Paclitaxel: Properties, Pharmacology, and Pharmacokinetics
advertisement

PACLITAXEL
INTRODUCTION
About cancer treatment in general
Cancer is a complex and multifactorial disease caused by a combination of genetic and epigenetic
changes within cells, altered apoptosis mechanisms, and changes in telomerase enzyme activity.
Cancer can be caused by a variety of factors, including exposure to external agents such as
radiation, chemicals, and pathogens, as well as internal factors such as hormones, mutations,
immune conditions, and aging. Identifying the specific triggers that initiate cancer in an individual
can be difficult, as it is often a combination of several factors. Contact inhibition, a mechanism
that regulates normal cell growth and division, is absent in many types of cancer cells. While
programmed cell death is a protective barrier to tumorigenic growth, elevated levels of oncogenic
signals and shortening of telomeric DNA sequences can cause tumorigenesis. Cancer is a leading
cause of death worldwide, responsible for about 9.6 million deaths in 2018 and projected to cause
13.2 million deaths by 2030, with developing nations being at greater risk. Effective prevention
and treatment strategies for cancer include maintaining a healthy lifestyle, avoiding carcinogens,
getting vaccinated against cancer-causing viruses, and undergoing regular cancer screenings.
Treatment options vary depending on the type and stage of cancer and may include surgery,
chemotherapy, radiation therapy, immunotherapy, targeted therapy, and palliative care.
Understanding the various factors that contribute to cancer can help in developing effective
prevention and treatment strategies.
Cancer is a rapidly emerging multifactorial disease that affects over 80% of people globally.
Surgery, radiotherapy, and chemotherapy are the most common treatments for controlling cancer,
but they can induce adverse side effects that vary between patients. Combining these treatments
has been found to be more effective. Selecting the best cancer therapy approach depends on various
factors such as the type of cancer, growth stages, age, management frequencies, quantity of
medicines, and healthiness of patients. To overcome the adverse side effects of these traditional
treatments, advanced techniques such as immunotherapy, hormone therapy, gene therapy, and stem
cell therapy can be used. Combining traditional and advanced treatments can increase the chances
of curing cancer and prevent relapses.
Paclitaxel, also known as Taxol, is an anti-mitotic drug derived from the Pacific yew tree. It was
discovered in a plant-screening program for new anti-cancer agents and was found to have a unique
mechanism of action that targets microtubule assembly. Taxol was approved by the FDA in 1992
for treating ovarian cancer and in 1994 for breast cancer. It is now used as a single chemotherapy
agent or combined with other drugs for treating ovarian cancer, breast cancer, and non-small-cell
lung cancer.
PART 1: PACLITAXEL PROPERTIES
I.
General properties
1.
Background
Taxol was discovered in 1963 in the bark of the T. Brevifolia tree and was found to have cytotoxic
activity against many types of cancer. However, the low yield and scarcity of Taxol in nature made
it difficult to extract and meet the demand for the drug. To overcome these issues, a semi-synthetic
method was proposed and approved by the FDA in 1992, which is now extensively used for bulk
production. Taxus species have become endangered, and Taxol is found only in mature trees, which
yield low content of Taxol. Currently, seedling cultures and improving forestation are considered
the best practical approaches to produce Taxol and precursors required for its chemical synthesis.
The biosynthesis pathway of toxoids is similar in all Taxus species and their tissues. Genetically
improved Taxus species producing high content of Taxol in needles provide a good option for
large-scale production.
Generic
Name:
Paclitaxel
Brand
names:
Taxol,
Abraxane
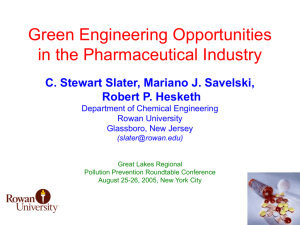
IUPAC name: (2α,4α,5β,7β,10β,13α)-4,10-Bis(acetyloxy)-13-{[(2R,3S)-3-(benzoylamino)-2hydroxy-3-phenylpropanoyl] oxy}-1,7-dihydroxy-9-oxo-5,20-epoxytax-11-en-2-yl benzoate
Chemical Formula: C47H51NO14
Chemical Structure:
2.
Physical Properties
3.
Chemical Properties
Paclitaxel, better known as Taxol, is a complex diterpenoid compound. Taxol has two molecules;
(a) a taxane ring containing four-membered oxetane side ring positioned at C4 and C5, and (b) a
homochiral ester side chain positioned at C13, which is the active site of the compound, and
attaches to microtubules, stabilizes the tubulin proteins, and activates tubulin depolymerization in
GTP (guanosine triphosphate) independent manner. The taxane ring system is a complex
tetracyclic structure that contains several functional groups, including an ester, a carbamate, and
an oxetane ring.
Paclitaxel is a lipophilic compound and is insoluble in water but soluble in organic solvents, such
as ethanol and methanol. Its solubility can be increased by formulating it with a solvent, such as
Cremophor EL and ethanol. However, this formulation can cause side effects, such as
hypersensitivity reactions, due to the toxicity of Cremophor EL.
Paclitaxel is a microtubule-stabilizing agent that works by binding to the beta-subunit of tubulin,
a protein that is essential for the formation of microtubules. By binding to tubulin, paclitaxel
prevents the disassembly of microtubules, resulting in cell cycle arrest and apoptosis (programmed
cell death).
Paclitaxel is a chiral compound, which means that it exists in two mirror-image forms, or
enantiomers. The two enantiomers of paclitaxel are designated as R-paclitaxel and S-paclitaxel.
R-paclitaxel is the active form of the drug, while S-paclitaxel is inactive. The separation of the two
enantiomers of paclitaxel is important for understanding the pharmacokinetics and
pharmacodynamics of the drug.
