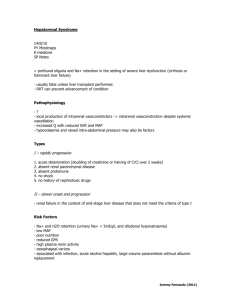
pathophysiology - HDP401 NOTES
advertisement

Week 1 Neoplasia CANCER: CELLULAR REPRODUCTIONS - Under a normal conditions, cellular reproduction ( i.e cell division or proliferation )is tightly regulated process - Cells respond to certain stimuli and growth factors by altering their rate of reproduction - Embryogenesis: is a time of rapid proliferation of non specialized ( undifferentiated) cells called stem cells. - During development cells become specialized in function and structure; some are more differentiated than others - The cell cycle refers to the stages of cell goes through during its lifetime, including cell division - The more specialized a cell, the less frequently that cell goes through the cell cycle to divide. Less differentiated cell cycle more frequently. - Cancer is a condition of unregulated ( uncontrolled) cell production THE CELL CYCLE ● The stages of a cells life with respect to its reproduction is called the cell cycle ● The cell cycle has four distinct phases: 1. Mitosis ( M phase) is the phase of cell division; continually dividing cells cycle from one mitosis to the next 2. G is the post mitiotic growth phase where RNA and protein synthesis and cell growth occurs 3. S phase where DNA synthesis occurs in preparation for cell division 4. G2 is the pre-mitotic phase, also characterized by RNA and protein synthesis - Most cells in our body halt their cell cycle in G1 during some point in their lifespan and enter a phase that is often called G0. this allows cells to differentiate for specialized functions, these cells enter the cell cycle in response to growth stimuli - Highly differentiated cells exit the cell cycle and therefore do not divide Cellular adaption and transformation - Cells can adapt to their environment and stimuli in a number of ways: 1. Atrophy: decrease in cell size 2. Hypertrophy: increase in cell size 3. Hyperplasia: increase in cell number 4. Dysplasia; cells display increased mitosis, are varying sizes and shapes, and have large nuclei, they are considered pre-cancerous 5. Neoplasia: cells are divided out of control and have abnormal cell structure. They are said to have been transformed into cancerous cells. Cancer definitions - Cancer is the 2nd leading cause of death in canada and the US. and includes almost all malignant neoplasms - Neoplasm or tumor: an abnormal mass of cells which grow without response to normal regulatory controls tend to grow after the stimulus for growth has ceases - Malignant ( cancerous) tumors are usually consists of less differentiated abnormal cells which proliferate at a high rate; cells from an irregularly shapes mass cells invade( spread) surrounding tissue and break away to form new tumors at distant sites ( i.e metastasize) - Benign tumors usually consist of more differentiated, relatively normal cells wich proliferate at a higher than normal rate cause damage to adjacent tissue by compression; do not spread are usually not life threatening Malignant neoplasms simply the division of abnormal cells without control and it can invade the nearby tissues. In addition this cells can spread other parts of the body through blood and the lumph system. Malignant cells - are believed to develop from mutations that occurs during differentiation Are undiffrentaied (can’t recognize what makes it different) and are much different from the normal tissue cells surrounding them, especially W.R.T function, nuclear size and shape - Lack contact inhibition, adhesiveness and cohesiveness- invasion and metastasis - Local and systemic effects of tumor locally , malignant tumors cause death to surrouding tissues in several ways - Tend to compress blood vessels and outgrow their blood supply - Iscehmia and tissue necrosis - Rob normal surrounding cells of nutrients ( nutrient trapping) - Replace normal tissue - Loss of function - Liberate toxins and enzymes that destroty both normal and tumor tissue - Causes obstruction of passageway - Cause pain e.g by putting pressure on sensory nerves Systemic effects - Anemia - Weakness and fatigue - Weight loss ( cachexia) - Bleeding - Infections SPREAD OF MALIGNNAT TUMORS Malignant tumors spread by producing secondary tumors that are identical to the original primary tumor -Tumors spread by three ways: 1. Invasion of neighbouring tissues 2. Metastasis- the spread of cancerous cells through blood and lymph system to other organs or tissues of the body 3. Seeding - the spread of to a culture vessel for cell culture activities Invasion - occurs when tumor cells grow into adjacent tissue. Tumor cells lack adhesive properties and can secrete enzyme that allow them to break down confining conecctive tissue Metastasis - Metastasis occurs when tumor cells break free of a tissue and are circulated to distant tissues in the blood and/ or lymph - Secondary tumors can be contained by local lymph nodes or lodge in capillary beds they come across - The lungs are a common site of metastasis because pulmonary capillaries are often the first beds encountered by systemic tumor cells the liver is also a common site for 2 dgree tumors Seeding - Seeding involves the spreading of tumor cells along membranes or within fluids other than blood or lymph - Malignant cells break away and travel with the movement of fluid e.g> ovarian cancer can spreadthroughout the peritoneal cavity Development of cancer ( carcinogenesis) - Carcinogenesis: the process by which normal cell become transformed into malignant cells; initially involves changes in the DNA ( mutation) most cancers require multiple changes in DNA caused by several factors Stages of carcinogensis 1. induction/initation: exposure to carcinogenic agents tha causes the initial irreversible genetic modification agents may be chemical, physical or biologic 2. Promotion: previously initiated cells are induced into unregulated proliferation by various promoter chemicals, grwth factors and hormones—tumor development; this stage is reversible if promoter is removed; may occur after long latency period after initiation chracterized by dysplasia 3. Progression: tumro cells ( unregulated growth) acquire malignant changes that promote invasiveness, metastatic properties and autonomous growth; chrctarized by anaplasia - Initiators: radiation, components of cigartte smoke, hydrocarbons, certain dyes, nitrosamines, aflatoxin, asbestos, certain veruses - Promoters: hormones, nitrate, cigarette smoke, alcohol Genteic chnages in carcinogenesis-proto-oncogenes - There are two main classes of genes responsible for controlling cell growth and replication: proto-oncogenes and tumor suppressor genes Proto-oncogenes promotes controlled growth; when genetically altered, proto-oncogenes become oncogenes which confer unregulated proliferative and invasive properties on the cells - Protein encoded by proto-oncogenes include surface membrane proteins, cytoplasmic proteins-conveying signals and proteins that bind to DNA and regulate gene transcription Examples of oncogenes oncogene Functions of oncogne protein Tumor type HER2 Cell surface recptros Breast, cancer, ovarian ras G protein ( signaling) Lung, colonic, pancertaic Myc Transcription factor Multiple tumor types fes Tyrosine kinase ( singaling) Leukemia- blood cell cancer Tumor suppressor genes - Tumor supressor genes normally inhibit growth; when genetically altered, control function are lost leading to unregulated proliferation Protein encoded by tumor suppressor genes include cell cycle regulators, surface receptors. Cell adhesion proteins transcirpting factor DNA repair proteins Research evidence suggests that mainly human neoplasms result from a combination of oncogene acriavtion and tumor suppressor gene inactivation Examples of tumor suppressor genes T.S. game Functions of T.S. gene protein Tumor types P53 Cell cycle regaualtor Several Retinoblastoma ( RB) Cell cycle regulator Retinoblastoma, small cell lung cancer , sarcoma , breast and ovarian brca1 DNA repair Breast, ovrain Ras an example of an oncogene - - proliferation of many cell types is regulated by growth factors or mitogens secreted locally into the tissue. Examples include: insulin like growth factor, vascular endothelial growth factor, fibroblast growth factors, and transforming growth factor. These growth factors exerts their effects by binding to membrane receptors and activation and intracellular signaling cascade that ultimately increases the production of proteins responsible for cell type progression - Ras is involved in growth factor signaling by activation the mitogen activated signaling cascade which increases proliferation When the gene that codes for Ras is mutated, the Ras protein can continuously activate cellular proliferation, even in the absence of growth factors. This mutation is a common finding in lung, colon and pancreatic cancers P53; AN example of a tumor suppressor gene - P52 is protein that has the baility to stop cell cycle in the G1 phase P53 is activated when DNA smages occurs. By stopping the progression into the 5 phase, p53 prevents damaged DNA from being replicated and passes on to daughter cells In the DNA cannot be repaired, p53 activities teh cellular apoptosis program and the cell is destroyed Motion in the p53 gene prevents this safety switch from being turned on, and allows DNA mutations to be passed on to the daughter cells. P53 mutations are found in virtually neoplasma Another tumor suppressor gene is the breast cancer gene ( IE. BRCA-1). This protein is believed to be involved in DNA repair. Mutation in this gene are found in rare breast and ovarian cancers. Factors in cancer development ( carcinogene) Genetic - In 50 types of cancer altered oncogenes or tumor suppressor gene are inherited e.g; breast cancer ( BRCA1 and BRCA2) retinoblastoma Biologic - Chronic irritation and inflammation: associated with increase mitosis and cell transformation e.g; colon cancer- ulcerative colitis, adenocarcinomas of the esophagus - barrets esophagus - Age: many cancers are more common in edlerly perhaps due to increase number of rectaive oxygen species ( free radicals) , deteririoting cellular reaction and poor nutrition - Hormones; inadequate progesterone and estrogne - endometrial cancer; expression of estrogen receptros in breast tumors ; testostrone may continue to prostate cancer Bilogic - Viruses; some have transforming properties where they alter host cell DNA e.g: hepatitis B virus ( HBV) and HCV– HEPATOCELLUAR CARCINOMA; herpes simplex virus 2 ( HSV-2) and human papillomavrius ( HPV) cervical cancer ( eraly decataion with PAP smear) Lifestle - Smoking : cigarette smoke contains both inducer and promoter – cancer of the lung, larynx, esophgus, pancreas, kidney, cevix and baldder - Chewing tobacco: cancer of roal cavity and esophagus - alchohol ; believed to enhance transport of carcinogens; exacerbates carcinogenic effects of cigarette smoke- cancer of oral cavity and esophagus - Diet: smoked, charbroilled, slated or otherwise preserved foods, foods fried in refused fat are assocaited with gastric cancer; high fat, protien and beef or low fiber diets– colon cancer environmental/chemical - Many chemicals in the industrial workplace and in pollution have been identified as carcongoen; asbestos, nickel- lung cancer, benzene- lukemia, anline dyes-baldder cancer- herbicides- non hodgjins lymphoma - Alos includes the chemical in food from preparation 9 see biological factors ) and cigarette smoke Radiation - High energy radiation rays radioactive chemicals cause chromosomal ( DNA) damage; ultraviolet ( sun) rays- skin cancer; ionizing radaion - leukimia Naming tumors Tumros are named by a root–cell type of origin, and suffix -beningn tumor or malignant tumor of specific tissue type Roots Suffixes Examples Fatty tissue- lip beningn - oma Lipoma: benign tumor of fatty tissue Gland tissue- adeno Malignant epithelial tissue Carcinoma Adenoma: benign tumor of glandular cells Fibrous tissue- fibro Malignant connective tissue - Sarcoma Adenocarcinoma: malignant tumor of epithelial lining of a gland bone-osteo Nervous tissue Osteoma: benign mass of lamellar bone Osteosacroma: malignant tumor of osteoblasts Note - Oma- suffix is sometimes used for specific malignant tumors e.g: lymphomas and melanoma Staging of tumros - Staging is classification system that is useful in determining the prognosis of a cancer and the most apropriate therpay - Cancers are placed in one of four stages ( 1,2,3,4,5) where stages i tumors are small and well localized and stage IV tumros are larger and have metastasized to other sites Cancers are assessed according to the TNM system - T : indicates the nature and the size of the primary tumor - N: indicates the involvements of regional lymph nodes - M: indicates the spread of metastasis of the tumor The TNM score determines the stage of the cancer. The specific of this nomeclature are different for every cancer Cancer dignosis and managements - Serum analysis is used to detect tumor markers which are antigens expressed on the surface of tumor cells or substance released fron normal cells in response to a tumor - Serum analysis is ised for screening diagnosis estblishing prognosis, monitoring treatment, detrecting recoccurnace Include - Hromoones and enzyme which are over expressed by the tumor e.g: the prostate specific antigen ( PSA) which is released into the blood by prostate tumors - Protien that are normally expressed during fetal development - Genetic testing: the polymerase chain reaction ( PCR) is used to amplify DNA abnromlaities specific to tumor cells which allows detection among small numbers of cancer cells - Used for lukemia, lumphomas, meonomas, neurobalstoma and several carcinoma - New research is related to the use of egne therapy where genes are introduced into the pateins cells in attempts to correct the cells metbolsim , or destroy cancer cells Cancer tretaments - Treatments of cancer involves surgery, chemotherapy or radition, pften a combination of these is required If cancer is known to be hromones sensetive hromones manipulation or hormone antagonist drug may be of benefits Biological therpay with interleukins and interferon can sometimes be used to increase the activity of the immune systems to help destroy transformed cells Nutritional supplementation is often useful to prevent malnuatition and show cachexia Week 2 neoplasia Lung cancer ● ● Lung cancer is the number one cause of death d/t cancer It has historically been more common in males and in most cases (> 80 %) have been linked to smoking ● Highest risk is for those who begin smoking earlier in their lives, smoke heavily ● Second hand smoke has also been implicated in the risk of lung cancer. Risk factors of lung cancer - asbestos, polyvinyl chloride (PVC’s ) a nd some radioactive materials in mining and warfare can cause local increases in lung cancer incidence. Industrial chemicalexposure in combination with smoking greatly increases risk Symptoms of lung cancer - Symptoms of lung cancer may be d/t local effects of the tumour or they may be d/t metastasis or paraneoplastic effects. - Local effects may include irritation and obstruction of airways: dyspnea, SOB, persistent and productive cough and wheeziness of the chest • There may also be hemoptysis ; chest pain ; voice hoarseness - Tumour compression of the superior vena caca may causes swelling of the neck veins and facial edema. Tumours near the visceral pleura may cause pleural effusion, pneumothorax or hemothorax Systemic effects: -general fatigue, malaise, anorexia and weight loss - Prostate cancer Benign prostatic hyperplasia Breast cancer Paraneoplastic effects result from tumour production of hormone-like secretions such as compounds similar or identical to ACTH, ADH, PTH PROSTATE CANCER - This is a common form of cancer , the 2nd most common cancer in males, especially for those > 50 years old. It is seldom seen in young males though in those cases where it does occur at a young age the prognosis is often much worse ie. >60 % mortality within 3 years. Predisposing factors include - older age, incidence increases significantly after 5o race/ethnicity , for example it is more common in the Afro-american population - environmental contaminants , eg. exposure to the heavy metal cadmium - exposure to oncogenic viruses Treatments - Surgery, chemotherpay and radiation - Estrogen therapy BENIGN PROSTATIC HYPERPLASIA - This increase in size and change in structure of the prostate is very common in males over 50 years of age. The enlargement or growth is usually on the medial and lateral regions of the gland, thus causing a narrowing or restriction of the urethra and a subsequent restriction of urine flow. Manifestations( signs) include: - hesitancy - frequency - reduced force of the urine stream BREAST CANCER This is the most common form of cancer found in females Risk factors include: Gender -much higher risk in females Age - increased risk with increasing age - esp after age 50 Family history of breast cancer Reproductive history eg . higher risk if nulliparous., delayed reproduction (eg. first • pregnancy after age 30) , early menarche or delayed menopause. Early Sign and symptoms of breast cancer include - - presence of a palpable mass on self examination or medical examination. These masses tend to be firm but poorly defined, non-mobile (fixed) usually painless and singular. They are most common in the upper outer quadrant. nipple discharge - nipple retraction or puck Additional note on Breast Cancer - Two genes for breast cancer are known. Named BRCA1 and BRCA2 . They account for about 5% of cases of breast cancer. Screening is available for these genes. Fibrostic breast conditons - Range of breast tissue changes that involve tissue masses that tend to respond to hormonal changes throughout the menstrual cycle Usually being more prominent and causing greater symptoms in the post- ovulatory or luteal phase of the cycle This condition is very common especially in women in their 30's or 40's and is the most common cause of surgical procedures of the breast. These breast lumps are not precancerous and as such pose no risk for breast cancer though they do need to be distinguished from cancerous masses • - Usually well defined mobile round granular masses - Usually detected on breast self examination or in routine mammography and often further analysed using ultrasound and biopsy Colorectal cancer - This cancer is has one of the higher mortality rates for cancers in those > 50 years old largely as a result of too late detection Predisposing Factors: - Diet: a diet high in animal fats and refined carbohydrates, low in fibre - This increases transit time and probably the increases exposure time to carcinogens - Pre-existing conditions: such as familial multiple polyposis and ulcerative colitis - Genetic (familial) factor Signs and Symptoms: Early S/S4 tend to be vague and may include changes in the bowel pattern such as periods of diarrhea and constipation alternating. Early proctoscopic examination may reveal a small mass Later there may be more distinct changes in fecal output including:' diarrhea if the tumour is in the ascending colon or above constipation if the tumour is in the descending colon or below flattened or ribbon-like stools if it is in the sigmoid or rectum occult (hidden) blood if it is more proximal –eg.the ascending colon - frank (obvious red) blood if it is in the distal colon ( eg. rectum) Late SIGN AND SYMPTOMS can include: - the s/s of obstruction local pain - s/s of perforation and the resulting peritonitis presence of a palpable mass that puts pressure on spinal nerves leading to s/s of nerve compression such as sciatic and back pain, paresis and bladder dysfunction - typical late cancer s/s such as cachexi Week 3 notes : eye and ear disorders Anatomy of the eyes Anatomy of the ear Glaucoma - Disease in which there is a rise in intraocular pressure ( the pressure inside the eye) or IOP - Pressure rises it is translated throughout the eye and it leads to compression of the blood vessels that supply the retina - Leads to retinal ischemia/ infarction and the result will be vision loss - Glaucoma occurs as a result of obstructed outflow/reabsorption - There are two forms of Glaucoma: Glaucoma ➢ Chronic or open glaucoma ➢ Incidence begins to increase significantly after age 50 ➢ Gradually but progressive, symptoms are often not detected (asymptomatic) or they may just involve very mild blurring of the vision and some haloing around lights and so it is a major cause of vision loss ➢ As the IOP slowly rises there is loss of peripheral vision because initially the pressure compresses mainly the smaller arteries and arterioles of the choroid that supply the outer/peripheral retina ➢ Routine testing of peripheral visual field. ➢ Routine measurement of IOP ➢ Treatment is usually by using pharmaceuticals —however, the partially vision loss cannot be restored Glaucoma ➢ Acute or closed angle glaucoma ➢ Most commonly a result of a congenital abnormally narrow angle ➢ The iridocorneal angle is much narrower than normal so that in the event of a wide pupil dilation the radial iris muscles contract and bulge in the middle and may contact the cornea, adhering to it and effectively blocking the angle so that there is little or no aqueous outflow ➢ IOP will rise rapidly leading to severe and immediate Sign and symptoms of acute or closed glaucoma - such as photophobia, extreme corneal pain , redness of the eye, severe headache and nausea , halos around lights , bulging cornea and of course a dilated unresponsive pupil. This is a medical emergency and can rapidly lead to permanent and significant vision loss (within 24-72 hours). The treatment may involve pharmaceuticals Cataracts • Involves an opacity or loss of transparency of the lens Possible causes of cataracts include: • Senile cataracts associated with aging • Traumatic cataracts can result from trauma • Chemical cataracts as a result of exposure to a wide variety of industrial chemicals • Metabolic cataracts which are most commonly a result of diabetes • Congenital cataracts which may result from in utero exposure to infections such as rubella or toxoplasma or to chemicals or episodes of hypoxia Treatments of cataracts - usually involves removal of the lens and replacement with an artificial intraocular lens Detached retina • Associated with aging d/t gradual shrinkage of the vitreous or with an episode of sudden deceleration that created torsional movements in eye and leads to a tear in the retina Signs and symptoms of detached retina - can include a perception of a dark curtain moving across the visual field; flashing lights and a high incidence of “floaters” in the visual field Usually no pain associated with this but it must be corrected immediately to minimize the degree of permanent vision loss Hearing loss • Hearing loss can result from damage anywhere along the pathway but some losses are very common and a result of typical human activity. • Exposure to very intense sound waves – either single events of extreme intensity or prolonged exposure to high intensity • Workplace noise exposure • Inflammation associated with middle ear infections can also lead to hearing loss by forming a scar Nervous system - The CNS is is protected by structures including the skull, spinal vertebrae, meninges, and cerebrospinal fluid CSF - Flow: Lateral ventricle → third ventricle → fourth ventricle → central canal of spinal cord → subarachnoid space - Production; SF is produced mainly by a structure called the choroid plexus in the lateral, third and fourth ventricles Cranial nerve and functions Spinal plexuses and integrative pathways I Anatomy and physiology of neurons ANS ( autonomic nervous system) Function - is a component of the peripheral nervous system that regulates involuntary physiologic processes including heart rate, blood pressure, respiration, digestion, and sexual arousal. Divison - Sympathetic -arouses the body and loses energy ( actiavtes the fight and flight mode) - Parasympathetic- state of calm and it retsores energy - Enteric - Veins that are swollen, red, hard, or tender to the touch - Veins that are llen, red, hard, or tender to the touch - Veins that are swollen, red, hard, or tender to the touc week 4 notes : neurological disorders - ascow coma scale - the glasgow coma scale ( GCS) is a neurological scale wich aims to give a reliable and objective way of recording the conscious state of a person for initial as well as subsequent assessment 1 2 3 4 5 6 Eye Does not open eyes Opens eyes in response of painful stimuli Opens eyes in response to voice Opens eyes spontaneo usly N/A N/A Verbal Makes not sounds Incompreh ensible sounds Utters inappropria te words confused , disoriented Oriented, converses normally n/a Motor Makes no movement Extension to painful stimuli ( decerebrat e response) Abnormal flexion