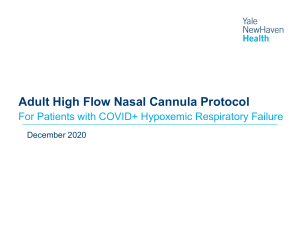
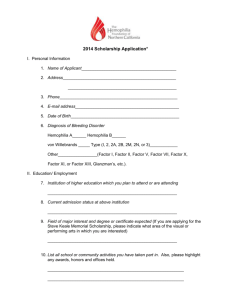
247 Reviews on Recent Clinical Trials Send Orders for Reprints to reprints@benthamscience.net Reviews on Recent Clinical Trials, 2019, 14, 247-260 SYSTEMATIC REVIEW ARTICLE ISSN: 1574-8871 eISSN: 1876-1038 High Flow Through Nasal Cannula in Stable and Exacerbated Chronic Obstructive Pulmonary Disease Patients BENTHAM SCIENCE Andrea Bruni1,#, Eugenio Garofalo1,#, Gianmaria Cammarota2, Paolo Murabito3, Marinella Astuto3, Paolo Navalesi1, Francesco Luzza4, Ludovico Abenavoli4 and Federico Longhini1,* 1 Department of Medical and Surgical Sciences, Intensive Care Unit, University Hospital Mater Domini, Magna Graecia University, Catanzaro, Italy; 2Anesthesia and Intensive Care, “Maggiore della Carità” Hospital, Novara, Italy; 3 Department of Anesthesia and Intensive Care, A.O.U. "Policlinico -Vittorio Emanuele", Catania, Italy; 4Department of Health Sciences, University of Catanzaro "Magna Graecia", Viale Europa, 88100 Catanzaro, Italy Abstract: Background: High-Flow through Nasal Cannula (HFNC) is a system delivering heated humidified air-oxygen mixture at a flow up to 60 L/min. Despite increasing evidence in hypoxemic acute respiratory failure, a few is currently known in chronic obstructive pulmonary disease (COPD) patients. Objective: To describe the rationale and physiologic advantages of HFNC in COPD patients, and to systematically review the literature on the use of HFNC in stable and exacerbated COPD patients, separately. ARTICLE HISTORY Received: April 29, 2019 Revised: June 19, 2019 Accepted: June 20, 2019 DOI: 10.2174/1574887114666190710180540 Methods: A search strategy was launched on MEDLINE. Two authors separately screened all potential references. All (randomized, non-randomized and quasi-randomized) trials dealing with the use of HFNC in both stable and exacerbated COPD patients in MEDLINE have been included in the review. Results: Twenty-six studies have been included. HFNC: 1) provides heated and humidified airoxygen admixture; 2) washes out the anatomical dead space of the upper airway; 3) generates a small positive end-expiratory pressure; 4) guarantees a more stable inspired oxygen fraction, as compared to conventional oxygen therapy (COT); and 5) is more comfortable as compared to both COT and non-invasive ventilation (NIV). In stable COPD patients, HFNC improves gas exchange, the quality of life and dyspnea with a reduced cost of muscle energy expenditure, compared to COT. In exacerbated COPD patients, HFNC may be an alternative to NIV (in case of intolerance) and to COT at extubation or NIV withdrawal. Conclusion: Though evidence of superiority still lacks and further studies are necessary, HFNC might play a role in the treatment of both stable and exacerbated COPD patients. Keywords: Chronic obstructive pulmonary disease, high flow nasal cannula, hypercapnia, non-invasive ventilation, oxygen, positive-pressure respiration, respiratory insufficiency, respiratory therapy. 1. INTRODUCTION High-Flow through Nasal Cannula (HFNC) is an innovative system that delivers heated humidified air-oxygen mixture, with an inspiratory fraction of oxygen (FiO2) from 21 to 100%, at flow up to 60 L/min [1, 2]. The flow is generated by an air-oxygen blender or a dedicated machine with a turbine; the flow goes through an active heated humidifier and *Address correspondence to this author at the Intensive Care Unit, University Hospital Mater Domini, Department of Medical and Surgical Sciences, Magna Graecia University, Catanzaro, Italy; Tel: +393475395967; Fax: +3909613647313; E-mail: longhini.federico@gmail.com # These authors contributed equally to this work. 1876-1038/19 $58.00+.00 it is delivered to the patient through a single branch with a large bore nasal cannula at its distal end. Increasing evidences encourage HFNC use in the daily clinical practice. For instance, in those patients with hypoxemic Acute Respiratory Failure (ARF) of varying etiologies, HFNC decreases: 1) oxygen therapy risk of escalation of oxygen therapy, defined as crossover to HFNC, or switch to non-invasive (NIV) or invasive mechanical ventilation (iMV); 2) the risk of tracheal intubation without impacting mortality and Intensive Care Unit (ICU) or hospital lengths of stay [3]. If on one hand there is a strong evidence that supports HFNC use in patients with hypoxemic ARF, on the © 2019 Bentham Science Publishers 248 Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 other hand it is not nowadays well known in those patients with chronic or acute-on-chronic respiratory failure. Chronic Obstructive Pulmonary Disease (COPD) is the fourth leading cause of chronic morbidity in the world [4]. COPD history may present exacerbations, which are characterized by worsening of respiratory symptoms, sometimes requiring hospitalization [4]. COPD patients are invited to smoking cessation and pharmacological treatments (such as bronchodilators) are generally required. In the most severe patients with severe resting chronic hypoxemia, the prescription of long-term oxygen therapy (LTOT) (>15 hours/day) is needed [4]. Indeed, LTOT increases patients’ survival rate. In patients with severe chronic hypercapnia and a history of hospitalization for hypercapnic ARF, long-term NIV decreases mortality and prevent re-hospitalization [4]. However, both LTOT and NIV are affected by poor tolerance, leading to low adherence to the treatment. The easiness of application, the improved comfort, together with some physiological effects and advantages, would make possible the use of HFNC in stable COPD patients at home, during rehabilitation and even during hospitalization for episodes of exacerbation. In this systematic review, we describe the rationale and physiologic possible advantages in COPD patients. In addition, we analyze the current literature on HFNC use in stable and exacerbated COPD patients, separately. 2. METHODS AND SEARCH STRATEGY 2.1. Search Methods for Identification of Studies We have performed an electronic search of Medline from inception until April 9, 2019 with no language restrictions. Controlled vocabulary terms (when available), text words, and keywords have been variably combined. Blocks of terms per concept have been created. We have used the following search strategy: “("respiratory failure" [MeSH Terms] OR "acute respiratory failure" [All Fields] OR "respiratory insufficiency" [All Fields] OR "respiratory failure" [All Fields] OR "COPD" [All Fields] OR "Chronic Obstructive Pulmonary Disease" [All Fields] OR "chronic respiratory failure" [All Fields] OR "hypercapnic" [All Fields] OR “Hypercapnic Acute Respiratory Failure” [All Fields] OR "acute no chronic respiratory failure" [All Fields]) AND ("high flow nasal oxygen" [All Fields] OR "high-flow nasal oxygen" [All Fields] OR "high flow nasal cannula" [All Fields] OR “high-flow nasal cannula" [All Fields] OR "high flow oxygen" [All Fields] OR "high-flow oxygen" [All Fields] OR “High-Flow Oxygen Therapy” [All Fields])”. This systematic review reports findings according to PRISMA guidelines. 2.2. Studies Selection Studies have been considered only if including adult COPD patients undergoing HFNC due to any reason (domiciliary support, rehabilitation, support therapy for exacerbation or weaning). All studies dealing with the potential advantageous mechanisms of HFNC in COPD patients have Bruni et al. been all considered for an introductive narrative review. In the second part, we have included randomized or non-RCTs (including crossover design) and observational studies comparing HFNC with a control group (standard oxygen therapy, non-invasive ventilation). The studies have been classified according to the stability or exacerbation of the treated disease. Titles and abstracts have been independently screened by two authors (AG and EG) according to the inclusion criteria and the full texts of the potentially relevant reports have been retrieved. The full-text reports have been independently examined by two authors (AG and EG). We have included all studies dealing with HFNC in stable or exacerbated COPD in different settings. We have excluded only reviews, editorials and commentaries. Included studies have been recorded using a Microsoft Excel standardized report form. All disagreements have been resolved by discussion and referral to a third author (FL) if necessary. 