Tooth Eruption & Shedding: Stages, Theories, and Mechanisms
advertisement

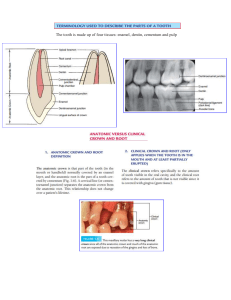
DR. SOWJANYA.R I MDS CONTENTS Definitions Evolutionary concepts Molecular level of tooth development Stages of teeth development Physiologic tooth movement Theories of eruption Mechanics of tooth eruption Rhythm of eruption Chronology of teeth Disturbances in tooth eruption Factors affecting tooth eruption Shedding of teeth Conclusion DEFINITIONS Eruption (Latin ‘erumpere’- “to break out”.) Maury Massler and Schour(1941): a process whereby the forming tooth migrates from its intraosseous location in the jaw to its functional position within the oral cavity. STAGES OF TOOTH EVOLUTION REPTILIAN STAGE ( HAPLODONT) EARLY MAMMALIAN STAGE ( TRICONODONT) TRIANGULAR STAGE (TRITUBERCULAR MOLAR) QUADRITUBERCULAR MOLAR RADIOGRAPHIC STAGES 10.Root apex completed. 9.Root almost completed,open apex. 8.Two thirds of root completed. 7.One third of root completed. 6.Crown completed. 5.Crown almost completed. 4.Two thirds of crown completed. 3.One third of crown completed. 1952 2.Initial calcification. 1.Crypt present. 0.Crypt absent. Movements at each stage Stage 1 – no pre eruptive movements Stage 2-follicular movement begins Stage 3– preeruptive movement begins Stage 4-5 – pre emergent eruptive spurt Stage 6- eruptive movement begins Stage 7-8- alveolar crest pierced Stage 9-gingival margin pierced Stage10- tooth completed erupted PHYSIOLOGIC TOOTH MOVEMENT • PRE ERUPTIVE TOOTH MOVEMENT • ERUPTIVE / PRE FUNCTIONAL TOOTH MOVEMENT • POST ERUPTIVE / FUNCTIONAL TOOTH MOVEMENT PRE ERUPTIVE TOOTH MOVEMENT • Made by deciduous and permanent tooth germs within tissues of the jaw before they begin eruption • Helps in positioning of tooth and its crypt within the growing jaws preparatory to tooth eruption • All movements take place in crypt and BEFORE ROOT FORMATION The most useful description of the eruption pattern has been that of Darling and Levers. Their cross-sectional orthopantomographic data derived from patients between 2 and 22 years of age revealed that eruption of posterior teeth could be divided into five stages: (1) concentric growth of the tooth follicle; (2) bodily movement of the tooth until it reaches the occlusal plane; (3) equilibrium with no occlusal movement of the tooth; (4) second phase of bodily movement of the tooth associated with the spurt of growth during adolescence; and (5) further equilibrium, achieved by about 18 years of age and persisting into adult life. Follicular growth Histologic evidence indicates that the permanent tooth germs, which bud from the developing deciduous teeth, generally assume a position lingual to their precursors. As the deciduous teeth develop and erupt, the permanent tooth follicles undergo sometimes complicated migrations from their initial to their preeruptive positions. Once crown formation has begun, however, the follicles of the posterior teeth move buccally with little, if any, radiographic evidence of occlusal or mesiodistal movement. The tooth crypt behaves as a cyst during this phase, symmetrically expanding vertically and mesiodistally. The center, as seen from the buccal aspect, remains at the same distance to the inferior alveolar canal. This apparent immobility from the lateral view persists until the entire crown has calcified and approximately 2 to 4 mm of the root has developed. Pre-emergent eruptive spurt During the second phase, root formation continues as the tooth begins a period of rapid eruption in the occlusal direction. All points on the developing tooth move occlusally, including the lengthening root. Radiographic studies of a maxillary central incisor examined at 6week intervals found that eruption pursued a smooth course with an increasing rate as it approached gingival emergence.” HISTOLOGY • Bodily tooth movement - it is the movement of the entire tooth germ which cause bone resorption in the direction of tooth movement and deposition behind it. • Eccentric tooth growth - relative growth of in one part of tooth while the rest of the tooth remains constant. e.g. crown maintains the constant relation with the surrounding alveolar bone while increase in the alveolar height is compensated for the root growth. RELATIVE POSITION OF PRIMARY AND PERMANENT TEETH PATTERN OF MOVEMENT OF PERMANENT MOLARS Maxillary molars in the tuberosity facing distally Swing around with growth of the maxilla Mandibular molars in the base of the ramus facing mesially Tilt to be upright with growth of the mandible ERUPTIVE TOOTH MOVEMENT • Mechanism remains similar for both set of tooth. • Made by a tooth to move from its position within the bone of jaw to its functional position in occlusion • Divided into intraosseous and extra-osseous phases • Initiation of ROOT FORMATION and ends when teeth reach occlusal contact. ANATOMIC STAGES Noyes, Schour 1931 Stage I : Preparatory stage (opening of the bony crypt) Stage II : Migration of the tooth toward the oral epithelium Stage III : Emergence of crown tip into the oral cavity (Beginning of clinical eruption) Stage IV : First occlusal contact Stage V : Full occlusal contact Stage VI : Continuous eruption Stages of tooth eruption HISTOLOGIC CHANGES •Changes in tissues overlying teeth •Changes in tissues around the teeth •Changes in tissues underlying teeth CHANGES IN TISSUES OVERLYING TEETH • Alteration of the connective tissue of the dental follicle to form pathway for the erupting tooth . • Histologically ,the future erupting pathway appears as a zone with decreased and degenerated connective tissue fibre's, cells, blood vessels and nerves and these changes are due to the loss of blood supply to this area, as well as release of enzyme that aids in degradation of these tissue. • An altered tissue space overlying the tooth become visible as an inverted funnel shaped are with the follicle fibre's directed towards the mucosa this is called as gubercular cord. • This structure guide in eruption. For successful tooth eruption, there must be resorption of overlying bony crypts so that the tooth can erupt-osteoclast differentiate and resorb a portion of the bony crypts overlying the erupting tooth. The eruption pathway initially small later increase to allow movement of the tooth. When the tooth is near the oral mucosa the REE comes and fuses with overlying mucosa and later forms a thin membrane. Later due to the further movement of the tooth stretches an thins the membrane over the crown tip. At this stage the mucosa becomes blanched because of the lack of blood supply to the area. The tooth that will erupt slightly remain stationary for few days and then again erupt.in this manner the supporting tissues are able to make adjustment to the eruptive tooth movement. CHANGES IN TISSUES AROUND THE TEETH Initially dental follicle is composed of delicate connective tissue. Gradually as the tooth erupts collagen fibres become prominent. First fibres to appear at the cervical area of the root. As the eruption proceeds the other fibres also become visible along the root surface and the alveolar bone. Some fibres release as the tooth moves later reattaches to stabilize the tooth so in this manner the tooth stabilization process is performed by the same group of fibres through out the tooth eruption. Alveolar bone remodelling continue during tooth eruption ,as the tooth moves occlusally ,the alveolar bone increase in height and change shape to accommodate the crown . CHANGES IN TISSUES UNDERLYING TEETH • As the tooth erupt, space is provided for the root to lengthen, primarily due to the crown moves occlusally and increase in the height of alveolar bone so changes in the fundic region are believed largely compensatory to the lengthening of the root. • Fine bony trabeculae appears in the fundic area. • They compensate for the tooth eruption , and provide some support at the apical tissue. • “BONY LADDER” - The ladder becomes denser as a alternate layers of bone plates and connective tissue are laid down. • At the end of prefunctional eruptive phase • The bony ladder is gradually resorbed i.e one plate at a time, to make space for developing root tip. • This process takes place from 1-1.5 years in deciduous teeth 2-3 years in permanent teeth. • The rate of tooth eruption depends on the phase of movement : Intraosseous phase: 1 to 10 µm/day Extra osseous phase: 75 μm/day POST ERUPTIVE PHASE Movements made by the tooth after it has reached its functional position in occlusion Divided into 3 categories ACCOMODATION FOR GROWTH COMPENSATION FOR OCCLUSAL WEAR ACCOMODATION FOR INTERPROXIMAL WEAR ACCOMODATION FOR GROWTH – Occurs between 14-18 years by formation of new bone at the alveolar crest and base of socket to keep in pace with increasing heights of jaws COMPENSATION FOR OCCLUSAL WEAR – Compensation primarily occurs by continuous deposition of cementum around the apex of tooth ACCOMODATION FOR compensated by mesial drift INTERPROXIMAL WEAR – THEORIES OF TOOTH ERUPTION 1. Root elongation theory 2. Pulpal constriction theory 3. Growth of periodontal tissues theory 4. Pressure from muscular action upon the 