Paclitaxel undergoes extensive metabolism in the liver by the cytochrome P450 enzyme system,
particularly the CYP3A4 isoform. The major metabolites of paclitaxel are 6alphahydroxypaclitaxel and 3'-p-hydroxypaclitaxel, which are less active than the parent compound.
In summary, paclitaxel is a lipophilic, microtubule-stabilizing agent with a complex chemical
structure that consists of a taxane ring system with a side chain at the C-13 position. Its solubility
can be increased by formulation with a solvent, such as Cremophor EL and ethanol. Paclitaxel is
a chiral compound, and its active form is R-paclitaxel. The drug is extensively metabolized in the
liver by the cytochrome P450 enzyme system.
II.
Pharmacology:
1.
Indication:
In 1992, Taxol was approved and registered by The Food and Drug Administration (FDA) for
treating ovarian cancer in 1992 and for breast cancer in 1994. It is now used either as a single
chemotherapeutic agent or combined with other chemo-drugs for treating ovarian cancer, breast
cancer and non-small-cell lung cancer.
Also used in the treatment of Kaposi's sarcoma. Abraxane® is specfically indicated for the
treatment of metastatic breast cancer and locally advanced or metastatic non-small cell lung cancer.
2.
Pharmacokinetics:
(Absorption, distribution, metabolism, elimination/excretion; bioavailability)
a.
Absorption
Low oral bioavailability [PO] f<10%
Paclitaxel is an antineoplastic drug used to treat various types of cancer. Unfortunately, it has a
very low level of oral bioavailability, at less than 10%. This means that when taken orally, only
a small amount of the drug reaches the bloodstream.
Paclitaxel is currently administered as an intravenous infusion, owing to its low oral
bioavailability. Several attempts have been made to develop oral paclitaxel formulations; however,
there are currently no oral paclitaxel-based products available on the market and oral
administration has not been studied in humans.
Besides, several studies have been conducted to improve the oral bioavailability of paclitaxel. One
study found that the relative oral bioavailability of paclitaxel-loaded nanosponges was 256.
Another study used glycyrrhizic acid as a carrier to improve the oral bioavailability of paclitaxel.
When a 24-hour infusion of 135 mg/m^2 is given to ovarian cancer patients, the maximum plasma
concentration (Cmax) is 195 ng/mL, while the AUC is 6300 ng•h/mL.
Following intraperitoneal administration of paclitaxel to patients with ovarian cancer, mean plasma
concentrations were reported to be 1000- to 3000-fold lower than those measured in the
peritoneum during the first 48 hours post instillation. However, plasma concentrations (0.19 to
0.47 𝜇 mol/L) 30 to 60 minutes post-instillation in patients administered 175 mg/m2 were
equivalent to concentrations achieved following 24-hour intravenous infusions of identical
dosages.
The peak plasma concentrations of paclitaxel achieved during 6- and 24-hour infusions are in the
range of drug concentrations capable of inducing significant biologic and cytotoxic effects in vitro
(0.1-10 umol/l.).' Plasma concentrations increase throughout the infusion, suggesting a long halflife; values reach a peak at the end of the infusion, and start to decline immediately upon cessation
of therapy (Figures 3.1 and 3.2).9,10 Peak plasma concentrations are proportional to the paclitaxel
dose. At the recommended dosage of 135 mg/m', administered as a 24-hour infusion, a
concentration of 0.3-0.4 umol/L should be achieved.
Formulation
As a result of the poor aqueous solubility of paclitaxel, the development of a suitable formula tion
for human administration was difficult. The formulation that resulted and is currently available
solubilises paclitaxel (6 mg/ml) in a l:l (v/v) solution of polyoxyethylated castor oil (,Cremophor
EL') and dehydrated alcohol, USP.
Paclitaxel is formulated in a mixture of ethanol and Cremophor EL (polyethoxylated castor oil).
Cremophor reduced the electrophoretic mobility of serum lipoproteins along with the appearance
of a lipoprotein dissociation product. After serum was exposed to Cremophor in vitro or in vivo
there was substantial binding of paclitaxel to the lipoprotein dissociation product(s), and this could
represent an important factor in the distribution of paclitaxel [11].
b.
Distribution
It has been consistently demonstrated in human pharmacokinetic studies that paclitaxel has a very
large volume of distribution at steady state (Vss = 50 to 400 L/m2, but this is reduced in the
females). In steady state, Volume of distribution is 5-6 liters per kg of body weight, 67.1 L/m2 in
1 to 6-hour infusion and about 227 to 688 L/m2 [apparent volume of distribution at steady-state,
24-hour infusion], shows extensive extravascular diffusion and/or high binding with tissue
components. Paclitaxel is highly bound by plasma proteins, primarily albumin. Initial in vitro
studies using either equilibrium dialysis or ultracentrifugation methods have provided estimates
that 95 to 98% of paclitaxel is bound to human plasma proteins.
Recently, it has been reported that unbound paclitaxel may bind significantly to dialysis filtration
devices, such that the amount of paclitaxel detected in dialysate could be reduced, falsely elevating
estimates for plasma protein binding. After modification of their methods, these investigators have
reported one of the lowest estimates of average paclitaxel plasma protein binding at 88%, a
value that nevertheless represents substantial plasma protein binding. The presence of
cimetidine, ranitidine, dexamethasone, or diphenhydramine did not affect protein binding of
paclitaxel.
Although paclitaxel distributes fast in tissue and body fluid and binds extensively to plasma
proteins (89-98%), it is readily cleared from plasma. It has large volumes of distribution, owing
to its association with microtubules.
