission: FECAL-ORAL How transmitted: Ingestion of contaminated food or water Duration of infectiousness: 1-2 weeks before onset of illness until 1 week after onset of jaundice 4 A 6-yr old boy developed low grade fever and vesicular rash on the face, chest and extremities. Onset of illness was 2 days after admission to the wards. The patient was diagnosed to have Varicella. Facts about Varicella Etiologic agent: Varicella virus Mode of transmission: CONTACT and AIRBORNE How transmitted: Direct contact with skin lesions, indirect contact with contaminated items or surfaces, airborne spread of respiratory tract secretions Duration of infectiousness: 48 hours prior to skin rash until all vesicles have crusted What Type of PPE Would You Wear? Giving a bed bath? Suctioning oral secretions? Transporting a patient in a wheel chair? Responding to an emergency where blood is spurting? PPE Use in Healthcare Settings What Type of PPE Would You Wear? Drawing blood from a vein? Cleaning an incontinent patient with diarrhea? Irrigating a wound? Taking vital signs? PPE Use in Healthcare Settings What Type of PPE Would You Wear? Giving a bed bath? Generally none Suctioning oral secretions? Gloves and mask/goggles or a face shield – sometimes gown Transporting a patient in a wheel chair? Generally none required Responding to an emergency where blood is spurting? Gloves, fluid-resistant gown, mask/goggles or a face shield PPE Use in Healthcare Settings Drawing blood from a vein? Gloves Cleaning an incontinent patient with diarrhea? Gloves w/wo gown Irrigating a wound? Gloves, gown, mask/goggles or a face shield Taking vital signs? – Generally none INFECTION CONTROL is…