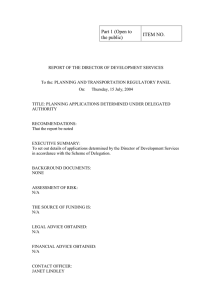
GIS at work in mapping RoCs Distribution answering the “WHERE” question Where are our Recipients of Care and how best can we serve them? DEAN FRED MWENYA M&EA FHI360 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED Table of Contents 1.0 Introduction................................................................................................................................................... 2 2.0 Objective (s) .................................................................................................................................................. 2 3.0 Process .......................................................................................................................................................... 3 4.0 Output Map.................................................................................................................................................... 7 5.0 Discussion/Conclusion.............................................................................................................................. 8 6.0 Recommendations .................................................................................................................................... 11 7.0 References .................................................................................................................................................. 12 8.0 About the Author ....................................................................................................................................... 12 1 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED 1.0 Introduction The tremendous potential of GIS to benefit the health care industry is just now beginning to be realized. Both public and private sectors are developing innovative ways to harness the data integration and spatial visualization power of GIS. The types of companies and organizations adopting GIS span the health care spectrum--from public health departments and public health policy and research organizations to hospitals, medical centers, and health insurance organizations (1). In its most basic use, GIS answers the question of “Where?” (2). This can mean questions such as “Where are people living?” “Where are diseases starting?”, in this case “where are our Recipients of Care and how best can we serve them?” FHI360, as a TA partner to Eastern Provincial Health Office CoAG, in particular Petauke District Hospital, which is one of the high volume sites managing PLWHIV (Tx-Curr as at 31st July, 2021 was 5483), leveraged the use of GIS to map Recipients of Care distribution in the whole of Petauke and Lusangazi district with Petauke District Hospital as the reference point. The primary reason for doing so was to study the RoCs distribution patterns with respect to retention on treatment. The findings from the output map were then used to make recommendations targeting the improvement of Retention. 2.0 Objective (s) 1) To generate a Tx-Curr list, i.e. a line list of all RoCs active on treatment as at 13/07/2021 using the PEPFAR QAQI. 2) To cluster the RoCs address to known wards in Petauke District 3) To use the Tx-Curr ward data and append to an existing ward attribute table in QGIS. 4) To create 10km, 20km, 30km and 40km buffer zones around Petauke District Hospital for the proximity analysis. 5) To generate an output map showing the distribution of RoCs based on Tx-Curr in respective wards. 6) To make appropriate recommendations that would greatly benefit the RoCs. 2 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED 3.0 Process The chart below shows the process that was used to achieve the above stated objectives. Prepare Datasets Tx-Curr + RoCs Addresses Shapefiles + CSV Data Load ZMB Admin, Wards, Health Facilities Append Tx-Curr to Ward Table in GIS Create choropleth Map based on TX-Curr by Ward Select Hospital Create 10Km Buffer Zones around Hospital Create Output Map 3 Cluster Addresses by Wards FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED The first step was to prepare the datasets to use in the QGIS system. The version of QGIS which was used was v.3.18. The Tx-Curr line list was generated using the PEPFAR QAQI from SmartCare as at 13/07/2021, however this report does not list the addresses of the RoCs and so other reports with addresses such as due for Viral Load were used to index match the two reports in order to add the address field using the NUPN as the Primary Key. All duplicates were removed before doing this process and sorted out manually, then later added to the master list. Note that this process was done before the coming of the Admin tool. In short, the admin tool can output a list of RoCs active on Treatment with their addresses and other fields such as their phone numbers. It is highly recommended for this process as doing it the other way has its own challenges, for instance, not all clients were index matched as the matching reports didn’t have them and so their addresses had to be added in manually (about 800-plus such cases). PEPFAR QAQI SNIP (Source: SmartCare Legacy v.5.21.0721). The other datasets which had to be prepared where GIS shapefiles for administrative boundaries of Zambia and inner provincial and town boundaries, and also a shapefile showing all wards in Petauke 4 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED District. A list of health facilities in Zambia in CSV format was also prepared. All these datasets were obtained via online open sources. It must be noted that, herein also lies a challenge on how recent the datasets are, however, for the purpose intended they worked just fine. The next key step was clustering addresses based on wards. The purpose of doing so was to come up with a complete set of Tx-Cur distribution to be represented in the output map as choropleth map rather than showing the RoCs as Points, which would have crowded the map. The clustering was done with the help of a DAPP Field Officer (FO), Mr. Michael Mwale (credits to him) who was worked at PDH since 2013, i.e. for 8 years and knows the areas and wards quite well. He provided what is called Volunteered Geographical Information (VGI) in GIS terms. However, the limitation here is that there were a few addresses (251) that could not be mapped to any ward because the FO did not recognize them. In addition 275 RoCs had no addresses listed in the system and so they could not be mapped to any ward. A sample of the clustering is shown in a snip table on the next page. Sample Snip: Clustering of Addresses by Ward After loading the shapefiles in GIS and doing