to painful sti,uli ( decorticate response) flexion/wit hdrawal to painful stimuli) Localized painful stimuli Obeys commands Intracranial pressure Elavated ICP S/S ● Decreased in levels of consciousness ● Headache ● Nausea and vomiting ● Vision changes: A. fixed dilated and unresponsive pupils ● B. papiledema ● C. strabismus ● ● CVS changes ● - changes in temperature regulation ● - changes in respiratory control ● - changes in the CSF ● – seizures ● Common lesions/ herniations of the brian - Supratentoral: lesions are those that develop above the tentorium cerebellum - Infratentorial lesions: are those found below the tentorium cerebelli can lead to eraly effects on the brainstem Hydrocephalus - - Hydrocephalus involves an accumualtion of cerebral spinal fluid There are two main forms A. communicating hydrocephalus decrease of outflow of CSF from the subrachnoid villi. This could be d/t i) a congenital deficit or abnromally of the arachnoid villi ii) an obstruction of the arachnoid villi as a result of accumulation of infection debris iii) obstaruction as a result of scarring formed B. non-communiacting or obstructive hydrocephalus- in which there are an obstruction of outflow from the ventricaulr system out into the subarachnoid space could be d/t i) a congenital deficit or abnormality of some aspect of the ventrucaulr system ii) an obstruction of the ventricles or cerebral aquaduct as reuslst of tumor compression iii) traumatic damage to the ventricles or aqueduct iv) infection leading to obstruction Coma and brian detah - Loss of consciousness and coma can result from a wide variety of causes- both intracranial and extracranial Some extracranial causes can include: - Metabolic changes such as hypoglycemia, uremia, diabetic ketoacidosiss, hepatitis and hypothyroidism Respiratory problem leading to hypoxia Drug intoxication including alcohol, opiates and barbituates Carbon monoxide posioning Shock ( eg, acrdiogenic, septic etc) Hyperthermia Some intracranial causes include - Meningitis Epilepsy hemorrhage , aneurysm etc. in the cerebral circulation CVA’s Cellular injury - Clinical death: is the absence of vital signs. There is no measurable respiratory or cardiac activity to sustain body functions and no movement Brain death or neurological death: for this to be declared the following criteria m ust be observed No spontaneous meovements including seizures for a period of at least one hour No brainstem reflexes that can be elicited including - No papillary reflexes ie. fixed dilated and unresponsive No gag reflex No vestibule occurla response to cold water exclusion criteria: before brain death can be declared the following ruled out: - hypothermia: ( ie. body core temp <32.2 c) drug intoxication metabolic and endocrine distrbances as hypoglycmice and metabolic acidosis HEAD TRUMA - Can lead to two levels of brian damage -primary and secondary Primary brian damage is the direct result of the trauma and might include compression or laceration damage to brian tissue Secondary brain damage could result from - Inflammation leading to elevated ICP Infection of brian tissue Disruption of blood flow as a result of damage to blood vessels leading to ischemia for bria tissue Disturbance of respiratory function d/t factors such as airway obstruction or altered resp. Control by damage to the medulla and pons Post truamtic syndrome - NOTES The effects may last for days to months to years and can iclude manifestations such as Hedacahe, vertigo, irritability, memory deficit, decreased ability to concentrate, sleep disturbance, emotional lability, a variety of phobias and behavioural changes Primary barin injury ● ● -occurs as a direct reuslt of the initail insult Over so rapidly limitation for prevention Secondary injury ❖ Progressive damage reuslting from the bodys physiologic response to the initial insult ❖ Occurs over time cen be prevent high mortality and morbidity Critical factor in determining the neuroal cell fate fater injury - Degree of adenosine triphosphate (ATP) depletion Mechanism of brain injury - Ischemia and hypoxia Ischemia- decreased blood flow Primary insulty —---------> inability of neurons to egnerate ATP - Secondary response —---> oxygen free radical excitatory a.a inflame cells —---> hydroxyl radicals superoxide peroxide Hypoxia- decreased oxygen at cellular level Ischemia and hypoxia usually occur together Cellaulr energy failure - Neuronal tissue highly sensitive to oxygen deprivation 5-10 mins without oxygen —> irreversible brain damage Great ATP requirement and limited capacity for anaerobic DEPENDENT ON GLUCOSE for ATP production Store very LITTLE GLYCOGEN TWO MECHNISMS CAN CAUSE BRIAN CELL DETAH: Anaerobic metabolism Mitochondrial dysfunction: —--> anaerobic glycolytic pathways —> puruvate converted to lactate—> hydrogen ions—--> cellular acidosis Deterioration of ion gradients; K+ efflux, NA+ Cl-Ca2+ influx Excitatory amino acids ● ● ● ● Excessive glutamate may be released because of imapired membrane integrity Repuatke mechanisms fail to remove excess g;utamte because they are energy dependent processes Excess glutamate stimulates nearby neurons that then take uplarge amounts of injurious calcium ions: calcium overload injury NMDA receptor activation stimulates nitric oxide production in neurons in excess it may increase the production og reactive nitrogen species that function as free radicals to damage cellular components Reperfusion Oxygen reenters cells, unpredictable transfer of electrons to oxygen can produce reactive oxygen products that behaves as free radicals ( hydroxyl radical, superoxide peroxide) Cell membranes may undergo LIPID PEROXIDATION in response to free radical damage with subsequent formation of arachidonic acid Week 5 notes: neurological disorder Cerebral circualtion - The anterior cerebral artery supplies the anterior frontal lobe ( for higher cortex functions personality, reason, judemnet, etc) - The medial and superior aspect of posterior frontal lobe including the motor cortex for control ove the lower body ( pectroal gridle) - The medial and superior aspect of the anterior parietal lobe including the somatosenspory cortex for the lower body The posterior cerebral artery supplies: the occipital lobe including the visual sensory visual association area - The middle cerebral artery supplies: the alteral anterior frontal lobe which is responsible for motor control over the upper body- face, pectroal girdle, thorax - The lateral anterior parietal lobe which is responsible for somatosensory function - For the upper body - Most of the temporal lobe including the auditory sensory areas - The left middle cerebral artery supplies the blood flow for the broca’s ( speech motor ) area for wrenicke’s ( speech comprehension ) area Blood brain barrier - Capplireis here frim tighter junctions with a thicker basement membrane layer and an interaction with astrocytes - Prevent wider swings in ion and hormone and nutrient level that occur in the rest of the bodies ECF from occuring in the brain ISF - Prevent the entry of many toxins into brain tissue - Prevents entry of most pathogens into brain tissue Cerebral vascular occlusive disease - There aere a vriety of vsaculr pathologies that can cause focal ischemia and infraction of brai tissue including - A) local cerebral vessel obstruction such as atheroscelrosiis which then promotes local thrombus formation - B) remote origin emboli. Thromboemobliusm ( or gas or fat emboli) may be formed elsewhere in the bidy esp in the herat and these travel through the vessels until they lodge somewhere in the cerebral circaultion Cerebral aneurysms - c.) cerebral aneurysms - Most common occur at the area around the branching of a major artery where the vessel wall is intrinsically weaker - Occurs in the high pressure interconnections of the circle of willis and as an aneurysm enlarges it occupies space which will increase ICP - Altered flow will increase the risk of a thromembolsim - If they rupture —---> large volume blood loss leading to severe cerebral ischemia and the development if large volume hematomas ( especially leaking into subarachnoid space) Cerebral vascaurl accidents - A CVA or stroke describes the acute neurological deficit these processes produce. CVA’s are a major cause of death and permnante fucntion deficit Risk factors predisposing to CVA’s include 1. Non modifiable factros: older age, lipid abnormalities, elevated librnogen levels, systemic hypertension, diabetes, sickle cells disease, polyethemia, and atrial librillation 2. Modifiable risk factors include: use of alcohol, smoking, amphetamines, cocaine as well as obesity, edentary lifestyle and oral contarceptive use Meningitis - Meninges are inflamed - Escherichia coli - Streptococcus pneumonia - Hemophilus infulenzae - Neisseria meningitis S/S of becatreial meningitis - Fever - Severe headache - Nause and vomiting - Nuccal rigidity ( neck stiffness) and often plan in the back, abdomen and extermeiteis - Kernigs. Signs - resistance to extension at the knee while lying on teh side with the hip flexed - Brudzinski’s sign– flexion at the neck result in flexion at the hip and knee - Direct result of inflammation of the meninges and the pain associated with it. Many movements tug at the meninges anbd elcit pain Encephalitis - Inflammation of the berain. There are several causes, but the most common is a viral infection - Encephalitis often causes only mild flu-like signs and symptoms — such as a fever or headache – or no symptoms atr all. Somtimes the flu like symtpoms are more severe. Encephalitis can alos cause confused thinking, seizures, or problem with movement or with senses such as sight or hearing - In some cases, encephaultis can be life thretahening. Timely diagnosis and treatment are importa because its difficult to predict how enecepahlitis will affect each individual - Most people with viral encephalitis have mild flu-like symptoms such as - Headache - Fever - Aches in muscle or joints - Fatigue or weakness - Sometimes the sign and symptoms are more severe and might include confusion, agitation, or hallucination - Seizures ‘loss of sensation or paralysis in certain area of the face or body - Muscle weakness ‘problem with speech or hearing - Loss of consciousness ( including, coma) In infants and young children, sign and symptoms also includes - Bluging the soft spot ( fontanels ) of an infant’s skull - Nause and vomiting - Body stiffness - Proof feeding or not waking for a feeding - Irritability Week 6 neurological disorder Spinal cord injury - A complete spinal cord injury at a specific site there will be loss of control over functions affected by the nerves and tracts of that location and everywhere below it - Many spinal cord reflex functions below the injury site may remain intact but any voluntary control these reflexes will be lost - Reflexes will be lost if they are at the immediate injury site - The permnanent effects the injury will depend on where the spinal cord damage occurs as indicate the following - C1-c2 ( spinal cord segments) some or no control over the neck and head movement and there will be quardiplegia. No diaphragm control since the phrenic nerve is located at c3-c5 so the individual will require immediate and continuing mechanical ventialtions - C5-c6 full neck and head control and some shoulder control. If at c5 then there may be flexion at the elbow. If at c6 possibly some wrist control and no control over the lower limbs. There is complete diaphragm control so no assistance with ventilation is required - T5: full hand and finger control and the use of intercostals muscle for breathing but there will be no SNS control over vasomotor function - T6: there will be abdominal muscle control but still no control over the lower limbs - T7 good SNS control over vasomotor function - L1-L3: there will be hip control and the ability to do knee extensions - S2-s4 there will be leg to ankle control and voluntary control over bowel and bladder function as well as sexual function. Compliactions of SCL - Spinal shock - Autonomic dysrellexia - Edema and deep vein thrombosis d/t blood pooling as result of decreased SNS vasomotor contro and the immobility - Decubitus ulcers and joints contractures d/t the immobility - Increased risk of further injury d/t a.) spstic motor control involving jerky motions that makes falling and other injuries more likely and b) loss of sensory function causing decreased