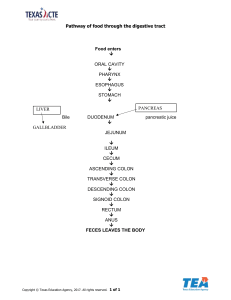
Digestive system 1. Lynn has a family history of colon cancer and is scheduled for a screening colonoscopy. During the procedure, three polyps were discovered and removed via hot biopsy forceps technique. The polyps were reported as benign. What diagnoses and procedure(s) codes capture these services? a. 45315, 45331 b. 45384 c. 45378 d. 21130, 45378, 45384 2. Dr. Blue performs a secondary closure of the abdominal wall for evisceration (outside the postoperative period). He opens the former incision and removes the remaining sutures; necrotic fascia is debrided down to viable tissue. The abdominal wall is then closed with sutures. How would you report the closure? a. 11043 b. This is a bundled procedure and not reported c. 39541 d. 49900 3. Heather lost her teeth following a motorcycle accident. She underwent a posterior, bilateral vestibuloplasty, which allows her to wear complete dentures. How would you report this procedure? a. 40845, 15002 b. 40843-50 c. 40844 d. 40843 4. Dr. Erin is treating a 58-year-old male patient with a history of chewing tobacco. Dr. Erin finds a 3.4 cm tumor at the base of his tongue. She places needles under fluoroscopic guidance for sub-sequential interstitial radioelement application. How would you report the professional services? a. 41019, 77002-26 b. 41019, 77012-26, 77021-26 c. 61770, 41019-59 d. 77002 5. An 88-year-old male patient suffering from dementia accidentally pulled out his gastrostomy tube during the night. Dr. Keys, an interventional radiologist, takes him into an angiography suite, administers moderate sedation (an independent observer was present during the procedure), probes the site with a catheter and injects contrast medium for assessment and tube placement. Dr. Keys finds that the entry site remains open and replaced the tube into the proper position. The intra-service time for the procedure took 45 minutes. How would Dr. Keys report his services? a. 49440, 99149, 99150 b. 49440, 49450-59 c. 49450, 99144, 99145 d. 49450 6. Katherine had a hernioplasty to repair a recurrent ventral incarcerated hernia with implantation of mesh for closure. The surgeon completed debridement for necrotizing soft tissue due to infection. How would you report this procedure? a. 49566, 11005-51, 49568 b. 49565, 11005-51, 49568 c. 49565 d. 49525, 11006, 49568-51 7. A 28-year-old patient underwent a proctosigmoidoscopy with ablation of five tumors under moderate sedation. The same provider performed the procedure and the sedation. The intra-service time for the procedure was 30 minutes. How would you report this procedure? a. 45320-P1 b. 45320 x 5 c. 45320 d. 45320, 99144 8. Harry had a sphincterotomy and an ERCP with a stent placed into the bile duct. How would you report this procedure? a. 43268, 43262 b. 43262 c. 43260, 43268 d. 43264 9. Incidental appendectomy during an intra-abdominal surgery does not usually warrant a separate identification. If it is necessary to report a separate identification, what modifier should you add? a. 52 b. 59 c. 51 d. 57 10. Sharon had a laparoscopic cholecystectomy with cholangiography. How would you report this procedure? a. 47605, 47570-59 b. 47605 c. 47563 d. 47579 11. A 52-year-old patient is admitted to the hospital for chronic cholecystitis for which a laparoscopic cholecystectomy will be performed. A transverse infraumbilical incision was made sharply dissecting to the subcutaneous tissue down to the fascia using access under direct vision with a Vesi-Port and a scope was placed into the abdomen. Three other ports were inserted under direct vision. The fundus of the gallbladder was grasped through the lateral port, where multiple adhesions to the gallbladder were taken down sharply and bluntly: The gallbladder appeared chronically inflamed. Dissection was carried out to the right of this identifying a small cystic duct and artery, was clipped twice proximally, once distally and transected. The gallbladder was then taken down from the bed using electrocautery, delivering it into an endo-bag and removing it from the abdominal cavity with the umbilical port. What CPT and ICD-9 codes should be reported? A. 47564 C. 47610 B. 47562 D. 47600, 12. A 70-year-old female who has a history of symptomatic ventral hernia was advised to undergo laparoscopic evaluation and repair. An incision was made in the epigastrium and dissection was carried down through the subcutaneous tissue. Two 5-mm trocars were placed, one in the left upper quadrant and one in the left lower quadrant and the laparoscope was inserted. Dissection was carried down to the area of the hernia where a small defect was clearly visualized. There was some omentum, which was adhered to the hernia and this