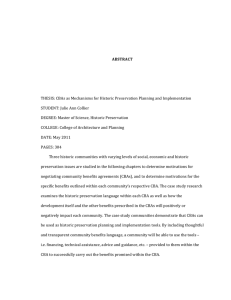
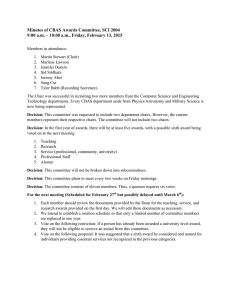
AIDS Care Psychological and Socio-medical Aspects of AIDS/HIV ISSN: 0954-0121 (Print) 1360-0451 (Online) Journal homepage: https://www.tandfonline.com/loi/caic20 Improved long-term antiretroviral treatment outcomes amongst patients receiving communitybased adherence support in South Africa Geoffrey Fatti, Eula Mothibi, Najma Shaikh & Ashraf Grimwood To cite this article: Geoffrey Fatti, Eula Mothibi, Najma Shaikh & Ashraf Grimwood (2016) Improved long-term antiretroviral treatment outcomes amongst patients receiving community-based adherence support in South Africa, AIDS Care, 28:11, 1365-1372, DOI: 10.1080/09540121.2016.1191605 To link to this article: https://doi.org/10.1080/09540121.2016.1191605 View supplementary material Published online: 02 Jun 2016. Submit your article to this journal Article views: 629 View related articles View Crossmark data Citing articles: 4 View citing articles Full Terms & Conditions of access and use can be found at https://www.tandfonline.com/action/journalInformation?journalCode=caic20 AIDS CARE, 2016 VOL. 28, NO. 11, 1365–1372 http://dx.doi.org/10.1080/09540121.2016.1191605 Improved long-term antiretroviral treatment outcomes amongst patients receiving community-based adherence support in South Africa Geoffrey Fatti, Eula Mothibi, Najma Shaikh and Ashraf Grimwood Kheth’Impilo, Cape Town, South Africa ABSTRACT ARTICLE HISTORY Retaining high levels of patients in care who are virally suppressed over long treatment periods has been an important challenge for antiretroviral treatment (ART) programmes in sub-Saharan Africa, the region having the highest HIV burden globally. Clinic-linked community-based adherence support (CBAS) programmes provide home-based adherence and psychosocial support for ART patients. However, there is little evidence of their longer-term impact. This study assessed the effectiveness of CBAS after eight years of ART. CBAS workers are lay healthcare personnel providing regular adherence and psychosocial support for ART patients and their households through home visits addressing household challenges affecting adherence. A multicentre cohort study using routinely collected data was undertaken at six public ART sites in a high HIVprevalence South African district. Patient retention, loss to follow-up (LTFU), viral suppression and CD4 cell restoration were compared between patients with and without CBAS, using competing-risks regression, linear mixed models and log-binomial regression. 3861 patients were included, of whom 1616 (41.9%) received CBAS. Over 14,792 patient-years of observation, the cumulative incidence of LTFU was 37.3% and 46.2% amongst patients with and without CBAS, respectively, following 8 years of ART; adjusted subhazard ratio (CBAS vs. no CBAS) = 0.74 (95% CI: 0.66–0.84; P < .0001). Amongst patients on ART for 6.5–8 years, proportions not achieving viral suppression were 11.4% and 19.4% in patients with and without CBAS, respectively; adjusted risk ratio = 0.47 (95% CI: 0.26–0.86; P = .015). Annual CD4 cell increases from baseline were 62.8 cells/ µL/year and 51.5 cells/µL/year amongst patients with and without CBAS, respectively, after 6.5 years or more (P = .034). After adjustment, annual CD4 cell recovery was 15.1 cells/µL/year (95% CI: 2.7–27.6) greater in CBAS patients (P = .017). ART patients who received CBAS had improved long-term patient retention, viral suppression and immunological restoration. CBAS is an intervention that can improve longer-term ART programme outcomes in resource-limited settings. Received 18 September 2015 Accepted 16 May 2016 KEYWORDS Antiretroviral treatment; community-based adherence support; South Africa; HIV; outcomes; lay health workers Introduction Excellent adherence to antiretroviral treatment (ART) is vital for treatment success, to prolong survival and to prevent the development of drug resistant mutations (Nachega et al., 2011). Long-term data show that adherence tends to wane with time, and sustained efforts are required to ensure good long-term adherence to ART (Nachega, Mills, & Schechter, 2010). Sub-Saharan Africa remains the region with the highest burden of HIV globally, having 71% of all people living with HIV (UNAIDS, 2014b). The impact of ART has made dramatic improvements in life expectancy in many sub-Saharan countries (UNAIDS, 2015). However, sustaining