awareness of harmful stimuli - Hypotension ( postural d/t lack of SNS regaultion of vasomotor response leading to fainting when trying to rise - Paralytic ileus Seizure disorder - General tonic clonic seizures or grand Mal Seizures, these are the common from of seizures and they take classic form usually associated with seizures in which there is the loss of consciousness and tehre are convulsions - Can be preceded by a prodromal elect referred to as an aura. The aura may involve visual, auditory or olfactory or even motor effects. ( recall the burnt toast eg) however in many cases the individual has no warning and directly enter the tonic phase - The postal ictal or recovery phase often begins with flaccid coma like state d/t neurotransmitter exhaustion Status epilepticus - Series of seizures in sucession with no break for recovery between them and often with no regaining of consciousness between seizures. There are considerable risks d/t acidosis, hypoxia, hypoglycemia and fever. This can lead to cardiac arrest. Respiratory and or detah of the possibility of permanent brain damage Dementia - Dementia is a disorder that is charactrized by a decline in in composition involving one or more cognitive domains ( learning and memory. language , excessive function, complex attention, perceptual motor, social cognition) ( 1) - The deficits must represent a decline from previous level of function and be severe enough to interfere with daily function and independence. The most common form of dementia in older adults is alzheimer disease acconting for 60 to 80 percent of cases - Mild cognitive impairment is an intermediate clinical stage between normal congition and dementia. While specific subtle chnages in cognition can occur in normal aging, MCI cal also be a precursor to dementia. At the same time, MCI may alos represent a reversible condition in the setting of depression, as a complication of certain medications, or during the recovery from an acute illness. - As the population ages, the overall burden of dementia is increasing worldwide. With an aging population and growing awareness of AD and other late life dementias, clinicals should be equipped to test for cognitive impairment and ask about functional decline to avoid failure to recognize casses of AD and related dementia. Clinicals will need to accurately digbose and manage the eraly cognitive manifetsiaon of AD and other dementias The most common neurodegenerative conditions causing demntias are - Alzheimer disease - Dementia with lewy bodies: one of the most common type of degenrative dementia, second to alzheimer disease. In addition to dementia, distinctive clinical features include visual hallucinations, parkinsonism, cognitive fluctuatic, dysautonomia, sleep disorder and neuroleptic sensitivity - Frontotemporal dementia : group of clinically and neuropathologically heterogeneous neurodegenerative disorders chracterized by prominent changes in social bhevaiour and personality of aphasia accompanied by degeneration of the frontal or temporal bone - Parkinson disease dementia Parkinson disease dementia ( pdd) - Cognitive dysfunction is common in parkinson disease and exists on a continuum of severity prevalence increases with the duration of the movement dsorder. When severe, dementia often surpasses the motor features of PD as a major cause of disabi;ity and mortality - While PD can coexist with other common cause of dementia, such as alzheimer disease and vscaulr dementia, mild cognitive impariment and dementia are increasingly recognized as common features of PD itself. The clinical characteristic and course of current investigation.clinical features can generally distinguish between PD and other movement disorders associated with dementia, such as dementia with lew bodies or progressive suprenuclear palsy. However, whether PD dementia and DLB are distnct disorders, or whether they represent different presentation of the same disease, is an area of debate and investigation. Alzheimers disease - The basic pathological chnages that occur in alzheimers disease involver atrophy of the cerebral cortex with neurons being lost especially in the frontal and temporal lobes - The diagnosis of alzheimers is difficult since it is S/S can be confused with depression, tumor of brian injury, nutritional deficiences, sevre anemia or durg toxocoties - Protein makers associated with the disease shw promise as eraly dignostic tools - Alzheimers can appear at any age although the frequency increases with increasing - The disease is progressive moving through stages of severity ALZHEIMER’S DISEASE - Stage 1: S&s include eraly cognitive changes with mild mental impariment ( loss of intellectual function) this may involve forgetfulness of recent events of being overwhelmed by simple tasks succh as banking or sorting change when shopping - Stage 2: this stage generally involve imapired judement and the this can lead to a need for constant supervision. Memory loss increases so that basic information such as address and phone number cant be recalled. There is often changes in behaviour so that often inappropriate social behaviour, agitation/irritation and repetitive behaviour patterns. - Stage 3; in this stage there is often a loss of bowel and bladder control ( incontinence) as well as a lack of interest and inability for personal hygiene and self care. Parkinson’s disease - The pathophysiology of this disease involves a dcrease in the neuron production of the neurotransmitters dopamine ( or its precursor l dopa ) - The causes of primary parkinsons are unknown ( idiopathic) primary parkinson’s occurs most commonely in the elderly ( after age 60) Secondary parkinson’s can be linked to: - Carbon monoxide poisoning and variety of chemical exposture’s An episode of encephalitis Post truma to the head ( recall mohammed ali the famous boxer and other boxers) Cerebral vascualr disease of other neurodegnrative diseases Exposture to some antipsychotic/tranquilizer drugs such as chlorpromazine Parkinson’s disease - Menifestaion of this disease are inietially insidious with a gradual slowing of movement and some muscle weakness but it is relentlessly progressiv. Multiple sclerosis - Problem of demyeliation of the axons of neurons - The demyelination occurs in a ptchy distribution and where the myelin sheathdegnerates is still leaves the axons intact but now the rate ( and efficiency) of nerve impulse conduction is greatly reduced - The effects is as if impulses were not conducted so that there will be function loss that depends on which nerves are affected - Wide range of possible signs and symptoms making the disease more difficult to diagnose Risk afctors for M.S include: - GENDER: ie. about 2x more common in women AGE: ie. more common in the middle years -over 15 And under 55 years of age range GEOGRAPHY: the incidences is highest in white and more affluent population in temperature climate zone such as in n.e north america ( great lakes region) northern europe, new zealand and australia- for unknown reasons. - Genetics: there is a higher incidence within some families and there are autoimmune aspects to the disease Eraly manifestaions - Transitory diplopia, blindness, blurry vision or scotomas - Motor effects such as muscle weakness and tremors - Sensory effects shc as paresrhesia - fatigue , emotional swings - Bowel or baldder problems such as urgency, frequency and constipation Intermediate manifestaion include - Speech problems - Increasing visual problems - Worsening, bowel and bladder problems - Decreased muscle control and strength leading to a general decreased in mobility, altered - Gair, muscle spasticity and contractures - Reduces sexual fucntions such as impotence in men Late maniifestaions include - Reduced mobility or immobility leading to decubitus ulcers. Contractures - Speech impairment/ communication problems - Blindness - Increased risk of respiratory infection - Incotinence - Depression and other emotional problems Cerebral palsy ( CP) - Cerebral palsy occurs at the rate of about one to five cases per 1000 live births, it involves brain damage causing neuromuscaulr disability. This may involve damage to the motor cortex, basal nuclei, cerebellum, pyramidal tracts or extrapyramidal tracts. It may involves all degrees of motor deficit ranging from minor coordination loss or loss of muscle tone to severe disability with muscle paralysis. Cerebral paslsy is not a progressive disorder. Causes of cerebral palsy - 1. Problem in letal development - 2. Birth injuries that lead to anoxia ( lack of oxygen) ischemia - 3. Anoxia neonat orum- occuring in the period from birth to the end of the fourth week post partum - 4. Problem in infancy S&S- effects on mobility - In infancy there is often a decrease in muscle tone and a delay in motor development from what is normally expected - Muscle spasticity - Athetosis - Anaxic movement Week 7 Burns - Injuries to tissues caused by contact with dry heat, moist heat, electricity, chemicals, friction, or radiant and electromagnetic energy Burn injuries influence a variety of systemic, circulatory and metabolic changes Integumentary, cardiovascular, respiratory, thermoregulation and metabolic, renal, immunity, psychological Children and elderly more susceptible, also those of lower scocioeconomic status Terminal injuries Integument Effects Skin is largest organ of the body constituting 20% of body weight Three zones of injury described in burn wound Necrosis is the area in the burn wound where coagulation necrosis has occurred Zone of stasis is a region of decreased blood flow that is reversible with adequate resuscitation Zone of hyperemia comprised of minimally injured tissue that usually recovers normal function Depth Classification Divided into four classifications based on American Burn Association criteria First degree Superficial; outer epidermal layers Second degree Superficial partial thickness (epi and parts of dermis) and deep partial thickness (entire dermis) Third degree full thickness (entire epi, dermis and subcutaneous) Fourth degree full thickness with bone or muscle involvement First degree burns ● ● ● ● ● Involve only outermost layers of the epidermis Signs and symptoms: local discomfort, erythema, HA, chills, nausea and vomiting Typically self-limiting, healing in 3-6 days e.g. mild sunburn Second degree burns Superficial Partial-Thickness Burns ● ● ● ● ● Involve the epidermis to the level of the dermis appear red to pale ivory; blisters, pain Injuries typically heal in 7-21 days in the absence of wound infection Hair typically reappears Deep Partial-Thickness Burn ● ● ● ● ● ● Involve entire dermis Mottled appearance large areas of waxy-white tissue surrounded by light pink or red tissue; flat, dry blisters, edema, pain Usually excised early and treated with skin graft to diminish scarring and achieve early wound closure Third and fourth degree bruns Third-Degree Burns ● ● ● ● Involve epidermis, dermis, and underlying subcutaneous tissue Appear white, cherry red or black, with deep blisters ● ● ● ● ● Wound has dry, hard, leathery texture Extensive edema; no pain Often require skin grafting Fourth Degree Burns ● ● ● ● Full-thickness injuries that extend beyond the dermis to involve muscle, bone, or both Often occur in victims of high-voltage electrical injury or those with prolonged exposure to intense heat Terminal injuries ● ● ● ● ● ● ● Besides depth, extent of injury is also important Refers to percentage of total body surface area (TBSA) burned Rule of nines used to calculate rough estimate of TBSA involved Lund and Browder chart is more precise Includes consideration of age and anatomic part Minor, Moderate, Major Burn Shock and Acute Resuscitation ● ● ● ● ● ● ● ● ● Capillary leak occurs within minutes and persists for 24 hours fluid lost in the area of the burn and internally collects in nearby soft tissues causing interstitial edema Rate and volume of fluid lost directly related to severity of burn Necessitates fluid and colloid replacement Immune Response also contribute to burn shock Cytokines act directly on the burn wound and activate agents that cause further local and systemic inflammation; multisystem organ failure Fluid and fibrinogen leave the dilated, permeable vessels System complaoctions of terminal bruns Cardiovascular Dysfunction - CO drops (reason unknown); vital organ perfusion is impaired Metabolic Response - Stress of burn and release of epi, NE