was delivered back into the peritoneal cavity. The mesh was tacked on to cover the defect. What procedure code(s) should be used? A. 49560, 49568 C. 49652 B. 49653 D. 49653, 49568 14. An 82-year-old female had a CAT scan which revealed evidence of a proximal small bowel obstruction. She was taken to the Operating Room where an elliptical abdominal incision was made, excising the skin and subcutaneous tissue. There were extensive adhesions along the entire length of the small bowel: the omentum and bowel were stuck up to the anterior abdominal wall. Time- consuming tedious lysis of adhesions was performed to free up the entire length of the gastrointestinal tract from the ligament to Treitz to the ileocolic anastomosis. The correct CPT code is: A. 44005 B. 44180-22 C. 44005-22 D. 44180-59 15. 55-year-old patient was admitted with massive gastric dilation. The endoscope was inserted with a catheter placement. The endoscope is passed through the cricopharyngeal muscle area without difficulty. Esophagus is normal, some chronic reflux changes at the esophagogastric junction noted. Stomach significant distention with what appears to be multiple encapsulated tablets in the stomach at least 20 to 30 of these are noted. Some of these are partially dissolved. Endoscope could not be engaged due to high grade narrowing in the pyloric channel. It seems to be a high grade outlet obstruction with a superimposed volvulus. What code should be used for this procedure? A. 43246-52 B. 43241-52 C. 43235 D. 43234 16. The patient is a 78-year-old white female with morbid obesity that presented with small bowel obstruction. She had surgery approximately one week ago and underwent exploration, which required a small bowel resection of the terminal ileum and anastomosis leaving her with a large inferior ventral hernia. Two days ago she started having drainage from her wound which has become more serious. She is now being taken back to the operating room. Reopening the original incision with a scalpel, the intestine was examined and the anastomosis was reopened , excised at both ends, and further excision of intestine. The fresh ends were created to perform another end- to-end anastomosis. The correct procedure code is: A. 44120-78 B. 44126-79 C. 44120-76 D. 44202-58 17. PREOPERATIVE DIAGNOSIS: Diverticulitis, perforated diverticula POST OPERATIVE DIAGNOSIS: Diverticulitis, perforated diverticula PROCEDURE: Hartman procedure, which is a sigmoid resection with Hartman pouch and colostomy. DESCRIPTION OF THE PROCEDURE: Patient was prepped and draped in the supine position under general anesthesia. Prior to surgery patient was given 4.5 grams of Zosyn and Rocephin IV piggyback. A lower midline incision was made, abdomen was entered. Upon entry into the abdomen, there was an inflammatory mass in the pelvis and there was a large abscessed cavity, but no feces. The abscess cavity was drained and irrigated out. The left colon was immobilized, taken down the lateral perineal attachments. The sigmoid colon was mobilized. There was an inflammatory mass right at the area of the sigmoid colon consistent with a divertiliculitis or perforation with infection. Proximal to this in the distal left colon, the colon was divided using a GIA stapler with 3.5 mm staples. The sigmoid colon was then mobilized using blunt dissection. The proximal rectum just distal to the inflammatory mass was divided using a GIA stapler with 3.5 mm staples. The mesentary of the sigmoid colon was then taken down and tied using two 0 Vicryl ties. Irrigation was again performed and the sigmoid colon was removed with inflammatory mass. The wall of the abscessed cavity that was next to the sigmoid colon where the inflammatory mass was, showed no leakage of stool, no gross perforation, most likely there is a small perforation in one of the diverticula in this region. Irrigation was again performed throughout the abdomen until totally clear. All excess fluid was removed. The distal descending colon was then brought out through a separate incision in the lower left quadrant area and a large 10 mm 10 French JP drain was placed into the abscessed cavity. The sigmoid colon or the colostomy site was sutured on the inside using interrupted 3-0 Vicryl to the peritoneum and then two sheets of film were placed into the intra- abdominal cavity. The fascia was closed using a running #1 double loop PDS suture and intermittently a #2 nylon retention suture was placed. The colostomy was matured using interrupted 3-0 chromic sutures. I palpated the colostomy; it was completely patent with no obstructions. Dressings were applied. Colostomy bag was applied. Which CPT code should be used? A. 44140 B. 44143 C. 44160 D. 44208 18.Patient is going into the OR for