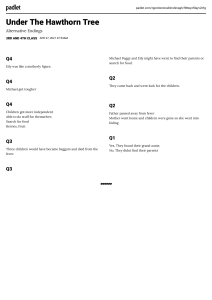
OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi C HA P TER 1 Parasites and humans 1.1 Mission impossible On New Year’s Day of 1880, the young Fernanda Lesseps stood on board of a steam launch in the mouth of the Rio Grande, some 15 km east of the modern city of Colòn, on the Carribean coast of the Isthmus of Panamà, then a province of neighbouring Colombia. On that day, she symbolically put a shovel full of sand into a box that had been emptied of its champagne bottles, to mark the start of the construction work for the Panama Canal. Fernanda was performing this symbolic act on behalf of her father, Count Ferdinand Lesseps. He was in his seventies and a public hero because of his success as the architect of the Suez Canal, which officially opened on 17 November 1869, and for which Guiseppe Verdi was commissioned to write an opera. (In fact, Verdi did not complete the piece in time, so his masterpiece Aida premiered in Cairo on 24 December 1871, with pomp and glamour.) Ferdinand Lesseps, therefore, had every reason to be confident that he would also succeed in constructing the long-desired maritime shortcut from the Atlantic to the Pacific Ocean in due time. For this purpose, Count Lesseps had just founded his new company ‘Compagnie Universelle du Canal Interocéanique’ to finance the work. Furthermore, in January 1881, around 200 engineers from France and other European countries, together with 800 labourers, had arrived in Colòn to start the building of the canal. How could Count Lesseps foresee that it would take 34 years, from his daughter’s act on New Year’s Day, and the involvement of American companies and engineers to finish the project? Eventually, the canal officially opened on 15 August 1914, by the passing of the vessel SS Ancon. Over this time, an estimated 80,000 people worked on the canal and more than 30,000 lost their lives in the effort. It was the parasites of the hot and humid lowlands of Panama that proved the hardest problem to overcome. But let us see what happened. Work on the canal began in 1882 along the route of the Panama Railroad that was constructed in 1855. Lesseps first started the task by erecting moorings, roads, and barracks for the labour force. But the lowland tropics were different from the Arabian deserts of the Suez Canal. In fact, social insects proved to be the first problem and an unexpected gateway to disaster. In particular, termites were quick to destroy the wooden constructions that had been erected. Furthermore, heavy trafficking by ants inside the barracks proved to be a nuisance and a challenge for maintaining hygiene. Lesseps, therefore, decided to put housings and storage facilities on wooden stilts. To prevent termites and ants gaining access to the buildings above, and to deter them from attacking the wooden structures, the stilts were placed in large, waterfilled drums. This counter-measure was a success and termites were no longer a problem. However, the tropics were far from defeated. These water drums soon attracted hordes of mosquitoes that used the pools as their breeding grounds. Whereas this created additional nuisances of more insect bites, the real threat emerged with the arrival of yellow fever, for which mosquitoes act as a vector. By the end of 1881, already some 2000 men were at work. In 1882, 400 deaths from yellow fever were reported, and in 1883 a total of 1300 men had died from 1 OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi 2 PARASITES AND HUMANS the disease. Probably as much as one-third of the labour force became infected at any one time. By December 1888, the rampaging yellow fever, together with the everincreasing cost of the construction, led to the financial collapse of Lesseps’ company, which was dissolved in February 1889. The ambitious work was stopped by a small, invisible parasite ( Wills 1996). Yellow fever is caused by a single-strand RNA virus belonging to the family of Flaviviridae (group B arboviruses), a family with several representatives causing severe haemorrhagic fevers (like Ebola or Lassa). The virus affects specialized surface cells, for example, in the liver, or the heart. The first symptoms appear three to six days after the infection with swellings and cell death. In the majority of cases, the infection is short and intense, and the patients fully recover; and recovered patients acquire a long-lasting immunity against the disease. In a minority of cases (around 15% of patients), however, the infection develops into a severe problem. Sudden high fever, yellow tint in the eyes, jaundice, and bleeding that leads to ‘black vomit’ are the typical symptoms. In the process, the liver cells are destroyed, which leads to acute liver failure (and so to jaundice). Such infections, if untreated, are associated with high case mortality of patients (40% of cases). The blood remains infective and can be transmitted further by mosquitoes during a period from the first to the third day of fever (Cook and Zumla 2008). Yellow fever is not initially native to the Americas but originated in West Africa. There, the virus has a reservoir in wild animals, especially in monkeys. With the increasing trade connections between Africa and the Caribbean in the sixteenth and seventeenth centuries, yellow fever spread by trading ships to the New World. It was first recorded in 1648 in the Yucatan peninsula