There is a study involving a single adult patient who received a 24-hour infusion of paclitaxel,
where the CSF concentrations of the drug were undetectable at the end of the infusion, while
plasma concentrations were 2.7 μmol/L. Most studies on paclitaxel infusions of different durations
have used a first-order 2-compartment model to analyze the data. However, a recent study
suggested the presence of a third compartment in a 24-hour infusion, possibly due to improved
assay sensitivity. In children receiving 24-hour paclitaxel infusions, a 2-compartment model
incorporating a saturable distribution process was found to be the most accurate in describing the
drug concentrations during the infusion. The drug concentrations gradually increased during the
infusion but decreased rapidly after the infusion ended, indicating rapid systemic clearance. This
discrepancy between intra-infusion and post-infusion drug disposition couldn't be adequately
explained by the first-order 2-compartment model. Other studies have also observed similar
plasma concentration patterns after 24-hour paclitaxel infusions, suggesting the presence of
saturable distribution in adults as well.
The systemic clearance of paclitaxel is on average 350mL/min/m2 and of docetaxel is
300mL/min/m2
Terminal half-life has ranged from 1.3 to 8.6 hours (mean 5 hours) [40, 93], and total body
clearance has ranged from 11.6 to 24.0 L/hr/m2. Preclinical results in animals have shown high
levels in most tissues. Being highly protein-bound, paclitaxel has a high affinity for distribution in
specific tissues including kidney, lung, spleen, and extracellular fluids like ascites and pleural
fluids [40, 95] but the uptake of the drug in the brain is minimal. Exposure to paclitaxel is relatively
high in tumour tissue compared with other tissues, and in addition to slow elimination from tumor
tissue, the AUC in tumour tissue is about five-fold higher than that in plasma [97].
c.
Metabolism
Less than 5 to 10% of administered paclitaxel was recovered as unchanged drug in the urine of
treated patients. Moreover, possible metabolites of paclitaxel have not been observed in the urine
of treated rats and humans. On the basis of these findings, alternative explanations for plasma
paclitaxel disappearance were investigated (e.g. hepatic metabolism, biliary excretion, extensive
tissue binding).
Hepatic.
After intravenous administration of paclitaxel, 90% the drug undergoes an extensive P-450
mediated hepatic metabolism by cytochrome enzymes (CYP3A and CYP2C8).
In vitro studies with human liver microsomes and tissue slices showed that paclitaxel was
metabolized primarily to 6a-hydrox-ypaclitaxel by the cytochrome P450 isozyme CYP2C8; and
to two minor metabolites, 3’-p-hydroxypaclitaxel and 6a, 3’-p-dihydroxypaclitaxel, by CYP3A4.
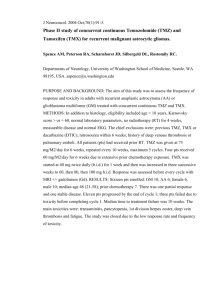
Paclitaxel
6α-hydroxypaclitaxel (type of reaction: Aliphatic hydroxylation) _CYP2C8
6α, 3'-p-dihydroxypaclitaxel (type of reaction: ……) _ CYP3A4
3′-p-hydroxypaclitaxel (type of reaction: Aromatic hydroxylation) _ CYP3A4
d.
Elimination
About 70–80% of the drug being excreted into bile by adenosine triphosphate- (ATP-) binding
cassette multidrug transporters such as P-glycoprotein (P-gp) and multidrug resistance protein 2
(MRP-2), either as metabolites or as the parent drug. Variation in MRP-2 activity has been found
to have direct effect on the effective exposure to paclitaxel. The bioavailability is poor following
oral administration due to enterocyte expression of P-gp and first-pass metabolism in the liver.
Most of the drug is eliminated in feces.
Less than 10% drug in the unchanged form is excreted in the urine, indicating extensive nonrenal
clearance. (excreted in feces ~ 70%, of which 5% is the unchanged form).
Eg: In 5 patients administered a 225 or 250 mg/m2 dose of radiolabeled paclitaxel as a 3-hour
infusion, a mean of 71% of the radioactivity was excreted in the feces in 120 hours, and 14% was
recovered in the urine.
Renal clearance contributes minimally (less than 10%) to overall clearance of paclitaxel; thus, dose
modification does not appear to be necessary in patients with renal dysfunction.
When a 24-hour infusion of 135 mg/m^2 is given to ovarian cancer patients, the elimination
half=life is 52.7 hours.
Clearance: Clearance at 1 to 6 hours infusion time is 5.8 to 16.3 liters/hour/m2 and in the case of
a 24-hour infusion 14.2 up to 17.2 liters/hour/m2. More detail:
21.7 L/h/m2 [Dose 135 mg/m2, infusion duration 24 h]
23.8 L/h/m2 [Dose 175 mg/m2, infusion duration 24 h]
7 L/h/m2 [Dose 135 mg/m2, infusion duration 3 h]
12.2 L/h/m2 [Dose 175 mg/m2, infusion duration 3 h]
3.
Drug interaction
Paclitaxel has no known severe interactions with other drugs.
Serious interactions of paclitaxel include:
adenovirus types 4 and 7 live, oral
eluxadoline
idarubicin
idelalisib
influenza virus vaccine trivalent, adjuvanted
ivacaftor
nefazodone
palifermin
quinidine
Paclitaxel has moderate interactions with at least 98 different drugs.
Paclitaxel has mild interactions with at least 81 different drugs.
a.
Drug–drug interactions
Drug interactions with paclitaxel have been reviewed. The most important of these are the
pharmacodynamic interactions with other cytostatic drugs, but pharmacokinetic interactions have
also been described.
Drug–drug interactions (DDIs) affecting the pharmacokinetics of paclitaxel have not been
systematically studied, likely because of ethical considerations of testing potentially harmful DDIs
in cancer patients. Clinicians often extrapolate from case observations, in vitro data, and limited
epidemiological studies to optimally manage polytherapy during cancer treatment.