an appendectomy with a ruptured appendicitis. Right lower quadrant transverse incision was made upon entry to the abdomen. In the right lower quadrant there was a large amount of pus consistent with a right lower quadrant abscess. Intraoperative cultures anaerobic and aerobic were taken and sent to microbiology for evaluation. Irrigation of the pus was performed until clear. The base of the appendix right at the margin of the cecum was perforated. The mesoappendix was taken down and tied using 0-Vicryl ties and the appendix fell off completely since it was already ruptured with tissue paper thin membrane at the base. There was no appendiceal stump to close or to tie, just an opening into the cecum; therefore, the appendiceal opening area into the cecum was tied twice using figure of 8 vicryl sutures. Omentum was tacked over this area and anchored in place using interrupted 3-0 Vicryl sutures to secure the repair. What CPT and ICD-9-CM codes should be reported? A. 44950, 540.1 B. 44960, 49905, 540.1 C. 44950, 49905, 540.0 D. 44970, 541 19. 15 year-old female is to have a tonsillectomy performed for chronic tonsillitis and hypertrophied tonsils. A McIver mouth gag was put in place and the tongue was depressed. The nasopharynx was digitalized. No significant adenoid tissue was felt. The tonsils were then removed bilaterally by dissection. The uvula was a huge size because of edema, a part of this was removed and the raw surface oversewn with 3-0 chromic catgut. Which CPT code(s) should be used? A. 42821 B. 42825, 42104-51 C. 42826, 42106-51 D. 42842 20. 34-year-old male developed a ventral hernia when lifting a 60 pound bag. The patient is in surgery for a ventral herniorrhaphy. The abdomen was entered through a short midline incision revealing the fascial defect. The hernia sac and contents were able to easily be reduced and a large plug of mesh was placed into the fascial defect. The edge of the mesh plug was sutured to the fascia. What procedure code(s) should be used? A. 49560 B. 49561, 49568 C. 49652 D. 49560, 49568 21. A 67-year-old male patient with a history of carcinoma of the sigmoid colon is referred for a diagnostic colorectal cancer screening. The patient completed all treatment for his cancer in 2004. The physician performed a diagnostic flex sigmoidoscopy exam to screen for recurrent colon cancer and examine the anatomic site. During the exam, the physician found three polyps in the rectosigmoid junction. They were removed by hot biopsy forceps. The path report indicated the polyps were benign. Code the encounter. A. 45333, V10.05, 211.3 C. 45338, V10.05 B. 45331, V12.72, 211.3 D. 45339, 211.3, V12.72 22. Postoperative Diagnosis: Calculi of the gallbladder Procedure: Removal of gallbladder Indications: The patient is a 40-year-old woman who has a six month history of RUQ pain, which ultrasound revealed to be multiple gallstones. She presents for removal of her gallbladder. Procedure: The patient was brought to the OR and prepped and draped in a normal sterile fashion. After adequate general endotracheal anesthesia was obtained, a trocar was placed and CO2 was insufflated into the abdomen until an adequate pneumoperitoneum was achieved. A camera was placed at the umbilicus and the gallbladder and liver bed were visualized. The gallbladder was enlarged and thickened, and there was evidence of chronic inflammatory changes. Two additional ports were placed and graspers were used to free the gallbladder from the liver bed with a combination of sharp dissection and electrocautery. Several attempts were made before it was decided that additional exposure was needed and I converted to an open approach. The trocars were removed and a midline incision was made. At this time, it was clear that there were multiple adhesions in the area, and once these were carefully taken down, we were able to grasp the gallbladder. The cystic duct was carefully ligated and the gallbladder carefully removed from the field. The area was copiously irrigated, and a needle biopsy of the liver was taken. Then the skin was reapproximated in layers. Sponges and needle counts were correct, and the patient was taken to the recovery room in good condition. A. 47600-22 C. 47562, 47600-22, 47001 B. 47600-22, 47001 D. 47562-22, 47000 23. A patient with rectal bleeding undergoes a proctosigmoidoscopy. During the proctosigmoidoscopy, the physician identifies internal hemorrhoids. The proctoscope was withdrawn, and the anus was prepped and draped. A field block with Marcaine 0.25% was then placed. Anoscope was inserted. There was a prolapsing hemorrhoid in the anterior midline. This was rubber band ligated by applying two bands. In the posterior midline, there was another hemorrhoid that was banded in