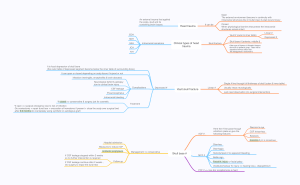
An external trauma that applied the scalp, skull and its containing brain tissues. Open The external environment become in continuity with intracranial structures like in bullet injury & stab wound injury Closed When physiological barriers that protect the intracranial structures remain intact It can be Head trauma Linear # EDH Vault # (outer & inner table) SDH SAH Intracranial hematoma ICH Clinical types of head trauma Skull fracture Depressed # Skull base # (anterior, middle & Other type of fractures is Diastatic fractures that occur in pediatric group . There will be separation between suture lines . The management is conservative IVH It is focal depression of skull bone (the outer table of depressed segment become below the inner table of surrounding bone) It can open or closed depending on scalp tissue if injured or not Infection (meningitis, encephalitis & brain abscess) Neurological deficit & epilepsy due to cortical brain injury CSF leakage Single # line through full thickness of skull (outer & inner table) Complications Depressed # Linear # Vault skull fracture Usually intact neurologically Just need observation (no surgical intervention) Pneumocephalus Intracranial bleeding *if closed => conservative & surgery just for cosmetic *if open => surgical emergency due to risk of infection -Do craniectomy + repair dural tear + evacuation of hematoma if present + close the scalp over surgical bed -after 6-9 months do cranioplasty using synthetic or autologous graft Treatment ACF # Here the # line pass through cribriform plate so give the following features Raccoon’s eye CSF rhinorrhea Epistaxis Anosmia if pt. is conscious Hospital admission Otorrhea Measures to reduce ICP Antibiotic prophylaxis If CSF leakage stopped within 2 weeks so no further intervention is required If CSF leakage continue after 2 weeks , Do surgery to repair the dural tear Follow up Otorrhagia Management => conservative Skull base # MCF # Hemotympani if no apparent bleeding Battle sign Facial N. injury => facial palsy Vestibulochoclear N. injury => hearing loss + disequilibrium PCF # => rare bcz occipital bone is hard Intracranial hematoma epidural 1. Extradural h.(EDH): • Hematoma between Inner table of skull bone and dura. • MMA injury. How occur? • 90% skull fracture. Most common • Frontal or temporal.site of EDH • Biconvex in CT. • Lucida interval. • Surgical emergency. Blood appear hyperdense on CT 2-subdural hematoma • Collection of blood in SD space. • Between brain and dura. Diffuse axonal injury • Associated with serious So patient usually in brain injury. comma • Mainly venous injury. Source • Acute, sub acute or chronic. Acute = hyperdensity Subacute = isodensity + mass effect • Cresent in CT Chronic = hypodensity كونسيرتف وهمات نطي فلود، كالسيوم جنل بلوكر 3. Subarachnoid hemorrhage: • Hrr. With in subarachnoid space. • Between arachnoid and piamater. • Due to head trauma. Or HTN • Due to ruptured cerebral aneurysm. • Occipital headach. Severe • Meningism. عندي وجع راس مصاير مثلة گبل سبيس اكوبانك ليشن 4. Intracerebral hematoma ICH • Bleeding within a cerebral parenchyma. • Due to torn perforating vesseles, cortical or sub cortical. • Traumatic or spontenious(hypertensi Hemorrhagic stroke on). • Commonly frontal or temporal. 5. Intraventricular hrr.( IVH) Either due to trauma or rupture of AV malformation • Bleeding into ventricular system. Serious presentation = comma state Bcz the trauma affect core of brain and associated with diffuse axonal injury Treatment conservative And surgery if bleeding cause hydrocephalus by clott formation - so Make external ventricular drainage system Hyperdense within the ventricular system and may there is air fluid level ..! Other type of injury is contusion of brain which usually occur in poles of brain There is coup and countercoup contusion due to acceleration & deceleration injury Presentation: same as that of SOL On CT we will see mixed or heterogenous density Management = conservative + surgical intervention in special circumstances focal affect كل هذا اللي حجينا هو diffuse effect اكو 1-concussion Transient, reversible loss of consciousness or neurological deficits ساعة٢٤ مؤقت ما يتجاوز It’s functional disturbance of neurons , not organic damage so on CT and MRI it’s normal Management = conservative, observation and reassurance 2-diffuse axonal injury It’s severe and serious injury that occur in head trauma and lead to comma state which need RCU admissions when GCS < 8. After stage of comma the patient will be in vegetative state 3-diffuse cerebral edema It’s called cytotoxic or malignant edema. We should use all conservative measures to control it & if we cannot we will use decompressive craniectomy Clinical presenration and squele: 1. Vital signs disturbance: BP, PR, RR, Temp. 2. Decreasing conscious level: GCS 3. Intracranial hypertension: signs and symptomes of raised ICP. 4. Pupillary examination(size and light reflex). False localizing sign 5. Cranial nerve palsies: abducent nerve is the commonest n. Involved because of the longest anatomical course. Optic and oculommotor فولز لوكاليزن ساين Hemiparesis Hemplegia Diplegia Quadriplegia 6. Motor weakness. 7. Sensory loss. 8. Respiratory irregularties: ataxic breathing, chyene- stokes breathing. 9. Herniation syndrom. 10. Brain death. Important in spinal cord injury not in head Brain has soft consistency so hematoma will compress it & result in herniation at following site Herniation syndrom • All line of management to prevent this .. Herniation beneath Subfalcine. falx cerebral or cingulate gyrus • Uncal. Herniation of medial part of temporal lobe through tentorium cerebelli & cause compression on brain stem • Central. Herniation of diencephalon through tentorium cerebelli Tonsilar = herniation of tonsils of cerebellum through foramen magnum Reverse or upward herniation occur in posterior cranial fossa tumor Management-- medical to reduce ICP --- 4H * head elevation 30 degree not more than it *hypothermia * hyperventilation *hypertonic solution such as manittol Surgeria - craniotomy - craniectomy -craniostomy or burrhole