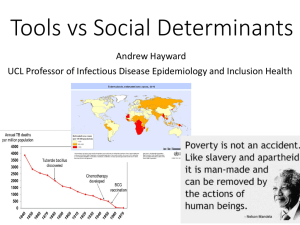
Mariano Marcos State University COLLEGE OF HEALTH SCIENCES Department of Physical Therapy City of Batac, Ilocos Norte TUBERCULOSIS MEDICAL BACKGROUND Submitted by: Abainza, Nicole Andrie Domingo, Elaine Jean Ligot, Kylie Tabunan, Trisha Zacarias, Allen Neithan Submitted to: Jeffreel M. Conception, PTRP PT167 Instructor FEBRUARY 2023 TUBERCULOSIS INTRODUCTION Tuberculosis (TB) is a disease caused by germs that are spread from person to person through air. TB usually affects the lungs, but it can also affect other parts of the body, such as the brain, kidney, or spine. A person with TB can die if they do not get treatment. This chapter will discuss the medical background of Tuberculosis, with it’s etiology, epidemiology, risk factors, anatomy and physiology, pathophysiology, clinical signs and symptoms, differential diagnosis, medical management, and physical therapy management. LEARNING OUTCOMES Upon the completion of this lesson, the student will be able to: 1. Describe the underlying causes and occurrence of tuberculosis. 2. Explain the pathophysiology of tuberculosis. 3. Differentiate the diagnosis related to tuberculosis. 4. Practice the various physical therapy assessment and intervention that are use for patient with tuberculosis. LEARNING INPUTS AND CENTRAL ACTIVITIES DEFINITION An acute or chronic infection caused by Mycobacterium tuberculosis generally transmitted by the inhalation or ingestion of infected droplets and usually affects the lungs. Although the primary infection site is the lung, mycobacteria commonly exist in other parts of the body and this is referred to as extrapulmonary tuberculosis. The extrapulmonary sites may include the renal system, skeletal system, GI tract, meninges, and genitals. Extrapulmonary tuberculosis occurs with increased frequency in people with HIV infection. Latent infection is defined as harboring M. tuberculosis without evidence of active infection. Active infection, on the other hand, is based on the presence of clinical and laboratory findings. EPIDEMIOLOGY ● ● ● ● ● ● ● ● ● ● ● ● ● Tuberculosis (TB), a highly infectious bacterial disease, was prominent in the first half of the 1900s. With improved sanitation and medical care, TB was largely controlled. A recent resurgence of the disease probably resulted from the migration patterns of people globally and the poor becoming poorer in high-income countries. TB affects many organ systems, including the lungs, and is more prevalent in people living in poor sanitary conditions with poor health. Mycobacterium tuberculosis is highly contagious but responds well to medication. TB remains a global health problem with the highest rates in Southeast Asia, sub-Saharan Africa, and Eastern Europe. Before the development of anti-TB drugs in the late 1940s, TB was the leading cause of death in the United States. Drug therapy, along with improvements in public health and general living standards, resulted in a marked decline in incidence. Between 1985 and 1992 there was a 20 % increase in new TB cases in the United States. Now, after years of rising TB infection rates, the United States has started to see a decrease in the annual number of cases. Cases of multidrug-resistant TB have continued to rise annually, and there remains a huge reservoir of individuals who are infected. Multidrug-resistant TB has emerged as a major infectious disease problem throughout the world. The AIDS pandemic, the increased incidence of TB in populations without easy access to anti-TB medications (homeless people and economically disadvantaged people), the deterioration of the public health infrastructure, interruptions in the drug supply, and inadequate training of health care providers in the epidemiology of TB are some factors contributing to the increased incidence of multidrug-resistant TB. RISK FACTORS Some of the main risk factors for tuberculosis include: 1. Poverty. People living in poverty often lack access to quality healthcare. 2. HIV Infection. Because HIV attacks the immune system, it puts people at greater risk of getting sick from other bacteria and viruses. The combination of HIV and TB can be especially deadly because the two diseases feed off each other. In 2021, about 187,000 people with HIV died of TB worldwide. 3. Homelessness. People who are homeless often live in crowded conditions with little or no access to healthcare 4. Substance Abuse. Intravenous (IV) drug use and alcoholism weaken the immune system. 