the same manner. Code the procedures. A. 46221, 45300-51, 46600-51 C. 46945, 45300 B. 46221, 45300-51 D. 46934, 45300-51, 46600-51 24. A patient diagnosed with GERD presents to the same day surgery department for an upper GI endoscopy. The procedure is done in order to treat the GERD by delivering thermal energy to the muscle of the gastric cardia and lower esophageal sphincter. Anesthesia was administered and as the physician begins the procedure, the patient’s blood pressure drops to a dangerously low level. The physician decides not to finish the procedure due to the risk it may cause the patient. What are the codes for this procedure and diagnosis? A. 43257-73, 530.7, 458.8 C. 43257-74, 530.81, 458.29 B. 43499, 530.81, 458.9 D. 43257-53, 530.81, 458.29, V64.1 25. Preoperative diagnosis: History of prior colon polyps Postoperative diagnosis: Colon polyps, diverticulosis, hemorrhoids Procedure: A rectal exam was performed and revealed small external hemorrhoids. The video colonoscope was passed without difficulty from anus to cecum. The colon was well prepped. The instrument was slowly withdrawn with good views obtained throughout. There was a 3 mm polyp in the proximal ascending colon. This polyp was removed with hot biopsy forceps and retrieved. There was a 4 mm rectal polyp located 10 cm from the anus in the proximal rectum. The polyp was removed by hot biopsy forceps. There was also moderate diverticulosis extending from the hepatic flexure to the distal sigmoid colon. Code the CPT® procedure(s). A. 45384 C. 45380, 45384 B. 45384, 45384-51 D. 45383 26. A patient with esophageal cancer is brought to the OR for subtotal esophagectomy. A thoracotomy incision is made and the esophagus is identified. The tumor is carefully dissected free of the surrounding structures. No invasion of the aorta or IVC is identified. The cervical esophagus is controlled with pursestring sutures and then transected above the sternal notch. The esophagus is then dissected free of the stomach and the entire specimen is removed from the chest cavity and sent to pathology. The stomach is then pulled into the chest cavity and anastomosed to the remaining cervical esophageal stump. The anastomosis is tested for patency and no leaks are found. Hemostasis is assured. The chest is examined for any signs of additional disease but is grossly free of cancer. The chest is closed in layers and a chest tube is place through a separate stab incision. The patient tolerated the procedure well and was taken to the PACU in stable condition. A. 43101 C. 43107 B. 43117 D. 43112 27. Patient with RUQ pain and nausea suspected of having a stone or other obstruction in the biliary tract is brought in for ERCP under radiologic guidance. Procedure: The patient was brought to the hospital outpatient endoscopy suite and placed supine on the table. The mouth and throat were anesthetized. Under radiologic guidance, the scope was inserted through the oropharynx, esophagus, stomach and into the small intestine. The ampulla of Vater was cannulated and filled with contrast. It was clear that there was an obstruction in the common bile duct. The endoscope was advanced retrograde to the point of the obstruction, which was found to be a stone that was removed with a stone basket. The rest of the biliary tract was visualized and no other obstructions or anomalies were found. The scope was removed without difficulty. The patient tolerated the procedure well. A. 43260, 74328-26 C. 43265 B. 43264, 74328-26 D. 43269, 74329 28. Preoperative Diagnosis: Lower left inguinal pain Postoperative Diagnosis: Inguinal hernia Procedure: This 30-year-old patient presented with lower left inguinal pain and on examination was found to have a left inguinal hernia. The decision to perform a left inguinal hernia repair was made. The procedure was performed in the outpatient hospital surgery center. Risks and benefits of the surgery were discussed with the patient and the patient decided to proceed with the surgery. A skin incision was placed at the umbilicus where the left rectus fascia was incised anteriorly. The rectus muscle was retracted laterally. Balloon dissector was passed below the muscle and above the peritoneum. Insufflation and deinsufflation were done with the balloon removed. The structural balloon was placed in the preperitoneal space and insufflated to 10 mm Hg carbon dioxide. The other trocars were placed in the lower midline times two. The hernia sac was easily identified and was well-defined. It was dissected off the cord anteromedially. It was an indirect sac. It was taken back down and reduced into the peritoneal cavity. Mesh was then tailored and placed overlying the defect, covering the femoral, indirect, and direct spaces, tacked