patient retention over long treatment periods has been a particular challenge to ART programmes, with a recent meta-analysis reporting average 5-year retention at 56% (Fox & Rosen, 2010, 2015). Viral suppression also decreases over increased treatment durations, with a review indicating only 63% of patients achieve viral suppression (by intention-to-treat) after 24 months (Barth, van der Loeff, Schuurman, Hoepelman, & Wensing, 2010). Rising levels of HIV drug resistance is also occurring (Aghokeng et al., 2011; Hamers, Sigaloff, Kityo, Mugyenyi, & de Wit, 2013). As primary healthcare facilities delivering ART have become increasingly overburdened with the large number of ART patients, the quality of clinic adherence counselling has reduced and increasing numbers of patients have become lost to follow-up (LTFU) (Bekker et al., 2014; Cornell et al., 2010). To address these challenges, and considering the severe shortage of professional healthcare workers in the region (Bärnighausen, Bloom, & Humair, 2007), lay community-based health worker programmes have been established to support sub-Saharan ART patients. CONTACT Geoffrey Fatti geoffrey.fatti@khethimpilo.org Supplemental data for this article can be accessed at 10.1080/09540121.2016.1191605. © 2016 Informa UK Limited, trading as Taylor & Francis Group 1366 G. FATTI ET AL A review of these programmes has shown favourable impact on short-term ART programme outcomes (Wouters, Van Damme, van Rensburg, Masquillier, & Meulemans, 2012). However, there are little available data of the longer-term outcomes of ART programmes in the region, and evidence regarding the longer-term impact of community-based support programmes is particularly lacking. South Africa has the world’s largest ART programme with over 2.6 million people who have initiated ART (UNAIDS, 2014b). The aim of this study was to assess the longer-term effectiveness of a clinic-linked community-based adherence support (CBAS) programme for ART patients in a high HIV prevalence district of South Africa. Clinical, immunological and virological outcomes were compared after eight years of ART between patients who received and did not receive CBAS at six public healthcare facilities. Methods CBAS intervention CBAS workers are clinic-linked, lay healthcare personnel who provide adherence support through addressing psychosocial barriers to adherence amongst ART patients, and undertake home visits and refer to social services and others to address these challenges (see programme description, supplemental online material). Support starts from the time of pre-ART preparation and continues throughout long-term care. During the initial home assessment, household issues are assessed including tuberculosis (TB) screening and HIV testing status of household members. The psychosocial barriers to adherence including nutrition security, substance abuse, depression, domestic violence, non-disclosure and stigma are assessed and addressed. Issues affecting adherence are discussed at clinic multidisciplinary team meetings, and interventions agreed by the team are implemented by the CBAS worker or social worker. Following the first visit, patients are visited weekly for a month, and then on a monthly basis. Once stable, patients are visited at least quarterly. CBAS workers provide one-on-one counselling regarding adherence and psychosocial problems, and follow-up on progress made regarding referrals to social workers. Health promotion education and symptom screening for TB and opportunistic infections is performed, with referral to clinics if indicated. CBAS workers also advise on medication storage and do adherence checks. Where patients are not comfortable with home visits or if they work, adherence and psychosocial support is provided at the clinic. CBAS workers have a specific geographic area which they support. Each worker is assigned 80–120 patients, and tracks patients with a paper-based diary. Visit details, including interventions, are recorded by the CBAS worker and captured electronically by clinicbased data capturers. Patients who default clinical visits are also traced by CBAS workers. Each community worker reports to an area coordinator who oversees the work quality through audits and home visits with the community worker. Study design and setting A multicentre cohort study utilising routine clinical data was conducted at six ART facilities