7. Foreign body theory 8. Cellular proliferation theory alveolar process theory 9. Vascular theory 5. Resorption of alveolar crest theory 10. Blood vessel thrust theory 6. Hormonal theory 11. Periodontal ligament contraction theory 12. Bone remodeling theory 13. Dental follicle theory 1) ROOT ELONGATION THEORY Thomas Bell 1835 He stated that eruption of teeth was due to root elongation wrote, "As ossification proceeds, the roots of the teeth continue to elongate until first those of the incisors, and subsequently the others, CROWN COMPLETION ROOT GROWTH STARTS can no longer be contained within the alveoli." TOOTH ERUPT IN ORAL CAVITY Because roots form at the time of eruption, they have long been considered the force responsible for eruption . ROOT GROWTH ENDS LIMITATIONS • Gowgiel (1967) using irradiation to prevent root formation in 10 day old male, albino rats, observed that the crowns continued to erupt. • Witkop,( 1975) Rootless teeth do erupt is most obvious in cases of dentin dysplasia Type I. • Experimentally when root forming tissues are removed the tooth does not show cessation of eruption which is the next drawback of the study. • Submerged tooth where there is a fully developed root but fails to erupt. In other words, root formation and elongation is not required for tooth eruption. It may, however, accelerate eruption speed. 2) PULPAL CONTRICTION THEORY Zuckerkandl,Walkhoff,Eidman-1937 • Growth of the root dentin and constriction of the pulp providing pressure that moves the tooth occlusally. Evidence against theory is: In case of pulpless tooth: in which there is no growth of root dentin • And no constriction of pulp but still eruption is possible. • Permanent premolar jumps into occlusion after the extraction of the deciduous teeth. 3) GROWTH PERIODONTAL LIGAMENT THEORY A) Pull by surrounding connective tissue: UNDERWOOD -1972 - Connective tissue surrounding the tooth pulls it into oral cavity - evidence against: PDL fibers are being pulled by tooth B) Alveolar bone growth: HERMANN and NIZEL-1973 - Squeezes the tooth out of alveolus into oral cavity - histologic and x-ray evidence against the theory: Bone does not actually touch the tooth. 4) PRESSURE FROM MUSCULAR ACTION UPON ALVEOLAR PROCESS Berten (cited by Demolis) Musculature of the cheek and lips upon alveolar process squeeze the crown of tooth in the oral cavity. Evidence against: Eruption of lateral incisors and premolar Mouth breathers Unilateral facial paralysis Eruption of teeth in patients with muscular dystrophies 5) RESORPTION OF ALVEOLAR CREST THEORY Aichel and Weidenreich They proposed that resorption of alveolar crest and subsequent exposure of the crown of the tooth in the oral cavity. Evidence against the theory Histologically when they observed alveolar crest is the site of most rapid and continuous growth of the bone. The alveolar process forms during tooth development and is locally deficient in sites where primary or permanent teeth fail to develop (Brash, 1928; Lands- Berger, 1924). Thus, alveolar bone growth, tooth development, and eruption are interdependent. Formation of bone apical to developing teeth has long been proposed as one mechanism for eruption (Brash, 1928). There is no doubt that bone forms in these sites, but bone formation per se is not sufficient for tooth eruption either. 6) HORMONAL THEORY Sir Arthur Keith CLINICAL EVALUATION: Evidence for theory: Action of Thyroid and pituitary hormones( Baume, Becks & Evans) Have reported that in rats, hypophysectomy (pitutary gland) was followed by retardation in the eruption of the incisor tooth. In addition the tooth attained only about two third of normal size and show distortion at apical end and later by injection of an anterior pituitary extract restored the eruption rate to normal. Complete mechanism not proposed. 7) FOREIGN BODY THEORY Gottleib Calcified body tends to be exfoliated by tissues just as any other foreign body CONCLUSION: No actual mechanism proposed 8) CELLULAR PROLIFERATION THEORY Noyes (1911) - Cellular proliferation of pulpal surrounding tissue cause increase in osmotic pressure and forces and that cause tooth eruption. Addison and Appleton (1915) - In a morphological study involving normally erupting rat incisors, arrived at the conclusion that eruption was the result of cellular proliferation and growth of the apical tissues. Evidence against the theory: Main and Adams (1966) examined the effects of anti-mitotic and hypotensive drugs on the eruption rate of the rat incisor. From their experiments, they concluded that there was no direct relationship between the rate of eruption and blood pressure or cellular proliferation. 