increases MR, heat, nutritional requirements Renal Dysfunction - Hypovolemia causes renal dysfunction - Nephrons also damaged by myoglobin, drugs - Decreased peristalsis; gastric ischemia and stress → acute peptic ulcers GI Immunity - Sepsis is a significant complication - Loss of skin barrier and invasive monitoring equipment Respiratory dysfunctions - Acute lung injury is the result of obstruction (bronchospasm - and edema), inhalation of toxic fumes and thermal injury - Inhalation injury results in chemical denaturing of pulmonary - tissue and edema - Onset within first few hours but clinically manifests 2-4 hours - later - Acute respiratory distress syndrome (ARDS) usually seen - within 6 days Elemental of burn injury survival ● Meticulous wound management ● Adequate nutritional support to establish positive nitrogen ● balance ● Early surgical excision and grafting of full-thickness wounds Wound healing ● Main concerns are flexor ● contractures, excessive scarring, ● and keloid formation ● If adequate range-of-motion ● exercises are not instituted early in ● hospital course, new tissue will ● shorten and contracture will result; ● therapy aimed at extension of body ● parts ● Scarring is genetically inherited ● ● burn garments prevent hypertrophic scarring Term 2 GI pathology Liver function; The liver doesn’t look spectacularly complex in structure but in fact it is an extremely complex organ with a huge array of enzymes etc. that allow it to carry out a very wide range of funtions including; In CHO metabolism; it can do i. glycogenesis - building glycogen from excess blood glucose especially immediately after a meal ii. glycogenolysis. Between meals as blood glucose levels fall it can convert the glycogen it has stored back into glucose to maintain blood [glucose] iii. gluconeogenesis. When fasting and after the stored glycogen has been used up the liver can convert nonpCHO’s such as lipids and proteins into glucose to maintain blood [glucose] iv. overall it has a critical role in maintaining the blood [glucose] under regulation by insulin and glucagon in Protein metabolism; -synthesis of the blood proteins including the clotting proteins ( prothrombin, fibrinogen and the factors), albumins ( for maintaining blood OP) and globulins (transport proteins) as well as complement proteins that are necessary for immune function. 1. Deamination which involves removal of the amino group from amino acids so that the remaining carbon skeleton can be used to build many other molecules including CHO’s and fatty acids. The amino group is a toxic nitrogenous waste and so the liver converts it to water soluble urea so that it can be eliminated by the kidney. 2. Transamination which allows the liver to convert any nonessential(12) or any essential (8) amino acid into any other non-essential amino acid so that in this way in spite of whatever proteins were ingested the liver will be able to ensure that the amino acid profile that circulates in the blood to the tissues will be the optimum for protein synthesis functions. In Lipid metabolism; - lipolysis. The liver can break down lipids for use as an energy source of to do gluconeogenesis - lipogenesis. The liver can synthesize many lipids including triglycerides ( for storage), HDL’s and LDL’s ( for transport) and cholesterol. Lipid production of cholesterol is critical because it is used for many functions including as a membrane component, for bile salt production and as a necessary precursor to the synthesis of steroid hormones such as aldosterone, corticosteroids, progesterone, testosterone and estrogen. - in Storage; The liver can store glycogen, triglycerides, all the lipid soluble vitamins (A,D,E,K) and vit. B12 as well as iron as ferritin (bound to a protein) or transferrin ( for transport to the bone marrow) - Detoxification. The many enzymes it has allows it to break down a wide range of chemicals that may have been ingested accidentally or produced by bacteria as well as many drugs and even alcohol. Thus it reduces risks of toxic destruction of tissues - Regulation of hormone levels in the blood. Most hormones can be broken down by the liver so that they cannot accumulate in the blood. - Removal of pathogens and foreign materials that enter the blood via the GI tract. Specialized phagocytic cells called Kuppfer cells line the liver sinuses ( as reticuloendothelial tissue) and engulf foreign cells as the percolate through the liver - preventing them from entering general circulation. Note that all blood flow from the GI circulation ( splanchnic circulation) must first go through the hepatic portal vein and thus through the liver before entering general circulation. This way the liver can adjust everything about blood chemistry before it reaches the other tissues. - Destruction of worn out red blood cells (RBC’s) occurs in the liver. THe iron in heme of hemoglobin is stored as ferritin for reuse, the globin protein is broken down into amino acids for reuse and the piment in heme which is toxic is converted to conjugated water soluble bilirubin and added to the bile so that it can be eliminated in feces ( turns them brown) - The liver synthesizes bile salts which it adds to the bile. These salts are responsible for emulsification of fats (mechanical digestion - making large globules into smaller globules) so that lipase enzymes can act more effectively to chemically digest the fats. Jaundice. This term refers to the yellowish-bronze colouration of connective tissue in the skin and other locations d/t the accumulation of bilirubin pigment that is produced when hemoglobin is broken down. It is usually most obviously seen in the sclera of the eyes. There are three main ways for jaundice to develop; Prehepatic jaundice; This involves the excessively high rate of RBC destruction so that , although the liver function is normal it is unable to completely process the high levels of bilirubin produced ie. it is unable to completely conjugate it all into a water soluble form so that blood levels of both conjugated and unconjugated bilirubin will rise. The main causes of this will be ABO and Rh blood incompatabilties (eg. transfusion reactions), Malaria and sickle cell disease. Manifestations will include hyperbilirubinemia ( conjugated and unconjugated), dark coloured feces ( d/t high bilirubin level eliminated via the bile into the small intestine) and dark urine ( d/t high levels of the bilirubin in the feces being reabsorbed and then filtered out via the kidneys). There will also be the typical s/s of anemia d/t the destruction of RBwC’s. Posthepatic jaundice; This is a result of an obstruction of the biliary tract ( eg.t he common bile duct or the hepatic duct or the outlet of the common bile duct into the duodenum. Typically these obstructions occur d/t obstuction by gall stones (cholelithiasis) or inflammation of the duodenal mucosa d/t alcohol abuse. In these cases the bile is unable to enter the duodenum and so backs up toward the liver. Manifestations include pale stools ( since bilirubin doesn/t reach the SI), dark urine ( the bilirubin re-enters the blood and is filtered out by the kidney) , hyperbilirubinemia (conjugated) and steatorrhea which is seen as fatty/oily/greasy and often foamy stools as a result of greatly reduced fat digestion since the bile salts necessary for fat emulsification are not reaching the SI from the liver. Often this lack of fat digestion leads ot inadequate absorption of vit.K produced by the gut flora and so since the vit.K is needed for clotting protein production by the liver there will be bleeding disorders. There may also be severe pruritis since the bile salts are not secreted so instead they will enter the blood and irritate skin and other tissues. Hepatocellualr or intrahepatic Jaundice; This involves some problem with the liver itself which could be d/t infection by viruses or bacteria or exposure to toxins including some drugs ( eg. acetaminophen) or alcohol or environmental toxins leading to liver inflammation or hepatitis. In this case the liver will not be able to carry out many of its critical functions and there will be many serious manifestations including; - hyperbilirubinemia ( unconjugated) and obviously pale stools and urine - hormone imbalances since the liver will not be breaking down hormones they will accumulate to high levels. There are many possibilities here but some common effects include gynecomastia ( enlarged breasts in males d/t accumulated adrenal estrogens) hirsutism ( increased hairiness in females d/t accumulated adrenal androgens), cushings syndrome ( d/t accumulated aldosterone and glucocorticoids) etc. etc. - increased episodes of drug overdose and other toxicity reactions because of decreased liver breakdown of drugs - decreased fat digestion d/t decreased liver bile salt production leading to some steatorrhea and decreased vit.K absorption - much wider variation in blood [glucose] and amino acid profile as a result of decreased liver ability to carry out the wide range of chemical reactions necessary. With hepatocellular jaundice you may see hemorrhagic symptoms because the livers functions have been directly compromised by a liver pathology so that it's capacity to produce prothrombin, fibrinogen and other clotting factors may have been reduced. With post hepatic jaundice - liver function may be normal but since no bile is reaching the duodenum then fat emulsification, digestion and absorption will be reduced and so the absorption of fat soluble vitamins such as vitamin K will also be reduced. Vit. K is essential for prothrombin synthesis in the liver. Hepatitis Hepatitis is an inflammation of the liver. It can occur as a result of a number of causes including bacterial or parasitic infection , chemical toxicity by chemicals such as alcohol, acetaminophen, many solvents etc. or by viral infections. There are quite a few forms of viral hepatitis including; Hepatitis A : Also referred to as HAV it is an RNA virus. Hep A is the most common viral hepatitis and though the incidence is declining in North America it still very common worldwide , especially in the developing nations. The mode of transmission of Hep A is the fecal oral route which usually means that it is found in contaminated water, milk and a wide variety of foods such as vegetables that have been grown using fecally contaminated irrigation water or exposed to contaminated dust. It is often also associated with shellfish which are filter feeders and accumulate the virus from contaminated waters. It is also possible to transfer the virus in anal-oral sex. Young children (under 7 years old) are often completely asymptomatic when infected. People at greatest risk include tourists to the developing countries where sanitation may not be as effective, child care workers (ie. dealing with young children and their diapers), health care workers ( when handwashing is inadequate). The usual incubation period is 2-6 weeks and the individual can be infectious 2 weeks before showing jaundice or other s/s. The signs and symptoms involve an acute hepatitis with a mild fever, vomiting, anorexia , fatigue and malaise (ie. typical signs of most viral infections) along with hepatomegaly (enlarged liver) and , of course, jaundice. Usually recovery is quite rapid and there are almost never any long term effects such as chronic hepatitis or cirrhosis. Very rarely hepatic failure may occur. The virus seems to be completely cleared from the system and the individual now has life- long resistance. A vaccine is available and is highly recommended for anybody doing much international travel. Hepatitis B : also known as HBV is different from the other viral forms of hepatitis in that the virus is a DNA virus. It is quite common and a far greater risk than Hep A. The virus is transmitted in body fluids. Primarily it is transmitted in blood and blood products. It has become much less commonly transmitted in blood transfusions because of effective screening but it may be associated with surgical accidents or other exposures to blood such as needle stick injuries, shared (reused) needles, shared razors or piercing tools etc. The virus can also be found in saliva , semen and vaginal secretions (and to a lesser extent in tears and urine) so it cn be transmitted by sexual activity. Those at most risk include intravenous drug users, long term male prisoners, frequent recipients of blood products, recipients of dialysis treatment, gay