in iLembe district, KwaZulu-Natal, South Africa. All facilities are primary healthcare facilities. Two facilities are located in rural areas and the remainder are in urban/semi-urban areas. In 2012, the district antenatal HIV prevalence rate was 37.4% (South African National Department of Health, 2013). All facilities are supported by Kheth’Impilo, a non-governmental organisation that supports the South African Department of Health. Kheth’Impilo provides clinical staff and innovations to strengthen public health systems. Inclusion criteria, outcomes and definitions Adults with CD4 cell counts ≤200 cells/µL and/or a World Health Organization (WHO) stage IV defining illness were eligible to start ART as per the 2004 South African national treatment guidelines (South African National department of Health, 2004). From April 2010, ART eligibility criteria were expanded to include adults with CD4 cell counts ≤350 cells/µL if they were pregnant or diagnosed with active TB (South African National department of Health, 2010). All adults (≥16 years of age) not previously enrolled for ART starting triple-drug ART between 1 January 2005 and 30 September 2010 with documented date of birth, gender and date of starting ART were included. Database closure was 30 September 2014. Patients were allocated to receive CBAS during the pre-treatment preparation period by the community area co-ordinator if community workers were active in the area of the patients home, community worker capacity was available, and if consent was obtained. Clinical and socioeconomic factors were not criteria in the choice of allocation of patients to receive CBAS or not. For analyses, patients were assigned to the CBAS group if they were allocated to and received support from a named CBAS worker since the start of ART. Receipt of CBAS was captured in the clinical AIDS CARE database by clinic-based data capturers following the ART initiation visit. All patients (CBAS and nonCBAS) received three group training sessions regarding HIV education and adherence prior to starting ART. Outcome measures were: patient retention in care eight years after starting ART, LTFU after 8 years, reported all cause-mortality, proportions of patients not achieving viral suppression (viral load ≥400 copies/mL) amongst patients having a viral load measurement between 6.5 and 8 years after starting ART, and CD4 cell slope amongst patients with a recorded baseline CD4 cell count and one or more measurements between 6.5 and 8 years of ART. Patient losses (patient attrition) was defined as a combined endpoint of mortality or LTFU. Patient deaths were recorded as reported to clinic healthcare workers. All patients visited the clinic on a frequency determined by clinic professional staff (generally monthly), and a patient was defined as LTFU if no visits to the clinic occurred for 180 days or more (Chi et al., 2011). Patients transferring to other facilities were censored on the date of last clinic visit. Laboratory measurements were performed by the South African National Health Laboratory Service. Data collection and statistical methods Individual-level clinical data were collected prospectively by designated site-based data capturers at each patient clinic visit using standardised custom-designed electronic databases, which were regularly pooled to a central data warehouse using standard operating procedures. Regular data cleaning and quality control procedures were implemented. 1367 Baseline characteristics were compared between groups using the Wilcoxon rank-sum and Pearson’s χ 2 tests for continuous and categorical data, respectively. Outcome analyses were by intention-to-treat ignoring subsequent changes in exposure status. Kaplan–Meier estimates, the logrank test and multivariable Cox’s proportional hazards regression were used to analyse time till patient attrition and retention in care. Time to mortality and LTFU were analysed using cumulative incidence functions and competing-risks regression using the method of Fine and Gray (1999; Schoni-Affolter et al., 2011). The number needed to treat to prevent a case of LTFU were calculated as appropriate for timeto-event outcomes (Altman & Andersen, 1999). Multivariable log-binomial regression was used to analyse viral suppression on ART. Mixed-effects linear models were used to analyse CD4 cell slope (Boscardin, Taylor, & Law, 1998). Separate models were produced