into place. After this was completed, there was good hemostasis. The cord, structures, and vas were left intact. The trocars were removed. The wounds were closed with 0 Vicryl for the fascia, 4-0 for the skin. Steri-Strips were applied. The patient was awakened and carried to the recovery room in good condition, having tolerated the procedure well. What are the correct procedure and diagnostic codes? A. 49505-LT, 550.90 C. 49507-LT, 550.92 B. 49505-LT, 49568, 550.90 D. 49501-LT, 49568, 550.92 29. Preoperative Diagnosis: Chronic tonsillitis. Chronic adenoiditis. Postoperative Diagnosis: Same. Procedure: Tonsillectomy and adenoidectomy. Patient is a 24-year old male who was taken to the operating room and put under IV sedation by the anesthesia department. An initial curettage of adenoids was done and packing was placed. The left tonsil was then identified and dissected out extracapsular and removed with scissors. Hemostasis was maintained by packing the left tonsil. Next, the right tonsil was identified and incision was made. Dissection was done extracapsular and the right tonsil was then removed. Both the right and left tonsil were sent as specimens as well as adenoid tissue. What are the procedure and diagnosis codes. A. 42826, 42831-59, 474.01 C. 42821-50, 42809-59, 474.00, 474.01 B. 42826, 42831-51-59, 42809, 474.02 D. 42821, 474.02 30. Diagnostic upper GI endoscopy of the esophagus, stomach, and duodenum was performed after esophageal balloon dilation (less than 30 mm diameter) was done at the same operative session. Code the procedure(s). A. 43235 C. 43226, 43200 B. 43249 D. 43220, 43235 31. A patient with ongoing symptoms of weight loss, constipation, and blood in stool verified with occult testing underwent a rectal approach colonoscopy with snare removal of three colonic polyps. The pathology report, which was returned to the physician the same day of the procedure, revealed benign colon polyps. How should you report this? a. 44393, 211.3 b. 45385 x 3, 783.21, 564.00, 792.1, 211.3 c. 45378, 45385 x 3, 211.3 d. 45385, 211.3 32. A patient was fully prepped for a diagnostic colonoscopy; however, an object then shifted into the descending colon just below the splenic flexure. The physician was unable to advance the scope beyond the splenic flexure. How would you report this diagnostic colonoscopy? a. 44388-52 b. 45330 c. 45378-53 d. None of the above 33. Jennifer, a 3-year-old patient, swallowed a marble that became lodged in her esophagus. An esophagotomy via thoracic approach was completed for removal of the foreign body. The patient tolerated the procedure well and was returned to the recovery room in good condition. How should you code this procedure? a. 43045 b. 43020 c. 43215 d. 43135 34. An otherwise healthy 22-year-old patient was scheduled for repair of an incarcerated bilateral recurrent inguinal hernia. The patient was taken into a same-day OR, where she was prepped, positioned, and draped in the usual fashion. The anesthesiologist administered general anesthesia and indicated the patient was ready for the surgery to begin. The surgeon created the incision and started the procedure. At this point, the patient went into shock due to the surgery and the procedure was halted. The patient was stabilized and returned to the recovery room. How should the surgeon report this procedure? a. 49507-74, 998.0, 550.10, V64.1 b. 49521-53, 550.13, 998.0, V64.1 c. 00830-P1, 49521-51, 550.10, 998.0, V64.1 d. 49521-47, 550.13, 998.0, V64.1 35. How would the following case be coded? Preoperative diagnosis: Lesion, buccal submucosa, right lower lip Postoperative diagnosis: Same Procedure performed: Excision of lesion, buccal submucosa, right lower lip Anesthesia: Local Procedure: The patient was placed in the supine position. A measured 7x8 mm hard lesion is felt under the submucosa of the right lower lip. After application of 1% Xylocaine with 1:1000 epinephrine, the lesion was completely excised. The lesion does not extend into the muscle layer. The 8-cm wound was closed with complex mattress sutures to the submucosal level and dressed in typical sterile fashion. The patient tolerated the procedure well and returned to the recovery area in satisfactory condition. a. 40816, 210.4 b. 40814, 40831-51, 210.4 c. 40814, 528.9 d. 40814, 210.4 36. A patient underwent an EGD with transendoscopic ultrasound-guided transmural fine needle aspiration. How should you code this procedure? a. 43242, 76942-26 b. 43242 c. 43235, 43238-59 d. 43235, 43242-51, 76942-26 37. A patient underwent a laparoscopic repair of a paraesophageal hernia with fundoplasty with implantation of mesh. During the procedure, a laparoscopic esophageal lengthening was completed. Which codes capture this