Paclitaxel is metabolized by the cytochrome P450 isoenzymes CYP2C (CYP2C8, CYP2C9) and
CYP3A4, and drugs that inhibitor induce these isoenzymes would be expected to alter
themetabolism of paclitaxel. In vitro ranitidine, diphenhydramine, vincristine, vinblastine, and
doxorubicin had little orno effect on the metabolism of paclitaxel, but barbiturates stimulated
hydroxylation of the sidechain by induction of CYP3A isoforms but ketoconazole, verapamil,
diazepam, quinidine, dexamethason, cyclosporine, teniposid, etoposid, and vincristine, protease
inhibitors that inhibit the metabolism and elimination of paclitaxel. In contrast, cytochrome P450
inducers or isoenzymes CYP2C8, CYP2C9, CYP3A4 will decrease the concentration of paclitaxel
in the blood, such as the anticonvulsants phenobarbital, phenytoin.
EXAMPLE
With other anticancer agents, drug interactions may occur depending on the drug used in
combination with paclitaxel. Cisplatin (usually administered after paclitaxel) if administered first
reduces renal excretion of paclitaxel by 20 to 25% and increases bone marrow suppression.
Taking paclitaxel with doxorubicin will increase blood levels of doxorubicin, increasing its
anticancer effectiveness but also increasing undesirable effects on the heart.
Anthracyclines
The combination of doxorubicin plus paclitaxel is cardiotoxic. Various authors have suggested that
after a median cumulative dose of 480 mg/m2, 50% of patients will have a reduced left ventricular
ejection fraction and 20% will develop congestive heart failure.
In 36 women with previously untreated metastatic breast cancer, paclitaxel dose-dependently
increased the plasma concentrations of doxorubicin and its metabolite doxorubicinol; this was
attributed to competition for biliary excretion of taxanes and anthracyclines mediated by P
glycoprotein. Two studies of the combination of epirubicin plus paclitaxel have shown less
reduction in left ventricular ejection fraction and no clinical evidence of cardiac failure.
Ketoconazole
In patients with ovarian cancer, ketoconazole, 100– 1600 mg as a single oral dose 3 hours after
paclitaxel 175 mg/m2 as a 3-hour continuous intravenous infusion, did not alter plasma
concentrations of paclitaxel or its principal metabolite, 6-alpha-hydroxypaclitaxel.
Platinum-containing cytotoxic drugs (carboplatin)
In 21 patients with advanced non-small cell lung cancer carboplatin had no effect on the
pharmacokinetics of paclitaxel 135–200 mg/m2 as a 24-hour intravenous infusion. Peripheral
neuropathy occurred in 13 of 37 patients treated with paclitaxel 175 mg/m2 and carboplatin. The
authors concluded that clinically important neurotoxicity increases with every cycle of
chemotherapy. The peripheral neuropathy mainly affected sensory fibers without involving motor
nerves. The same paclitaxel/carboplatin chemotherapy in 28 women caused no signs of acute
central neurotoxicity or neuropsychological deterioration; however, 11 patients had a peripheral
neuropathy.
Clopidogrel
For example, a metabolite of clopidogrel that inhibits CYP2C8 in vitro was linked to a very low
CL of paclitaxel and increased risk of neuropathy in an ovarian cancer patient. This was later
supported by a small case series in which seven out of eight patients treated with clopidogrel and
paclitaxel experienced grade 3 neutropenia. More recently, 48 patients treated with paclitaxel and
clopidogrel were found to have increased rates of neuropathy compared with a control group of 88
patients using low-dose aspirin in place of clopidogrel. The study concluded that the risk of
peripheral neuropathy is approximately two-fold higher in patients using clopidogrel and paclitaxel
in doses of 135 mg/m2 or greater.
Patient characteristics and background are shown in Table I. A total of 5 patients received paclitaxel
and clopidogrel concomitantly. The therapeutic regimen for the patients included was carboplatin
(nedaplatin) + paclitaxel (4 cases), paclitaxel alone (1 case), carboplatin + paclitaxel + radiation
therapy (2 cases), or carboplatin + paclitaxel (1 case). A total of 8 cases were analyzed. The only
drug used that influences CYP2C8 was clopidogrel. None of the 8 cases had any notable problems
regarding blood cell counts prior to chemotherapy.
b.
Food Interactions
Avoid echinacea. Co-administration may decrease the effectiveness of
immunosuppressants, and echinacea may induce CYP3A4 increasing paclitaxel metabolism.
Exercise caution with grapefruit products. Grapefruit inhibits CYP3A4 metabolism, which
may increase the serum concentration of paclitaxel.
Exercise caution with St. John's Wort. This herb induces the CYP3A4 metabolism of
paclitaxel and may reduce its serum concentration.
Using this medicine with any of the following medicines is not recommended. Doctor may decide
not to treat you with this medication or change some of the other medicines you take.
Measles Virus Vaccine, Live
Mumps Virus Vaccine, Live
Rotavirus Vaccine, Live
Rubella Virus Vaccine, Live
Varicella Virus Vaccine, Live
Zoster Vaccine, Live
Using this medicine with any of the following medicines is usually not recommended but may be
required in some cases. If both medicines are prescribed together, Doctor may change the dose or
how often you use one or both medicines.
