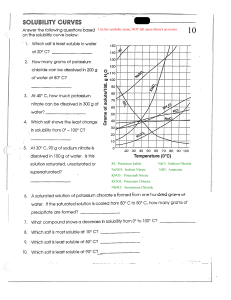
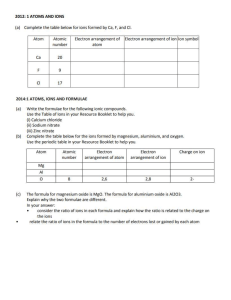
ELECTROLYTES DIETARY SOURCES OF ELECTROLYTES JUICE, calcium, chloride, vitamin c, Energy drinks are reach in electrolytes Are substances that help our organs to function normally like the analyte calcium and potassium that helps our heart to function properly. In electrolytes, we examine the sodium, magnesium, calcium, potassium and chloride. And these are the basic electrolytes that we are going to examine in clinical chemistry. There are some machines tatlo lang ang ineexamine, it is Sodium, Potassium, and the Calcium. Ang magnesium mejo special yan so mahal yung machine pag may magnesium and chloride or pag lima siya. Usual doon sa primary and secondary laboratories, we have only 3 electrolytes that are being examined. Going back to our laboratory, we have Primary, Secondary, and Tertiary Laboratory. The difference between Primary and Secondary is naidagdag ang electrolytes that’s why naging secondary sya. Electrolytes come from what you eat and drink Basics are Sodium, potassium, chloride They balance fluids in your body Maintain your blood’s proper pH They carry electrical signals to power your nerves and muscles Pedialyte has the electrolytes Foods rich in electrolytes: Oresol (contains sodium chloride) Gatorade Banana (contains potassium) Sodium chloride, magnesium, potassium they balance the body fluid , they maintain your blood proper ph and they carry electrical signals from yuor muscles, and they nano electrolyte (di ko maintindihan) andelectrolyte substance that will conduct electricity when dissolve in water and also in some polar covalescent compounds are electrolytes. Ano yung tinatawag na table salt? Sodium and chloride ELECTROLYTE Calcium Chloride Potassium Magnesium Dietary sources of electrolytes: 1. Banana - rich in Potassium and calcium=for nagtatae 2. Yogurt= calcium and probiotics = for healthy gut 3. Potatoes = potasium 4. Spinach = calcium and magnesium 5. Celery = sodium content 6. Milk = calcium 7. Almond= calcium 8. Coconut water= sodium/ potassium 9. Egg= calcium Sodium What do electrolytes Do? Promotes neuromuscular impulses Maintain body fluid volume and osmolarity Ditribute body water between fluid compartments Regulate acid base balance Note: We cannot leave without electrolytes in our body because it distribute water . we need to replenish it imediately to avoid fainting. FUNCTIONS IN THE BODY Necessary for muscle contraction, nerve function, blood clotting, cell division, healthy bones and teeth Maintains fluid balance in the body Regulates heart contaction, helps maitain fluid balance Necessary for muscle contaction, nerve function, heart rhythm, bone strength, generating energy and building protein Maintains fluid balance and necessary for muscle contaction and nerve function NORMAL ADULT RANGE 4.5-5.5 mEqL 97-107 mEqL 3.5-5.3 mEqL 1.5-2.5 mEqL 136-145 mEqL WHat are they? Electrolytes are minerals found in the body fluids that carry an electrical charge and are essential to keeping the heart, nerves and muscles functioning properly. As such, it is important to maintain a precise and constant balance of electrolytes. - CATION- positively charges - ANION- negatively charged Cations = anions for hemostasis to exist in each fluid compartment Commonly measured in mEq/L CATIONS SODIUM (Na+ POTASSIUM (K+) CALCIUM (Ca++) MAGNESIUM (Mg+) ANIONS CHLORIDE BIOCARBONATE PHOSPHORUS SULFATE 2. Electrolytes are charged particles (ions) that are dissolved in body fluid. 