2.3. Risk of Bias Assessment The methodological quality of included parallel-group RCTs have been assessed using Review Manager software (RevMan 5.3; Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen, Denmark). Randomized and nonrandomized crossover studies have been assessed according to a modified version of the checklist proposed by Ding et al. [5]. We have evaluated all studies for randomized sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other bias. 3. RESULTS The electronic search has identified 363 potentially relevant studies (358 from MEDLINE and 5 from references retrieving). Thirty-one full-text articles have been assessed for eligibility, and 26 have been considered relevant for this review and included in the qualitative synthesis. Detailed description of the selection process flow is provided in Fig. (1). Selected studies included a mean (standard deviation) patients sample size of 73 (98), ranging from 12 to 321 patients; the average age was 72.8 (2.9) years. 3.1. Potential Advantageous Mechanisms of HFNC in COPD Patients 3.1.1. Heated Humidification The epithelium of the respiratory tract acts as a fragile interface between the respiratory system and the air. A thin layer of fluid, composed of an aqueous and a mucous (Gel) films, covers and protects the epithelium. The presence of the Gel film assures a correct motion of the cilia and the transport of the mucus from the lungs to the airways opening. The beat frequency depends on the temperature and at 37°C it is around 750 beats/min. In healthy individuals, the upper respiratory tract provides a warm, humid environment that plays a nonspecific defense function and facilitates the mucociliary movement of the normal airway epithelium [2]. Atmospheric air is at about Identification High Flow Through Nasal Cannula in COPD Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 Records identified through database searching (n = 358) 249 Additional records identified through other sources (n = 5) Records screened (n = 363) Records excluded (n = 332) Eligibility Full-text articles assessed for eligibility (n = 31) Full-text articles excluded, with reasons (n = 5) studies not reporting on HFNC (n = 3) review (n = 2) Included Screening Records after duplicates removed (n = 363) Studies included in qualitative synthesis (n = 26) Fig. (1). Flow Diagram. Study flow diagram according to the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols recommendations. 20°C, with an AH = 10 mg/L and RH of 55-60%. Its passage through the airways and bronchi permits full saturation of water vapor [100% relative humidity (RH), absolute humidity (AH) = 44 mg/L] and heating at 37°C which mainly occurs in the nose. However, the point (isothermal saturation limit) where the gas gets fully heated (37°C) and humidified (44 mg/L), is further deep and usually close to the 4th or 5th bronchial generation [6]. Such conditions are optimal to keep a normal function of the airway epithelium, and every little modification might impair the epithelial cell role [7]. The administration of inadequately conditioned medical gases, such as during conventional oxygen therapy (COT) or NIV, shifts the isothermic saturation boundary farther deepens the bronchial tree, affecting the ciliary motion, damaging the respiratory tract epithelial cell and reducing the water content of the bronchial secretions [8-10]. In this regard, active heated humidification of gases increases the gas temperature and humidity, and reduces the inflammatory responses associated to iMV, epithelial cell cilia damage, and airway water loss [11]. HFNC provides temperature and humidity-controlled gas to the airway. In an in vitro study on cultured human airway epithelial cells, Chidekel et al. have showed that humidification was beneficial to preserve the cellular structure and function, and to reduce airway epithelial inflammation, when compared to cells exposed to a dry condition over an 8-hour exposure time. These benefits were higher with a temperature at 37°C and the RH at 90%, as provided by a HFNC system [12]. In fourteen patients with idiopathic bronchiectasis, provision of heated (37°C) and humidified (44 mg/L) air for 3 hours per day for 7 consecutive days resulted in significant enhancement of mucus clearance, measured by the deposition of the radio-pulmonary aerosols (99 mTc), as compared with baseline assessment [13]. In another single-center study, 108 patients with COPD or bronchiectasis have been randomized to receive for 1 year or HFNC (fully saturated at 37°C with a flow of 20-25 L/min) or standard therapy [14]. Despite a short (1.6 hours/day) daily application, HFNC reduced the exacerbation frequency by 19%, the number of exacerbation days by 54% and prolonged the time to first exacerbation from 27 to 52 days [14]. These data suggest that keeping the airway humidified could ameliorate the mucociliary clearance and cough effectiveness, reducing the accumulation of secretions in deeper airway and, potentially, diminishing the risk of exacerbations and also hospital or ICU acquired infections, such as ventilator-associated pneumonia and non-ventilator ICU-acquired pneumonia [10]. 3.1.2. Anatomical Dead Space Washout The anatomical dead space is the volume of air located in the segments of the respiratory tract responsible for conduct- 250 Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 ing air from airways opening to the alveoli, without acting in the process of gas exchange. Dead space includes the upper airways, trachea, bronchi, and terminal bronchioles. In healthy adults, the dead space is normally estimated at 2mL/kg of body weight, which consists in the 30% of the tidal volume. HFNC determines a wash out effect from carbon dioxide (CO2) of the pharyngeal dead space. Moller et al. have assessed the CO2 wash out effect by HFNC at different flows and respiratory rate in a 3D upper airway model; the investigators used a radioactive 81mKr-gas tracer and a gamma camera to detect its distribution in the upper airway model. The clearance of tracing gas from upper airway model had a linear and a strong relationship with the flow applied by the HFNC; in particular, every increment of 1 L/min of the flow applied through HFNC determined a 1.8 ml/s increase of the clearance in the nasal cavities. Furthermore, the wash out effect was also time dependent: the lower was the respiratory rate (and therefore longer the expiratory time), the higher was the wash out effect [15]. In particular, CO2 elimination was greater and more precocious in the nasal compartment rather than in the pharyngeal sections [15]. Clearance from CO2 of the nasal cavity (40-50 ml in healthy adults) comprises at least 30% of the anatomical dead space in adults [16]. Therefore, the CO2 wash out effect is potentially relevant for patients with an incremented ratio between dead space and tidal volume, such as in COPD patients with exercise intolerance [17]. It should be also mentioned that, while interfaces for NIV, or oxygen masks are characterized by an additional instrumental dead space, HFNC does not [2]. In 11 stable COPD patients, Braunlich et al. have reported that HFNC at a flow of 20 L/min reduce the arterial partial pressure of CO2 (PaCO2) to a similar extent to NIV [18]. More recently, in 14 post-extubation COPD patients recovering from an exacerbation [19] and in 30 exacerbated COPD patients at NIV discontinuation [20], HFNC significantly have decreased the respiratory drive and work of breathing, as compared to COT. In both studies, CO2 wash out was advocated as one of the two mechanisms to decrease the diaphragmatic workload, together with the generation of small amounts of positive end-expiratory pressure (PEEP) [19-20]. 3.1.3. “PEEP” Effect In healthy subjects during unassisted spontaneous breathing, end-expiratory pharyngeal pressure is about 0.3 and 0.8 cmH2O, with open and closed mouth, respectively [21-23]. Compared to unassisted spontaneous breathing, HFNC generates greater pharyngeal pressure during expiration, while it drops to zero during inspiration [22]. Similar findings have also been reported by Parke et al. in 15 patients scheduled for elective cardiac surgery [24] and by Braunlich et al. in 28 patients with stable COPD or idiopathic pulmonary fibrosis [25]. The pressure generated by HFNC depends on the flow delivered to the patient and the nasal prongs size in relation to the nostrils [24, 26]. Ritchie et al. have also suggested that the high flow delivered by HFNC acts as an expiratory resistance to patient’s exhalation, causing the “PEEP” effect Bruni et al. [21]. Ritchie et al. [21], Mundel et al. have also hypothesized that the augmentation of expiratory resistance by HFNC could resemble also the pursed-lip breathing pattern adopted by COPD patients, which is a strategy aimed to diminish the respiratory rate and to prolong the expiratory time, finally resulting in a reduction of expiratory flow limitation and dynamic hyperinflation [27]. The “PEEP” effect is recommended as a mechanism to improve end-expiratory lung volume and oxygenation in healthy volunteers [28], in post-cardiac surgical patients [29], in patients with hypoxemic ARF [3, 30] and after extubation [31]. In patients with chronic respiratory disorders, such as COPD, the application of external PEEP through HFNC may be of help in case of the presence of dynamic lung hyperinflation and intrinsic PEEP. Indeed, the application of an external PEEP through NIV, to counteract intrinsic PEEP, reduces the work of breathing in COPD patients [32]. Compared to COT, HFNC has also been shown to reduce the respiratory muscle effort in both stable COPD patients [33] and in those recovering from an episode of exacerbation [20]. However, it should be noted that both studies did not directly assess the amounts of intrinsic PEEP and this hypothesis about HFNC remains to be verified. 