Abametapir
Abiraterone Acetate
Adenovirus Vaccine
Amiodarone
Bacillus of Calmette and Guerin
Vaccine, Live
Bexarotene
Candesartan
Carbamazepine
Ceritinib
Cholera Vaccine, Live
Cisplatin
Clopidogrel
Conivaptan
Crizotinib
Dabrafenib
Dengue Tetravalent Vaccine, Live
Doxorubicin
Doxorubicin Hydrochloride Liposome
Ethinyl Estradiol
Fedratinib
Fexinidazole
Fluconazole
Fosnetupitant
Fosphenytoin
Idarubicin
Dalfopristin
Lapatinib
Infliximab
Influenza Virus Vaccine, Live
Itraconazole
Ketoconazole
Leflunomide
Mitapivat
Netupitant
Nilotinib
Omaveloxolone
Oxcarbazepine
Pazopanib
Phenobarbital
Phenytoin
Pirtobrutinib
Pixantrone
Poliovirus Vaccine, Live
Selpercatinib
Smallpox Vaccine
St John's Wort
Taurursodiol
Teriflunomide
Testosterone
Tretinoin
Typhoid Vaccine, Live
Valspodar
Yellow Fever Vaccine
Quinupristin
Using this medicine with any of the following medicines may cause an increased risk of certain
side effects, but using both drugs may be the best treatment for you. If both medicines are
prescribed together, doctor may change the dose or how often you use one or both medicines.
c.
Other Interactions
Certain medicines should not be used at or around the time of eating food or eating certain types
of food since interactions may occur. Using alcohol or tobacco with certain medicines may also
cause interactions to occur. Discuss with your healthcare professional the use of your medicine
with food, alcohol, or tobacco.
What drugs and food should I avoid while taking Paclitaxel (Taxol)?
Paclitaxel contains alcohol and may cause a drunken feeling when the medicine is injected
into your vein. Avoid drinking alcohol on the day of your paclitaxel injection.
Avoid being near people who are sick or have infections. Tell your doctor at once if you
develop signs of infection.
Avoid activities that may increase your risk of bleeding or injury. Use extra care to prevent
bleeding while shaving or brushing your teeth.
4.
Pharmacodynamics:
a. Mechanism of action of paclitaxel:
* General mechanism: Paclitaxel is an antimicrotubule agent. It promotes the assembly of
microtubules by enhancing the action of tubulin dimers and stabilizing current microtubules while
inhibiting their disassembly. Due to the stability of the microtubules, the late G2 phase stops, and
cell replication becomes inhibited. Paclitaxel may also distort mitotic spindles causing the
chromosomes to break.
* Biological background:
- Microtubule:
+ The largest largest of the three types of cytoskeletal fibers (In eukaryotes)
+ A microtubule is made up of tubulin proteins arranged to form a hollow, straw-like tube, and
each tubulin protein consists of two subunits, α-tubulin and β-tubulin (~25 to 30nm in diameter).
+ Play a significant role in forming the mitotic spindle fibers during cellular divisions. Also, they
offer stability to cell organization and cytoplasmic movement inside the cell.
- Cytoskeleton:
+ A complex, dynamic network of interlinking protein filaments present in the cytoplasm of all
cells, including those of bacteria and archaea. In eukaryotes, it extends from the cell nucleus to the
cell membrane and is composed of similar proteins in the various organisms. It is composed of
three main components, microfilaments, intermediate filaments and microtubules, and these are
all capable of rapid growth or disassembly dependent on the cell's requirements
+ The cytoskeleton organizes other constituents of the cell, maintains the cell’s shape, and is
responsible for the locomotion of the cell itself and the movement of the various organelles within
it.
- Cell cycle:
+ A cell cycle is a series of events that takes place in a cell as it grows and divides
+ Cell division: Cell division is the process by which a parent cell divides into two daughter cells.
In eukaryotes, there are two distinct types of cell division: a vegetative division (mitosis),
producing daughter cells genetically identical to the parent cell, and a cell division that produces
haploid gametes for sexual reproduction (meiosis), reducing the number of chromosomes from
two of each type in the diploid parent cell to one of each type in the daughter cells
b. Mechanisms of action against cancer:
* Paclitaxel (Taxol) induces mitotic cell cycle arrest: Taxol targets microtubules and causes its
polymerization and stabilization to disrupt mitotic cell in living cancer cells.
- Taxol induces microtubules stabilization: It hyper-stabilizes their structure. This destroys the
cell's ability to use its cytoskeleton in a flexible manner.
Paclitaxel disrupts the microtubules dynamic and induces cell apoptosis. It has a binding pocket in
β-tubulin, which binds to GTP molecule, the hydrolysis of GTP allows depolymerization of
microtubules.
(Tubulin is the "building block" of mictotubules, and the binding of paclitaxel locks these building
blocks in place. The resulting microtubule/paclitaxel complex does not have the ability to
disassemble. This adversely affects cell function because the shortening and lengthening of
microtubules (termed dynamic instability) is necessary for their function as a transportation
highway for the cell. Chromosomes, for example, rely upon this property of microtubules during
mitosis)
Taxol promotes the conformational changes in M-loop of β-tubulin, which results in stable lateral
interactions between proto-filaments, leading to prevention in the microtubule depolymerization
or also known as microtubules stabilization. The failure of chromosomes to attach with
microtubules halts the cell from proceeding to the next phase, disrupts the mitotic spindle assembly
which induces spindle assemble checkpoint (SAC), causing mitotic arrest which eventually will
end up in apoptosis . It is assumed that the consequence of microtubule dysfunctionality is the
G2/M phase arrest, which is needed for cell death in cancer.
- Mitotic slippage:
Cancer cells tend to resist the apoptotic effect of Taxol by escaping the mitotic arrest and induce a
premature exit from the mitosis process before the cell apoptosis happens. This escape plan of the
cancer cells is known as mitotic slippage which the cells exits mitosis and “slip” into tetraploid G1
phase as there is no proper chromosome segregation and cytokinesis. The subsequent event of
mitotic slippage is either the cells got arrested in G1 phase, post-slippage cell death, or continue
the cell cycle but in a genomically unstable mode. This highlights that the entry of cells into mitosis
is a prerequisite event for Taxol killing effect but the apoptosis is not limited to be occurring from
G2/M phase arrest only.