5. Kidney Disease and Diabetes. Chronic conditions, such as kidney disease and diabetes, weaken your immune system, making it harder for the body to fight off TB. 6. Working in Healthcare. Doctors, nurses, and other healthcare workers get exposed to lots of patients on a regular basis, which means they’re also more likely to be close to someone with tuberculosis. 7. Smoking Tobacco. Smoking can increase your risk of getting TB and dying from it. The WHO estimates 8 percent of TB cases worldwide can be linked to smoking 8. Babies, Young Children, and Elderly People. The immune system can be more vulnerable when someone is very young or very old. ETIOLOGY Tuberculosis (TB) is caused by a type of bacterium called Mycobacterium tuberculosis. It's spread when a person with active TB disease in their lungs coughs or sneezes and someone else inhales the expelled droplets, which contain TB bacteria. Although TB is infectious, it doesn’t spread easily. You usually have to spend a lot of time in contact with someone who is contagious in order to catch it. Children with TB or people with a TB infection that occurs outside the lungs do not spread the infection. ANATOMY & PHYSIOLOGY Lungs ● cone shaped and are described as having an apex, a base, three borders (anterior, inferior, and posterior), and three surfaces (costal, medial, and diaphragmatic) ● highest point of the apex of each lung approximately 1 inch above the middle third of each clavicle. ● Upper Respiratory Tract: nose, pharynx, and larynx ● Lower Respiratory Tract: extends from the level of the true vocal cords in the larynx to the alveoli within the lungs. Generally, the lower respiratory tract may be divided into two parts: the tracheobronchial tree, or conducting airways, and the acinar or terminal respiratory units. ● Tracheobronchial tree (conducting airways): are not directly involved in the exchange of gases in the lungs. They simply conduct air to and from the respiratory units. Airway diameter progressively decreases with each succeeding generation of branching. ● Terminal respiratory (acinar) units: made up of respiratory bronchioles, alveolar ducts, and alveoli. These structures together are termed the acinus and participate in gas exchange. Alveoli ● where gas exchange occurs ● Two major types of epithelial cells exist along the alveolar wall: the Squamous pneumocytes (type I) cells and the Granular pneumocytes (type II) cells. ● Squamous pneumocytes (type I) cells are flat and thin and cover approximately 93% of the alveolar surface. ● Granular pneumocytes (type II) cells are thick, cuboidal shaped, cover 7% of the alveolar wall, and are involved in the production of surfactant. Surfactant is a lipoprotein that lowers alveolar surface tension at end-expiration and thereby prevents the lung from collapsing. ● The alveoli, like the bronchi, contain cellular components of inflammation and immunity. The alveolar macrophage engulfs and ingests foreign material in the alveoli and provides a protective function against disease. Capillaries ● composed of a single layer of endothelial cells deliver blood in close proximity to the alveoli. ● Capillaries can distend and accommodate the volume of blood being delivered to the lung. ● The alveolar-capillary interface is where the exchange of gases occurs. The thickness of the alveolar-capillary membrane is between 0.5 and 1.0 µm. PATHOPHYSIOLOGY Tuberculosis may occur in 3 stages: 1. Primary infection Infection requires inhalation of particles small enough to traverse the upper respiratory defenses and deposit deep in the lungs, usually in the subpleural airspaces of the middle or lower lobes. Larger droplets tend to lodge in the more proximal airways and typically do not result in infection. Infection usually begins from a single droplet nucleus, which typically carries few organisms. Perhaps only a single organism may suffice to cause infection in susceptible people, but less susceptible people may require repeated exposure to develop an infection. To initiate infection, M. tuberculosis bacilli must be ingested by alveolar macrophages. Bacilli that are not killed by the macrophages actually replicate inside them, ultimately killing the host macrophage (with the help of CD8 lymphocytes); inflammatory cells are attracted to the area, causing a focal pneumonitis that coalesces into the characteristic tubercles seen histologically. In the early weeks of infection, some infected macrophages migrate to regional lymph nodes (eg, hilar, mediastinal), where they access the bloodstream. Organisms may then spread hematogenously to any part of the body, particularly the apicalposterior portion of the lungs, epiphyses of the long bones, kidneys, vertebral bodies, and meninges. Hematogenous dissemination is less likely in patients with partial immunity due to vaccination or to prior natural infection with M. tuberculosis or environmental mycobacteria. 