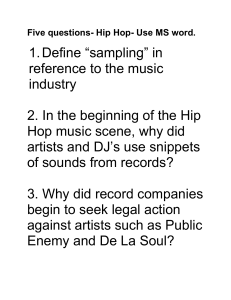
. 367 . Chinese Journal of Traumatology 2011;14(6):367-370 Case reports Irreducible traumatic posterior hip dislocation with entrapment and a buttonhole effect André-Pierre Uzel*, Ricardo Bertino, Guy Daculsi and George Yves Laflamme 【Abstract】The authors reported the case of a 27year-old man who sustained an irreducible postero-lateral traumatic dislocation of the hip with capsular and labral entrapment. Initial X-rays showed only a small acetabular fragment. After two attempts to reduce the hip with muscle paralysis under general anaesthesia failed, the patient was treated by immediate open reduction through a posterolateral approach. Surgical exploration of the hip revealed a small osteochondral fragment attached to a large piece of labrum and capsule, clogging the acetabulum. The femoral head crossed over the torn capsule with a buttonhole effect. These elements were relieved, the bone fragment was fixed with a 2 mm screw and the capsule was repaired. At the 10year follow-up, the functional outcome was excellent with a Harris score of 100 points and no signs of necrosis or osteoarthritis. The authors propose a literature review of this uncommon lesion. Key words: Hip dislocation; Tears; Acetabulum; Necrosis T which the femoral head does not cross the acetabular rim. We report a case of actual irreducibility, where the femoral head crossed over a buttonhole through the capsule and did not cross the edge of the acetabulum, due to a bucket-handle tear in the acetabular labrum. raumatic dislocation of the hip is a surgical emergency. The incidence of aseptic necrosis varies from 4.8%, if the hip is reduced within 6 hours after injury, to as high as 52.9%, if the hip is reduced in more than 6 hours after injury. 1 Most commonly, in more than 85% of cases, the dislocation occurs in a posterior direction.2 Thompson-Epstein’s classification3 distinguishes 5 types of posterior hip dislocation based on size, comminution of the posterior wall fragment or the presence of a femoral head fracture. Irreducible hip dislocation is a rare condition: only 3% of cases in Canale and Manugian’s4 report. We must distinguish the non-concentric reduction, which results from a failure to fully seat the femoral head secondary to interposed soft tissues4-7 and/or an incarcerated osseous fragment7, from an actual irreducible dislocation4,8-10, in DOI: 10.3760/cma.j.issn.1008-1275.2011.06.009 Department of Trauma and Orthopaedic Surgery, C H R U de P o in t e-A -P it re, 9 7 1 59 P o in t e-A -P it re, Guadeloupe, France (Uzel AP and Bertino R). CHU Bordeaux, CIC-IT INSERM, Hospital Xavier Arnozan, 33000 Bordeaux, France (Daculsi G). Division of Orthopaedic Surgery, Hospital du Sacré Coeur, 5400 GouinOuest, Local J-3245, Montreal, Quebec H4J 1C5, Canada (Laflamme GY) *Corresponding author: Tel: 33-0690575564, Fax: 330590891744, Email: andre-pierre.uzel@wanadoo.fr Chin J Traumatol 2011;14(6):367-370 CASE REPORT On December 25, 1999, a 27-year-old male victim of a car accident was admitted to the emergency department with isolated trauma to the right hip. A dermoabrasion of the front of the knee indicated a dashboard injury. X-rays showed a posterior dislocation and a small acetabular rim fracture (Figure 1). The patient was taken to the operating theater for emergency reduction. Under general anaesthesia, a Bigelow manoeuvre (closed reduction) with curare was attempted without success. A second attempt under C-arm fluoroscan control failed to reduce the femoral head into the acetabulum. During the postero-lateral approach, shredding was identified in the perior wall of the acetabulum. We found an osteochondral fragment measuring 2 cmx1 cm attached to the labrum with a 3-cm capsular tear incarcerated in the acetabulum. The cartilage in the femoral head was explored, and abrasions were identified on the femoral head adjacent to the fovea capitis over a surface of 1.5 cm². . 368 . A femoral head extractor was introduced along the femoral neck through the greater trochanter in order to disengage the femoral head, as well as to access the osteochondral fragment and the interposed soft tissues deep in the acetabulum. The labrum was sewed up to the soft tissues, the capsule was repaired using absorbable sutures and the osteochondral fragment was fixed with a 2 mm cortical screw. We did not use suture anchors on these soft tissues because the peripheral elements were still intact. The trochanteric pelvis muscles were repaired. Fluoroscan imaging and postoperative X-rays confirmed the concentric reduction with symmetrical widening of the joint space. The rehabilitative regimen consisted of longitudinal traction with bed rest for one month, followed by weight-bearing as tolerated, ambulation with crutches and an active range of motion protocol. At the 3rd month of follow-up, the patient could walk without pain or limp and his hip mobility had returned to normal. He was able to resume his work as an agricultural worker three months after surgery and CT scan