- Paclitaxel’s effect is dose-dependent:
+ Taxol had been claimed to exert different mitotic effects in low concentrations, it produces
aneuploidy cells in the absence of mitotic block. In vitro studies suggested that Taxol’s mechanism
is dose-dependent, and the Taxol-induced cell death could be independent from mitotic arrest.
+ In low concentration, Taxol utilized other pathways to inhibit cell proliferation without arresting
mitosis. (e.g. In A549 cells, at very low concentration of Taxol (3–6nM) it is insufficient to inhibit
mitotic cycle but it induced p53 and p21 proteins to cause the G1 and G2 arrest instead But at
higher concentrations (100nM) Taxol will predominantly activate G2/M phase arrest.)
+ At higher dosage, instead of inhibiting the microtubules depolymerization, Taxol increases
microtubules mass and number to cause its stabilization. Additionally, the high Taxol dosage was
also observed to regulate certain gene expressions or signaling pathways.
* Taxol induces gene-directed apoptosis:
Several apoptosis-related or survival signaling genes were shown to be activated by Taxol for
instance JNK, p34, NFκB, tumor necrosis factor-α (TNFα) and Bcl-2 proteins. One of the genedirected pathways that was extensively discussed for Taxol’s mechanism of action is the Bcl-2
family of proteins which are apoptotic regulators that control cell survival.
* Immunomodulation effects by Taxol:
Various studies had shown that Taxol has regulating effect on immune cells such as effector T cells
(Teff) , regulatory T cells (Treg), macrophages, dendritic cells and others. Taxol treatment has both
stimulatory and suppressive effects on the immune system, standard dose of Taxol is
immunosuppressive and inhibits a group of immune cells involved in tumor elimination. But lower
dose of Taxol exerts an opposite effect and promotes anti-tumor immunity which stimulated its
potential role in immunogenic effects. Thus, the understanding of the role of Taxol in
immunomodulation could potentially provide an improved therapeutic regimen for cancer
treatment.
c. Adverse effects of paclitaxel with systemic administration:
- Paclitaxel has a black box warning for hypersensitivity reactions and bone marrow suppression.
Patients should be premedicated with corticosteroids, diphenhydramine, and H2 antagonists prior
to infusion to avoid anaphylaxis and severe hypersensitivity reactions. The recommendation is for
dexamethasone at 20 mg IV or orally (10 mg if the patient has advanced HIV) 12 and 6 hours
before the paclitaxel dose. Diphenhydramine should be administered 30 to 60 minutes before the
dose at 50 mg IV. Cimetidine 300 mg, famotidine 20 mg, or ranitidine 50 mg would all be
appropriate choices to be administered IV at 30 to 60 minutes before the dose. Severe
hypersensitivity reactions would include dyspnea requiring bronchodilators, hypotension requiring
treatment, angioedema, and/or generalized urticaria. In cases of serious hypersensitivity reaction,
stop the infusion and discontinue paclitaxel. Minor hypersensitivity reactions do not require
treatment to be interrupted or discontinued. Minor hypersensitivity reactions would include
flushing, dyspnea, hypotension, skin reactions, or tachycardia.
- The most prevalent side effects of paclitaxel are alopecia, nausea and vomiting, mucositis,
neutropenia, leukopenia, anemia, hypersensitivity reactions, arthralgia, myalgia, and weakness.
Peripheral neuropathy is another common side effect, and patients with preexisting neuropathies
may have an increased risk. The dose should be reduced by 20% for patients who develop severe
neuropathy.
- Other less common side effects include flushing, edema, hypotension, skin rash, stomatitis,
thrombocytopenia, hemorrhage, increased serum alkaline phosphatase and AST, local injection
site reaction, increased serum creatinine, along with many more. Injection site reactions are
generally mild (erythema, tenderness, skin discoloration, or swelling) and tend to occur more often
with an extended infusion duration, for example, 24 hours. It is worth noting that delays of
injection site reactions can extend from 7 to 10 days. Patients may also experience infusion-related
hypotension, bradycardia, and/or hypertension. Due to that concern, the recommendation is that
the patient's vital signs undergo frequent monitoring, especially during the first hour of infusion.
The presentation and occurrence of adverse effects varies from patient to patient and is often
schedule dependent. Neutropenia,for example, is more frequent with 24-h infusions compared with
3-h infusions, but most frequent with 1-h infusions. Certain adverse effects (e.g., neutropenia) are
fairly common, whereas other adverse effects (e.g., bradycardia) tend to be rare. In addition, some
adverse effects may not be directly caused by paclitaxel itself. Biologic effects such as acute
hypersensitivity and peripheral neuropathies have been described as related to the CrEL vehicle
and are under investigation with CrEL-free formulations of paclitaxel. (Because cytotoxic drugs
like paclitaxel are often hydrophobic, toxic solubilizing agents such as Cremophor/ethanol (CrEL)
are often used to administer the drug.)
Clinical studies over the last 20 years have led to changes in the paclitaxel dosing and scheduling
regimens, namely reductions in infusion times and increases in dose density. Premedication with
steroids and histamine blockers has allowed for shorter infusion times (1 – 3 h). On the other hand,
infusion times < 1 h appear to increase the risk of severe anaphylactic shock.
Toxicity:
- Rat (ipr) LD50=32530 µg/kg. Symptoms of overdose include bone marrow suppression,
peripheral neurotoxicity, and mucositis. Overdoses in pediatric patients may be associated with
acute ethanol toxicity.
- Hyaluronidase is the antidote for paclitaxel and is commonly used for the treatment of
extravasation. If the needle/cannula is still in place, administer 1 to 6 mL into the existing IV line.
If the needle/cannula is no longer inserted, the hyaluronidase may be injected subcutaneously
clockwise around the area of extravasation. This procedure may be repeated several times over the
next 3 to 4 hours.