procedure? a. 43327, 43282-59 b. 43333, 43283-51 c. 43281, 43282-59, 43283-51 d. 43282, 43283 38. A patient underwent an enterectomy in the small intestine with four resections and anastomoses. How should you report this type of procedure? a. 44130 b. 44120 x 4 c. 44111 d. 44120, 44121 x 3 39. Veronica, a 55-year-old patient, has left upper quadrant pain with a negative ultrasound. Veronica’s physician explains the need for a diagnostic and possible surgical procedure to determine the cause of this pain. She agrees to the procedure, completes overnight fast and prep, signs a consent for surgery, and is then taken to a procedure room. After nasal spray of 2% Xylocaine is administered, the tube is introduced through one nostril, down the back of the throat, and positioned into the stomach as the patient swallows. The diagnostic duodenal intubation and aspiration is completed. However, the physician decides to reposition the tube under fluoroscopic guidance and obtain multiple duodenal fluid specimens during the same operative session. The patient tolerates the procedure well and is moved to the recovery suite. How would you report the physician services? a. 43757 b. 43756, 43757-52 c. 43755 d. 43755, 43756-59, 43757-59 40. A patient has an adjustable gastric restrictive device component removed and replaced via a laparoscopic procedure. How should you code this procedure? a. 43773 b. 43772, 43773-51 c. 43888 d. 43845 ANSWERS 1. “b” This answer must have the diagnosis codes and procedure code. The diagnoses codes report special screening for the colonoscopy, family history of colon cancer, and benign polyps of the colon. The procedure code 45384 reports a therapeutic procedure with removal of the polyps. 2. “d” You can find this answer in the index of the CPT Professional Edition under Suture, Abdomen. 3. “d” You can find this answer in the index of the CPT Professional Edition under Vestibuloplasty. You can find the definition of the vestibule of the mouth at the beginning of the digestive system above code 40800. Modifier -50 isn’t necessary because the code description states “bilateral.” 4. “a” You should append modifier -26 to the radiology code to indicate the professional portion of this procedure. You can find this procedure in the index of the CPT Professional Edition under Placement, Needle, Interstitial Radioelement Application, Head. 5. “c” This is a replacement procedure via the same access site. The same provider who does the procedure reports the moderate sedation codes. You can find the rules for moderate sedation in Appendix G of the CPT Professional Edition. 6. “a” Use add-on code 49568 to report the implantation of the mesh in addition to debridement and hernioplasty. Modifier -51 is not attached to add-on codes (see Appendix A). 7. “c” The code 45320 includes moderate sedation. 8. “a” The parenthetical notes under code 43268 direct the use of code 43262 for the sphincterotomy. 9. “a” Report modifier -52. This statement is printed in the CPT Professional Edition under the code 44950. You can find this answer by looking up appendectomy in the index and cross referencing the codes. 1O.“c” Always review how the procedure is being performed – laparoscopy, excision, etc. This is a key to finding and reporting the correct code. 11. B One way to narrow down your choices is by the diagnosis. The patient has chronic cholecystitis. In the ICD-9-CM manual, look under cholecystitis/chronic, referring you to code 575.11. Verify code in the tabular section for accuracy. The patient had a laparoscopic cholecystectomy, eliminating multiple choice answers C and D. An examination of the bile duct was not performed, eliminating multiple choice answer A. 12. B The patient is having a laparoscopic ventral hernia repair, eliminating multiple choice answers A. The hernia is incarcerated as the report states that omentum was adhered to the hernia and was delivered back into the peritoneal cavity, eliminating multiple choice answer C. A parenthetical note in the code descriptive for the laparoscopic hernia repair codes state, that mesh insertion is included when reporting these codes when performed, eliminating multiple choice answer D 13. A Patient is having the surgery performed by a laparoscope, eliminating multiple choice answers B and C. The surgical procedure performed was an appendectomy, eliminating multiple choice D. 14. C This surgical procedure was not performed by a laparoscope: it was an open surgery, eliminating multiple choice answers B and D. It is documented the adhesions were “extensive” and the procedure was “time consuming” to free up the attachments to the gastrointestinal tract. These are key words in indicating modifier 22 should be appended to the procedure code. Appendix A lists the modifiers. 