males and health care workers such as nurses, doctors, dentists and hygienists. The incubation period ranges from 1-6 months .One problem with HBV is the high frequency of asymptomatic carriers ( about 50%) and the other problem is that a certain % of cases (around 10 % ) develop chronic hepatitis that may progress to cirrhosis and others will go on to develop hepatic cancer. There is a Recombinant DNA vaccine that is available and it is routinely given to health care workers and school age children. Hepatitis C or HCV: This is a single-stranded RNA virus which is primarily transmitted via the blood so the highest risks are associated with blood transfusions, intravenous drug use and needle-stick injuries. Other body fluids don’t seem to be a risk. HCV can manifest as an acute or chronic disease but typically it is chronic and slowly progressive and creates a significant risk of liver cancer (hepatocellular carcinoma) and cirrhosis. In some cases it can also be an asymptomatic carrier condition. There are no preventative vaccines or effective treatments currently so universal precautions and adequate screening of the blood supply are essential. Hepatitis D or HDV or delta virus; This is an incomplete RNA virus and is unable to replicate or infect very effectively except in the presence of HBV. HDV is transmitted via the blood and it will increase the severity of an HBV infection. Hepatitis E or HEV ; This virus is a single stranded RNA virus which creates s/s similar to HAV and like HAV it is fecal-orally transmitted. Typically you see a severe though self limiting acute infection. It is more common in Asia and Africa and it can cause significant mortality, especially to pregnant women. Generally for Acute viral hepatitis infections there are several distinct stages to the course of the infection including; The pre-icteric stage or prodromal stage. Which can be very vague and generalized involving few symptoms or things like fatigue, malaise, nausea and muscle aches like many other viral infections. There may be some URQ discomfort d/t livefr enlargement and elelvated blood levels of intracellular hepatic enzymes ( eg. ALT, AST etc.). The icteric stage involves jaundice ( elevated blood levels of bilirubin as seen as yellowish colouration in skin and connective tissues . There may be a wide variety of manifestations of decreased liver function such as prolonged clotting time, pale stools, dark urine, pruritis, wider variations in blood chemistry and endocrine imbalances as well as hepatomegaly and ||URQ| pain. The post-icteric stage or recovery stage may last for weeks and show gradually reducing s/s . Alcohol abuse and alcohol liver disease: Several important aspects of alcohol need to be understood; it is extremely toxic- no living cells can tolerate exposure to it for very long without dying. That is why the liver is so well adapted to detoxifying this chemical Alcohol is lipid soluble and so it is rapidly absorbed along the entire length of the digestive tube from mouth to large intestine. It also is able to rapidly cross the blood brain barrier that protects us against so many other toxins. Alcohol has an extremely high energy content.. Much higher than CHO’s it delivers about 75% more calories by weight than carbohydrates. A single serving of alcohol is about as many calories as eating a whole potato but it also has no nutrient content. The brain can normally only use glucose as an energy source but since alcohol can be quickly metabolized into acetyl CoA the brain can utilize it as well. In fact because of its high energy content the brain will preferentially use alcohol as an energy source and so we can develop neurological dependence. As dependence increases there is a risk that when alcohol is not available the brain will undergo a withdrawal response. This can be a very serious problems for those addicted to alcohol because the withdrawal symptoms can include; tremors, Delirium tremens, hallucinations, a variety of psychoses and seizures. Alcohol acts as a neurodepressant - similar to barbituates and other pharmaceuticals so it may exacerbate their effects and , of course, decrease many brain functions Since alcohol is so toxic the liver has adapted by having two different systems for detoxifying it; A. Alcohol dehydrogenase enzyme found in the hepatocytes cytoplasm. B. MEOS or Microsomal Ethanol Oxidation System – and array of enzymes that participate in the detox of many chemicals. MEOS is found in the smooth endoplasmic reticulum of hepatocytes. For both systems increasing levels of alcohol intake will provoke an increase in the production of the enzymes for detox. This will lead to the development of tolerance. Heavy drinkers are able to consume more alcohol and not show the toxic inebriating qualities as quickly because they are detoxifying the alcohol more quickly. Drunkenness becomes much more expensive to achieve ( bizarre a goal as that may be) but more importantly this increase in detox enzyme levels will interfere with pharmaceutical drug actions. Many pharmaceuticals are broken down by the same enzyme systems as alcohol and this has two important implications. If an alcohol abuser is not drinking then the enzymes are available for detox of other drugs so in order to maintain an adequately therapeutic circulating level of the drug a much larger dose must be taken. Often dosages far higher than typical are require. If, however, the individual begins drinking alcohol again then the alcohol competes with the pharmaceutical for detox enzymes and so even a low dose of the drug may lead to toxic overdose blood levels. For this reason few practitioners are willing to prescribe a high dose of a drug to treat other health issues because of the risk of overdose. The competitive effect of alcohol for the detox enzymes also can lead to toxicities for a variety of industrial solvents, carcinogens ( eg. Aflatoxins and nitrosamines) vitamins( mainly A & D ) anesthetics and some simple over the counter drugs such as acetaminophen),. Alcohol abuse, of course, has many other negative effects including; interference with the liver metabolism of uric acid leading to uric acid accumulation. This is referred to as gout and it can be very painful as uric acid crystals accumulate in tissues such as the joints. Direct damage to the GI mucosa leading to high risk of peptic ulcers and pancreatitis Malnutrition as a result of a decrease in food intake since alcohol can meet the bodies requirement for energy ( high caloric content) and so an individual can feel satiated and not seek food intake. Alcohol though has no nutrient content so general malnutrition develops and this can often be observed as tissue wasting. Often the muscles of the arms and legs decrease significantly in mass. Since the liver is the site of alcohol detoxification – prolonged exposure of the liver to alcohol can lead to direct damage to liver tissue. Initially the liver is able to cope with cell loss caused by ethanol toxicity because it has a limited ability to regenerate. New cells grow back to replace those that are killed. Eventually ,though, alcohol damage will exceed the ability to regenerate and so the necrotic tissue is replaced by fibrous connective tissue or scar. This replacement of normal ( parenchyma) tissue with scar is referred to as cirrhosis . Scar has two disadvantages. Scar only fills in spaces where tissue damage has occurred and it is unable to carry out the functions of normal tissue such as hepatocytes and so we see many of the same s/s as with other forms of hepatitis/hepatocellular jaundice. Blood chemistry varies more widely – including [glucose] and amino acid profile. Blood hormone levels are more variable and often reach much higher levels ( eg. Gynecomastia, amenorrhea, hirsutism, Cushings syndrome etc.). Many metabolic byproduct levels rise to toxic status, unconjugated bilirubin levels rise and bile production is reduced. The levels of blood proteins produced by the liver are also reduced – including complement, clotting proteins , transport globulins and albumins. The second disadvantage to scar is that it is a much more disorganized tissue so that the normal sinus channels of the liver through which blood from the splanchnic circulation percolates from the hepatic portal vein to the hepatic vein become disrupted. This slows the passage of blood through the liver and backs it up into the splanchnic circulation ( ie. Increased hepatic portal pressure). This elevated portal pressure can lead to varicosities ( varicose veins) in the GI circulation- especially it can cause esophageal varicies that can gradually erode away and lead to massive bleeding into the gut. This can lead to hypovolemic shock d/t blood loss and azotemia as a result of rapid digestion of all those blood proteins in the gut. Azotemia is neurotoxic in its effects and can lead to coma.. Abdominal ascites and edema are also common as a result of the increased local venous hydrostatic pressure ( ie. Increased portal pressure) and also because the compromised liver is no longer producing adequate albumins so that the blood Osmotic pressure is reduced. Before alcohol causes cirrhosis there are a number of alcohol-induced changes in the liver. Initially the liver is provoked into greater lipogenesis and the fat is accumulated in the hepatocytes and the liver enlarges and becomes yellowish in colour. This condition is referred to as Fatty Liver Disease. It can be reversed if an individual ceases to ingest large amounts of alcohol but it is also the first step to cirrhosis if alcohol abuse is not discontinued. Alcoholic hepatitis is an intermediate stage that will follow fatty liver disease is alcohol consumption continues. The s/s can be similar to those of other forms of hepatitis – including jaundice, hepatomegaly, s/s of reduced liver function etc but if there is very high levels of alcohol intake it can also become dramatically and rapidly fatal. In many cases – because of the regenerative capacity of the liver – if drinking is discontinued the condition can resolve. If not it can progress to cirrhosis. Appendicitis: This is a common problem affecting 7- 12 % of the population at some point. It can occur at any age but it is most common in the age 5-30 range – especially for 20-30 year olds. It involves obstruction inflammation and infection of the appendix ( a narrow blind tube at the junction of the ileum and the large intestine- a evolutionarily vestigial organ with no function in humans so the typical treatment involves surgical involvement with typically no complications. Obstruction may be d/t fecoliths, scar tissure, twisting (eg.volvulus) andforeign bodies such as buttons, plastic, fruit pits, coins etc. This leads to stasis of secretions/contents leading to irritation that results in inflammation. Subsequently there can be overgrowth of bacteria the invade the wall leading to further inflammation. The increased pressure, stretching of the wall and inflammatory mediators can lead to severe pain and gradually erosion of the wall. The inflammation can cause local peritonitis and there is the risk of rupture leading to severe bacterial peritonitis. The earlier peritonitis can also lead to increased LI wall permeability leading to bacterial peritonitis. Early s/s - include a sudden onset of generalized abdominal pain ( epigastric of periumbilical) that is often wavelike or intermittent. The pain results from stretching of the appendix wall. This severe pain can lead to anorexia, nausea ( possible vomiting) and an SNS response. Later s/s - ( ie 2-12 hours later) pain becomes localized in the lower right quadrant and becomes more steady. This is d/t local parietal peritonitis. It may be aggravated by walking, coughing, bending or external pressure. There is often rebound tenderness –ie area is compressed and pain reduces but returns when the pressure is released. Often there will also be systemic s/s including mild fever, leukocytosis, malaise and increased ESR. There may also be constipation or diarrhea and rigid abdomen associated with peritonitis( spasming of abdominal muscles over the inflamed area) Notes on first aid. It is a medical emergency(911) and no laxatives should be given( could provoke rupture), no pain relief medication that might masks/s and no heat applied because it could exacerbate the inflammation. Complications include – perforation of the appendix wall ( often