3.1.4. Provision of Stable Inspired Oxygen Fraction (FiO2) When assessing oxygenation through arterial blood gases, it is essential to know FiO2, to compute the ratio between the arterial partial pressure of oxygen (PaO2) and FiO2 (PaO2/FiO2). Nasal prongs and masks provide oxygen to a patient as expressed in L/min, and the FiO2 cannot be estimated, since it varies according to the patient’s minute ventilation. When delivering oxygen through a Venturi mask, a nominal FiO2, up to 60%, is delivered to the patient. However, it should be strengthened that FiO2 is nominal and not actual. Indeed, Venturi mask has holes to prevent CO2 rebreathing and patient may potentially also re-breath part of the exhaled air. Furthermore, if the inspiratory peak flow of the patient exceeds the flow provided by the Venturi mask, the patient breathes part of atmospheric air [31]. In ten healthy volunteers, Ritchie et al. have measured the FiO2, end-tidal O2 and end-tidal CO2 from a hypopharyngeal catheter during HFNC at flow rates of 10, 20, 30, 40 and 50 L/min. During nose breathing at rest, the delivered FiO2 was not affected by atmospheric air at flow >30 L/min; when the inspiratory peak flow was increased with the exercise to an extent greater than the flow delivered by HFNC, FiO2 significantly decreased under the prescribed concentration [21]. In exacerbated COPD patients, the mean inspiratory peak flow has been reported to be around 70 L/min and to exceed 60 L/min in about 70% of the patients [34]. Therefore, HFNC use may guarantee a more stable FiO2, as compared to COT through nasal prongs, oxygen or Venturi mask. 3.2. Treatment Comfort Patient comfort and device tolerance are two of the most important determinants for NIV and treatment success [35, 36]. Breathing dry oxygen generates discomfort and pain related to mouth, throat and airways dryness, particularly in High Flow Through Nasal Cannula in COPD Table 1. Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 251 Physiologic effects of HFNC reported in stable COPD. Ref. Airway Pressure Braunlich et al. [43] + Respiratory RespiraEndEffort / tory Respiratory Intrinsic Tidal Expiratory Minute Quality Expiratory Comfort Dyspnea PaCO2 of Life Work of Work Rate PEEP Volume Time Ventilation Lung Breathing Load Volume - - + + - + + - - - Fraser et al. [44] Pisani et al. [33] - - - - - Vogelsinger et al. [45] Atwood et al. [46] + - - - - = = = Storgaard et al. [47] - + Nagata et al. [48] - + Biselli et al. [49] - Cirio et al. [50] - - - - + - Modifications of physiologic parameters, compared to conventional oxygen therapy, in stable COPD patients. The sign “+” indicates and increment or improvement, “=” no modification and “-” a reduction, as compared to conventional oxygen therapy. PEEP, positive end-expiratory pressure; PaCO2, arterial partial pressure of carbon dioxide. critically ill patients [37]. For this reason, clinical practice guidelines recommend to humidify dry oxygen when administered at flow >4L/min [38]. HFNC is characterized by delivery of fully humidified inspired oxygen/air admixture, which improves patients’ comfort and facilitates secretion elimination [31]. Compared to COT, it has been shown that HFNC improves comfort in a multicenter randomized controlled trial conducted in 105 hypoxemic patients after extubation [31], in 30 exacerbated COPD patients recovering from an episode of exacerbation at NIV withdrawn [20] and in 42 exacerbated COPD patients receiving HFNC or NIV after extubation [39]. Of note, recently Mauri et al. have reported that, in 40 patients with hypoxemic ARF, a high (37°C) temperature worsened the patient’s comfort, compared to lower temperature (31°C) [40]. Nowadays, no studies have so far investigated the effects of different temperatures and/or flow rates on comfort in stable and/or exacerbated COPD patients. 3.3. HFNC in Stable COPD Patients In COPD patients with severe chronic hypoxemia at rest (PaO2 < 55mHg), or PaO2 ranging from 55 to 59 mmHg in the presence of signs of Cor Pulmonale or hematocrit > 55%, LTOT is indicated for at least 15 hours/day. LTOT has proven to improve survival rate [4, 41]; however, the treatment compliance is hampered by a low tolerance of patients [42]. From literature research, we have identified 9 studies dealing with HFNC in stable COPD patients (Table 1). The risk of bias has been assessed in all studies and it is reported in Fig. (2). It should be mentioned that the assessment of performance bias (i.e., the blinding of participants and personnel with respect to the assigned treatment) is at high risk due to the impossibility of treatment blinding. Braunlinch et al. firstly have reported HFNC use in severe (GOLD C/D) COPD patients [43]; the authors have assessed the modifications of generated mean nasopharyngeal pressure, breathing pattern, comfort and dyspnea at incremental flow rates (from 20 to 50 L/min). HFNC progressively increased the mean nasopharyngeal pressure from 0.92 ± 0.49 mbar (at 20 L/min) up to 3.01 ± 1.03 mbar (at 50 L/min) irrespective of the used nasal prongs size. Furthermore, compared to spontaneous breathing at room air, HFNC reduced the respiratory rate, the minute ventilation, the respiratory work load (as assessed by the rapid shallow breathing pattern) and PaCO2, whereas increased by the 24% the tidal volume at 50L/min. In all tested conditions, HFNC guaranteed a good comfort and dyspnea relief [43]. In 30 COPD patients using LTOT over 15 hours/day, Fraser et al. have shown that HFNC significantly reduced the transcutaneous CO2, diminished the respiratory rate, prolonged the expiratory time and increased both the tidal vol- 252 Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 Bruni et al. Fig. (2). The graph depicts the review authors' judgments about each risk of bias item as percentages across all included studies conducted in stable COPD patients. ume and the end-expiratory lung volume, as opposed to COT [44]. More recently, in 14 consecutive COPD patients, Pisani et al. have reported that both HFNC and NIV significantly reduced the respiratory rate and effort, prolonged the expiratory time and decreased dynamic intrinsic PEEP, as compared to spontaneous breathing [33]. Furthermore, both HFNC and NIV slightly, though not significantly, decreased PaCO2, as opposed to baseline [33]. In 77 COPD patients with the indication to LTOT, Vogelsinger et al. have applied in consecutive both COT and HFNC for 60 minutes, with a 30-min wash out phase in between. Compared to COT, HFNC has been better tolerated and reduced the FiO2 requirement and PaCO2, without modifications of lung volumes [45]. Atwood et al. have randomized 32 moderate-to-severe stable COPD patients to receive COT or HFNC [46]. As opposed to COT, HFNC reduced the respiratory rate without any increase in tidal volume or PaCO2. Furthermore, HFNC reduced the ventilatory effort in the absence of modifications of PaCO2 or tidal volume, suggesting also a relevant wash out effect of the upper airway and ventilatory efficiency improvement [46]. This study was limited by a short-term evaluation without the assessment of potential clinical benefits of enhanced humidification, wash out effect and ventilatory efficiency improvement [46]. In a prospective randomized controlled trial, 200 COPD patients with the indication to LTOT have been randomized to receive either COT or COT plus HFNC (at 20 L/min for at least 8 hours/night) [47]. Compared to COT, HFNC significantly reduced the rate of exacerbation and hospitalization, dyspnea and PaCO2 at 12 months, without modification of the survival rate. Certain deterioration at 12 months of the quality of life and exercise performance, measured through 6-minute walk test, was observed in patients receiving COT, while not in those receiving HFNC [47]. HFNC has been also tested in stable COPD patients during sleep [48, 49]. In 29 COPD patients