for CD4 cell increases from the start of ART, and using the six month CD4 cell count as a baseline. The following a priori specified covariates that were plausible confounders were eligible to be included in multivariable regression models to control for confounding: baseline age, gender, baseline CD4 cell count, baseline WHO clinical stage, baseline TB treatment, year of starting ART, pregnancy when starting ART, time on ART, urban/rural site. Covariates were included in multivariable models where their inclusion produced a ≥10% shift in the point estimate of the prime exposure variable (receipt of CBAS) (Maldonado & Greenland, 1993). Modification of the effect of CBAS on outcomes was assessed by stratifying effect measures by plausible modifiers. Data were analysed using Stata (TM) version 13.1 (Statacorp, College Station, TX, USA). Permission for the study was granted by the University of Cape Town Health Research Ethics Committee. Results Figure 1. Kaplan–Meier estimates of patient retention in care after starting ART amongst patients who received and did not receive CBAS. 3861 patients were included, of whom 1616 (41.9%) received CBAS and 2245 (58.1%) did not. Characteristics of patients included at the start of ART are shown in Table 1. Patients who received CBAS had a higher proportion with advanced (stages III or IV) WHO clinical stage disease (610/1225; 48.6%) compared to patients who did not receive CBAS (643/1665; 38.6%); P < .0001. Patients who started CBAS had a higher proportion who received concomitant TB treatment at baseline. A slightly higher proportion of patients who received CBAS were from rural settings. The total observation time was 14,792 patient-years. During the study period, 50/1616 (3.1%) and 77/2245 (3.4%) patients who received and did not receive 1368 G. FATTI ET AL Table 1. Characteristics of patients at the start of ART. Median age, years (IQR) (n = 3861; 0% missing) Male gender, n (%) (n = 3861; 0% missing) Median CD4 cell count, cells/µL (IQR) (n = 3762; 3% missing) CD4 cell count < 100 cells/µL, n (%) (n = 3762; 3% missing) WHO stage (n = 2920; 24% missing) Stages I and II, n (%) Stages III and IV, n (%) Baseline TB, n (%) (n = 2766; 28% missing) Pregnancy amongst women, n (%) (n = 2005; 22% missing) Year of starting ART, median year (IQR) (n = 3861; 0% missing) Rural clinics, n (%) (n = 3861; 0% missing) With CBAS (n = 1616) Without CBAS (n = 2245) P-value 34.9 (29.8–41.4) 35.2 (29.6–43.1) .62 504 (31.2%) 773 (34.4%) .035 149 (98–193) 151 (100–188) .48 409 (25.7%) 541 (25.0%) .62 <.0001 645 (51.4%) 610 (48.6%) 124 (8.3%) 1022 (61.4%) 643 (38.6%) 139 (10.9%) .022 47 (5.3%) 54 (4.8%) .58 2009 (2007–2010) 893 (55.3%) 2009 (2008–2010) 1115 (49.7%) <.0001 .001 Note: CBAS, community-based adherence support; WHO, World Health Organization; ART, antiretroviral treatment; IQR, interquartile range. Figure 2. Cumulative incidence of loss to follow-up after starting ART amongst patients who received and did not receive CBAS. CBAS, respectively, were reported as having died (P = .56). A further 404/1566 (25.8%) and 655/2168 (30.2%) of patients who received and did not receive CBAS, respectively, were LTFU (P = .003). Following 8 years of ART, the Kaplan–Meier estimates of patient retention amongst patients with and without CBAS were 61.8% and 56.8%, respectively (P < .0001) (Figure 1). After controlling for confounding, overall patient attrition was reduced by 25% amongst patients who received CBAS, adjusted hazard ratio=0.75 (95% CI: 0.66–0.86; P < .0001) (Figure 3). After 8 years of ART, the Fine and Grey cumulative incidence estimates of LTFU were 37.3% and 46.2% amongst patients who received and did not receive CBAS, respectively (P < .0001) (Figure 2). After controlling for confounding, LTFU was reduced by 26% Figure 3. Adjusted outcome measures (patients with CBAS vs. patients without support). Estimates for attrition, loss to followup, and unsuppressed viral load are adjusted hazard ratio, adjusted subhazard ratio, and adjusted risk ratio, respectively. Horizontal bars are 95% confidence intervals. amongst patients who received CBAS, adjusted subhazard ratio (asHR)= 0.74 (95% CI: 0.66–0.84; P < .0001) (Figure 3) (see table, supplemental online material). The reduction in LTFU associated with CBAS was particularly evident amongst patients with advanced clinical disease, asHR=0.58 (95% CI: 0.47–0.73; P < .0001); and