indicated by sudden cessation of the pain) potentially leading to life threatening peritonitis - gradually developing bacterial peritonitis as inflammation continues - abdominal abscess leading to obstruction Peritonitis. This term refers to inflammation of the peritoneum. There are two main causal categories of peritonitis. Chemical peritonitis occurs when any caustic or irritating substances enter the peritoneal/abdominal cavity. This can include solid materials like surgical sponges or gauze , or instruments, suture materials etc but most commonly it is chemicals such as blood that has leaked in or perhaps caustic materials that have entered the cavity via gut perforations or ruptures – this can include gastic HCl or pepsin through stomach ulcers, enteric and pancreatic enzymes through duodenal peptic ulcers, bile from a gall bladder rupture or perforation or enzymes in pancreatitis. The other main form of peritonitis is infection. Typically this will be gut bacteria that have passed through into the cavity through diverticulitis or appendicitis but it can also occur if there is chemical peritonitis that has caused peritoneal inflammation that increases the permeability of the gut wall allowing bacteria to pass through – ie bacterial peritonitis as a sequel to chemical peritonitis. Bacterial peritonitis can also occur as a result of abdominal ascites or as a result of bacterial infection resulting from peritoneal/ internal dialysis. Peritonitis may be localized leading to local severe pain etc but it may also be generalized to much of the peritoneum./abdominal cavity. In this case the pain will be extremely severe with an accompanying severe SNS response as well as nausea and vomiting. It can lead to paralytic ileus or silent bowel – a form of functional obstruction since the inflammation interferes with neural control over peristalsis and peristalsis ceases. Peritonitis can be very difficult to treat and resolve and has a very high mortality rate associated with it. Intestinal Obstructions They can be classified into two main categories A. Mechanical (physical obstructions) including; Adhesions- abdominal fibrosis. Scars lead to tension and constriction Hernias- protrusions through weakened walls-> trapping and strangulation Volvulus – twisting leading to compressed BV and nerves-> gangrene Intussusception – proximal area invaginates into distal portion) or telescoping Neoplasms either intrinsic (inside) or extrinsic ( compressing from outside) Foreign bodies–gallstones, impacted feces -especially in narrowed regions of the gut Strictures – congenital or d/t scarring in radiation therapy, Crohn's, diverticulosis B Paralytic Ileus –cessation of peristalsis as a result of impairment of neurological control. This can happen d/t direct irritation such as with handling in surgery, trauma etc. or with visceral peritoneal irritation such as in peritonitis. It can also be associated with ischemic effects such as a thrombosis or a pinched blood vessel with volvulus or intussusception. Sometimes severe systemic effects from diseases such as pneumonia, MI or electrolyte imbalances ( eg. hypokalemia) can also cause it. Renal pathology Urinary Tract Infections: or UTI’s can be classified as Lower UTI’s are infections involving the bladder (cystitis) or urethra (urethritis) and they are far more common than upper UTI’s. The most common causative organisms are usually bacteria that are normal flora of the GI tract, especially Escherichia coli but also including Klebsiella, Proteus, Enterobacter etc. Other possible causes are some STD’s and some vaginal normal flora but they tend to be much less common. Predisposing factors include; 1. - gender ie. much more common in females d/t their shorter urethra which is less distance for bacteria to travel between urine flushings in order to reach the bladder. 2. - poor hygiene - it is important to reduce the bacterial population around the urethral orifice 3. - catheterization and other invasive procedures that can introduce bacteria further up the urethra or into the bladder 4. - other underlying pathologies like chronic renal failure or prostatitis or urinary calculi that reduce urine flow and so decrease the flushing action 5. -Diabetes which involves reduced immunity, decreased bladder sensitivity and a high level of glucose in urine that can support bacterial growth. 6. - some sexual practices 7. - age. The very young are at risk since they may have longer exposure to feces in diapers, the elderly may be at risk because they may have weaker abdominal muscles and less bladder muscle tone and so they have reduced urine flow but the biggest age group at risk is those 15-24 probably d/t greater sexual variation/less routinized practice Signs and symptoms of lower UTI’s include - urgency, frequency, often dysuria and some lower abdominal or back discomfort. In some cases, depending on the severity and bacterial species involved the urine may have a cloudy appearance and have a characteristic unpleasant odour or may be possibly tinged with blood if the bladder wall becomes too inflamed. The main complications of lower UTI’S include increased risk of an upper UTI by moving up the urinary tract directly, increased risk of forming urinary calculi and increased risk of future UTI’s. Treatment - generally involve antibiotics and increased fluid intake. Prevention - can involve increased fluid intake, drinking cranberry juice because of its high level of phenols and tannic acid which have an antimicrobial effect. Tea also contains tannins and has a mild diuretic effect. Improved hygiene and altered sexual practices ( eg. Pee right after sex) etc. can all help. Upper UTi’s can involve the ureters and kidneys including the renal pelvis and extending into the nephron tubules. This is referred to as pyelonephritis. The causes are typically direct spread from a lower UTI but it is also possible to have the infection arrive via the blood in a systemic infection. Congenital structural anomalies such as a duplex kidney ( two ureters leaving one kidney allowing reflux of urine) can also predispose. The signs & symptoms of upper UTIs usually involve all the s/s of lower UTI’s ( if you have an upper UTI it is unlikely that you would not have a lower UTI) plus there are usually a number of systemic s/s such as a moderate to high fever with shaking and chills, nausea and possibly vomiting, malaise, pain with percussion in the costa/vertebral angle and constant flank pain as the inflamed kidney stretches the renal capsule. Upper UTI’s can lead to complications such as Chronic renal failure as nephrons are gradually destroyed or if there is bilateral reduction in kidney function that develops quite quickly there could be acute renal failure. Renal Calculi or kidney stones or urolithiasis: Renal calculi are solid masses that precipitate out of the filtrate/urine typically in a crystalline form. The main factors that predispose to calculus formation include; A.) High solute concentration in the urine/filtrate. Some examples of cause include; - high [Ca++] d’t a high calcium or vit.D diet , bone disease leading to osteoporosis, hyperparathyroidism or immobility. - high oxalic acid or oxalate concentration in the diet. Sources include chocolate, tea , cocoa or rhubarb. - high magnesium ammonium phosphate as a result of a urinary tract infection by bacteria- especially with alkaline urine. - a high uric acid concentration associated with a high purine, high protein diet or with conditions of impaired liver function leading to decreased uric acid metabolism leading to gout symptoms. A common cause of this is alcohol abuse. - low water concentration of the urine that automatically leads to a high [solute]. This could be the result of a low water intake or some other form of dehydration. B.) Surfaces to act as foci for precipitation of solids. Charged surfaces especially stimulate precipitation of dissolved solutes. Tissue debris or scarred surfaces as a result of infection can provide these surfaces as can the presence of previoiusly formed calculi - ie. calculi lead to more calculi. C. Stasis of urine. Anything that causes urine to sit around or accumulate for long will allow the solute crystals to form more effectively. This could result from immobility ( eg. bed rest or unconsciousness), pregnancy as a result of progesterone induced relaxation of smooth muscle leading to retention of urine/ incomplete bladder emptying.. Obstruction of urine flow by previous calculi or infection can also do the same. D.) Urine pH . If the urine is consistently acidic it will increase the precipitation of uric acid and oxalates. If it is consistently alkaline it will increase precipitation of calcium or phosphate salts. Factors such as medications or medical infections or the use of antacids as well as ongoing challenges to systemic acid/base balance can alter the urine pH. Kidney stones - are often asymptomatic - passing through the system unnoticed. Symptoms occur when the stones are large enough and the passageways narrow enough to lead to abrasion or obstruction. In some locations such as the renal pelvis they can become quite large - looking like staghorn coral - without necessarily dislodging and causing s/s. Some typical s/s include ; - severe pain d/t abrasion and if the fluid accumulation leads to distension of the bladder or pelvis ( leading to swelling of the kidney and stretching of the renal capsule). The pain is often spasmodic or colicky pain as the smooth muscles spasm and it can be felt as flank pain or perineal depending on the site of obstruction/abrasion. Indications of the severity of the pain can be seen in scale of the SNS response. There is often accompanying nausea and vomiting. Sometimes we see fresh blood ( hematuria) d/t damage to small BV of the mucosal linings. Complications can include; - further kidney stone development - UTI’s as a result of tissue damage and obstruction leading to less effective flushing action and urine stasis. - Acute renal failure if the back up of urine leads to filtrate HP equalling glomerular blood HP so that no further glomerular filtration occurs. Benign Prostate Hyperplasia : This increase in size and change in structure of the prostate is very common in males over 50 years of age. The enlargement or growth is usually on the medial and lateral regions of the gland, thus causing a narrowing or restriction of the urethra and a subsequent restriction of urine flow. Typical manifestations include; - hestitancy - a delay in the initiation of urine flow until the pressure is high enough to overcome the resistance to flow - frequency as a result of incomplete emptying of the bladder which sometimes can lead to bladder hypertrophy and also nocturia since the bladder wasn’t emptied before going to bed - reduced force of the urine stream Typically the manifestations are initially mild and at best a mild annoyance but as the gland continues to enlarge it can lead to complications such as increased incidence of calculus formation and an increased risk of cystitis/urethritis. If the obstruction is very severe or complete it can lead to hydroureter ( dilation of the ureters) and possibly renal failure ________________________________________________________________________ ______ Acute Renal Failure: Acute Renal Failure (ARF) involves a significant and rapid decline in renal function d/t pathologic or intrinsic metabolic damage to the kidneys which will be typically lead to oliguria (very reduced urine output) and blood chemistry changes such as azotemia (highly elevated blood levels of nitrogenous wastes). The causes of ARF can be classified into three categories; A. Pre-Renal Causes; This generally means that the kidney was otherwise normal but that it is now receiving inadequate blood flow for a wide variety of reasons including; i.) Heart problems such as CHF or an MI ii.) Hypovolemic shock where there is inadequate blood volume to circulate such as in the case of severe dehydration (d/t GI losses, inadequate intake,burnsor excess diuretics) or hemorrhage leading to excess blood loss. iii.) Distributive shock in which case there is a normal blood volume but there is vascular pooling such as in the case of anaphylactic shock or septic shock iv.) Surgical/medical intervention causes such as when vessels are clamped during a surgery or as a result of increased vascular resistance stimulated by anesthetics. v.) Bilateral Renal Vascular