receiving LTOT, Nagata et al. have assessed the efficacy and safety of 6weeks of domiciliary HFNC for at least 4 hours per night at 30-40 L/min [48]. Compared to COT only, HFNC significantly improved the quality of life and reduced PaCO2 without any severe HFNC-related adverse events [48]. In 12 COPD patients and in a control group of 6 smokers, Biselli et al. have assessed HFNC effects (at 20 L/min) and COT (at 2 L/min) with respect to ventilation and work of breathing during sleep [49]. Compared to spontaneous breathing in room air, both COT and HFNC decreased the tidal volume and the minute ventilation during NREM sleep; however, the effect on PaCO2 was contradictory. If on one hand PaCO2 increased with COT, on the other it decreased in case of HFNC treatment. In addition, COT did not reduce the work of breathing, whereas HFNC decreased it by the 50% [49]. In 12 stable severe COPD patients, the effects of HFNC have been assessed during a constant load exercise at the 75% of maximum workload achieved at a previous incremental exercise test on cycle-ergometer [50]. Compared to breathing at room air, HFNC significantly increased the endurance time, the oxygenation during the exercise, while diminished the dyspnea and the leg fatigue scores, as reported by patients [50]. The differences among studies in term of setting of HFNC application, severity of the disease and assessed outcomes preclude us the possibility to conduct a pooled data analysis. However, we have summarized the findings of all the studies in Table 1. Of note, in the vast majority of the selected studies HFNC has reduced the respiratory rate, the work of breathing and the blood content of CO2, increased the tidal volume, while improved the quality of life and dyspnea. Further studies, properly designed and powered to assess differences in clinical outcomes (rather than physiologic ones), are deemed necessary. 3.4. HFNC in Exacerbated COPD Patients COPD exacerbations are complex events usually associated with increased airway inflammation, increased mucus production and marked gas trapping. During exacerbation, High Flow Through Nasal Cannula in COPD Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 253 Fig. (3). The graph depicts the review authors' judgments about each risk of bias item as percentages across all included studies conducted in exacerbated COPD patients. patients refer mainly worsening of dyspnea, increased sputum purulence and volume, cough and wheeze [4]. COPD exacerbation can be classified as mild (when treated with short-acting beta agonist bronchodilators [SABA] only), moderated (when the patient requires hospitalization, SABA and/or corticosteroids) and severe (when associated with ARF) [4]. Hypercapnic ARF is present or develops in approximately 20% of hospitalized COPD patients, and it is an indicator of increased risk of death [51]. Hypercapnic ARF establishes when the respiratory work load exceeds the respiratory muscles pump capacity, and a rapid shallow breathing pattern develops. Furthermore, dynamic hyperinflation also contributes to increase the respiratory work load, through the generation of intrinsic PEEP [51]. Nowadays, guidelines strongly recommend the use of NIV with a high certainty of evidence, whenever hypercapnic ARF with acidosis is present [51]. A trial of NIV is also recommended when the patients is considered to require endotracheal intubation and iMV, unless immediate deterioration [51]. In fact, NIV has been shown to improve gas exchange, reduce work of breathing and the need for intubation, decrease hospital length of stay and mortality [51]. Despite these advantages, NIV has been shown to suffer of poor patient-ventilator interaction, which determines a worsening of patient’s comfort and tolerance to the treatment and its failure [52-59]. Although patient-ventilator asynchrony can be partially managed by optimizing ventilator setting or using particular modes of ventilation [52-65], it remains difficult to recognize such events by the sole ventilator waveform observation without the use of additional signals [66]. As opposed to NIV, HFNC is not characterized by the drawback of patient-ventilator interaction and synchrony; furthermore, some physiological mechanisms which could be of clinical benefit in COPD patients have been reported in this review. For this reason, an increasing amount of literature is exploring the possible role of HFNC in exacerbated COPD patients with established hypercapnic ARF, at extubation or at NIV discontinuation. From the literature research, we have identified 10 studies reporting the use of HFNC in exacerbated COPD patients (Table 2). In particular, 4 case reports/case series have described HFNC use as an alternative to NIV, 2 studies have compared HFNC to COT as first line oxygen treatment at exacerbation, 3 studies have applied HFNC at exacerbated COPD patients after extubation (2 against NIV and 1 against COT) and, in the end, 1 study has compared HFNC to COT at NIV withdrawal (Table 2). The risk of bias has been assessed in all studies and it is reported in Fig. (3). As for studies investigating the role of HFNC in stable patients, also these studies suffer a high risk of performance bias due to the unblinded designs. The first HFNC applications in exacerbated COPD patients have been reported from 2014 as case reports [67-69] or series [70]. In these patients, HFNC was successfully applied after NIV treatment failure due to poor tolerance of the interface [67, 68, 70] or massive unmanageable air-leaks [69]. In these few patients, HFNC further has improved gas exchange [67-70], was well tolerated [67-70], significantly reduced the apnea index (from 12.1 to 3.7 events/hour) and the percentage time with SpO2 ≤90% (from 30.8 to 2.5%) [67]. These preliminary data from case reports have opened the possibility to assess the role of HFNC in exacerbated COPD patients, as alternative treatment to NIV. In a retrospective study, Kim et al. have assessed the feasibility to employ HFNC in 33 patients with hypercapnic ARF admitted to ICU. Compared to the pre-treatment condition, HFNC significantly decreased PaCO2 at 1 hour, without modifying oxygenation or respiratory rate [71]. In 2017, Pilcher et al. prospectively have randomized 24 exacerbated COPD patients to receive COT via nasal prongs and HFNC at 35 L/min, in a cross-over design [72]. In with a study by Kim et al. [71], HFNC slightly, though significantly, reduced the transcutaneous CO2 tension, without significant and clinically relevant modifications of respiratory and heart rate and SpO2 [72]. In a Chinese hospital, all COPD patients admitted in the ICU requiring iMV have been randomized to receive NIV or 254 Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 Table 2. Ref. Bruni et al. Physiologic effects of HFNC reported in exacerbated COPD. Setting Sleep Respiratory ICU Gas Treatment Related Respiratory Drive / Heart Rate Comfort Length of Exchange Success HypoventilaRate Work of Stay tion Breathing ReintubaMortality tion Rate Case report / case series Okuda et al. Alternative to [67] NIV + + Lepere et al. Alternative to [68] NIV + + Alternative to NIV + + Pavlov et al. Alternative to [70] NIV + + Plotnikow et al. [69] + Retrospective study Hypercapnic Kim et al. ARF, compared [71] to COT + = Randomized controlled or cross-over trials Hypercapnic Pilcher et al. ARF, compared [72] to COT + Zhang et al. [73] At extubation, compared to NIV = Di Mussi et al. [19] At extubation, compared to COT = Longhini et al. [20] At NIV withdrawal, compared to COT = Jing et al. [39] At extubation, compared to NIV = = - = = = = = - - - + + Modifications of physiologic parameters, compared to conventional oxygen therapy, in stable COPD patients. The sign “+” indicates and increment or improvement, “=” no modification and “-” a reduction, as compared to conventional oxygen therapy. ICU, intensive care unit; NIV, non-invasive ventilation; ARF, acute respiratory failure; COT, conventional oxygen therapy. HFNC after extubation [73]. HFNC was characterized by a shorter ICU length of stay, as compared to COT. No differences were recorded between treatments in terms of gas exchange (apart of oxygenation slightly better in NIV), 28-days reintubation rate and mortality [73]. In 14 COPD patients after extubation recovering from an exacerbation episode, Di Mussi et al. firstly have investigated the effects of HFNC with respect to work of breathing and gas exchange [19]. As compared to COT, HFNC significantly decreased the work of breathing and the respiratory drive, as assessed through the electrical activity of the diaphragm [19]. Similar findings have been also recently reported in a randomized cross-over trial by our group. In 30 COPD patients recovering from an episode of exacerbation with indi- cation to be weaned off from NIV, HFNC was compared with COT and NIV with respect to gas exchange, diaphragm function (as assessed by ultrasounds), respiratory rate, and patient comfort [20]. PaCO2 and pH were not different between HFNC and COT. However, while the diaphragm activation and respiratory rate significantly increased with COT, as compared to NIV, no modifications were shown during HFNC. Furthermore, HFNC resulted in improved comfort compared to both COT and NIV. Noteworthy, after NIV discontinuation and at the end of the study protocol, 15 patients received COT and 15 HFNC, by chance. In the next 48 hours after NIV withdrawal, NIV was reinstituted in 47% of patients receiving COT, while in 27% among those receiving HFOT. However, these last findings have been beyond the study aim and they must be considered with caution [20]. High Flow Through Nasal Cannula in COPD Table 3. Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 255 Possible clinical scenarios and settings for the use of HFNC in COPD patients. - Stable COPD Patients Exacerbated COPD Patients Aim of treatment 1. In alternative to COT 1. 2. 3. 4. Settings 1. 2. 3. 4 to 7 hours/night flow between 30 to 50 L/min FiO2 set to guarantee a SpO2 between 88-94% 1. 2. 3. In alternative di NIV in case of intolerance In alternative to COT After extubation At NIV withdrawal Continuous treatment till resolution of the condition flow between 40 to 60 L/min (titrated according patient’s comfort) FiO2 set to guarantee a SpO2 between 88-94% COPD, Chronic Obstructive Pulmonary Disease; COT, conventional oxygen therapy; FiO2, inspired oxygen fraction; SpO2, peripheral oxygen saturation; NIV, non-invasive ventilation. In the end, Jing et al. have randomized 42 exacerbated COPD patients after extubation to receive NIV or HFNC [39]. HFNC was not inferior to NIV in weaning COPD patients from iMV, with regard to gas exchange and vital signs. Patients randomized to receive HFNC required less bronchoscopy for suction of secretions, as opposed to NIV; furthermore, HFNC and NIV did not differ in terms of time spent under iMV, need for reintubation, ICU length of stay and all cause of 28-days mortality. Of note, HFNC has been reported to be more comfortable than NIV [39]. As for data regarding HFNC in stable COPD patients, we could not conduct a pooled data analysis due to the heterogeneity among studies in term of setting of HFNC application, assessed outcomes and reason of HFNC treatment. Anyhow, these preliminary data open the possibility of application of HFNC as an alternative interface to COT or NIV for COPD patients with exacerbation, in different clinical situations. However, further randomized controlled trials are deemed to assess potential benefits on major clinical outcomes. 4. DISCUSSION HFNC is increasingly used in the daily clinical practice, in patients with hypoxemic ARF due to strong and growing body of favorable evidences [1, 3]. In contrast, little is known in HFNC use in those patients with hypercapnic ARF, where no clear evidence of superiority of HFNC to both COT and NIV still exists. In stable severe hypoxemic COPD patients, COT is delivered at home to increase the blood oxygenation and resulting in an improved survival rate [4]; however, COT remains affected by a low tolerance by patients, due to dryness of compressed medical oxygen. HFNC provides heated and humidified air-oxygen admixture, making oxygen therapy more comfortable to patients. Furthermore, HFNC has been shown to reduce the PaCO2 with a minor energy expenditure cost by the respiratory muscles (i.e., reduced work of breathing and respiratory rate), to improve the quality of life and exercise performance and to reduce dyspnea, as compared to COT. The compliance of a patient to a prescribed therapy strictly depends on comfort and tolerance to the treatment, remarkably for medical devices such as oxygen therapy and NIV [35]. In principles, the improved comfort and reduced work of breathing, together with COPD symptoms relief, would improve the adherence to the therapy. Despite these physiological advantages, nowadays a clear evidence of HFNC superiority against to COT still lacks in stable COPD patients. Indeed, based on the current literature, domiciliary HFNC may be safely used in stable COPD patients for 4 to 7 hours/day, during the night time, at a flow between 30 to 50 L/min and a FiO2 set to guarantee a SpO2 ranging between 88-94% (Table 3). While in stable COPD patients, HFNC could be an alternative to the oxygen therapy, in exacerbated COPD with hypercapnic ARF and respiratory acidosis its role may be more complex, through fascinating. To date, guidelines strongly recommend the use of NIV in exacerbated COPD patients with respiratory acidosis [51]. In these patients, NIV is most commonly applied in pneumatically-triggered and cycled-off Pressure Support mode through a face mask [74]. However, this setting can be affected by discomfort to the interface and poor patient-ventilator interaction and synchrony, potentially leading to NIV failure [52, 55, 57, 59]. Comfort improvement can be attempted through the use of alternative interface (such as the helmet) [56, 75, 76]. Unfortunately, the helmet is characterized by a poor patientventilator interaction and pressurization performance [77]. Recent technical advances [78-81] and the use of proportional modes of ventilation based on the Electrical Activity of the Diaphragm, so-called Neurally Adjusted Ventilatory Assist (NAVA) [63], have been shown to limit such drawbacks. More recently, a specific setting of NAVA has been proposed to further improve pressurization and triggering performance in patients receiving iMV or NIV through both helmet and mask [53, 57, 59]. All these advances have been developed with the aim to improve patient’s comfort, and to theoretically reduce the rate of treatment failure and need for iMV. HFNC may potentially play a role of alternative treatment for those exacerbated COPD patients who failed NIV due to poor treatment tolerance. In particular, HFNC may be considered: 1) in case of respiratory acidosis, when NIV fails for intolerance [67-70], 2) after extubation when NIV cannot be used or is problematic [19, 39, 73], and 3) after NIV interruption at the resolution of the hypercapnic ARF, instead of COT [20]. As opposed to NIV, HFNC cannot be affected by a poor patient-ventilator interaction and synchrony; furthermore, HFNC is generally more comfortable to the NIV inter- 256 Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 face or COT, providing heated and humidified gas admixture [20]. Noteworthy, HFNC is also characterized by the ability to reduce the respiratory drive and effort [19, 20], to a similar extent than NIV [20]. Although some trials are ongoing to assess the potential benefits on patients’ clinical outcome [82], today HFNC could be considered in the clinical practice in some situations for COPD patients. Based on the current literature on exacerbated COPD patients, HFNC should be used only as an alternative interface in case of NIV failure (to avoid intubation), or instead of COT. The applied settings could consist in: 1) a flow rate between 40 to 60 L/min (higher than in stable COPD), and titrated according patient’s comfort, and 2) a FiO2 set to guarantee a SpO2 ranging between 88-94%. In the end, it should be mentioned that HFNC is easily applied by physicians to the patients with a variety of diseases and conditions. Large randomized controlled trials, conducted in hypoxemic patients, have never reported any absolute contraindications to HFNC, except for those patients whom NIV is contraindicated (such as severely alteration of the consciousness, facial injury, unstable hemodynamics or impaired airway patency). On the opposite, HFNC has the advantage to not require a tight contact with the patient’s face and therefore could be easily utilized in patients suffering of claustrophobia, which usually do not tolerate NIV [83]. Bruni et al. majority of the study is quite small, potentially generating positive results which could not be confirmed in larger studies [84]. For this reason, we strongly believe that further studies properly designed and powered to assess differences in clinical outcomes (rather than physiologic ones) are deemed necessary in both stable and exacerbated COPD patients. CONCLUSION HFNC may be advantageous either in stable and exacerbated COPD patients. In stable COPD patients, HFNC reduces the work of breathing, respiratory rate dyspnea and PaCO2, prolongs the expiratory time, improves the respiratory work load, the quality of life and exercise performance. In exacerbated