5.
Contraindication
Due to the black box warning for hypersensitivity reactions and bone marrow suppression,
paclitaxel should not be given to patients who have had a severe hypersensitivity reaction with
paclitaxel, patients with solid tumors who have a baseline neutrophil count of fewer than 1500
cells/mm^3, or patients with AIDS-related Kaposi sarcoma if the baseline neutrophil count is less
than 1000 cells/mm^3. Bone marrow suppression is dose-dependent and is a dose-limiting toxicity.
If it occurs, future doses should be reduced by 20% for severe neutropenia and consider supportive
therapy (growth factor treatment).
6.
Pharmacopoeia Standards:
Vietnameses National Drug Formulary 2018, page 1105-1108
International official name: Paclitaxel
Drug type: Anticancer, Taxane group
ATC code (Anatomical Therapeutic Chemical Code): L01CD01
o
L- Antineoplastic and Immunomodulating agents
o
L01 - Antineoplastic agents
o
L01C - Plant alkaloids and other natural products
o
L01CD - Taxanes
o
L01CD01 - paclitaxel includes solvent-based paclitaxel and paclitaxel albumin.
7.
Commercial product
Generic drug: Taxol by Bristol-Myers Squibb (patent expiration date 09/03/2013)
Recent commercial names: Anzatax; Canpaxel 30; Ciplaxel; Genepaxel Crem Less; Inoxel;
Intas Cytax 30; Intaxel; Kingxol; Mitotax; Paclirich; Paclitaxelum Actavis; Paclitaxin; Padexol;
Panataxel; Pastaxel; Pataxel; Paxus; Plaxel 30; Shu su.
(Images will be attached in slides)
Some typical commercial drugs:
Generic drug name
Manufacturer
Price (VND)
Anzatax
Pfizer
100mg:
3.800.000
30mg: 1.160.000
Canpaxel 30
Bidiphar
30mg: 700.000
Paclitaxin
Pharmachemie BV.
100mg: 1.700.000
Ciplaxel
Cipla., Ltd
Genepaxel Crem Less
Genovate Biotechnology Co.,
Ltd
Inoxel
Boryung Pharmaceutical Co.,
Ltd
Intas Cytax 30
Padexol
Intas Pharm., Ltd
Shin Poong Pharm Co., Ltd.
PART 2: SYNTHESIS METHODS
In the early years after marketed, Taxol was largely extracted from wild yew trees, its bark and
other parts. Leading pharmaceutical companies soon started large-scale farming of yew trees. By
now, extract of this chemical from raw tree materials is still playing a part in Taxol industry.
Unfortunately, Taxol makes up only a small proportion of the total taxoids in Taxus trees. Its
natural concentration is approximately 0.01% of a dry weight basis in Pacific yew.
I.
Total Synthesis:
Over the years, many approaches to the total synthesis of Taxol have appeared in the literature,
and Holton and Nicolaou, independently, have recorded successful approaches to this challenging
target. Due to the length of these approaches, the total synthesis of Taxol may not be feasible on
an industrial scale.
II.
Semi-synthesis:
To circumvent this problem, Greene, Potier and coworkers developed an efficient semi-synthetic
approach. The chemistry involves an enantioselective synthesis of (2'R, 3'S)a-hydroxy-~-amino
acid derivative 1.1.2 and its coupling to suitably protected 10-desacetylbaccatin III (10-DAB),
1.1.3, at the C-13 position. To date, the semi-synthetic approach appears to be the most practical
way of producing Taxol large scale. Since 10-DAB is isolated from the needles of the widely
distributed Taxus baccata (yield: ca. lg/Kg dry leaves), a renewable source of 10-DAB is available
in large quantities.
1.
Formulation of side chain (1.1.2):
2.
Coupling of side chain (1.1.2) to baccatin (1.1.3):
Coupling of 2.1.5 to baccatin was initially reported to be a very difficult operation, probably due
to the hindered nature of the C-13 hydroxyl group in baccatin. The C-2 hydroxyl group in 2.1.5
was protected as an acid-labile ethoxyethyl ether and the ester was hydrolyzed to the free amino
acid 2.1.10. Treatment of 7-triethylsilyl (TES) baccatin III (2.1.11) in toluene with 6 equiv of
2.1.10, 6 equiv of di-2-pyridyl carbonate (DPC), and 2 equiv of 4- (dimethylamino)pyridine
(DMAP) at 80 ~ for 100 h produced the C-2', C-7- protected 2.1.12 in 80% yield (yield based on
only 50% conversion). The protecting groups were removed by using 0.5% HC1 in ethanol to give
Taxol| in good yield (Scheme 3). This method suffers from two major drawbacks: esterification
required excess amounts of the expensive chiral amino acid (6 equiv or more) and only 50%
conversion was observed even under forcing conditions.
The esterification step was significantly improved by Commercon and co-workers. The
phenylisoserine side chain was introduced as an oxazolidine, 260 which underwent esterification
under standard DCC/DMAP coupling conditions in high yield [22]. The methodology avoided the
use of an excess of enantiomerically pure amino acid 1.1.2, and the coupling yield was over 90%.
The key intermediate was again a chiral epoxide (2.1.15, a homolog of 2.1.2), which was
synthesized by condensation of the boron enolate of (4S, 5R)-3- bromoacetyl-4-methyl-5-phenyl2-oxazolidinone (2.1.13) with benzaldehyde followed by treatment with lithium ethoxide, to
produce chiral epoxide 2.1.15 in high optical purity.
This semi-synthesis process is widely used even today also and has made the accessibility of the
drug to patients with low cost. Nevertheless, dependency on the resource of yew plant materials is
a major concern for the usefulness of this commonly used process.
III.
