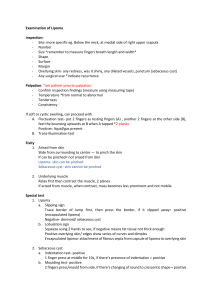
10.5005/jp-journals-10011-1256 Mahendra Raj et al REVIEW ARTICLE Intraoral Lipoma: Review of Literature and Case Report Mahendra Raj, Thanuja Ramadoss, G Anuradha, Shobana Devi ABSTRACT Lipomas are benign mesenchymal neoplasms of soft tissue that can be found in any part of the human body. Conversely, their presence in the oral mucosa is rather uncommon, with approximately 4% of the cases occurring in the oral cavity. The aim of this paper is to present the importance of diagnosis and treatment of intraoral lipoma. Clinicians must be able to recognize rare lesions, like intraoral lipomas, to provide appropriate treatment, thereby ensuring comfort and quality of life for the patient. Keywords: Benign mesenchymal neoplasm, Retromolar area. How to cite this article: Raj M, Ramadoss T, Anuradha G, Devi S. Intraoral Lipoma: Review of Literature and Case Report. J Indian Aca Oral Med Radiol 2012;24(1):36-38. Source of support: Nil Conflict of interest: None declared similar to that of the adjacent mucosa. On palpation, it was soft, slippery and nontender (Fig. 1). Based on the above findings, a provisional diagnosis of fibroma was given. A differential diagnosis of lipoma was given. The lesion was excised. On histopathological examination, it was reported as lipoma where adult adipocytes were seen interspersed with connective tissue stroma and thinned epithelium (Fig. 2). Correlating the clinical and histological findings, a final diagnosis of intraoral lipoma of the retromolar area was given. DISCUSSION Lipoma was first described by Roux in 1848 in a review of alveolar masses, where he referred it as ‘yellow epulis’. The pathogenesis of lipoma is uncertain but they appear to be more common in obese people. However, the metabolism INTRODUCTION Benign mesenchymal soft tissue neoplasms commonly occur in the oral cavity. Lipoma is one such benign tumor which occurs rarely in the oral mucosa. About 20% of the lipomas occur in the head and neck region. Out of which oral lipomas comprise only 1 to 4% of cases.1 Though the etiology of lipoma is unknown, possible causes which have been postulated are trauma, infection, chronic irritation, hormone alteration,2 metaphase of muscle cells, lipoblastic embryonic cell nest in origin.3 Lipoma appears to be more common in obese individuals.2 Lipomas present clinically as slowly enlarging, smooth-surfaced soft yellowish growth. Differentiating it from other mesenchymal tumors is mandatory as it plays a major role in treatment plan and diagnosis. This article presents a case of a intraoral lipoma in a rare location. Fig. 1: 1 × 1 cm well circumscribed, smooth, slippery, nontender mass CASE REPORT A 55-year-old male patient reported to the department with mobile teeth. On examination of the patient, a growth was noted in the right retromolar area. History revealed that the growth started 10 years back. It was initially small and has grown to the present size. Patient did not give any history of pain. Occassionally, the patient complained of discomfort while eating. Examination of the lesion revealed a 1 × 1 cm well circumscribed, pedunculated, smooth surfaced growth in the right retromolar area which was in proximity to the posterior third of the tongue. The color of the growth was 36 Fig. 2: Adult adipocytes seen with connective tissue stroma in 5× JAYPEE JIAOMR Intraoral Lipoma: Review of Literature and Case Report of lipoma is completely independent of normal body fat.4 In few cases of lipoma, rearrangement of 12q, 13q, 6p chromosomes have been observed.2 The accepted classification of benign lipomas includes the categorics: Classic lipoma; lipoma variants, e.g. angiolipoma, chondroid lipoma, myolipoma, spindle cell lipoma, hamartomatous lesions; diffuse lipomatous proliferation and hibernoma.5 Lipomas can occur in various anatomic sites, including major salivary glands and various parts of the mouth. The most common site of oral lipomas is the buccal mucosa, a region rich in fatty tissue, followed by the tongue, lips, floor of the mouth, palate and gingival. This pattern corresponds to the quantity of fat deposits in the oral cavity.3 Most patients with lipoma are above 40 years of age or older, lipomas are uncommon in children.6 Clinically, oral lipomas generally present as mobile, painless, submucosal nodules, with a yellowish color.7 They may be pedunculated or sessile. The consistency of the lesion varies from soft to firm, depending on the quality and distribution of fibrous tissue and depth of the tumor.2 The occurrence of multiple lipomas is associated with Cowden’s syndrome or multiple hamartoma syndromes.7 Generalized lipomatosis has been reported to contribute to unilateral facial enlargement in hemifacial hypertrophy. Lipomas have the principal differential diagnosis of fibromas, which is composed of fibrous tissue and much more firm.8 In view of their similar clinical features, other tumors, such as thyroglossal duct cysts, ectopic thyroid tissue, pleomorphic adenoma, mucoepidermoid carcinoma, and oral dermoid and lymphoepithelial cysts should also be included in the differential diagnosis. 