COPD, HFNC reduces the respiratory drive to an extent similar to NIV, while keeping similar gas exchange. It remains to clarify with proper randomized controlled trials whether these physiological benefits may translate into clinical outcomes improvement. LIST OF ABBREVIATIONS AH = Absolute Humidity ARF = Acute Respiratory Failure CO2 = Carbon Dioxide 4.1. Strengths and Limitations of this Review COPD = Chronic Obstructive Pulmonary Disease This review has some strengths and limitations requiring discussion. COT = Conventional Oxygen Therapy FiO2 = Inspiratory Fraction of Oxygen First of all, to our knowledge this is the first systematic review which includes a comprehensive and systematic literature search on HFNC in COPD patients. Although a comprehensive narrative review on the potential physiological benefits of HFNC in stable COPD patients exists [2], there is no review today which summarize findings in both stable and exacerbated COPD patients with respect to assessed (mainly physiological) outcomes. Furthermore, the interest in the use of HFNC in both stable and exacerbated COPD patients is raised in the last few years, while more robust evidence already exists in hypoxemic patients [3]. HFNC = High Flow Nasal Cannula ICU = Intensive Care Unit iMV = Invasive Mechanical Ventilation LTOT = Long-Term Oxygen Therapy NAVA = Neurally Adjusted Ventilatory Assist NIV = Non-Invasive Ventilation PaCO2 = Arterial Partial Pressure of Carbon Dioxide PaO2 = Arterial Partial Pressure of Oxygen Although a growing number of studies has been published, we could not conduct a pooled data analysis for several reasons. First of all, the vast majority of the studies assessed the effects of HFNC on different physiological outcomes, such as respiratory rate, respiratory drive, blood gases and comfort, rather than major clinical outcomes. It should be mentioned however that physiological studies are the solid ground to develop larger and well-targeted trials aimed to assess the differences in clinical outcomes. Second, as shown by risk of bias assessment, the quality of the studies is quite low, the number of the enrolled patients small and the heterogeneity among population very high, which preclude us the possibility to proceed with a further metaanalysis. Therefore, the application of GRADE methodology, to assess certainty in pooled estimates of effect, has not been conducted. Third, the conclusions, which could be generated by the current literature, would be strongly affected by weak evidence support. Indeed, the sample size of the vast PaO2/FiO2 = Ratio between Arterial Partial Pressure and Inspiratory Fraction of Oxygen PEEP = Positive End-Expiratory Pressure RH = Relative Humidity SABA = Short-Acting Beta Agonist CONSENT FOR PUBLICATION Not applicable. FUNDING None. CONFLICT OF INTEREST Dr. Navalesi’s research laboratory has received equipment and grants from Maquet Critical Care, Draeger and High Flow Through Nasal Cannula in COPD Intersurgical S.p.A. He also received honoraria/speaking fees from Maquet Critical Care, Orionpharma, Philips, Resmed, MSD and Novartis.Dr. Navalesi contributed to the development of the helmet Next, whose licence for patent belongs to Intersurgical S.P.A., and receives royalties for that invention. Dr. Longhini and Dr. Navalesi contributed to the development of a new device not discussed in the present study whose patent is in progress (European Patent application number EP20170199831). The remaining authors have disclosed that they do not have any conflicts of interest. Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 [5] [6] [7] ACKNOWLEDGEMENTS Andrea Bruni was responsible for conception and design of the study, the acquisition and interpretation of the data, and for drafting and revising the article for final approval of the version to be published. Eugenio Garofalo was responsible for conception and design of the study, the acquisition and interpretation of the data, and for drafting and revising the article for final approval of the version to be published. Gianmaria Cammarota was responsible for conception and design of the study, the interpretation of the data, and for revising the article for final approval of the version to be published. Paolo Murabito was responsible for conception and design of the study, the interpretation of the data, and for revising the article for final approval of the version to be published. Marinella Astuto was responsible for conception and design of the study, the interpretation of the data, and for revising the article for final approval of the version to be published. Paolo Navalesi was responsible for conception and design of the study, the interpretation of the data, and for revising the article for final approval of the version to be published. Francesco Luzza was responsible for conception and design of the study, the interpretation of the data, and for revising the article for final approval of the version to be published. Ludovico Abenavoli was responsible for conception and design of the study, the interpretation of the data, and for revising the article for final approval of the version to be published. Federico Longhini was responsible for conception and design of the study, the acquisition and interpretation of the data, and for drafting and revising the article for final approval of the version to be published. REFERENCES [1] [2] [3] [4] Renda T, Corrado A, Iskandar G, Pelaia G, Abdalla K, Navalesi P. High-flow nasal oxygen therapy in intensive care and anaesthesia. Br J Anaesth 2018; 120(1): 18-27. [http://dx.doi.org/10.1016/j.bja.2017.11.010] [PMID: 29397127] Pisani L, Vega ML. Use of nasal high flow in stable COPD: Rationale and physiology. COPD 2017; 14(3): 346-50. [http://dx.doi.org/10.1080/15412555.2017.1315715] [PMID: 28459282] Rochwerg B, Granton D, Wang DX, et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Med 2019; 45(5): 563-72. [http://dx.doi.org/10.1007/s00134-019-05590-5] [PMID: 30888444] Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J 2017; 49(3): 1700214. [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] 257 [http://dx.doi.org/10.1183/13993003.00214-2017] [PMID: 28182564] Ding H, Hu GL, Zheng XY, Chen Q, Threapleton DE, Zhou ZH. The method quality of cross-over studies involved in Cochrane Systematic Reviews. PLoS One 2015; 10(4): e0120519 [http://dx.doi.org/10.1371/journal.pone.0120519] [PMID: 25867772] Plotnikow GA, Accoce M, Navarro E, Tiribelli N. Humidification and heating of inhaled gas in patients with artificial airway. A narrative review. Rev Bras Ter Intensiva 2018; 30(1): 86-97. [PMID: 29742220] Kilgour E, Rankin N, Ryan S, Pack R. Mucociliary function deteriorates in the clinical range of inspired air temperature and humidity. Intensive Care Med 2004; 30(7): 1491-4. [http://dx.doi.org/10.1007/s00134-004-2235-3] [PMID: 15024566] Konrad F, Schiener R, Marx T, Georgieff M. Ultrastructure and mucociliary transport of bronchial respiratory epithelium in intubated patients. Intensive Care Med 1995; 21(6): 482-9. [http://dx.doi.org/10.1007/BF01706201] [PMID: 7560491] Lacherade JC, Auburtin M, Cerf C, et al. Impact of humidification systems on ventilator-associated pneumonia: a randomized multicenter trial. Am J Respir Crit Care Med 2005; 172(10): 1276-82. [http://dx.doi.org/10.1164/rccm.200408-1028OC] [PMID: 16126933] De Pascale G, Ranzani OT, Nseir S, et al. Intensive care unit patients with lower respiratory tract nosocomial infections: The ENIRRIs project. ERJ Open Res 2017; 3(4): 00092-2017. [http://dx.doi.org/10.1183/23120541.00092-2017] [PMID: 29164144] Jiang M, Song JJ, Guo XL, Tang YL, Li HB. Airway humidification reduces the inflammatory response during mechanical ventilation. Respir Care 2015; 60(12): 1720-8. [http://dx.doi.org/10.4187/respcare.03640] [PMID: 26329357] Chidekel A, Zhu Y, Wang J, Mosko JJ, Rodriguez E, Shaffer TH. The effects of gas humidification with high-flow nasal cannula on cultured human airway epithelial cells. Pulm Med 2012; 2012380686. [http://dx.doi.org/10.1155/2012/380686] [PMID: 22988501] Hasani A, Chapman TH, McCool D, Smith RE, Dilworth JP, Agnew JE. Domiciliary humidification improves lung mucociliary clearance in patients with bronchiectasis. Chron Respir Dis 2008; 5(2): 81-6. [http://dx.doi.org/10.1177/1479972307087190] [PMID: 18539721] Rea H, McAuley S, Jayaram L, et al. The clinical utility of longterm humidification therapy in chronic airway disease. Respir Med 2010; 104(4): 525-33. [http://dx.doi.org/10.1016/j.rmed.2009.12.016] [PMID: 20144858] Moller W, Celik G, Feng S, et al. Nasal high flow clears anatomical dead space in upper airway models. J Appl Physiol 1985; 105(3): 854-8. Jiang Y, Liang Y, Kacmarek RM. The principle of upper