some clipping in order to only remain with Petauke District and its wards, Facility data as CSV was added and necessary labels were also added. The attribute 5 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED table (as shown on the next page) for the Petauke Wards Shapefile was edited in order to append TxCurr Data per ward after consolidating the figures in excel after the clustering process. The Tx-Curr appended to the attribute table was used as a basis to create a choropleth map which assigns a colours to a range of figures, in this case the Tx-Curr. Buffer zones were created in steps of 10km around Petauke District Hospital up to 40km. Finally, map elements were added and an output map was created as shown in 4.0 Output Map Petauke Wards Attribute Table showing Tx-Curr data Appended to it 6 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED 4.0 Output Map 7 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED 5.0 Discussion/Conclusion Petauke has 22 wards (note that the map used was before Lusangazi was made into a district as well). As seen in the output map, the bulk of the Tx-Curr of the RoCs (2768) is clustered between a 10km radius to 20km. However, what is of concern is the fact that Petauke District Hospital, which has no catchment area since it’s a referral Hospital, has RoCs coming as far as beyond 20Km, and as the chart shows on the next page, beyond Petauke and beyond Eastern Province. As FHI360 we also ran a client Experience & Retention Survey from August to September, 2021, from which RoCs who stay far from PDH were asked if they would like to get a transfer to their nearest facilities; 53.8% said yes, while 46.2% said no (n=531). Out of the ones that said no, they said they were quite comfortable with collecting from PDH, while others cited issues of lack of confidentiality at their nearest facilities. 8 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED RoC TX-Curr Distribution (n=5483) Unknown Ward Unknown Ward-No Address Outside Zambia Outside Eastern Province Outside Petauke Chisangu Ukwimi Lusangazi Mawanda Mateyo-Mzeka Singozi Nyakawise Chilimanyama Nyika Nsimbo Mbala Kovyane Ongolwe Msumbazi Manjazi Kaumbwe Matambazi Mwangaila Chingombe Kapoche Manyane Lusinde 251 275 4 Beyond Petauke: 665 19 116 0 51 73 Petauke: 4818 5 563 0 39 272 2768 170 364 0 71 0 0 340 5 0 0 73 24 0 0 500 1000 1500 2000 2500 3000 The chart above shows that only 4818 RoCs stay within Petauke whereas the rest (665) stay beyond Petauke. 4818 is what was used to generate the output map. The table below shows additional information which could not be placed on the map, because there were no suitable shapefiles for, that is, the presence of rivers and farming areas within the wards. This 9 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED information is necessary in order to plan for RoCs for example who stay in wards which are bordered by rivers, which get flooded and cut them off during the rainy season. These RoCs will miss their clinical/lab/pharmacy appointments if they get blocked by the flooded rivers and so planning their schedules well in advance is important, especially making use of the 6MMD DSD Model. Similarly, knowing where the farms are is also important, as it was discovered through the Client Experience and Retention Survey that there are some RoCs who are migratory; that is, they have two physical addresses, and one of those addresses turns out to be a farm far away from Petauke District Hospital. These RoCs migrate to their farms during the rainy/farming season. Therefore planning for these RoCs is also important in keeping retention levels high. Ward Name Lusinde TX-Curr in Ward Rivers in Ward 0 Lusinde Manyane Kapoche Chingombe Mwangaila 24 73 0 0 Matambazi Kaumbwe Manjazi Msumbazi Ongolwe Kovyane Mbala 5 340 0 0 71 0 364 Nsimbo Nyika Chilimanyama Nyakawise Singozi MateyoMzeka Mawanda Lusangazi Ukwimi Chisangu 170 2768 272 39 0 Muvuvye Nil Nil Nil Matambazi Nil Nil Msumbazi Ongolwe Nil Nil Matonga, Muvuvye, Msumbazi Nil Chilimanyama Msanzala Msanzala Farms in Ward Farms Farms in Mozambique No data Farms No data Farms in Mozambique Farms No data No data No data No data Farms No data Farms Farms Farms 563 Msanzala Farms 5 Msanzala, Chilimanyama Farms 73 Msanzala, Chilimanyama No data 51 Msanzala, Chilimanyama Farms 0 Nil No data Table: Rivers and Farms in Wards & respective Tx-Curr. 10 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED 6.0 Recommendations From the findings from the output map, the following are the recommendations 1) First and foremost, all facilities, especially, the high volume sites in Eastern Province and beyond should do this mapping as well, for effective planning in improving retention outcomes. At facility level; for PDH: 1) Since most of the Tx-Curr is clustered between 10km to 20km of Petauke District Hospital, the forming of UAG groups can be reinforced in order to improve retention outcomes as RoCs in groups are known to keep appointments better than individuals, as fellow group members keep track of their friends and remind them of appointments. 2) For RoCs beyond 20km of Petauke District Hospital, they can be encouraged to get transfers to the nearest facilities, or community ARV dispensation programmes can be initiated by PDH in order to reach those RoCs and use the nearest health facilities as sites for such distribution. 3) Provide site mentorship to facilities that are near where the RoCs for PDH are so that the RoCs can feel more comfortable to get transfers to start collecting from those facilities. 11 FOR CONFIDENTIALITY REASONS, SOME FIELDS HAVE BEEN REDACTED 7.0 References 1: https://www.esri.com/news/arcuser/0499/umbrella.html (accessed 16/11/2021) 2: Cromley, Ellen K. and Sara L. McLafferty. (2012). GIS and Public Health. The Guilford Press: New York, 2nd edition. GIS Software https://qgis.org/en/site/forusers/download.html 8.0 About the Author Public Health Specialist and Computer specialist with 5 plus years of experience, working in International NGOs in conjunction with Zambia’s Ministry of Health and local NGOs in health promotion USAID/CDC/DOD/PEPFAR funded projects. Having worked in different health settings and in different towns in Zambia, using his skills gained for Program Monitoring Evaluation, Accountability and Learning and Business Intelligence. Offering a client centred data management approach to influence positive behavioural change and to track all program deliverables (inputs, outputs, outcomes, impacts and overall goal attainment). Contact: +260974886901/+260968723207 | EMAIL: dean.fred.mwenya@gmail.com 12