and in the Spanish settlement of Havana, Cuba (where it was eliminated in 1901 by destroying the breeding sites of mosquitoes). Twenty years later, in 1686, yellow fever had reached Brazil and, in 1690, the island of Martinique. Yellow fever (as well as other African-origin diseases) was a prime factor in the depopulation of tropical America at these times. Following the trading routes, yellow fever subsequently jumped back from the Americas to the European continent, where it caused an outbreak in Cadiz, Spain, in 1730. Later, such outbreaks were also observed in Marseille, France, and in 1878 in England. After its first introduction in Central America, yellow fever had established an animal reservoir too, mainly in howler monkeys. Epidemic outbreaks in howler monkeys had repeatedly occurred, starting in Panama and spreading along the east coast of Central America to Guatemala. In 1914, Sir Andrew Balfour (1873–1931), then the founder of the Wellcome Museum of Medical Science and later (1923) first director of the London School of Hygiene and Tropical Medicine, noted that a yellow fever epidemic in Trinidad lead to a ‘silent forest’, since all Howlers had died from the infection (Balfour 1914; Cook and Zumla 2008). In the meantime, epidemiologists have elaborated on the forest cycle of yellow fever. For people of modern western civilizations, the fear induced by major diseases, such as yellow fever, is hard to imagine. Yellow fever, in fact, was one of the most feared diseases in the eighteenth and nineteenth centuries. Not only at the Panama Canal construction site, but also elsewhere, the French paid a heavy toll to this disease. Around 1800, for example, the French controlled large territories in the Caribbean, Central America, Mexico, Louisiana, and Canada. In 1801 a rebellion under the black leader Toussaint Louverture erupted in the French colony of Haiti. Napoleon was forced to send his brother-in-law, General Le Clerc, to subdue the rebellion, but over 27,000 troops, including Le Clerc himself, died from yellow fever within months after their arrival in Santo Domingo. At the same time, yellow fever had little effect on the black African rebels whose ancestors came from West Africa— the same region where yellow fever had been around for a very long time and where people were less susceptible to the infection. One consequence of the epidemic was that the French withdrew from the Americas and sold Louisiana to the United States (Oldstone 1998). But others suffered, too. During an epidemic in Philadelphia in 1793, the American capital at the time, the disease claimed over 10% of the population (around 40,000 people). Between 1793 and 1796, the British army in the Caribbean lost about 80,000 men, over half of them to yellow fever. Even in the peaceful period between 1817 and 1836, the annual death rate of British soldiers in the West Indies was six to ten times as high than at home, primarily due to diseases OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi SOME LESSONS PROVIDED BY YELLOW FEVER 3 Figure 1.1 A fumigation car for the control of yellow fever in Panama City, 1905. Such controls measures were used in preparation of the construction of the Panama Canal by American companies. Control of mosquito populations was first introduced by the US Army medical scientist Walter Reed and his team in Havana, Cuba, after 1900. Photo supplied courtesy of Panama Canal Museum. such as yellow fever. West Africa even became nicknamed the ‘White Man’s Grave’, mostly because of the widespread presence of yellow fever in this area; the associated mortality was thirty times as high as in the homeland (Crosby 1986). Ironically, African slaves were highly praised in the New World precisely because black Africans showed higher levels of resistance to the virus than did the native Indians of the Americas. Up to the early years of the twentieth century, massive yellow fever epidemics repeatedly swept through the Caribbean and up the North American coasts regularly terrifying people. Yellow fever remains a health problem in tropical America today. Local epidemics occurred as late as 1997–98 in Santa Cruz, Bolivia. Transmission in the jungle forest cycle is documented for the Amazon basin for the last decades and regular infections of humans occur in this area, usually with high case mortality rates. In the Amazon basin, recurrent epidemics are noticed every five to ten years, spreading along the tributaries of the river Amazon in accordance with the reestablishment of susceptible monkey populations in the gallery forests (Izurieta et al. 2009). As early as 1881, an Havanna physician, Carlos Juan Finlay, suggested that yellow fever was a mosquitoborne disease. In the Spanish–American War of 1898, the United States backed the rebels in Cuba and Puerto Rico. The presence of US military in these areas created the health problems that so generated political pressure to investigate the disease. With bold experiments in research stations just outside Havana, where volunteers were exposed to mosquitoes, the US Army medical scientist Walter Reed (1851–1902) and his team (‘The Reed Commission’) finally proved, in 1900, that yellow fever is indeed vectored by an insect (Aedes aegypti). This insight led to successful campaigns against mosquito breeding grounds. The control measures now made possible allowed completion of the construction of the Panama Canal during the years of 1906–1914 (Figure 1.1). By 1928 the South African virologist Max Theiler (1899–1972) and his Harvard mentor Andrew Sellards showed that the agent of yellow fever is a virus. In 1937, Theiler, then working at the Rockefeller Institute, developed a safe and successful vaccine that is still in use today, a discovery for which he was awarded the Nobel Prize in 1951. 