2. Latent infection Occurs after most primary infections. In about 95% of cases, after about 3 weeks of uninhibited growth, the immune system suppresses bacillary replication, usually before symptoms or signs develop. Persons with LTBI have M. tuberculosis in their bodies, but do not have TB disease and cannot spread the infection to other people. A person with LTBI is not regarded as having a case of TB. The process of LTBI begins when extracellular bacilli are ingested by macrophages and presented to other white blood cells. This triggers the immune response in which white blood cells kill or encapsulate most of the bacilli, leading to the formation of a granuloma. Tubercle bacilli (mycobacterium tuberculosis) can survive in this material for years; the balance between the host’s resistance and microbial virulence determines whether the infection ultimately resolves without treatment, remains dormant, or becomes active. Infectious foci may leave fibronodular scars in the apices of one or both lungs (Simon foci, which usually result from hematogenous seeding from another site of infection) or small areas of consolidation (Ghon foci). A Ghon focus with lymph node involvement is a Ghon complex, which, if calcified, is called a Ranke complex LTBI may be detected by using the tuberculin skin test (TST) or an interferongamma release assay (IGRA). It can take 2 to 8 weeks after the initial TB infection for the body’s immune system to be able to react to tuberculin and for the infection to be detected by the TST or IGRA. Within weeks after infection, the immune system is usually able to halt the multiplication of the tubercle bacilli, preventing further progression. 3. Active infection Healthy people who are infected with tuberculosis have about a 5 to 10% lifetime risk of developing active disease, although the percentage varies significantly by age and other risk factors. In 50 to 80% of those who develop active disease, TB reactivates within the first 2 years, but it can also reactivate decades later. Any organ initially seeded may become a site of reactivation, but reactivation occurs most often in the lung apices, presumably because of favorable local conditions such as high oxygen tension. Ghon foci and affected hilar lymph nodes are much less likely to be sites of reactivation. Conditions that impair cellular immunity (which is essential for defense against TB) significantly facilitate reactivation. Thus, patients coinfected with HIV and not receiving appropriate antiretroviral therapy (ART) have about a 10% annual risk of developing active disease. PATHOGENESIS OF TB Droplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and travel to the alveoli. Tubercle bacilli multiply in the alveoli. A small number of tubercle bacilli enter the bloodstream and spread throughout the body. The tubercle bacilli may reach any part of the body, including areas where TB disease is more likely to develop (such as the brain, larynx, lymph node, lung, spine, bone, or kidney). Within 2 to 8 weeks, special immune cells called macrophages to ingest and surround the tubercle bacilli. The cells form a barrier shell, called a granuloma, that keeps the bacilli contained and under control (LTBI). If the immune system cannot keep the tubercle bacilli under control, the bacilli begin to multiply rapidly (TB disease). This process can occur in different areas in the body, such as the lungs, kidneys, brain, or bone (see diagram in box 3). LTBI vs TB Disease SITES OF TB DISEASE TB disease can occur in pulmonary and extrapulmonary sites. Pulmonary TB disease most commonly affects the lungs; this is referred to as pulmonary TB. In 2011, 67% of TB cases in the United States were exclusively pulmonary. Patients with pulmonary TB usually have a cough and an abnormal chest radiograph and may be infectious. Although the majority of TB cases are pulmonary, TB can occur in almost any anatomical site or as a disseminated disease. Extrapulmonary TB disease occurs in places other than the lungs, including the larynx, the lymph nodes, the pleura, the brain, the kidneys, or the bones and joints. In HIV-infected persons, extrapulmonary TB disease is often accompanied by pulmonary TB. Persons with extrapulmonary TB disease usually are not infectious unless they have 1) pulmonary disease in addition to extrapulmonary disease; 2) extrapulmonary disease located in the oral cavity or the larynx; or 3) extrapulmonary disease that includes an open abscess or lesion in which the concentration of organisms is high, especially if drainage from the abscess or