airway unidirectional flow facilitates breathing in humans. J Appl Physiol 1985; 105(3): 854-8. Elbehairy AF, Ciavaglia CE, Webb KA, et al. Pulmonary gas exchange abnormalities in mild chronic obstructive pulmonary disease. Implications for dyspnea and exercise intolerance. Am J Respir Crit Care Med 2015; 191(12): 1384-94. [http://dx.doi.org/10.1164/rccm.201501-0157OC] [PMID: 25826478] Bräunlich J, Seyfarth HJ, Wirtz H. Nasal high-flow versus noninvasive ventilation in stable hypercapnic COPD: A preliminary report. Multidiscip Respir Med 2015; 10(1): 27. [http://dx.doi.org/10.1186/s40248-015-0019-y] [PMID: 26339486] Di Mussi R, Spadaro S, Stripoli T, et al. High-flow nasal cannula oxygen therapy decreases postextubation neuroventilatory drive and work of breathing in patients with chronic obstructive pulmonary disease. Crit Care 2018; 22(1): 180. [http://dx.doi.org/10.1186/s13054-018-2107-9] [PMID: 30071876] Longhini F, Pisani L, Lungu R, et al. High-Flow oxygen therapy after noninvasive ventilation interruption in patients recovering from hypercapnic acute respiratory failure: A physiological crossover trial. Crit Care Med 2019; 47(6): e506-11. [http://dx.doi.org/10.1097/CCM.0000000000003740] [PMID: 30882477] 258 [21] [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] [32] [33] [34] [35] [36] Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 Ritchie JE, Williams AB, Gerard C, Hockey H. Evaluation of a humidified nasal high-flow oxygen system, using oxygraphy, capnography and measurement of upper airway pressures. Anaesth Intensive Care 2011; 39(6): 1103-10. [http://dx.doi.org/10.1177/0310057X1103900620] [PMID: 22165366] Groves N, Tobin A. High flow nasal oxygen generates positive airway pressure in adult volunteers. Aust Crit Care 2007; 20(4): 126-31. [http://dx.doi.org/10.1016/j.aucc.2007.08.001] [PMID: 17931878] Garofalo E, Bruni A, Pelaia C, et al. Evaluation of a new interface combining high-flow nasal cannula and CPAP. Respir Care 2019; 64(10): 1231-9. [http://dx.doi.org/10.4187/respcare.06871] [PMID: 31164484] Parke RL, Eccleston ML, McGuinness SP. The effects of flow on airway pressure during nasal high-flow oxygen therapy. Respir Care 2011; 56(8): 1151-5. [http://dx.doi.org/10.4187/respcare.01106] [PMID: 21496369] Bräunlich J, Beyer D, Mai D, Hammerschmidt S, Seyfarth HJ, Wirtz H. Effects of nasal high flow on ventilation in volunteers, COPD and idiopathic pulmonary fibrosis patients. Respiration 2013; 85(4): 319-25. [http://dx.doi.org/10.1159/000342027] [PMID: 23128844] Dysart K, Miller TL, Wolfson MR, Shaffer TH. Research in high flow therapy: Mechanisms of action. Respir Med 2009; 103(10): 1400-5. [http://dx.doi.org/10.1016/j.rmed.2009.04.007] [PMID: 19467849] Mundel T, Feng S, Tatkov S, Schneider H. Mechanisms of nasal high flow on ventilation during wakefulness and sleep. J Appl Physiol 1985; 114(8): 1058-65. Riera J, Pérez P, Cortés J, Roca O, Masclans JR, Rello J. Effect of high-flow nasal cannula and body position on end-expiratory lung volume: A cohort study using electrical impedance tomography. Respir Care 2013; 58(4): 589-96. [http://dx.doi.org/10.4187/respcare.02086] [PMID: 23050520] Corley A, Caruana LR, Barnett AG, Tronstad O, Fraser JF. Oxygen delivery through high-flow nasal cannulae increase end-expiratory lung volume and reduce respiratory rate in post-cardiac surgical patients. Br J Anaesth 2011; 107(6): 998-1004. [http://dx.doi.org/10.1093/bja/aer265] [PMID: 21908497] Lee CC, Mankodi D, Shaharyar S, et al. High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: A systematic review. Respir Med 2016; 121: 100-8. [http://dx.doi.org/10.1016/j.rmed.2016.11.004] [PMID: 27888983] Maggiore SM, Idone FA, Vaschetto R, et al. Nasal high-flow versus Venturi mask oxygen therapy after extubation. Effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med 2014; 190(3): 282-8. [http://dx.doi.org/10.1164/rccm.201402-0364OC] [PMID: 25003980] Appendini L, Patessio A, Zanaboni S, et al. Physiologic effects of positive end-expiratory pressure and mask pressure support during exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1994; 149(5): 1069-76. [http://dx.doi.org/10.1164/ajrccm.149.5.8173743] [PMID: 8173743] Pisani L, Fasano L, Corcione N, et al. Change in pulmonary mechanics and the effect on breathing pattern of high flow oxygen therapy in stable hypercapnic COPD. Thorax 2017; 72(4): 373-5. [http://dx.doi.org/10.1136/thoraxjnl-2016-209673] [PMID: 28104830] Sharma G, Mahler DA, Mayorga VM, Deering KL, Harshaw O, Ganapathy V. Prevalence of low peak inspiratory flow rate at discharge in patients hospitalized for COPD exacerbation. Chronic Obstr Pulm Dis (Miami) 2017; 4(3): 217-24. [http://dx.doi.org/10.15326/jcopdf.4.3.2017.0183] [PMID: 28848933] Elliott MW. The interface: Crucial for successful noninvasive ventilation. Eur Respir J 2004; 23(1): 7-8. [http://dx.doi.org/10.1183/09031936.03.00115903] [PMID: 14738223] Squadrone E, Frigerio P, Fogliati C, et al. Noninvasive vs invasive ventilation in COPD patients with severe acute respiratory failure Bruni et al. [37] [38] [39] [40] [41] [42] [43] [44] [45] [46] [47] [48] [49] [50] [51] deemed to require ventilatory assistance. Intensive Care Med 2004; 30(7): 1303-10. [http://dx.doi.org/10.1007/s00134-004-2320-7] [PMID: 15197438] Lellouche F, Maggiore SM, Lyazidi A, Deye N, Taillé S, Brochard L. Water content of delivered gases during non-invasive ventilation in healthy subjects. Intensive Care Med 2009; 35(6): 987-95. [http://dx.doi.org/10.1007/s00134-009-1455-y] [PMID: 19294366] Kallstrom TJ. AARC clinical practice guideline: oxygen therapy for adults in the acute care facility--2002 revision & update. Respir Care 2002; 47(6): 717-20. [PMID: 12078655] Jing G, Li J, Hao D, et al. Comparison of high flow nasal cannula with noninvasive ventilation in chronic obstructive pulmonary disease patients with hypercapnia in preventing postextubation respiratory failure: A pilot randomized controlled trial. Res Nurs Health 2019; 42(3): 217-25. [http://dx.doi.org/10.1002/nur.21942] [PMID: 30887549] Mauri T, Galazzi A, Binda F, et al. Impact of flow and temperature on patient comfort during respiratory support by high-flow nasal cannula. Crit Care 2018; 22(1): 120. [http://dx.doi.org/10.1186/s13054-018-2039-4] [PMID: 29743098] Nocturnal Oxygen Therapy Trial Group Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: A clinical trial. Ann Intern Med 1980; 93(3): 391-8. [http://dx.doi.org/10.7326/0003-4819-93-3-391] [PMID: 6776858] Katsenos S, Constantopoulos SH. Long-Term oxygen therapy in copd: Factors affecting and ways of improving patient compliance. Pulm Med 2011; 2011: 325362. [http://dx.doi.org/10.1155/2011/325362] [PMID: 21941649] Bräunlich J, Köhler M, Wirtz H. Nasal highflow improves ventilation in patients with COPD. Int J Chron Obstruct Pulmon Dis 2016; 11: 1077-85. [http://dx.doi.org/10.2147/COPD.S104616] [PMID: 27307723] Fraser JF, Spooner AJ, Dunster KR, Anstey CM, Corley A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue carbon dioxide while increasing tidal and endexpiratory lung volumes: A randomised crossover trial. Thorax 2016; 71(8): 759-61. [http://dx.doi.org/10.1136/thoraxjnl-2015-207962] [PMID: 27015801] Vogelsinger H, Halank M, Braun S, et al. Efficacy and safety of nasal high-flow oxygen in COPD patients. BMC Pulm Med 2017; 17(1): 143. [http://dx.doi.org/10.1186/s12890-017-0486-3] [PMID: 29149867] Atwood CW Jr, Camhi S, Little KC, et al. Impact of heated humidified high flow air via nasal cannula on respiratory effort in patients with chronic obstructive pulmonary disease. Chronic Obstr Pulm Dis (Miami) 2017; 4(4): 279-86. [http://dx.doi.org/10.15326/jcopdf.4.4.2016.0169] [PMID: 29354672] Storgaard LH, Hockey HU, Laursen BS, Weinreich UM. Longterm effects of oxygen-enriched high-flow nasal cannula treatment in COPD patients with chronic hypoxemic respiratory failure. Int J Chron Obstruct Pulmon Dis 2018; 13: 1195-205. [http://dx.doi.org/10.2147/COPD.S159666] [PMID: 29713153] Nagata K, Kikuchi T, Horie T, et al. Domiciliary high-flow nasal cannula oxygen therapy for patients with stable hypercapnic chronic obstructive pulmonary disease. A multicenter randomized crossover trial. Ann Am Thorac Soc 2018; 15(4): 432-9. [http://dx.doi.org/10.1513/AnnalsATS.201706-425OC] [PMID: 29283682] Biselli PJ, Kirkness JP, Grote L, et al. Nasal high-flow therapy reduces work of breathing compared with oxygen during sleep in COPD and smoking controls: A prospective observational study. J Appl Physiol 122(1): 82-8. Cirio S, Piran M, Vitacca M, et al. Effects of heated and humidified high flow gases during high-intensity constant-load exercise on severe COPD patients with ventilatory limitation. Respir Med 2016; 118: 