1.2 Some lessons provided by yellow fever This dramatic piece of history illustrates a number of issues that will be covered in this book and we can list them as follows. OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi 4 PARASITES AND HUMANS 1.2.1 The parasite life-cycle can be complex Yellow fever is a parasite that needs a vector—a more or less passive transport vehicle—to get from one human host to the next. Not all parasites are transmitted in this way. Most can jump from one host to the next directly, for example, via air in close contact (e.g. influenza virus), by transfer of body fluids (e.g. HIV or Ebola virus), or by water over larger distances (cholera, typhoid bacteria). Some parasites have evolved to utilize an intermediate host. For example, the causative agent of bilharzia, the digenean trematode, Schistosoma mansoni, uses the freshwater snail, Biomphalaria glabrata, as its intermediate host from where it is transferred to the (final) human host, and then back again to the snail. In the final host, Schistosoma reproduces sexually and the eggs penetrate the host’s veins, intestines, or bladder, where they cause harm. A few parasites have incorporated more than two hosts in their life-cycle, such as the lancet liver fluke (Dicrocoelium dendriticum) that passes through hosts of three phyla: snails (mollusca), insects (arthropoda), and then to a vertebrate (chordata). Finally, a large number of insect species have evolved to become parasitoids. Parasitoid larval stages are inside or on the surface of a host from which they extract their resources. The adult insect is free-living, searches for mates, and lays its eggs or larvae again into a host, on its surface, or at least in its vicinity. These variations on a theme have many consequences for the ecology and evolution of host–parasite interactions. 1.2.2 Not all host and parasite strains are the same Not all people infected by yellow fever progress to the second, more dangerous stage of the disease. Similarly, West Africans proved more resistant to yellow fever than French or British soldiers. In other words, hosts within or among populations vary in their susceptibility to a given parasite. On the other hand, not all yellow fever strains are the same either. Today, epidemiologists distinguish between urban yellow fever that is transmitted by the mosquito, Aedes aegypti, and which is prevalent in tropical urban areas. Sylvatic or jungle yellow fever is the same parasite but a variant that primarily causes a disease of monkeys in the tropical forests of South America and Africa. Humans only occasionally become hosts. It is transmitted by various species of mosquitoes. In addition, the infection is transmitted to offspring of an infected female mosquito from where it can again infect a monkey or a human. Differences not only exist between urban and jungle forms of yellow fever, there are also more or less virulent strains in general. For example, the standard yellow fever vaccine (YF-VAX) is based on strain 17D that was originally isolated from a patient named Asibi. The properties of this strain allowed Max Theiler to maintain it in cell culture, where it could be attenuated to become a safe, live vaccine. Hence, variants of the parasite play an obviously important role. Against the background of various flu epidemics caused by different strains (such as influenza type H1N1 ‘swine flu’, H5N1 ‘bird flu’, etc.), this has become an issue in our days again. 1.2.3 Complex physiological and molecular mechanisms underlie the infection The yellow fever virus has to reach a new host through the bite of an infected mosquito. Once inside the bloodstream of the human host, it must enter a target cell and multiply. These processes unfold at the physiological and molecular level, where a range of different proteins and biochemical mechanisms are involved. For example, the virus gains entry by a process of receptor-mediated endocytosis, i.e. it is ingested by the host cell. The synthesis of new viral RNA occurs in the cell cytoplasm. At the same time, the synthesis of viral proteins happens in the endoplasmic reticulum of the host cell. Then, new viruses (the virions) are assembled and can infect the next cells. Many of the proteins responsible for these processes have been identified. For example, structure protein C binds RNA to the viral nucleocapsid and thus ensures proper packaging of the genetic information (on RNA) into a (protein) capsule. The protein NS1 is involved in viral assembly and affects the release from the host cells. Viral structural protein E is an envelope protein crucially important for the attachment of virions to host cells, but also for haemaggluttination (clotting of red blood cells) and virus neutralization by the host. Changes in this protein are associated with a change of virulence and attenuation of virus strains. The host’s immune system OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi SOME LESSONS PROVIDED BY YELLOW FEVER responds to infection by activating