9) VASCULARITY THEORY Constant (1896) They proposed that rich vascular supply between teeth and its bony surrounding cause increase pressure by vessels that cause eruption of the tooth. Evidence for this theory: In case of periodontitis(hyperamia) -there is supra eruption of the tooth. Hyperaemia in submerged tooth. Evidence against theory It has been shown that surgical resection of growing root and associated structures eliminates the vascular supply in peri-apex without stopping eruption. This means that local vessels are not absolutely necessary for tooth eruption. 10) BLOOD VESSEL TRUST THEORY Sutton 1985 It points out that the flow of blood through the vessels of the dental pulp, and of the tissues surrounding the tooth, must produce hydrodynamic and hydrostatic forces within the blood vessels, and that these forces have a resultant towards the tooth crown, thus causing the tooth to move, crown first, through the bone during normal eruption Evidence against the theory Taylor and Butcher (1951) interrupted the sympathetic innervation to the rat incisor and ligated major arteries supplying blood to this tooth. From their observations they concluded that the rate of eruption of the incisor is not sensitive to even fairly noticeable changes in blood flow. Vascular theory Blood vessel thrust theory •Force exerted by tissue fluids • Force generated by blood •Outside blood vessel • Inside blood vessel •Tissue fluid pressure acts equally in all direction • Mainly toward cusps and vessels of PDL •Force generated by pressing on surrounding bone • No pressure placed on bone 11) PERIODONTAL LIGAMENT TRACTION THEORY Thomas (1964 and 1967) - suggested that tractional forces in the periodontal ligament due to molecular cross-linkage and fibre aggregation during collagen maturation must be considered as a force in tooth eruption. He felt that intermolecular and intramolecular cross-linkages produce tension in the oblique fibres of the periodontal ligament thus pulling the tooth coronally. Ness (1970) revised his opinion and stated that his favourite hypothesis was now that fibroblasts located in the periodontal tissue exert tension along their length, thus providing the force for movement of the rodent incisor. Experiments and studies •Certain drugs like vitamin C which is essential for collagen formation and latharytic agent which prevents cross-linking between collagen aggregates has shown positive results in preventing tooth eruption by decreasing growth of collagen fibers. 12) BONE REMODELLING THEORY The Marks and cahill -1984 They demonstrated that dental follicle need to be present for tooth eruption . Bony remodelling occurs around the erupting follicle regardless of the presence of the tooth crown or tooth. Suggesting that the remodelling process may be under the control of the dental follicle. However these experiments provide no evidence that the follicle is involved in determining of final tooth position. Evidence against theory: Formation of eruptive pathway within bone without coincident bone formation at the base of crypt. Bone remodelling occur only in presence of dental follicle Evidence against theory: Formation of eruptive pathway within bone without coincident bone formation at the base of crypt. Bone remodelling occur only in presence of dental follicle 13) DENTAL FOLLICLE THEORY CAHILL AND MARKS 1980 Investigations indicate a pattern of cellular activity involving the reduced dental epithelium and follicle associated with tooth eruption. The REE initiates a cascade of intercellular signals that recruits osteoclasts to the follicle by providing the conduit and the chemoattractant for osteoclasts, the dental follicle is necessary to permit the bony remodelling that occurs with tooth movement. Evidence for the theory In osteoporotic animals, which lack a factor that stimulates differentiation of osteoclasts , eruption is prevented, because no mechanism for bone removal exists. Local administration of this factor, colony-stimulating factor 1 permits the differentiation of osteoclasts, and eruption occurs. NEW THEORIES OF ERUPTION By Inger Kjaer-2013 Hypothesis : A tooth that will erupt depends on Space in the eruption path. Lift or pressure from below. Adaptability in the periodontal membrane. SPACE IN THE ERUPTION PATH The crown follicle destroys overlying bone tissue and thus creates the necessary space in the eruption path. The molecular-biological processes depend on the