amongst pregnant women, asHR = 0.34 (95% CI: 0.12– 0.98; P = .045). The numbers needed to treat to prevent one case of LTFU after two years was 10.4 (95% CI: 7.3–18.2). Mortality was equivalent between patients with and without CBAS; asHR=0.88 (95% CI: 0.61– 1.25; P = .48). Amongst patients on ART for 6.5 years-8 years, the proportions who had unsuppressed viral loads (utilising AIDS CARE 1369 the most recent available measurement). Figure 4 shows modelled CD4 cell trajectories. Median annual CD4 cell slopes from baseline amongst patients with and without CBAS were 62.8 cells/µL/year (IQR: 35.3–87.6) and 51.5 cells/µL/year (IQR: 26.7–71.1), respectively (P = .034) (see figure, supplemental online material). After adjustment for covariates, annual CD4 increase since starting ART was 15.1 cells/µL/year (95% CI: 2.7–27.6) greater amongst CBAS patients (P = .017) (crude difference = 13.6 cells/µL/year [95% CI: 1.0–26.3; P = .034]) (see table, supplemental online material). Using the CD4 cell measurement at 6 months as a baseline, the adjusted annual CD4 slope between 6.5 and 8 years of ART was 19.1 cells/µL/year (95% CI: 3.5–34.8) greater amongst CBAS patients (P = .016). Discussion Figure 4. Modelled CD4 cell trajectories from: (a) CD4 cell count at the start of ART, and (b) CD4 cell count 6 months after starting ART. The number of patients with one or more CD4 cell count measurements during each preceding one year period is indicated. the most recent measurement) in patients who received and did not receive CBAS were 11.4% (95% CI: 8.0%15.5%; n = 299 patients; proportion suppressed=88.6%) and 19.4% (95% CI: 11.1%–30.5%; n = 72 patients; proportion suppressed =80.6%), respectively (P = .067). After controlling for confounding, the risk of having an unsuppressed viral load on long term ART was significantly lower amongst patients who received CBAS; adjusted risk ratio=0.47 (95% CI: 0.26–0.86; P = .015) (Figure 3) (crude risk ratio=0.58 [95% CI: 0.33–1.03; P = .064]) (see table, supplemental online material). CD4 cell analyses were performed amongst patients with recorded CD4 cell counts at the start of ART and one or more measurement between 6.5 and 8 years of ART. Median CD4 cell increases from baseline amongst patients with and without CBAS were 425 cells/µL (IQR: 243–596; n = 288 patients) and 350 cells/µL (IQR: 178–483; n = 50 patients), respectively (P = .025) (using This study provides unique data on the longer-term impact of CBAS for ART patients in a very high HIV prevalence setting in sub-Saharan Africa. Patients who received CBAS had improved retention and viral suppression up till 8 years of ART, and improved longterm immunological restoration. The effect of CBAS is likely mediated through a variety of mechanisms: Firstly, improved understanding of HIV and the importance of adherence through counselling improve motivation and behaviour skills related to ART adherence (Fisher, Fisher, Amico, & Harman, 2006). Secondly, greater disclosure, reductions in perceived stigma, and improvement in psychosocial problems likely contribute to improved adherence (Hodgson et al., 2014; Lowther, Selman, Harding, & Higginson, 2014). Thirdly, community support widens the “community safety net” and harnesses social capital, a powerful social force determining ART patient retention (Foster, 2007; Hickey et al., 2015; Ware et al., 2009). Patient retention is one of the most important determinants of the impact of ART programmes, and has been an important challenge in sub-Saharan Africa (Fox & Rosen, 2015). LTFU is the most important cause of patient attrition. Psychosocial support through home visits act as powerful prevention action against patient attrition (Wouters et al., 2012). CBAS workers also actively trace defaulting patients in the community, which has been shown to improve ART outcomes (Kabore et al., 2010), and is a service which may otherwise be unavailable. ART patients need to be empowered to self-manage their chronic illness in low-income settings (Wouters et al., 2012). Patient empowerment encompasses a wide range of educational and counselling activities to increase patients’ chronic disease management skills. Without 1370 G. FATTI ET AL these, patients are more likely to discontinue treatment and clinic visits or to develope viral rebound, particularly as treatment adherence tends to wane with increasing duration of treatment (Nachega et al., 