15. B The endoscopy was performed along with a placement of a catheter, eliminating multiple choice answers C and D. Since the placement was a catheter, multiple choice answer A is eliminated. The correct answer is 43241 with modifier -52 appended to indicate that the endoscope did not pass into the duodenum and/or jejunum. 16. A The surgery was not performed with a laparoscope, eliminating multiple choice answer D. The patient did not have a diagnosis of congenital atresia, eliminating multiple choice answer B. This was an unplanned return to the operating room due to the patient having a complication from the original surgery that was performed a week ago, eliminating multiple choice answer C. 17. B The surgery was not performed by a laparoscope, eliminating multiple choice answer D. The patient had a colostomy (Artificial surgical opening anywhere along the length of the colon to the skin surface for the diversion of feces) done, not an anastomosis (surgically creating a connection between bowel segments to allow flow from one to the other), eliminating multiple choice answer A. The op note documents that the distal left colon was divided and the sigmoid colon excised, eliminating multiple choice answer C. 18.B Patient had an open surgery appendectomy, eliminating multiple choice answer D. The scenario documents that there was also an abscess, eliminating A and C. The diagnosis is indexed under Appendicitis/with peritoneal abscess, referring you to code 540.1. Verify code in the tabular section for accuracy. 19. C The age of this patient is 15, eliminating multiple choice answer B. The patient only had tonsils removed eliminating multiple choice A. Part of the uvula was removed, eliminating multiple choice answer D. 20. D The surgery was not performed by a laparoscope, eliminating multiple choice answer C. There is no mention of the hernia being incarcerated or strangulated, eliminating multiple choice answer B. According to CPT guidelines in the hernia repair section, codes 49560-49566 can be reported with mesh add-on code, 49568. 21. A A sigmoidoscopy is performed for a diagnostic colorectal cancer screening since the patient has a history of colon cancer. During the procedure the removal of three polyps are done by hot biopsy forcep s. The correct procedure is 45333. Since the patient has a history of colon cancer, the V10.05 is coded. This is indexed in you ICD-9-CM manual, History/malignant neoplasm (of)/colon. Code 211.3 is coded since polyps were found. According to ICD-9-CM guidelines, when the patient is coming in for a screening exam only and a condition is discovered during the screening then the code for the condition is assigned as an additional diagnosis. So for this procedure, the polyps were discovered during the screening, not before, and can only be assigned as an additional diagnosis. 22. B. The removal of the gallbladder (cholecystecomy) was begun as a laparoscopic procedure. During the procedure, the surgeon decides that additional exposure is needed to complete the procedure. The procedure is converted to an open approach. When a laparoscopic approach is converted to an open approach, you code for the approach used to complete the surgery. You cannot code for both. Modifier 22 is appropriate for the additional work involved in the case. 47001 is coded to report the needle liver biopsy that was performed during this open procedure. 23. B. Hemorrhoids were removed by rubber band ligation, eliminating C and D. There were two different scopes used to indentify the internal hemorrhoids. Only code 45300 (Proctosigmoidoscopy) will be billed. 46600 (Anoscopy) is a “separate procedure,” meaning this is only coded when it is not an integral part of the another procedure performed at the same time. For this procedure, the doctor is removing the hemorrhoids while performing the anoscopy, making the anoscopy an integral component (included) in the procedure code for removal of the hemorrhoids. The 51 modifier is appended to the second procedure code since there was an additional procedure performed in the surgery. 24 .D. 43257 is the correct procedure for the Upper GI Endoscopy delivering thermal energy, eliminating multiple choice answer B. Modifier 73 and 74 are reported for the facility codes which eliminates answers A and C. The correct modifier for the physician’s service is 53. For the diagnosis codes GERD is indexed in the ICD-9-CM manual under Reflux/Gastroesophageal, you are referred to code 530.81. 458.29 is indexed under Hypotension/postoperative. V64.1 is reported to indicate the surgery was not carried out. 25. A. This colonoscopy involved polyps being removed by hot biopsy forceps which leads to code 45384. This is only coded once regardless of the number of polyps that was removed with this one technique. 