128-32. [http://dx.doi.org/10.1016/j.rmed.2016.08.004] [PMID: 27578482] Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J 2017; 50(2): 1602426. High Flow Through Nasal Cannula in COPD [52] [53] [54] [55] [56] [57] [58] [59] [60] [61] [62] [63] [64] [65] [66] [http://dx.doi.org/10.1183/13993003.02426-2016] [PMID: 28860265] Bruni A, Garofalo E, Pelaia C, et al. Patient-ventilator asynchrony in adult critically ill patients. Minerva Anestesiol 2019; 85(6): 67688. [http://dx.doi.org/10.23736/S0375-9393.19.13436-0] [PMID: 30762325] Longhini F, Liu L, Pan C, et al. Neurally-adjusted ventilatory assist for noninvasive ventilation via a helmet in subjects with COPD exacerbation: A physiologic study. Respir Care 2019; 64(5): 582-9. [http://dx.doi.org/10.4187/respcare.06502] [PMID: 30755472] Cortegiani A, Garofalo E, Bruni A, Sanfilippo F, Longhini F. Predatory open-access publishing in palliative and supportive care. J Pain Symptom Manage 2019; 57(3): e1-3. [http://dx.doi.org/10.1016/j.jpainsymman.2018.11.021] [PMID: 30595355] Garofalo E, Bruni A, Pelaia C, et al. Recognizing, quantifying and managing patient-ventilator asynchrony in invasive and noninvasive ventilation. Expert Rev Respir Med 2018; 12(7): 557-67. [http://dx.doi.org/10.1080/17476348.2018.1480941] [PMID: 29792537] Vaschetto R, Longhini F, Persona P, et al. Early extubation followed by immediate noninvasive ventilation vs. standard extubation in hypoxemic patients: A randomized clinical trial. Intensive Care Med 2019; 45(1): 62-71. [http://dx.doi.org/10.1007/s00134-018-5478-0] [PMID: 30535516] Longhini F, Pan C, Xie J, et al. New setting of neurally adjusted ventilatory assist for noninvasive ventilation by facial mask: A physiologic study. Crit Care 2017; 21(1): 170. [http://dx.doi.org/10.1186/s13054-017-1761-7] [PMID: 28683763] Longhini F, Abdalla K, Navalesi P. Non-invasive ventilation in hypoxemic patients: Does the interface make a difference? Ann Transl Med 2016; 4(18): 359. [http://dx.doi.org/10.21037/atm.2016.09.20] [PMID: 27761463] Cammarota G, Longhini F, Perucca R, et al. New setting of neurally adjusted ventilatory assist during noninvasive ventilation through a helmet. Anesthesiology 2016; 125(6): 1181-9. [http://dx.doi.org/10.1097/ALN.0000000000001354] [PMID: 27649505] Costa R, Navalesi P, Cammarota G, et al. Remifentanil effects on respiratory drive and timing during pressure support ventilation and neurally adjusted ventilatory assist. Respir Physiol Neurobiol 2017; 244: 10-6. [http://dx.doi.org/10.1016/j.resp.2017.06.007] [PMID: 28673877] Liu L, Xia F, Yang Y, et al. Neural versus pneumatic control of pressure support in patients with chronic obstructive pulmonary diseases at different levels of positive end expiratory pressure: A physiological study. Crit Care 2015; 19: 244. [http://dx.doi.org/10.1186/s13054-015-0971-0] [PMID: 26059238] Longhini F, Scarlino S, Gallina MR, et al. Comparison of neurallyadjusted ventilator assist in infants before and after extubation. Minerva Pediatr 2018; 70(2): 133-40. [PMID: 26583456] Navalesi P, Longhini F. Neurally adjusted ventilatory assist. Curr Opin Crit Care 2015; 21(1): 58-64. [http://dx.doi.org/10.1097/MCC.0000000000000167] [PMID: 25486574] Vaschetto R, Cammarota G, Colombo D, et al. Effects of propofol on patient-ventilator synchrony and interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit Care Med 2014; 42(1): 74-82. [http://dx.doi.org/10.1097/CCM.0b013e31829e53dc] [PMID: 23982026] Cammarota G, Olivieri C, Costa R, et al. Noninvasive ventilation through a helmet in postextubation hypoxemic patients: Physiologic comparison between neurally adjusted ventilatory assist and pressure support ventilation. Intensive Care Med 2011; 37(12): 1943-50. [http://dx.doi.org/10.1007/s00134-011-2382-2] [PMID: 22005826] Longhini F, Colombo D, Pisani L, et al. Efficacy of ventilator waveform observation for detection of patient-ventilator asynchrony during NIV: A multicentre study. ERJ Open Res 2017; 3(4): 00075-2017. Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 [67] [68] [69] [70] [71] [72] [73] [74] [75] [76] [77] [78] [79] [80] [81] 259 [http://dx.doi.org/10.1183/23120541.00075-2017] [PMID: 29204431] Okuda M, Kashio M, Tanaka N, et al. Nasal high-flow oxygen therapy system for improving sleep-related hypoventilation in chronic obstructive pulmonary disease: A case report. J Med Case Reports 2014; 8: 341. [http://dx.doi.org/10.1186/1752-1947-8-341] [PMID: 25312578] Lepere V, Messika J, La Combe B, Ricard JD. High-flow nasal cannula oxygen supply as treatment in hypercapnic respiratory failure. Am J Emerg Med 2016; 34(9): 1-2. [http://dx.doi.org/10.1016/j.ajem.2016.02.020] Plotnikow G, Thille AW, Vasquez D, Pratto R, Desmery P. Highflow nasal cannula oxygen for reverting severe acute exacerbation of chronic obstructive pulmonary disease: A case report. Med Intensiva 2017; 41(9): 571-2. [http://dx.doi.org/10.1016/j.medin.2016.11.009] [PMID: 28089165] Pavlov I, Plamondon P, Delisle S. Nasal high-flow therapy for type II respiratory failure in COPD: A report of four cases. Respir Med Case Rep 2017; 20: 87-8. [http://dx.doi.org/10.1016/j.rmcr.2016.12.006] [PMID: 28123947] Kim ES, Lee H, Kim SJ, et al. Effectiveness of high-flow nasal cannula oxygen therapy for acute respiratory failure with hypercapnia. J Thorac Dis 2018; 10(2): 882-8. [http://dx.doi.org/10.21037/jtd.2018.01.125] [PMID: 29607161] Pilcher J, Eastlake L, Richards M, et al. Physiological effects of titrated oxygen via nasal high-flow cannulae in COPD exacerbations: A randomized controlled cross-over trial. Respirology 2017; 22(6): 1149-55. [http://dx.doi.org/10.1111/resp.13050] [PMID: 28470831] Zhang JC, Wu FX, Meng LL, Zeng CY, Lu YQ. A study on the effects and safety of sequential humidified high flow nasal cannula oxygenation therapy on the COPD patients after extubation. Zhonghua Yi Xue Za Zhi 2018; 98(2): 109-12. [PMID: 29343034] Crimi C, Noto A, Princi P, Esquinas A, Nava S. A European survey of noninvasive ventilation practices. Eur Respir J 2010; 36(2): 3629. [http://dx.doi.org/10.1183/09031936.00123509] [PMID: 20075052] Antonelli M, Conti G, Pelosi P, et al. New treatment of acute hypoxemic respiratory failure: noninvasive pressure support ventilation delivered by helmet--a pilot controlled trial. Crit Care Med 2002; 30(3): 602-8. [http://dx.doi.org/10.1097/00003246-200203000-00019] [PMID: 11990923] Patel BK, Wolfe KS, Pohlman AS, Hall JB, Kress JP. Effect of noninvasive ventilation delivered by helmet vs face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA 2016; 315(22): 2435-41. [http://dx.doi.org/10.1001/jama.2016.6338] [PMID: 27179847] Navalesi P, Costa R, Ceriana P, et al. Non-invasive ventilation in chronic obstructive pulmonary disease patients: Helmet versus facial mask. Intensive Care Med 2007; 33(1): 74-81. [http://dx.doi.org/10.1007/s00134-006-0391-3] [PMID: 17039354] Olivieri C, Costa R, Spinazzola G, et al. Bench comparative evaluation of a new generation and standard helmet for delivering noninvasive ventilation. Intensive Care Med 2013; 39(4): 734-8. [http://dx.doi.org/10.1007/s00134-012-2765-z] [PMID: 23223773] Olivieri C, Longhini F, Cena T, et al. New versus conventional helmet for delivering noninvasive ventilation: A physiologic, crossover randomized study in critically Ill patients. Anesthesiology 2016; 124(1): 101-8. [http://dx.doi.org/10.1097/ALN.0000000000000910] [PMID: 26528774] Vaschetto R, De Jong A, Conseil M, et al. Comparative evaluation of three interfaces for non-invasive ventilation: a randomized crossover design physiologic study on healthy volunteers. Crit Care 2014; 18(1): R2. [http://dx.doi.org/10.1186/cc13175] [PMID: 24387642] Pisani L, Mega C, Vaschetto R, et al. Oronasal mask versus helmet in acute hypercapnic respiratory failure. Eur Respir J 2015; 45(3): 691-9. [http://dx.doi.org/10.1183/09031936.00053814] [PMID: 25504992] 260 [82] Reviews on Recent Clinical Trials, 2019, Vol. 14, No. 4 Ricard JD, Dib F, Esposito-Farese M, Messika J, Girault C. Comparison of high flow nasal cannula oxygen and conventional oxygen therapy on ventilatory support duration during acute-onchronic respiratory failure: study protocol of a multicentre, randomised, controlled trial. The ‘HIGH-FLOW ACRF’ study. BMJ Open 2018; 8(9): e022983. [http://dx.doi.org/10.1136/bmjopen-2018-022983] [PMID: 30232113] Bruni et al. [83] [84] Nishimura M. High-flow nasal cannula oxygen therapy in adults. J Intensive Care 2015; 3(1): 15. [http://dx.doi.org/10.1186/s40560-015-0084-5] [PMID: 25866645] Zhang Z, Xu X, Ni H. Small studies may overestimate the effect sizes in critical care meta-analyses: A meta-epidemiological study. Crit Care 2013; 17(1): R2. [http://dx.doi.org/10.1186/cc11919] [PMID: 23302257]