2010). Overburdened staff in under-resourced primary healthcare settings have a limited understanding of their counselling role, and are constrained in being able to deliver the patient-centred care to empower patients to improve their chronic disease management skills (Stein et al., 2008). CBAS is an important link between primary healthcare facilities and the community, integrates and streamlines delivery of treatment and holistic patient care, and aids the decentralisation of ART delivery to the community (Decroo et al., 2013). CBAS meets the emerging need associated with chronic HIV care, where due to the crippling shortage of professional healthcare workers and the growing caseload of people needing to be maintained on ART, professional workers roles are becoming progressively limited to technical medical and nursing tasks (Wouters et al., 2012). The UNAIDS Strategy of reaching 90–90–90 by 2020 (UNAIDS, 2014a) will require South Africa to have over 5 million people on ART. Reaching 90% retention with 90% viral suppression will be very challenging and may more likely be attained with an emphasis on CBAS and the rollout of chronic treatment clubs at facilities and in communities. This data provides evidence of the efficacy of this community-based approach to adherence and requires consideration if South Africa is to reach these targets. Challenges faced by the CBAS programme include the rural context of many patient’s residences and long distances between the home and clinic with inadequate transport systems; poor baseline patient knowledge regarding HIV/AIDS, and cultural preferences for traditional medication. The strengths of the study include that prospective, individual-level cohort data were collected enabling controlling for patient-level factors associated with outcomes. A consistency of improved outcomes (patient retention, LTFU, viral suppression and immunological restoration) in the intervention group was observed. Limitations of the study include the non-random allocation of patients to groups with the potential for selection bias and unmeasured or residual confounding. Patients were allocated to receive the intervention on the basis of availability of community workers, geography of patient’s residence, and patient consent. As consent was required to receive CBAS, it is possible that consenting patients were more committed to treatment and were more likely to have disclosed their HIV status to family members. The proportions of patients who declined CBAS (or who opted to receive CBAS in the clinic instead of at home) were not available in the dataset. In addition, the use of routine data may have resulted in information bias. Of note, however, is that nonrandomised studies of this type of intervention using routine health systems data are more pragmatic and suitable in low-income settings, as randomised experiments are costly, and suitable and feasible for only a small proportion of HIV interventions (Thomas, Curtis, & Smith, 2011). Also, the pre-study probability of these findings was high, as the results concur with studies of shorter-term outcomes (Fatti, Meintjes, Shea, Eley, & Grimwood, 2012; Wouters et al., 2012). Although it was expected as part of the programme that all patients commencing CBAS were to receive long-term CBAS after commencing CBAS, the duration of support that all patients included in the study actually received was not able to be determined from the available data. In addition, ascertainment of patient deaths through linkage of data with the national death registry was not conducted, and data capturers were not blinded as to the group allocation of patients. In conclusion, CBAS is an intervention associated with improved clinical, virological and immunological ART outcomes over eight years of patient treatment in a high HIV-prevalence, resource-poor setting in South Africa. Further research is needed to quantify the costeffectiveness of CBAS. Future randomised studies may provide greater rigour as to the effectiveness of this intervention. Further scale-up of similar programmes should be considered to support the large number of patients who are starting ART in Africa and other areas where the professional healthcare workforce is limited. Acknowledgements The authors wish to acknowledge patients included in the study, the Department of Health of KwaZulu-Natal, the Global Fund to Fight AIDS, Tuberculosis and