a number of signalling cascades and expressing the genes responsible for anti-viral defence; this includes the recruitment of lymphocytes that are able to recognize virus-infected cells and destroying them. This machinery is exceedingly complex and will be treated in more detail in Chapter 4. Note that parasites like yellow fever requiring a vector for transmission not only have to outwit the human (vertebrate) immune system, but also, for instance, that of the mosquito (an insect). These physiological and molecular mechanisms produce macroscopic phenomena that we know as parasite virulence and host resistance. Furthermore, these mechanisms are based on genes that become differentially expressed at various stages of infection, replication, and transmission. There is, therefore, a distinction between the mechanisms that lead to a certain outcome of the infection, the underlying genetic basis for these mechanisms, and the function of parasite virulence and host resistance, that is, their value for survival and reproduction (the fitness) of host and parasite. Indeed, there is overwhelming evidence that virulence and resistance are traits that show phenotypic and genotypic variation within populations and are able to evolve. We must, therefore, expect that these traits have been shaped by natural selection to increase the fitness of the carriers. Although it is necessary to consider the underlying physiological and molecular mechanisms, the mechanisms cannot answer questions about adaptive value and fitness, and vice versa. 1.2.4 Parasites and hosts are populations Parasites and hosts consist of individuals that form interacting populations. On the ecological scale, a population dynamic process unfolds from this interaction. Throughout history, yellow fever has caused many epidemics in different parts of the world. An epidemic emerges from the processes of infection, replication, and transmission of the parasite to the next host. This in turn depends on susceptibility, resistance, and clearing of infections by the hosts. But an epidemic is also an ecological process in which two species (host and parasite) interact with each other; their relative numbers, densities, and population 5 dynamics produce the changes in the level of infection over time. An epidemic is, therefore, as much governed by the laws of ecology and population dynamics as it depends on molecular mechanisms. At the same time, the interaction of the two populations generates selection for host and parasite. Therefore, hosts and parasites also change by the process of evolution as an epidemic unfolds. Hosts might not only become protected individually by their immune memory, but the host population as a whole adapts to the parasite through selective deaths. Descendants inherit the selected favourable resistance traits and will be protected for some time until a new epidemic starts with a different parasite or a sufficiently different variant of the same. Epidemics strongly remind us that host–parasite interactions are also a piece of evolution and ecology, not just of molecular biology. 1.2.5 Parasites can be controlled when we understand them The control of yellow fever is achieved by the control of mosquito breeding grounds as initially suggested and carried out in Havana by Walter Reed and his team. In addition, the host population can be protected by mosquito nets and by vaccination. The yellow fever vaccine is one of the safest known and it provides protection for at least ten years. Vaccination is possible because the vertebrate immune system contains memory cells that allow a faster and more efficient response to a second challenge of the same kind. Such highly specific memory is particular to the higher vertebrates but may exist in similar form in invertebrates too (Kurtz 2004). Not all vaccines and parasites allow for such a safe and durable protection, however. How protective memory forms is a question of immunology. However, ecology and evolutionary biology tell us that the consequences of vaccination are not only restricted to the individual host that gains protection, rather, vaccination alters the selection regime for the parasite population as a whole. Successful vaccination protects one part of the host population from infection and thus decreases the number of available hosts for the parasite. If enough hosts are so protected, the parasite may find itself unable to find a new host and becomes eliminated. On the other hand, the vaccine-associated OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi 6 PARASITES AND HUMANS selection pressure on the parasite leads to adaptations that might counteract the effect of the vaccine in the long term, especially when vaccination is not perfect. Again, we are reminded that the study of host–parasite interactions is not possible without an integrated approach that spans all levels from molecules to ecology and evolution. This approach touches on the traditional fields of population biology, behavioural studies, genetics, immunology, parasitology, physiology, biochemistry, or molecular biology to mention some. Furthermore, it requires the tools used in ecological and behavioural field studies, laboratory experiments, molecular techniques, mathematical modelling, computing, and a good nose for what might be going on between hosts and parasites. In fact, studying parasites and their ways has often be equated with the work of a detective (De Kruif 1926) and much of the fascination of the subject comes from the vast and yet unexplored terrain on which hosts and parasites—to paraphrase George E. Hutchinson (1903–91)—act out their evolutionary play in the ecological theatre. 