26. D. You first need to look at the approach of the surgery, which is the physician incising the chest (thoracotomy) to expose the esophagus, eliminating multiple choice answer C. The physician is not removing a lesion from the esophagus; the physician is removing the esophagus (esophagectomy) and replacing it with the stomach, eliminating multiple choice answer A. The next key term to help you choose between procedure code 43112 and 43117 is “cervical”. 43112 is the correct code since the stomach is pulled through the middle of the chest into the neck and the stomach is connected to the stump of the esophagus in the neck (cervical). 27. B. Radiological guidance was used for this procedure; there are parenthetical notes that inform you for each of these ECRP procedure codes to use 74328 or 74329 for radiological supervision and interpretation, eliminating multiple choice answer C. Since the surgery is being performed in an outpatient hospital, the physician does not own the equipment so modifier 26 needs to be appended to radiology code eliminating multiple choice answer D. 43264 is the correct code since there was a removal of a calculus (stone) from the common bile duct. 28. A .To start narrowing down your choices, you need to identify the type of hernia. The operative note indicates that it is an inguinal hernia. Next does the op not mention if the hernia is incarcerated or strangulated? No, so this eliminates multiple choice answers C and D. Code 49568 (Mesh) would not be coded. According to CPT® guidelines the mesh is only coded for incisional hernia repairs. This statement is found in the subsection above the hernia repair codes. In the ICD-9-CM index, look up, Hernia/inguinal referring you to 550.9X. Your fifth digit is “0” since there is no indication in the op note that the hernia is recurrent or bilateral. 29. D. One way to narrow down your choices is by looking up the diagnosis first. In the ICD-9-CM index, look up Adenoiditis/with chronic tonsillitis, referring you to code 474.02. This eliminates multiple choice answers A and C. The patient is having a tonsillectomy and an adenoidectomy, which leads to code 42821. 30. B. Patient is having an Upper GI endoscopy, eliminating multiple choice answers C and D, which report esophagoscopy. Your key terms to look for are “balloon dilation” which is in code description 43249. 31. d. The definitive diagnosis of benign colon polyps should be reported, not the signs and symptoms for this question. The signs and symptoms would be appropriate if there was not a definitive diagnosis available for the study. The diagnostic colonoscopy is included with the surgical colonoscopy; therefore, only code 45385 is required for correct procedure reporting. 32. c. The CPT® Professional Edition includes a definition of colonoscopy and coding tips. In the coding tip for colonoscopy, modifier -53 is appropriate with documentation regarding non-advancement of the scope beyond the splenic flexure. 33. a. One way to find this procedure in the index of the CPT® Professional Edition is under the main term “Esophagus,” “Removal,” and “Foreign Bodies.” In this question, an esophagotomy was completed; therefore, you should not report a code for an endoscopic approach. 34. a. This question indicates anesthesia was started and then the condition of the patient changed. Modifier -74 indicates a discontinued procedure after administration of anesthesia and is appended to the surgery code. 35. c. The complex repair is included with this excision code and should not be reported separately. The diagnosis in this question is a lesion, not a neoplasm. 36. b. Code 43242 includes the ultrasound. Review the parenthetical notes with this code to help determine correct reporting. 37. d. One way to find this procedure in the index of the CPT® Professional Edition is under the main term “Laparoscopy,” then “Esophagogastric Fundoplasty” and/or “Esophageal Lengthening.” Review the definition for modifier -51 in Appendix A of the CPT® Professional Edition to help determine placement of this modifier. 38. d. The add-on code 44121 is reported for each additional resection and anastomosis of the small intestine. In this case, four total resections and anastomoses were completed; therefore, report the addon code with three units. 39. a. The diagnostic procedure is included with the surgical procedure and should not be reported separately. 40. a. One way to locate this answer in the index of the CPT® Professional Edition is under the main term “Laparoscopy,” then “Gastric Restrictive Procedures.” Once the code range is located, cross-reference for correct code selection.