Malaria, the United States Agency for International Development, and the Presidents Emergency Plan for AIDS Relief. Disclosure statement No potential conflict of interest was reported by the authors. References Aghokeng, A. F., Kouanfack, C., Laurent, C., Ebong, E., AtemTambe, A., Butel, C., … Peeters, M. (2011). Scale-up of antiretroviral treatment in sub-Saharan Africa is accompanied by increasing HIV-1 drug resistance mutations in drugnaive patients. AIDS, 25(17), 2183–2188. doi:10.1097/ QAD.0b013e32834bbbe9 Altman, D., & Andersen, P. K. (1999). Calculating the number needed to treat for trials where the outcome is time to an AIDS CARE event. BMJ, 319(7223), 1492–1495. doi:10.1136/bmj.319. 7223.1492 Bärnighausen, T., Bloom, D. E., & Humair, S. (2007). Human resources for treating HIV/AIDS: Needs, capacities, and gaps. AIDS Patient Care and STDS, 21(11), 799–812. doi:10.1089/apc.2007.0193 Barth, R. E., van der Loeff, M. F., Schuurman, R., Hoepelman, A. I., & Wensing, A. M. (2010). Virological follow-up of adult patients in antiretroviral treatment programmes in subSaharan Africa: A systematic review. Lancet Infectious Diseases, 10(3), 155–166. doi:10.1016/s1473-3099(09)70328-7 Bekker, L., Venter, F., Cohen, K., Goemare, E., Van Cutsem, G., Boulle, A., … Wood, R. (2014). Provision of antiretroviral therapy in South Africa: The nuts and bolts. Antiviral Therapy, 19(Suppl 3), 105–116. doi:10.3851/IMP2905 Boscardin, W. J., Taylor, J. M. G., & Law, N. (1998). Longitudinal models for AIDS marker data. Statistical Methods in Medical Research, 7(1), 13–27. doi:10.1177/ 096228029800700103 Chi, B. H., Yiannoutsos, C. T., Westfall, A. O., Newman, J. E., Zhou, J., Cesar, C., … on behalf of the International Epidemiologic Databases to Evaluate AIDS Collaboration. (2011). Universal definition of loss to follow-up in HIV treatment programs: A statistical analysis of 111 facilities in Africa, Asia, and Latin America. PLoS Med, 8(10), e1001111. doi:10.1371/journal.pmed.1001111 Cornell, M., Grimsrud, A., Fairall, L., Fox, M., van Cutsem, G., Giddy, J., … Myer, L. (2010). Temporal changes in programme outcomes among adult patients initiating antiretroviral therapy across South Africa, 2002–2007. AIDS, 24, 2263–2270. doi:10.1097/QAD.0b013e32833d45c5 Decroo, T., Rasschaert, F., Telfer, B., Remartinez, D., Laga, M., & Ford, N. (2013). Community-based antiretroviral therapy programs can overcome barriers to retention of patients and decongest health services in sub-Saharan Africa: a systematic review. International Health, 5(3), 169–179. doi:10.1093/ inthealth/iht016 Fatti, G., Meintjes, G., Shea, J., Eley, B., & Grimwood, A. (2012). Improved survival and antiretroviral treatment outcomes in adults receiving community-based adherence support: 5-Year results from a multicentre cohort study in South Africa. Journal of Acquired Immune Deficiency Syndrome, 61(4), e50–e58. doi:10.1097/QAI.0b013e31826 a6aee Fine, J. P., & Gray, R. J. (1999). A proportional hazards model for the subdistribution of a competing risk. Journal of the American Statistical Association, 94(446), 496–509. Fisher, J. D., Fisher, W. A., Amico, K. R., & Harman, J. J. (2006). An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychology, 25(4), 462–473. Foster, G. (2007). Under the radar: Community safety nets for AIDS-affected households in sub-Saharan Africa. AIDS Care, 19(Suppl 1), 54–63. doi:10.1080/0954012060 1114469 Fox, M. P., & Rosen, S. (2010). Patient retention in antiretroviral therapy programs up to three years on treatment in sub-Saharan Africa, 2007–2009: Systematic review. Tropical Medicine and International Health, 15(Suppl 1), 1–15. doi:10.1111/j.1365-3156.2010.02508.x Fox, M. P., & Rosen, S. (2015). Retention of adult patients on antiretroviral therapy in low- and middle-income countries: 1371 Systematic review and meta-analysis 2008–2013. Journal of Acquired Immune Deficiency Syndromes, 69(1), 98–108. doi:10.1097/qai.0000000000000553 Hamers, R. L., Sigaloff, K. C., Kityo, C., Mugyenyi, P., & de Wit, T. F. (2013). Emerging HIV-1 drug resistance after roll-out of antiretroviral therapy in sub-Saharan Africa. Current Opinion in HIV and AIDS, 8(1), 19–26. doi:10. 