3. (Diko ma ss yung pic, masyadong malabo) Major Cations Extracellular - sodium Intracellular -potassium 4. Release is stimulated by: raised sympathetic tone, falling plasma volume, and certain prostagladins, such as PGE2 No direct effects promoting Na+ retention, it controls the renin-angiotensin-aldosterone axis Angiotensin II: Levels rise as a result of renin release In turn, it stimulates the realease of aldosterone Also increase tone in the efferent glomerular arteriole. The next effect is to enhance Na+ reabsorption from proximal tubule Aldosterone: Steroid hormone released from the adrenal cortex End product of the RAAS system Acts on the distal tubule and collecting duet to increase Na+ and water reabsorption (proportionately more Na+ than water) Arginine vasopressin (AVP), anti-diuretic hormone (ADH) Neuron cell bodies in supra-optic and paraventricular nuclei of the hypothalamus Stored in posterior pituitary Passive absorption of water from the collecting ducts along with a small degree of Na+ re-absorption, concentrating the urine RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM (RAAS SYSTEM ) SODIUM (Na+) INTRODUCTON: Most prevalent cation in the ECF Total body sodium is about 5000 mEq In normal individuals, the kidney strives to achieve Na+ balance - that is to have Na+ excretion equal to Na+ ingestion FUNCTION: Maintain balance of extracellular fluid, thereby it controls the movement of the water between fluid compartments Transmission of nerve impulses Neuro muscular and myocardial impulse transmission 1. REGULATION: A. Hormones increasing sodium reabsorption 1. Renin: released from the juxtaglomelular apparatus of the kidney 2. SODIUM (Na+): REGULATION B. Hormones Increasing Sodium Concentration: Atrial Natriuretic Peptide (ANP): A small peptide produced from the atrial wall as a result of atrial stretching Increase Na (and hence water) excretion by increasing GFR and blocking Na reabsorption in PCT Brain Natriuretic Peptide (BNP): Secreted by the hypothalamus, termed Brain Natriuretic Peptide (BNP) Have similar roles SODIUM (Na+): SAMPLE COLLECTION Serum: venous blood sample in gel vacutainer Urine: o 24 hours urine collection o No preservative is required o Store at 2-8 degree centigrade SODIUM (Na+): METHOD ESTIMATION Ions selective electrode o 2. Potentiometric measurements: Potentio-metry is to determine the difference in potential between a working (an indicator) electrode and a counter (a reference) electrode, Cathode is the working / indicator electrode. Anode is the counter / reference electrode. Indicator Electrode: Electrode that responds to analyte and donates / accepts electrons Reference Electrode: Second ½ cell at a constant potential Cell voltage is difference between the indicator and reference electrode Ecell = Ec - Ea ○ Where: Ee is the reduction potential at the cathode ○ Ea is the reduction potential at the anode. SODIUM (Na+): BIOLOGICAL REFERENCE RANGE Serum: 135 - 145 mEq/L Urine: o 24 hr urine sample: 40-220 mEq/day Note: For random, it is better to do FeNa+ Also used in calculation of Anion gap & Osmolality SODIUM (Na+): PANIC VALUE Serum level: >160 and <120 mEq/L SODIUM (Na+): ERRORS AFFECTING Na+ RESULT 1. Pseudohyponatremia (pag masyadong mababa) Sample collection from IV site, thus the sample is diluted by the hypotonic fluid (5% dextrose). - confirmed by dilution effect on other parameters High plasma glucose level: increase 100 mg/dl lowering Na 1.6 mmol/L, after 400 mg/dl, every 100 mg/dl lowering 2.4 mmol/L Corrected Sodium = [0.016 x (serum glucose - 100)] + serum Na Increased viscosity due to the Hyperproteinemia, Hyperlipidemia due subsequent decreased watery portion of plasma can thus cause