ectoderm in the dental follicle. Lift or pressure from below The hypothesis is that the root membrane functions as a glandular membrane. The innervation in the membrane causes, as in the glandular endcells, an overpressure that supplants to the root surface, periodontal membrane, and pulp tissue . This pressure causes the tooth to elevate in the eruption direction. The process can be compared to the innervation of a gland that affects pressure conditions and provokes glandular secretion. Adaptability in the periodontal membrane The adaptability or reorganization in the periodontal membrane is the third factor that is essential for eruption. A proof for this reorganization process is that cell necrosis— apoptosis has recently been demonstrated of the innermost root-close layer of the periodontium in erupting teeth. An apoptotic cell layer has been demonstrated in both primary and permanent teeth undergoing eruption movements FINALLY???? In summary, the aetiology behind the eruption process is that an innervation -provoked pressure in the apical part of the tooth results in an eruption that requires continuous adaptation from the periodontal membrane and the active movement of the crown follicle, destroying overlying bone tissue. CHRONOLOGY OF TOOTH ERUPTION Chrono ---- time Logos ---- study Definition - Chronology can be defined as the study which deals with the timings of the various stages of tooth development ,starting with the initiation of the 1st dental tissue laid down to the emergence of tooth into the oral cavity & its completion of calcification. Chronology of primary dentition Chronology of permanent dentition Lunt and Law 6+4 rule 6 Months = 4 Erupted Teeth 18 Months = 12 Erupted Teeth 24 Months = 16 Erupted Teeth 12 Months = 8 Erupted Teeth 30 Months = 20 Erupted Teeth Rule of “FOURS” for permanent teeth development Birth – 4 first molars have initiated calcification 4 years – all crowns have initiated calcification 8 years – all crowns completed 12 years – all crowns emerge 16 years – all roots completed Rule of “SIXES” in dental development 6 weeks old in utero – beginning of dental development 6 months old – emergence of first primary tooth 6 years old – emergence of first permanent tooth RHYTHM OF ERUPTION The circadian rhythm in eruption is potentially significant in clinical practice. Studies indicate that circadian rhythm exists during the pre-functional stage of eruption of human teeth. It is also believed that effect on eruption on supine position versus upright position during the night could be due to a change in the intra oral pressure against the erupting tooth from either resting soft tissue pressure or functional intra oral pressure (e.g. swallowing). Clinical significance 1) Timing of eruption: The amount of force, its direction, and its total hours of wear of appliance often are considered as the most important clinical factor that affects the treatment outcome. If teeth erupt primarily during the night with little or no net of eruption during the day, it is quite possible that wearing an appliance is effective during the night when the eruption is most active. 2) Daily rhythm in skeletal growth: Ample evidence demonstrates the skeletal growth requires an adequate level of GH which increases in the night. The rhythm in tooth eruption also reflects this increase soon after the child goes to sleep. The clinician should be aware that there is a rhythm in skeletal growth and modification of treatment may be more effective at the night than during the day. 3) Effect of tooth movement more generally: Because eruption depends on metabolic activity within PDL, the rhythmicity associated with postemergent eruption almost surely reflects a rhythm in PDL activity. The cellular activities of periodontal fibroblasts have a periodicity similar to eruption and orthodontic movements are also related to cellular activity in PDL. Therefore at the time of treatment planning clinician should explore fully this periodicity of periodontal cellular activity for the control of pain and hyalinization or undermined resorption. TO BE CONTINUED…. REFERENCES AR Tencate’s Oral Histology Orban’s Oral Histology & Embryology Mc Donald’s Dentistry for child and adolescent Tooth Eruption: Theories and Facts-S.C. MARKS, JR. AND H.E. SCHROEDER-1996 WILEY-LISS, Eruptive tooth movement — the current state of knowledge;H. L. Craddock and C. C. Youngson-British Dental Journal 2004 the Eruption Mechanism of Human Tooth Eruption: Review Article Including a New Theory for Future Studies on Process-2014.