1.3 Parasites in our times Is the worry about parasites and epidemics a thing of the past? Not really. Whereas we have vastly better means to deal with novel pathogens, parasites are not only present in less-developed countries, but are also a source of disquiet for the industrialized countries with high living standards (Barrett et al. 1998). Even conservative estimates suggest that hundreds of millions of people are infected by parasites worldwide and many thousands die because of infections every year. Influenza is an example well-known to the industrialized countries. It has a very long history in human populations, dating back to antiquity. A major pandemic (an epidemic spanning large parts of the world) was already recorded in the late-sixteenth century. Today, three types of influenza viruses (types A, B, and C) circulate, with types A and B the most prevalent and dangerous ones. Influenza virus has only eleven genes (!)—apparently enough to cause a lot of trouble. Type A viruses especially have caused major epidemics in recent history. Undoubtedly, the most famous pandemic is the one caused by H1N1-type (strains are labelled by the type of haemagglutinin, H, and neuraminidase, N) from spring to winter 1918 (the ‘Spanish flu’). It had a much higher casemortality rate than any recorded strain before and killed somewhere between 20 and 40 million people—equivalent to the number of casualties during World War I. The relationship of Spanish flu to swine and avian reservoirs is unclear. It is possible that swine served as host where influenza virus evolved before breaking out into the human population (Bush 2007). Influenza caused another major epidemic in 1957 (types H2N2 ‘Asian flu’ and H3N2 ‘Hong Kong flu’), starting from China and spreading worldwide. This pandemic strain emerged from a recombination of the still circulating H1N1- strain and elements of avian flu. The new strain displaced the old H1N1 in the process. In 1968, a human H2N2-strain again re-assorted with avian influenza virus to produce the pandemic H3N2 ‘Hong Kong flu’. And yet again, the previously circulating strains were displaced. Such serial replacement was undercut with the re-appearance of H1N1 in 1977 in China but which now caused only mild symptoms. H1N1 and H3N2 have now been circulating in humans for several decades. Seasonal influenza is a common occurrence and no real cause for major worries. As the historical record and the analysis of viral serotypes and genotypes show, this normal pattern is interrupted by major pandemic strains at intervals of some ten to twenty years. Such strains often emerge by recombination of human-adapted virus with elements of others, notably bird- or swine-adapted influenza. Against this background, the outbreak of bird flu hit the news in 2004. But avian influenza was no newcomer but had already been noticed in 1959; worldwide (up to 2006) it had caused 24 highly pathogenic outbreaks in birds (poultry), although each within a limited geographic area. Avian influenza is caused by several type A strains, of which four (H5N1, H7N3, H7N7, H9N2) have infected humans. Of those, strain H5N1 proved to cause the major worries as it seemed to readily cross the species’ barrier and jump from birds to humans. The case of 2004 was not the first appearance of H5N1. The strain had already been isolated from a goose in China in 1996. It was then seen in 1997 in Hong Kong, where it infected chicken and was transmitted to humans (18 cases, six deaths) and again in Hong Kong in February 2003 (two cases, one death). In OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi PARASITES IN OUR TIMES 1997, around 1.5 million chickens were culled to contain the disease. In late 2003, a highly pathogenic flu virus hit farms in Vietnam, confirmed as type H5N1 in January 2004; thousands of birds were culled but soon a few humans were hospitalized with severe respiratory illness that turned out to be H5N1 infections. During 2004, H5N1 continued to spread among birds in Japan, Hong Kong, Thailand, Cambodia, Laos, China, Indonesia, and Malaysia. At the same time, cases of human infections and fatalities accumulated in Vietnam and Thailand. The situation was very similar in 2005 when the virus spread further to Russia and central Asia. H5N1-viruses reached poultry in Turkey, wild birds in Croatia, and was found in an imported parrot in the UK in October 2005. By early 2006, the flu had spread further in wild bird populations, primarily waterfowl (swans), that were embarking on their spring migration. The study of bird migration, so far considered an enjoyable hobby of bird lovers and conservationists, suddenly looked like an important topic for human health. Also, human flu infections continued to occur. The symptoms were variable but nevertheless caused fatalities in many cases. Not surprisingly then, the scare in Europe and North America reached new heights. With few exceptions, it still seemed that bird-to-human transmission was the relevant route of infection. One reason seems to be that avian virus infects the lower respiratory tract (lungs), allowing for rapid progression to pneumonia, but