3 Oral lymphoepithelial cyst’s clinical appearance is very similar to oral lipomas but they usually occur in one-third decade of life, and common sites are floor of mouth, soft palate and mucosa of pharyngeal tonsils which is uncommon sites for oral lipomas. Oral dermoid and epidermoid cysts also present as submucosal nodules but commonly occur in midline of floor of the mouth. Since, oral lipoma can also present as a deep nodule with normal surface, color, salivary gland tumor and benign mesenchymal neoplasms should also be included in differential diagnosis.7 Lipomas may show alterations on conventional radiographs. Similar features detected on occlusal radiographs were only reported by Seldin et al. In this respect, computed tomography, ultrasonography and MRI are valuable tools in most cases.3 Lipomas have a less dense and more uniform appearance than the surrounding fibrovascular tissue when transilluminated. MRI scans are very useful in the diagnosis which CT scans and ultrasonography are less reliable. The histopathology remains the gold standard in the diagnosis of lipoma. Histologically, lipomas are classified as simple lipoma or variants, such as fibrolipoma, spindle cell lipoma, intramuscular or infiltrating lipoma, angiolipoma, salivary gland lipoma (sialolipoma), pleomorphic lipoma, myxoid and atypical lipomas.1 The most frequent histological subtype in the oral cavity was simple lipoma, followed by fibrolipoma. However, some authors reported a similar incidence of lipomas and fibrolipomas.3 Most oral lipomas are composed of mature fat cells that differ little in microscopic appearance from the surrounding normal fat as the fat cells in lipoma are larger in size measuring up to 200 mm in diameter. The tumor is well circumscribed and has a fibrous capsule. The treatment of oral lipomas irrespective of histological variant is simple surgical excision. Surgical resection is the treatment of choice for this tumor. However, advantages of suction-assisted lipectomy for medium sized (4 to 10 cm) or large lipomas (>10 cm) have been reported.4 Recurrence is rare.7 Intramuscular lipomas have a higher recurrence rate because of their infiltrative growth pattern, but this variant is rare in oral and maxillofacial region.9 Lesions, outside the oral cavity, may show greater recurrence rates after surgical excision.10 CONCLUSION Clinicians must be able to recognize rare lesions like intraoral lipomas to provide appropriate treatment, thereby ensuring comfort and quality of life for the patients. REFERENCES 1. Alvimar-Lima de Castro, Eni-Vaz-Franco-Lima de Castro, Renata-Callestini, et al. Osteolipoma of the buccal mucosa. Med Oral Patol Oral Cir Bucal 2010 1;15 (2):e347-49. 2. Kaur RP, Kler S, Bhullar A. Intraoral lipoma: Report of three cases. Dent Res J (Isfahan) Winter 2011;8(1):48-51. 3. Eduardo-Costa Studart-Soares, Fábio-Wildson-Gurgel Costa, Fabrício-Bitu Sousa. Oral lipomas in a Brazilian population: A 10-year study and analysis of 450 cases reported in the literature. Med Oral Patol Oral Cir Bucal 2010 Sep 1;15 (5): e691-96. 4. Epivatianos A, Markopoulos AK, Papanayotou P. Benign tumors of adipose tissue of the oral cavity: A clinicopathologic study of 13 cases. J Oral Maxillofac Surg 2000;58:1113-17. 5. Waseem Ahmed, Muhammad Amin, Shafiullah. Intraoral lipoma—an unusual site and size. PAFMJ 2009;2. 6. Sekar B, Dominic Augustine, Murali S. Lipoma, a rare intraoral tumor–a case report with review of literature. Oral and Maxillofacial Pathology Journal (OMPJ) 2011 JulyDec;2(2). 7. Matheus Coêlho Bandéca, Joubert Magalhães de Pádua, Michele Regina Nadalin, et al. Oral soft tissue lipomas: A case series. JCDA 2007 June;73:5. Journal of Indian Academy of Oral Medicine and Radiology, January-March 2012;24(1):36-38 37 Mahendra Raj et al 8. Gilberto Araujo Noro Filho, Bruno Vieira Caputo, Camila Correia dos Santos, et al. Diagnosis and treatment of intraoral lipoma: A case report. J Health Sci Inst 2010;28(2):129-31. 9. Neville Brad W, Dam, Allen, Bouquet. Oral and maxillofacial pathology (3rd ed). Elseiver 2009;524. 10. Rafieiyan, Hamian N, Anbari M, Abdolsamadi F. Lipoma of the tongue: A case report. DJH 2011;2(1). ABOUT THE AUTHORS Thanuja Ramadoss Senior Lecturer, Department of Oral Medicine and Radiology, Madha Dental College and Hospital, Chennai, Tamil Nadu, India G Anuradha Reader, Department of Oral Medicine and Radiology, Madha Dental College and Hospital, Chennai, Tamil Nadu, India Mahendra Raj (Corresponding Author) Shobana Devi Principal, Professor and Head, Department of Oral Medicine, Diagnosis and Radiology, Madha Dental College and Hospital, Chennai, Tamil Nadu, India, e-mail: drmahendraraj@yahoo.com 38 Senior Lecturer, Department of Oral Medicine and Radiology, Madha Dental College and Hospital, Chennai, Tamil Nadu, India JAYPEE