false low sodium concentrations Pseudohypernatraemia (Increase level of sodium) Sample collection from IV site confirmed by measurements of CL and K+ Drugs - SSRI, sodium valproate etc. HYPONATREMIA NOTE: For burns: ang lumalabas sa may burned part is white cell hindi dugo kaya ang sinasalin is Fresh Frozen Plasma Summary of Natremic Disorders Hyponatremia Hypernatremia Hypovolemic Na - H2O - Na - H2O - Eu-volemic Na - N H2O - Na - N H2O - Hypervolemic Na - H2O - Na - H2O - HYPERNATREMIA 04.06 PART 1: 28-30:45 PART 2: 0-2 POTASSIUM K Madami sa banana, apple, peanuts, legiums, orngaes and lemons in the picture, indicated are the atomic number, symbol, name, weight it also rich in beet greens, salmon, tomatoes, white button mushrooms, etc. major intracellular cation untreated changes in K+ levels can lead to serious neuromuscular and cardiac problems Normal K+ levels: 3.5-5 mEq/L Total body K+ content in a normal adult: 30004000mE1 98% intracellular, 2% in ECF Health Benefits of Potassium Contains potassium Regulates sugar Muscle contraction Low pressure Alkaline content Treats cramps Retains fluid Builds muscle Removes tiredness Balancing Potassium Most K+ ingested is excreted by the kidneys Three other influential factors in K+ balance: o Na+/K+ pump o Renal regulator o pH level HYPOKALEMIA (POTASSIUM DEFICIT) Serum K+ <3.5 mEq/L Caused by: SUDDEN o patients in Diabetic coma GRADUAL o Diarrhoea – Villous + UC o PS + GOO o Duodenal fistula o Ileostomy/USD o Poisoning o Beta agonists Alkalosis Shallow Respirations Irritability Confusion drowsiness Weakness. Fatigue Arrythmias – irregular rate, tachycardia Lethargy Thready pulse ↓ Intestinal Motility Nausea Vomiting Ileus What do you see? Irritability Paresthesia Muscle weakness (especially legs) ECG changes (tented/peak T wave) Irregular pulse Hypotension Nausea, abdominal cramps, diarrohea CALCIUM Errors affecting K+ result B. Pesudohypokalemia 1. Sample collection form IV site, thus the sample is diluted by the hypotonic (5% dextrose). – confirmed by dilutional effect on other parameters 2. High plasma glucose level 3. Increased viscosity ORDER OF COLLECTION BY CLSI 1. 2. 3. 4. 5. 6. 7. 8. Sterile blood culture Coagulation (light blue)/Citrate Non-additive (red top/Plain Gel separator tube (red or gold)/Plain Heparin tube (green top) EDTA (lavender/purple top) Fluoride tube (grey top) All other tubes HYPERKALEMIA Muscle twitches → Cramps → Paresthesia Irritability and anxiety ↓ BP EKG changes Dysrhythmias – irregular rhythm Abdominal cramping Diarrhea 99% percent in bones, 1% in serum and soft tissue (measured by serum Ca++) Works with phosphorous to form bones and teeth Role in cell membrane permeability Affects cardiac muscle contraction Participates in blood clotting Normal value 8.5-10.5 mg/dL Most abundant mineral in human beings Total calcium in an average adult is about 1,000 gm 99% in bones and teeth, hair, nails Rest in various tissues in body fluids Present in bones mainly in the foprm of calcium phosphate About 50% is bound to protein (protein-bound or non-diffusible calcium) About 5% with organic anions e.g. citrate (diffusible) The remaining 45%: free ionized calcium (freely diffusible) Ionized calcium: active form Functions Formation od bones and teeth Excitability and conductivity of nerves Neuromuscular transmission Excitability and conductivity of myocardium Coagulation of blood Action of hormones Sample Collection Serum: venous blood sample in gel vacutainer Urine: o 24 hours urine in collection o No preservative is required o Store at 2-8 degrees Method of Estimation 1. T. Calcium- Arsenzo