showed a good reduction (Figure 2). Unfortunately, the same patient was involved in another car accident on January 1, 2001 and sustained a second posterior dislocation of the right hip with no associated fractures. Closed reduction under general anaesthesia was successful and physical examination confirmed inherent stability of the hip. The same postoperative regimen was applied with traction for 1 month. He returned to work after one and a half months. At the latest follow-up in December 2010, the patient was asymptomatic and had a Harris score of 100. Only Brooker’s stage 1 heterotopic ossification was seen on the Xrays, with no signs of osteonecrosis or degenerative arthritis (Figure 3). Figure 1. X-rays showing posterior hip dislocation with a small piece of acetabular rim. Chinese Journal of Traumatology 2011;14(6):367-370 Figure 2. CT s c an s howing s uc c es s f ul reduc tion of the osteosynthesis. Figure 3. Anteroposterior view of the pelvis after 2 times of hip dislocations showing the integrity of the joint. DISCUSSION For Slatis and Latvala9, in more than half of their cases, posterior dislocation is complicated by fracture of the hip joint. As a complication of hip dislocation, sciatic nerve palsy is reported in 10%-15% of cases.11 Bilateral traumatic hip dislocation rarely occurs and few cases associated with acetabular fractures have been reported.12 An association with bilateral sciatic nerve palsy is rarer.13 Posterior dislocations of the hip are often the result of motor vehicle accidents in which the passenger’s knee hits the dashboard. Depending on the degree of hip adduction and flexion, the lesion may vary from pure dislocation to acetabular lip or femoral head fractures.4 For Paterson5, the size of the fractured fragment of the posterior wall increases as flexion and . 369 . Chinese Journal of Traumatology 2011;14(6):367-370 adduction lessen. When faced with a dislocation of the hip, to determine how isolated it is by appropriate X-ray assessment is important. The irreducibility of isolated dislocations may be due to an acetabular or femoral head fragment. The irreducibility of femoral head fractures occurring during posterior dislocation has been noted by several authors with the risk of transforming Pipkins’ type 2 into type 3 during reduction. 14,15 In addition, the irreducibility of a pure dislocation can be related to the incarceration of soft tissues of various origin: buttonholed through the capsule, 2 cases for Canale and Manugian4, 1 case for El-Andaloussi et al10; piriformis muscle wrapped around the femoral neck, 1 case for Proctor8, Slatis and Latvala9 and Canale and Manugian4 respectively; obstruction of the acetabulum by obturator internus, gemellus superior and inferior muscles, 1 case for Slatis and Latvala9. Buchholz and Wheeless16 found an anatomical variant of the typical acetabular rim fracture represented by a posterosuperior and superior fragment which may occur when the capsule, ileofemoral ligament and rectus femoris muscle attachments are wrenched. The case presented is reminiscent of the two previous explanations of irreducibility reported by Paterson5, also Buchholz and Wheeless16. When the classic clunk is not heard during the reduction of a dislocated hip, an intervening torn acetabular labrum should be suspected and investigated appropriately. According to Chun et al17, the presence of a radiopaque body in the articular spaces is indicative of the incarceration of a femoral or acetabular bone fragment. Thus, after reducing the dislocation, a CT-scan is needed to detect any osteochondral lesions, such as impaction of the femoral head, which may compromise the long-term functional prognosis of the hip.18 On the other hand, Kim et al7 carried out an arthro-CT or MRI in order to detect the interposition of soft parts and/or capsule and labrum damage. In our case, open surgical reduction offered the best opportunity to visualize the acetabulum by decoaptation of the hip. The hip joint can be distracted with the AO/ ASIF distractor from the iliac crest to the proximal femur or with traction placed by an assistant. On occasion, dislocation of the hip must be performed to allow for removal of the fragments. A forceful pulsatile lavage system may also help flush out the debris. duction should be performed immediately by a posterior approach to the hip, in preference to anterior or anterolateral approaches, if torn tissues and fractures need repair. It is important to carry out fluoroscan imaging to assess the full reintegration of the femoral head during the intervention. Osteosynthesis of the small bone fragments attached to the labrum and capsule should be repaired if possible. The importance of the capsule and labrum in the posterior stability of the hip has effectively been noted by several authors.6,20-22 During the postsurgical period, we mounted the patient with traction for the healing of the soft tissues, although Schlickewei et al23 preclude the need for it. Functional results may in fact be better with