Uploaded by
Haitian Barbie
Cardiac Lab Values: Enzymes, Troponin, BNP, CRP

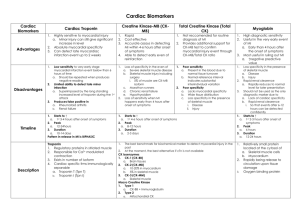
Cardiac Lab Values Cardiac Enzymes Creatine Kinase or CK: an isoenzyme present in heart muscle, skeletal muscle, brain tissue that catalyses’ conversion of creatine and uses ATP to create phosphocreatine and ADP important in tissues that consume ATP rapidly Measured in serum as a marker of damage of CK rich tissue (MI, rhabdomyolysis, acute renal failure…) Normal CK 1 or BB brain, nervous tissue, GI, GU tract 0% CK 2 or MB elevation is specific to myocardial Tissue injury Rises 4 – 6 hours after symptom onset (acute evaluation) Peak 18-24 hours (m/b/ several times normal) Return to baseline within 3 days after MI 10-13 units/L CK 3 or MM Constitutes almost all circulatory enzymes in normal people, skeletal muscle, cardiac muscle 96 – 100% 0 – 4% Total CK Men 38 – 174 units/L Women 96-140 units/L *African-Americans have higher baseline CK levels than Caucasians or Hispanic persons Creatinine phosphokinase – CPK Men Women 38 – 174 units/L 26 – 140 units/L Troponin – most sensitive test; myocardial muscle protein released into circulation after injury – normally negative 2 subtypes: T (cTnT) troponin T – cardiac specific troponin less than 0.1 ng/mL Troponin 1 (cTnl) – Troponin I Detectable w/in 1 – 3 hours after myocardial injury High specificity at 3 – 6 hours after onset of symptoms Peak w/in 12 hours Returns to normal in 14 – 15 days Monitored for healing and reperfusion Less than 1.5 ng/mL Lactic acid dehydrogenase (LDH) : intracellular enzyme widely distributed in kidney, heart, skeletal muscle, brain, liver, lungs Elevations reflect cellular death, leakage from cell Elevated levels may be non-specific but view in relation to other tests Ex: LDH remains elevated longer than CK after an MI Test 48-72 hours after onset of symptoms when pt receives medical attention 0 – 5 yo 5 – 12 yo 12 – 14 yo 14 – 16 yo Adult > 16 yo 425 – 975 370 - 840 370 – 785 370 – 645 313 – 618 ANP , BNP, NT-proBNP used to detect CHF, Left Ventricular (LV) dysfunction Higher levels found in pts with GFR < 60 mL/min & thin pts, lower in obese pts Recommended levels be drawn on admission, 24 hrs and at D/C Predictors of mortality, sudden cardiac death Also elevated in ARF, HTN, COPD, pneumonia, PE, ARDS, MI, Afib, ACS, valvular disease, myocarditis, cirrhosis Atrial Naturitic Peptide (ANP) – a potent natriuretic (causes loss of Na thru urine) agent and vasodilator, - mostly found in atria - Secreted in response to atrial stretching – produces diuresis and increases GFR. - Helps regulate extracellular fluid volume, blood pressure, sodium metabolism, promote Na excretion, - inhibits renin-angiotensin-aldosterone systems effect on aldosterone secretion. - Decreases atrial pressure by decreasing venous return, thereby reducing B/P and volume - Highly elevated in obvious heart failure, CVR disease, and increased cardiac filling pressures - Marker for early asymptomatic LV dysfunction and increased cardiac volume Reference value 20 – 77 ng/L Brain natriuretic peptide (BNP) or NT-proBNP (a pre form of BNP) – most common level but no significant difference - Found in high concentrations in cardiac tissues, especially the ventricles - Secreted in response to volume overload - stimulates diuresis, natriuretic, & vasodilation - originally found in “pig” brains - NT-proBNP is excreted in higher levels (3-5 times higher) than BNP and makes diagnosis easier - Since the level is higher in myocardial tissue is more useful than ANP - Inhibits the renin-angiotensin-aldosterone system - Marker of increased LV (left ventricular) filling pressures and LV dysfunction - Cleared by kidneys so pts with renal insufficiency may have skewed results due to prolonged excretion Reference values BNP, pg/mL < 100 HF unlikely > 500 HF likely < 200 HR unlikely > 500 HF likely if GFR < 60 NT-proBNP, pg/mL < 300 HF unlikely > 450 HF likely > 900 HF likely >1800 HF likely 21 – 50 yo 50 – 75 yo > 75 yo C-reactive Protein (CRP) – acute phase reactant made by liver and released into blood w/in a few hours after tissue injury, start of infection, or other inflammation. Not specific but helpful… Secreted by macrophages and T cells, binds to dead or dying cells and some bacteria, activates Elevated during inflammatory processes, elevated levels indicate risk for thrombosis Normal 0.1 to 2.5 mg/L Heart patients 4 – 10 mg/L Risk for future CV events screening tool: Low risk Average risk High risk <0.1 mg/dL 0.1 to 0.3 mg/dL > 0.3 mg/dL