from where it is not so readily transmitted, compared to human influenza viruses that primarily reside in the nose and throat. But analyses of viruses circulating in Asia during 2005 had shown that several amino acids near a receptor-binding site (affecting transmissibility) were changing. The virus was thus evolving and perhaps capable of direct human-to-human transmission. As the autumn of 2006 approached, more humans became infected, mainly in Asia and the Near East, and some viral isolates now carried mutations that made them resistant to some anti-viral drugs. Trade restrictions were put in place by many countries. In Germany, army contingents were deployed to control access to outbreak areas; people had to leave and enter through locks with disinfectants. Some panic buying of food items set in. Worries that there might not be enough medication or facemasks for everybody became prominent. Inevitably, religious 7 fanatics claimed the epidemic to be a fulfilment of divine prophecies. But then, in the winter of 2006–07, the major thrust of the epidemic in humans seemed to subside. Soon, H5N1 dropped out of the news and got forgotten. But H5N1 continues to infect birds (cases in Asia, Russia, Egypt, and Europe during 2009) and humans (cases in Egypt still reported in summer 2009). With rapidly-changing parasites, forgetting is not a good defence strategy. H5N1 is still among us. And an old foe, H1N1, came back as swine flu and was first noticed in spring 2009 in Mexico, although its actual origin is still controversial. Similar to the history of bird flu, a swine flu outbreak already had hit the US in 1976. This virus seemed to be related to H1N1 of the Spanish Flu. Hence, major concerns were issued and a nationwide vaccination campaign launched. Yet, the viruses never went far from the original area around Fort Dix, New Jersey. The H1N1 of 2009 was not really the same virus as before, however. The new swine flu virus transmitted easily from person-to-person causing flu-like symptoms but with generally mild effects similar to seasonal influenza. The virus spread like a bushfire, mainly among younger people. As of summer 2009, 168 countries or territories have reported the presence of H1N1. On 11 June 2009, the WHO declared the first flu pandemic since 1968. Fortunately, in hindsight, the effects were severe only in vanishingly few cases and the epidemic remained without much negative effect. The story of influenza viruses is in many ways similar to yellow fever, but influenza shows high rates of evolutionary change and can cause widespread epidemics much more easily. Clearly, direct transmission is a much better way to generate a pandemic than vector transmission, on which yellow fever depends. Because influenza is so changeable, it has been scrutinized as a case where the holy grail of evolutionary biology might be unlocked— the prediction of future evolution. The need is obvious: because it takes several months to produce a vaccine in large quantities, it would be an enormous advantage to be able to predict which viral strain is likely to cause the next seasonal influenza or even the next major pandemic. This attempt has so far met with limited success (Bush et al. 1999). Even for a simple organism like influenza A virus, it seems difficult to predict the course of future OUP CORRECTED PROOF – FINALS, 01/26/2011, SPi 8 PARASITES AND HUMANS evolution. There is no simple relationship between genetic sequence (which is what can be screened at large scales in a population) and the phenotype that determines the antigenic properties of the virus and thus the likelihood that it might successfully infect a host (Bush 2007). Nevertheless, progress is made and such predictions will certainly become more accurate in the not too distant future. These dramatic examples thus illustrate a number of issues that will be covered in this book and suggest that we humans should pay attention to our parasites. In fact, much of the progress in human medicine and welfare is due to improving public health by sanitation and hygiene, alongside the discovery of new medication. Progress can, therefore, not be confined to understand the physiological, biochemical, and molecular basis of how parasites and their hosts interact. Rather, the interaction is among living organisms that are subject to evolution by natural selection in a given ecological context. The traditional boundaries between fields are not helpful for this necessarily integrating approach and must be put aside. The terms ‘host’ and ‘parasite’ are probably the most universal ones throughout this book and they so capture the notion that the ultimate job is to understand how and why they interact in the way we see it, regardless from which field our wisdom comes from, and regardless of whether we take ‘parasite’ to mean a virus, nematode, or a parasitic insect. This is the idea this book will focus on. SUMMARY • Parasites have played an important but often underestimated role in human history. A virus (yellow fever) is one example of a deadly infection that changed the history of the Americas. • Major epidemics are still happening today. Influenza is a prominent case where recent outbreaks generated well-founded fears. • Human parasitic diseases illustrate the general principles. Only a combination of molecular understanding and insights from ecology and evolution will eventually be fruitful.