early mobilization and weight-bearing. In our case, we preferred traction in order to allow the soft tissues to heal. Our patient presented two episodes of dislocation and we studied the femoral anteversion on CT scan: 10° on the right side and 11° on the left. These results were physiological. Upadhyay et al24 found that reduced femoral anteversion predisposes an individual to traumatic posterior dislocation of the hip. In conclusion, good quality X-rays and careful interpretation of them are important before any closed reduction of a dislocated hip. It is essential that the type of dislocation be determined, and whether or not it is isolated. In cases of irreducible posterior dislocations, the surgical posterior approach must be adopted immediately in order to remove the interposition. Associated injuries to the capsule, labrum and muscles should be repaired. Conflict of interest statement The authors declare that they have no conflict of interest related to the publication of this manuscript. REFERENCES 1. Hougaard K, Thomsen PB. Traumatic posterior dislocation of the hip—prognostic factors influencing the incidence of avascular necrosis of the femoral head. Arch Orthop Trauma Surg 1986;106(1):32-35. We agree with Epstein19 that multiple attempts at closed reduction are contraindicated. The surgical re- 2. Phillips AM, Konchwalla A. The pathologic features and mechanism of traumatic dislocation of the hip. Clin Orthop Relat . 370 . Res 2000;(377):7-10. 3. Thompson VP, Epstein HC. Traumatic dislocation of the Chinese Journal of Traumatology 2011;14(6):367-370 four cases. Rev Chir Orthop Reparatrice Appar Mot 2005;91(2): 173-179. hip: a survey of two hundred and four cases covering a period of 16. Bucholz RW, Wheeless G. Irreducible posterior fracture- twenty-one years. J Bone Joint Surg Am 1951;33-A(3):746-778. dislocations of the hip. The role of the iliofemoral ligament and the 4. Canale ST, Manugian AH. Irreducible traumatic disloca- rectus femoris muscle. Clin Orthop Relat Res 1982;(167):118- tions of the hip. J Bone Joint Surg Am 1979;61(1):7-14. 122. 5. Paterson I. The torn acetabular labrum; a block to reduction 17. Chun KA, Morcuende J, El-Khoury GY. Entrapment of of a dislocated hip. J Bone Joint Surg Br 1957;39-B(2):306-309. the acetabular labrum following reduction of traumatic hip dislo- 6. Dameron TB Jr. Bucket-handle tear of acetabular labrum accompanying posterior dislocation of the hip. J Bone Joint Surg Am 1959;41-A(1):131-134. 7. Kim YT, Ninomiya S, Tashibana Y, et al. Acetabular labrum entrapment following traumatic posterior dislocation of the hip. J Orthop Sci 2003;8(2):232-235. 8. Proctor H. Dislocations of the hip joint (excluding ‘central’ dislocations) and their complications. Injury 1973;5(1):1-12. 9. Slatis P, Latvala A. Irreducible traumatic posterior dislocation of the hip. Injury 1974;5(3):188-193. cation in a child. Skeletal Radiol 2004;33(12):728-731. 18. Mascard E, Vinh TS, Ganz R. Indentation fractures of the femoral head complicating the traumatic dislocation of the hip. Treatment by intertrochanteric osteotomy. Rev Chir Orthop Reparatrice Appar Mot 1998;84(3):258-263. 19. Epstein HC. Traumatic dislocation of the hip. Clin Orthop Relat Res 1973;(92):116-142. 20. Cinats JG, Moreau MJ, Swersky JF.Traumatic dislocation of the hip caused by capsular interposition in a child. A case report. J Bone Joint Surg Am 1988;70(1):130-133. 10. El-Andaloussi Y, Ait Essi F, Arssi M, et al. Irreducible 21. Lieberman JR, Altchek DW, Salvati EA. Recurrent dislo- traumatic dislocation of the hip caused by labral and capsular cation of a hip with a labral lesion: treatment with a modified entrapment with a buttonhole effect. Rev Chir Orthop Reparatrice Bankart-type repair. Case report. J Bone Joint Surg Am 1993;75 Appar Mot 2006;92(3):279-282. (10):1524-1527. 11. Cornwall R, Radomisli TE. Nerve injury in traumatic dislocationof the hip. Clin Orthop Relat Res 2000;(377):84-91. 12. Sahin O, Ozturk C, Dereboy F, et al. Asymmetrical bilateral traumatic hip dislocation in an adult with bilateral acetabular fracture. Arch Orthop Trauma Surg 2007;127(8):643-646. 13. Singh AP, Sidhu AS, Singh AP. Traumatic bilateral hip dislocation with bilateral sciatic nerve palsy. Chin J Traumatol 2010;13(2):126-128. 14. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39-A(5):1027-1042. 22. Boisgard S, Aufauvre B, Jaud E, et al. Recurrent posttraumatic hip posterior dislocation: a case report and literature review. Rev Chir Orthop 1996;(82):462-465. 23. Schlickewei W, Elsasser B, Mullaji AB, et al. Hip dislocation without fracture: traction or mobilization after reduction? Injury 1993;24(1):27-31. 24. Upadhyay SS, Moulton A, Burwell RG. Biological factors predisposing to traumatic posterior dislocation of the hip. A selection process in the mechanism of injury. J Bone Joint Surg Br 1985;67(2):232-236. 15. Sy MH, Kinkpé CV, Dakouré PW, et al. Femoral neck fracture complicating orthopedic reposition of a dislocated hip: (Received May 23, 2011) Edited by LIU Gui-e