1097/COH.0b013e32835b7f94 Hickey, M. D., Salmen, C. R., Omollo, D., Mattah, B., Fiorella, K. J., Geng, E. H., … Cohen, C. R. (2015). Implementation and operational research: Pulling the network together: Quasiexperimental trial of a patient-defined support network intervention for promoting engagement in HIV care and medication adherence on Mfangano Island, Kenya. Journal of Acquired Immune Deficiency Syndromes, 69(4), e127–134. doi:10.1097/qai.0000000000000664 Hodgson, I., Plummer, M. L., Konopka, S. N., Colvin, C. J., Jonas, E., Albertini, J., … Fogg, K. P. (2014). A systematic review of individual and contextual factors affecting ART initiation, adherence, and retention for HIV-infected pregnant and postpartum women. PLoS ONE, 9(11), e111421. doi:10.1371/journal.pone.0111421 Kabore, I., Bloem, J., Etheredge, G., Obiero, W., Wanless, S., Doykos, P., … Tiam, A. (2010). The effect of communitybased support services on clinical efficacy and health-related quality of life in HIV/AIDS patients in resource-limited settings in sub-Saharan Africa. AIDS Patient Care and STDS, 24(9), 581–594. doi:10.1089/apc.2009.0307 Lowther, K., Selman, L., Harding, R., & Higginson, I. J. (2014). Experience of persistent psychological symptoms and perceived stigma among people with HIV on antiretroviral therapy (ART): A systematic review. International Journal of Nursing Studies, 51(8), 1171–1189. doi:10.1016/j.ijnurs tu.2014.01.015 Maldonado, G., & Greenland, S. (1993). Simulation study of confounder-selection strategies. American Journal of Epidemiology, 138(11), 923–936. Nachega, J. B., Marconi, V. C., van Zyl, G. U., Gardner, E. M., Preiser, W., Hong, S. Y., … Gross, R. (2011). HIV treatment adherence, drug resistance, virologic failure: Evolving concepts. Infect Disord Drug Targets, 11(2), 167–174. doi:10. 2174/187152611795589663#sthash.SanWVjpn.dpuf Nachega, J. B., Mills, E. J., & Schechter, M. (2010). Antiretroviral therapy adherence and retention in care in middle-income and low-income countries: Current status of knowledge and research priorities. Current Opinion in HIV and AIDS, 5(1), 70–77. doi:10.1097/COH.0b013e328 333ad61 Schoni-Affolter, F., Keiser, O., Mwango, A., Stringer, J., Ledergerber, B., Mulenga, L., … Chi, B. H. (2011). Estimating loss to follow-up in hiv-infected patients on antiretroviral therapy: The effect of the competing risk of death in Zambia and Switzerland. PLoS ONE, 6(12), e27919. doi:10.1371%2Fjournal.pone.0027919 South African National Department of Health. (2004). National antiretroviral treatment guidelines. Retrieved from http://www.doh.gov.za/docs/factsheets/guidelines/ artguidelines04/ South African National Department of Health. (2010). Clinical guidelines for the management of HIV & AIDS in adults and adolescents. Retrieved from http://www.fidssa.co.za/Guide lines/2010_Adult_ART_Guidelines.pdf 1372 G. FATTI ET AL South African National Department of Health. (2013). The 2012 national anatenatal sentinel HIV and herpes simplex type 2 prevalence survey in South Africa. Retrieved from http:// www.hst.org.za/publications/2012-national-antenatal-sentin el-hiv-herpes-simplex-type-2-prevalence-survey Stein, J., Lewin, S., Fairall, L., Mayers, P., English, R., Bheekie, A., … Zwarenstein, M. (2008). Building capacity for antiretroviral delivery in South Africa: A qualitative evaluation of the PALSA PLUS nurse training programme. BMC Health Services Research, 8, 240. doi:10.1186/1472-6963-8-240 Thomas, J. C., Curtis, S., & Smith, J. B. (2011). The broader context of implementation science. Journal of Acquired Immune Deficiency Syndromes, 58(1), e19–e21. doi:10. 1097/QAI.0b013e31822103e4 UNAIDS. (2014a). 90-90-90. An ambitious treatment target to help end the AIDS epidemic. Retrieved from http://www. unaids.org/en/resources/documents/2014/90-90-90 UNAIDS. (2014b). The gap report. Retrieved from http:// www.unaids.org/en/resources/documents/2014/20140716_ UNAIDS_gap_report UNAIDS. (2015). HIV treatment in Africa. A looming crisis. Retrieved from http://www.unaids.org/en/resources/ documents/2015/2015_HIVtreatmentinAfrica Ware, N. C., Idoko, J., Kaaya, S., Biraro, I. A., Wyatt, M. A., Agbaji, O., … Bangsberg, D. R. (2009). Explaining adherence success in sub-Saharan Africa: An ethnographic study. PLoS Med, 6(1), e1000011. doi:10.1371%2Fjournal. pmed.1000011 Wouters, E., Van Damme, W., van Rensburg, D., Masquillier, C., & Meulemans, H. (2012). Impact of community-based support services on antiretroviral treatment programme delivery and outcomes in resource-limited countries: A synthetic review. BMC Health Services Research, 12, 194. doi:10. 1186/1472-6963-12-194