lesion is extensive, or if drainage fluid is aerosolized. Persons with TB pleural effusions may have underlying pulmonary TB that is masked on a chest radiograph because the effusion fluid compresses the lung. These patients should be considered infectious until pulmonary TB disease is excluded. Miliary TB Miliary TB occurs when tubercle bacilli enter the bloodstream and disseminate to all parts of the body, where they grow and cause disease in multiple sites. It results in the formation of millet seed-sized (1 to 2 mm) tuberculous foci. Miliary disease has been classified as both an extrapulmonary and a pulmonary form of TB. This condition is rare but serious. “Miliary” refers to the radiograph appearance of millet seeds scattered throughout the lung. It is most common in infants and children younger than 5 years of age, and in severely immunocompromised persons. Miliary TB may be detected in an individual organ, including the brain; in several organs; or throughout the whole body. The condition is characterized by a large amount of TB bacilli, although it may easily be missed, and is fatal if untreated. Up to 25% of patients with miliary TB may have meningeal involvement. Central Nervous System When TB occurs in the tissue surrounding the brain or spinal cord, it is called tuberculous meningitis. Tuberculous meningitis is often seen at the base of the brain in imaging studies. Symptoms include headache, decreased level of consciousness, and neck stiffness. The duration of illness before a diagnosis is variable and relates in part to the presence or absence of other sites of involvement. In many cases, patients with meningitis have abnormalities on a chest radiograph consistent with old or current TB and often have miliary TB. CLINICAL SIGNS & SYMPTOMS Clinical signs and symptoms are absent in the early stages of TB. Many cases are found incidentally when routine chest radiographs are made for other reasons. When systemic manifestations of active disease initially appear, the clinical signs and symptoms listed here may appear. ● Fatigue ● ● ● ● ● ● ● ● ● ● ● Malaise Anorexia Weight loss Low-grade fevers (especially in late afternoon) Night sweats Frequent productive cough Dull chest pain, tightness, or discomfort Dyspnea Dyspnea Hemoptysis Fever DIFFERENTIAL DIAGNOSIS CAUSES Prolonged Pulmonary Eosinophilia ● ● ● ● Parasites Medications Radiation effects Malignancies ● ● It is a granulomatous disorder of unknown origin that can affect multiple body systems. It affects blacks 10 to 20 times more often than whites and women twice as often as men. It usually occurs in the third or fourth decade of life. ● Leading cause of morbidity and mortality among cigarette smokers Air pollution Occupational exposure to irritating dusts or gases Hereditary factors Infection Allergies Aging Harmful drugs and chemicals ● Pulmonary Sarcoidosis ● ● ● Chronic Obstructive Pulmonary Disease (COPD) MANIFESTATIONS ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● Acute respiratory illness with fever Night sweats Weight loss Dyspnea It can be confused with tuberculosis, but these patients deteriorate when treated with antituberculosis drugs. Shortness of breath which often gets worse with activity Dry cough that will not go away Chest pain Wheezing Intermittent episodes of wheezing or cough With a variable degree of chronic bronchitis and emphysema Excess phlegm or sputum Shortness of breath Trouble taking a deep breath. ASSESSMENT A. Physical Examination ● ● Dullness to chest percussion Auscultation revealed vocal fremitus sound ● Appearance of the Patient ● Cachexia- is loss of weight, muscle atrophy, fatigue, weakness, and significant loss of appetite in someone who is not actively trying to lose weight. ● Pallor- a pale color that can be caused by illness, emotional shock, or stress, avoiding excessive exposure to sunlight, anemia, or genetics. ● Vitals ● Tachypnea- is characterized by rapid breathing, a sufficient gas-exchange of the body, for example after exercise, in which case it is not hyperventilation ● Tachycardia- a form of cardiac arrhythmia which refers to a rapid beating of the heart. ● Fever- increase in internal body temperature to levels that are above normal ● Lungs ● Decreased breath sounds- refer to the specific sounds identified through auscultation of the respiratory system with a stethoscope. ● Rales- are the clicking, rattling, or crackling noises heard on auscultation of (listening to) the lung with a stethoscope during inhalation. ● Rhonchi- is the "coarse rattling sound somewhat like snoring, usually caused by secretion in bronchial airways". ● Bronchial breath sounds- are loud, harsh