III Spectrophotometric method Ca++ =Arsenzo III Ca-Arsenzo III complex (purple) 2. Ionized Calcium: ISE Biological Reference Range T. SerumL 8.5-10.5 mg/dL Ionized calcium: 0.9-1.3 mmol/L Urine: 24h urine sample: 100-250 mg/day 4/6/22 (2-7 2ND VID) CALCIUM ERRORS AFFECTING Ca++ level A. Pseudohypercalcemia: 1. Cleaning the venipuncture site 2. Tourniquet application 3. Clenching fist 4. Needle or syringe 5. Order of drawing tubes 6. Centrifugation and vigorous shaking of sample 7. Storage 8. Sample type 9. Lymphocytosis and thrombocytosis B. Pseudohypocalcemia 1. Sample collection from IV site 2. High plasma glucose level 3. Increased viscosity HYPERCALCEMIA Hyperparathyroidism Hypervitaminosis D Bone cancer Multiple myeloma Leukemia Polycythemia Milk-alkali syndrome Sarcoidosis Idiopathic infantile hypercalcemia HYPOCALCEMIA Hypoparathyroidism Rickets Osteomalacia Chronic renal failure Nephrotic syndrome HYPOCALCEMIA Serum calcium <8.9 mg/dL Caused by inadequate intake, malabsorption, pancreatitis, thyroid or parathyroid surgery, loop diuretics, low magnesium levels Clinical manifestations of hypercalcemia: Immobilization Bone demineralization CHLORIDE Calcium accumulates in the ECF and passes through the kidneys Calcium stones Calcium precipitation Cardiac dysrhythmias Mental status changes: lethargy, confusion, memory loss Decreased GI motility Nausea Constipation vomiting The total amount of chlorine in an average adult is about 80 gm Chlorine, in the form of chloride ions, is the chief anion of extracellular compartment Normal serum chloride level is 98-107 mEq/L (355375 mg/dl) The chloride content of cerebrospinal fluid is 120 to 130 mEq/L The interstitial fluid contains only about 4 mEq/L FUNCTIONS: 1. Maintenance of osmotic pressure 2. Maintenance of pH 3. Formation of hydrochloric acid Sample collection: Serum: venous blood sample in gel vacutainer Urine : 24 hours urine collection No preservative is required Store at 2-8 degree Method of estimation: By ion selective electrode Abnormal serum chloride levels: - - Changes in serum chloride level are parallel to those in serum sodium level Serum chloride level is raised (hyperchloraemia) in dehydration, respiratory alkalosis, metabolic acidosis and adrenocortical hyperactivity. Serum chloride level is decreased (hypochloraemia) in severe vomiting, prolonged gastric suction, respiratory acidosis, metabolic alkalois and Addison’s disease. MAGNESIUM - Tetany=”nag lock jaw?” FOODS RICH in magnesium: peanuts, beans - Convulsions WHAT DO WE DO? Mild Dietary replacement Severe IV or IM magnesium sulfate Monitor Neuro status Cardiac status Safety HYPERMAGNESEMIA MAGNESIUM cofactor for many enzymes- ATP utilization in muscle fiber role in protein synthesis and carbohydrate metabolism helps cardiovascular system function(vasodilation) regulates muscle contractions HYPOMAGNESEMIA Serum Mg++ level < 1.5 mEq/L Caused by poor dietary intake, poor GI absorption, excessive GI/ urinary losses HIGH RISK CLIENTS: Chronic alcoholism Malabsorption GI/urinary system disorders Sepsis Burns Wounds needing debridement CLINICAL MANIFESTATIONS OF HYPOMAGNESEMIA: - Confusion Depression Cramps SERUM Mg++ level>2.5 mEq/L Not common Renal dysfunction is most common cause Renal failure Addison’s disease Adrenocortical insufficiency Untreated DKA What do we do? - Increased fluids if renal function normal Loop diuretic if no response to fluids Calcium gluconate for toxicity Mechanical ventilation for respiratory depression Hemodialysis (Mg++ free dialysate)
 0
0
advertisement



Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users