Improving synthesis efficiency
At present, few plant cell and tissue culture-based methods have been commercialized for
producing plant bioactive compounds that are used in applications by pharmaceutical, food, and
cosmetic industries. Manufacture of plant metabolites through in vitro cell cultures is renewable,
economically feasible and environmentally friendly. The use of Taxus spp. cell cultures is
measured as a quick approach to achieve adequate quantity of tree. Different in vitro approaches
have been explored extensively to upsurge the paclitaxel content in Taxus cell cultures. Some of
them include selection of high-paclitaxel-yielding genotypes, application of nutrients and plant
growth regulators, and the employment of elicitation technique, i.e., using chemical elicitors (silver
thiosulfate, methyl jasmonate, etc), the heat shock treatment, providing mechanical stimulus, the
use of two-phase cultures, and many others. These approaches have significantly improved the
production of paclitaxel. However, truncated and unstable yield of paclitaxel, high manufacturing
budget, and impurity due to byproduct are some of the key bottlenecks for viable commercial
utilization of in vitro cell culture approaches. A German and Canadian biotechnology firm, Phyton
Biotech is one of the leading suppliers of paclitaxel in the world, which commercially produces or
provides starting material for paclitaxel and docetaxel API (Active Pharmaceutical Ingredient)
using their “green” Plant Cell Fermentation (PCF) technology facility.
REFERENCES:
Mallappa Kumara Swamy, T. Pullaiah, Zhe-Sheng Chen - Paclitaxel_ Sources, Chemistry,
Anticancer Actions, and Current Biotechnology-Academic Press (2021)
Maela C. Farrar; Tibb F. Jacobs – Paclitaxel – National Library of Medicine (2022)
Marupudi NI, Han JE, Li KW, Renard VM, Tyler BM, Brem H. Paclitaxel: a review of adverse
toxicities and novel delivery strategies. Expert Opin Drug Saf. 2007 Sep;6(5):609-21. doi:
10.1517/14740338.6.5.609. PMID: 17877447.
Denis, J., Greene, A. S., Guenard, D., Gueritte-Voegelein, F., Mangatal, L., & Potier, P. (1988).
Highly efficient, practical approach to natural taxol. Journal of the American Chemical Society,
110(17), 5917–5919. https://doi.org/10.1021/ja00225a063
Doi, T., Fuse, S., Miyamoto, S., Nakai, K., Sasuga, D., & Takahashi, T. (2006). A Formal Total
Synthesis of Taxol Aided by an Automated Synthesizer. Chemistry-an Asian Journal, 1(3), 370–
383. https://doi.org/10.1002/asia.200600156
Farina, V. (1995). The Chemistry and Pharmacology of Taxol and Its Derivatives. Elsevier Science
& Technology.
Fukaya, K., Kodama, K., Tanaka, Y., Yamazaki, H., Sugai, T., Yamaguchi, Y., Watanabe, A., Oishi,
T., Sato, T., & Chida, N. (2015). Synthesis of Paclitaxel. 2. Construction of the ABCD Ring and
Formal
Synthesis.
Organic
Letters,
17(11),
2574–2577.
https://doi.org/10.1021/acs.orglett.5b01174
Fukaya, K., Tanaka, Y., Sato, A., Kodama, K., Yamazaki, H., Ishimoto, T., Nozaki, Y., Iwaki, Y.,
Yuki, Y., Umei, K., Sugai, T., Yamaguchi, Y., Watanabe, A., Oishi, T., Sato, T., & Chida, N. (2015).
Synthesis of Paclitaxel. 1. Synthesis of the ABC Ring of Paclitaxel by SmI2-Mediated Cyclization.
Organic Letters, 17(11), 2570–2573. https://doi.org/10.1021/acs.orglett.5b01173
Hao, X., Pan, J., & Zhu, X. (2013). Taxol Producing Fungi. In Springer eBooks (pp. 2797–2812).
https://doi.org/10.1007/978-3-642-22144-6_124
Holton, R. J., Somoza, C., Kim, H. J., Liang, F., Biediger, R. J., Boatman, P. D., Shindo, M., Smith,
C. H., & Kim, S. (1994). First total synthesis of taxol. 1. Functionalization of the B ring. Journal
of the American Chemical Society, 116(4), 1597–1598. https://doi.org/10.1021/ja00083a066
Holton, R. J., Somoza, C., Kim, H. J., Liang, F., Biediger, R. J., Boatman, P. D., Shindo, M., Smith,
C. H., Kim, S., Nadizadeh, H., Suzuki, Y., Tao, C., Vu, P. M., Tang, S., Zhang, P., Murthi, K. K.,
Gentile, L., & Liu, J. (1994). The Total Synthesis of Paclitaxel Starting with Camphor. In ACS
symposium series (pp. 288–301). American Chemical Society. https://doi.org/10.1021/bk-19950583.ch021
Kanda, Y., Nakamura, H., Umemiya, S., Puthukanoori, R. K., Murthy, A. V. R., Gaddamanugu, G.,
Paraselli, B. R., & Baran, P. S. (2020). Two-Phase Synthesis of Taxol. Journal of the American
Chemical Society, 142(23), 10526–10533. https://doi.org/10.1021/jacs.0c03592
Kumar, A., Bilal, M., Ferreira, L. F. R., & Madhuree, K. (2022). Microbial Biomolecules:
Emerging Approach in Agriculture, Pharmaceuticals and Environment Management. Academic
Press.
Nicolaou, K. C., Yang, Z., Liu, J. B., Ueno, H., Nantermet, P. G., Guy, R. K., Claiborne, C. F.,
Renaud, J., Couladouros, E. A., Paulvannan, K., & Sorensen, E. J. (1994). Total synthesis of taxol.
Nature, 367(6464), 630–634. https://doi.org/10.1038/367630a0