breathing sounds with a midrange pitch. B. Ancillary Procedures ● ● ● Blood tests- Blood tests can confirm or rule out latent or active tuberculosis. These tests measure your immune system's reaction to TB bacteria. These tests require only one office visit. A blood test might be useful if you're at high risk of TB infection but have a negative response to the skin test, or if you've recently received the BCG vaccine. Imaging tests- If you've had a positive skin test, your doctor is likely to order a chest X-ray or a CT scan. This might show white spots in your lungs where your immune system has walled off TB bacteria, or it might reveal changes in your lungs caused by active tuberculosis. Sputum tests- If your chest X-ray shows signs of tuberculosis, your doctor might take samples of your sputum — the mucus that comes up when you cough. The samples are tested for TB bacteria. Sputum samples can also be used to test for drug-resistant strains of TB. This helps your doctor choose the medications that are most likely to work. Getting results of these tests can take four to eight weeks. MEDICAL MANAGEMENT Surgical Management Surgery may be indicated to resect lung segments that are chronically involved. The extent and severity of the disease determines the course of recovery. Pharmacologic Management 1. Antibiotics It can be effective in managing the disease well enough to avoid hospitalization. If detected early, the prognosis is favorable, provided the patient adheres to the medication schedule and the bacilli do not become resistant to the medications. The first-line drugs isoniazid (INH), rifampin (RIF), pyrazinamide (PZA), and ethambutol (EMB) are used together in initial treatment. There are a several different TB treatment regimens, chosen based on numerous factors. Dosing of first-line drugs can be done at different intervals. ● Isoniazid (INH): given orally once/day, has good tissue penetration, and is highly bactericidal. ● Rifampine (RIF): given orally, is bactericidal, is well-absorbed, penetrates will into cells and cerebrospinal fluid, and acts rapidly. It also eliminates dorman organisms in macrophages or causeous lesions that can cause late relapse. Thus, RIF should be used throughout the course of therapy. ● Pyrazinamide (PZA) is essential first-line drug and may also be used as part of treatment for multi-drug resistant disease (MDR TB). It is not generally recommended for the treatment of latent tuberculosis. ● Ethambutol (EMB) a bacteriostatic drug that inhibits cell wall synthesis preventing multiplying of bacilli. 2. Corticosteroids These are sometimes used to treat TB when inflammation is a major cause of morbidity and are indicated for patients with acute respiratory distress syndrome or closed-spaced infections, such as meningitis and pericarditis. Corticosteroids that are needed for other indications pose no danger to patients who have active TB and who are receiving an effective TB regimen. ● Dexamethasone. 2 mg orally or q 6 hrs for adults and children >25kg; children < 25kg are given 8 mg. PHYSICAL THERAPY MANAGEMENT 1. Tuberculosis is particularly infectious, thus special precautions should be taken by the physical therapist to prevent its spread during its infectious stage. 2. Patients are prone to excessive fatigue; treatments should be selected to promote improved oxygen transport without exceeding the patient’s capacity to deliver oxygen and without contributing to excessive fatigue. 3. Stimulation of the oxygen transport system with exercise is necessary to avoid the deconditioning and further compromise of oxygen transport. The patient therefore warrants being monitored closely. REFERENCES: Book: Goodman, C. C., & Snyder, T. E. K. (2007). Differential Diagnosis for Physical Therapists: Screening for Referral. W B Saunders Company. Frownfelter, D. L., Dean, E., & Dean, E. W. (2006). Cardiovascular and Pulmonary Physical Therapy: Evidence and Practice. Mosby. Website: Goldman, R. (2023). Tuberculosis: Risk Factors, Causes, and Prevention. Everyday Health. https://www.everydayhealth.com/tuberculosis/guide/risk-factors-causesprevention/ Mangamoori, J. (n.d.). Tuberculosis with a case presentation. https://www.slideshare.net/MangamooriJagadesh/tuberculosis-with-acase-presentation Nardell, E. A. (2023). Tuberculosis (TB). MSD Manual Professional Edition. https://www.msdmanuals.com/professional/infectiousdiseases/mycobacteria/tuberculosis-tb Transmission and Pathogenesis of Tuberculosis. https://www.cdc.gov/tb/education/corecurr/pdf/chapter2.pdf Tuberculosis physical examination - wikidoc. (n.d.). https://www.wikidoc.org/index.php/Tuberculosis_physical_examination