Obstruction such as in the case of an abdominal aortic aneurysm that compresses both renal arteries or perhaps bilateral thrombus obstruction. B. Post-Renal Causes: This involves obstruction of urine outflow from the urinary tract causing a backup into the kidneys which will raise the hydrostatic pressure of the tubular filtrate so that it exceeds of equals the hydrostatic pressure of the glomerular capillary blood so no net filtration can occur. This could occur d/d i.) obstruction of the bladder outlet to the urethra by an enlarged prostate or bladder inflammation. ii.) urethral obstruction by the prostatitis, blockage by a urinary calculus, a tumour or severe infection or by traumatic damage. C. Intra-Renal Causes; that involves an initial problem with the kidneys themselves. There are many possibilities here including; i.) exposure to nephrotoxic chemicals which damage the nephron tubules such as - some antibiotics reactions such as with penicillin, tetracycline, aminoglycosides and cephalosporins - heavy metal exposure such as to lead, mercury, arsenic or uranium - some organic solvents such as carbon tetrachloride, ethylene glycol and methanol (wood alcohol) - radio-opaque contrast media such as barium used in medical diagnostic tests - some pigments such as when there is exposure to large amounts of haemoglobin in transfusion incompatability reactions or DIC or with exposure to myoglobin in muscle crush injuries ii.) acute glomerulonephritis iii.) acute inflammatory diseases such as acute pyelonephritis ( upper UTI) ARF initially has an oliguric phase in which there is a great decrease in urine output as there is decreased kidney processing. This will lead to the blood chemistry changes such as elevated BUN (blood urea nitrogen ) or SUN ( serum urea nitrogen) as nitrogenous wastes are not eliminated. When more severe it is referred to as azotemia. There will also be elevated creatinine, potassium and phosphorus levels as well as acidosis. (d/t decreased HCO3- reabsorption and decreased H+ secretion by the tubules). Sometimes there are the blood chemistry changes but no oliguria with intrarenal causes because of a decreased tubular ability to concentrate urine. Other signs of decreased renal function will be uremia ( urine components increasing in the blood – eg. Urea etc) as well as hypertension and edema as a result of attempted compensation for the decreased GFR. The diuretic phase may develop if the causes of ARF are resolved – with in a few days or up to 6 weeks after oliguria. Generally this indicates a return to normal function or recovery though the chemical changes persist as function recovers and the excess wastes are gradually reduced. ARF is often potentially reversible if it is detected and effectively treated early enough. Treatment can include; ● - resolving the underlying causes such as by restoring blood flow, resolving the obstruction or removing the nephrotoxic agent. ● - maintaining fluid and electrolyte balance ● - maintaining the CHO intake but reducing protein intake to prevent protein catabolism and reduce the risk of producing nitrogenous wastes. ● - possibly dialysis to maintain acceptable blood chemistry. If treatment is successful then there may be no permanent damage but if not renal failure has the potential to become rapidly fatal. Chronic Renal Failure; This form of renal failure is very different from ARF. It tends to be a gradually developing insidious disease that is progressive, largely asymptomatic in the early stages and completely irreversible, Generally you have no idea that you have it until the stage when there is already very large scale damage and at that point there is nothing much you can do about it except try to slow down its rate of progress. It is primarily associated with systemic disorders such as hypertension and atherosclerosis linked to obesity, poor diets and a sedentary lifestyle. It is also strongly associated with poorly controlled diabetes. Chronic kidney diseases such as bilateral pyelonephritis can also lead to CRF. In typical cases the blood supply to the kidneys is slowly reduced and there is a subsequent loss of nephrons and as a result of that a decrease in GFR. We describe the progress of the disease in three stages. Stage1 : Renal Impairment or Decreased Renal Reserve This involves up to 60 % nephron loss and GFR decreases to 40-60 % of normal. Virtually no symptoms and the only signs are a measureable decrease in GFR and a high normal blood creatinine level. Stage II : Renal Insufficiency This involves up to a 75 % nephron loss and GFR is reduced to 20 - 40 % of normal. At this stage you see alterations in blood chemistry, Usually there is moderately elelvated BUN (eg. elevated blood urea and creatinine) , moderate acidosis and diuresis ( d/t the decreased ability of the remaining tubules to adequately concentrate urine). This may lead to polyuria and nocturia. Anemia is another common symptom as a result of a decreased kidney production of erythropoietin. Stage III or End Stage Renal Failure This involves a 90% nephron loss and a GFR down to 10-15 % of normal. At this point blood chemistry changes are severe and there is a wide range of manifestations including; - Uremia (urine in blood) d/t almost complete loss of kidney function. The breath and sweat will have a distinctly urine-like odour in many cases. Blood levels of nitrogenous wastes are very high at this point - referred to as azotemia and this is toxic to most tissues. - Elevated BP as the CVS attempts to compensate for the decreased GFR ( eg. renin-angiotensin mechanism)_ - Nervous system effects include lethargy, stupor and potentially coma d/t azotemia and acidosis. There is also often significant memory loss and peripheral neuropathy leading to decreased sensation and muscle control. CI. The skin often becomes dry, thin and brittle, sometimes with a whitish uric acid/ urea crystal frosting and banding of the nails. There is typically pruritis (itchiness) d/t the effects of accumulated phosphate crystals as well as azotemia - For the GI we often see nausea as a result of the emetic centres response to toxins in the blood. This can lead to severe anorexia. There may also be an increase in GI bleeding d/t a decrease in blood platelet levels. - The red bone marrow function is suppressed (bone marrow depression) by the azotemia and acidosis and this will lead to a decrease in production of WBC’s leading to decreased immunity, decreased RBC’s leading to anemia and decreased platelet production leading to bleeding disorders. - Hypocalcemia d/t a decreased in kidney activation of vit. D leading to decreased calcium absorption. THis can lead to decreased bone density and hyperphosphatemia as you respond to the the low blood calcium levels by increasing parathyroid hormone which breaks down bone and released phoshate and the decreased kidney function leads to decreased ability to clear or eliminate the excess phosphate. - Decreased sexual function d/t decreased libido ( azotemia and acidosis affecting the brain) and amenorrhea d/t altered endocrine function. At this stage increasingly frequent dialysis is required to maintain blood chemistry within acceptable parameters but ultimately the only longterm treatment is a kidney transplant ( though there are usually long waiting lists) - otherwise the condition will lead to death. The next two pathologies involve glomerular inflammation/disease Acute Post Streptococcal Glomerulonephritis or APSGN - a form of Acute Nephritic Syndrome. This pathology is most common in children especially around the age of 6-7 at about the time that most children begin school and encounter many more children and pathogens. It is about 2x as common in boys and typically develops at one to two weeks after a nasopharyngitis episode caused by group A, Beta-hemolytic Sreptococcus pneumoniae ( ie. Strept throat) as a result of a type III hypersensitivity reaction in which antibodies are produced to certain bacterial antigens to form antigen-antibody complexes that form an insoluable precipitate. This complex will then bind to the surfaces of endothelial cells that form the capillaries, line larger blood vessels or the heart chambers or even the heart valves. In APSGN they bind to the glomerular capillaries and cause inflammation. The inflammatory changes to the glomerulus lead to two main effects; i. the lumen of the glomerular capilleries is narrowed and this leads to a reduction in glomerular filtration (ie. a decreased GFR) ii. the glomerular capillary wall becomes more permeable d/t larger gaps between adjacent endothelial cells. This allows larger things that normally don’t filter to pass through into the filtrate, including blood proteins and cells. These two effects account for most of the manifestations of APSGN. The increased glomerular permeability means that now we will see RBS’s in the urine– hematuria – causing a dark coffee or tea like colour for the urine and there will also protein in the urine ( proteinuria) making the urine cloudy. In addition since some of the RBC’s and proteins will start to clog up the tubules they will consolidate and be molded into the shape of the tubules until they are forced out under pressure leaving tiny cylinder shaped objects in the urine known as urine casts or cylinduria. The decreased GFR will lead to an overall decrease in urine output or oliguria and in response to the decreased GFR the kidneys will release more renin which through the angiotensin effects will lead to widespread peripheral vasoconstriction thus raising the PVR and resulting in severe hypertension. The hypertension will cause and increase in hydrostatic pressure in the systemic capillaries and this will lead to widespread moderate systemic edema – seen especially in the face and dependent areas and with a general weight gain d/t fluid retention in the tissues. With the decrease in kidney function there will be significant blood chemistry changes including elevated B.U.N. or (S.U.N.) , metabolic acidosis, elevated creatinine and also elevated levels of serum ASO ( antistreptolysin O – an exoenzyme against Streptococcus and systemic signs of inflammation such as an increased ESR. The individual usually also has accompanying flank pain and feels typical symptoms such as malaise, lethargy and irritability. The prognosis for APSGN is usually pretty good for children – about 95% recover completely without further reoccurrence. For adults only about 60% completely recover without any kidney damage. Complications can include; - CHF – as a result of the heart having to work against severe hypertension - Encephalopathy – as a result of the hypertension leading to cerebral edema as well as the exposure to acidosis ( a neurodepressant) and moderate azotemia ( high levels of nitrogenous wastes in the blood) - ARF if there is continued severely decreased GFR and larger scale damage to tubules. If only slowly resolved and with longer term but more gradual tubular necrosis it could lead to CRF. Nephrotic Syndrome or Nephrosis This is another glomerular pathology that involves glomerular inflammation that develops in a different way. It can have many causes and so it can be thought of as a glomerular manifestation of a variety of pathologies. The most common form of nephrosis in children is called Minimal Change Nephrotic Syndrome – a primary form of nephrosis. It is seen mainly in preschool age children, 2-7 years old with a peak occurrence in 2-3 year olds. It is more common in males than females and accounts for about 80% of nephrosis in children. Predisposing factors include - a preceeding viral URI and in some cases a familial ( maybe genetic) factor. Treatment - This form of nephrosis if treated quickly and effectively (eg. Corticosteroids mainly) typically resolves completely with little or no permanent damage though it has a tendency to recur. Secondary nephrosis can occur secondary to a variety of pathologies including Acute glomerulonephritis, SLE, drug toxicities, insect stings and other animal venoms, sickle cell disease , malaria, diabetes or Tuberculosis. In nephrotic syndrome the inflammatory change in the glomerulus is a little different leading to a greater loss of proteins but usually no loss of RBC’s so we see no hematuria but often much larger loss of blood proteins – gross proteinuria. Especially high levels of albumins are lost in the urine – gross albuminuria and this loss leads to hypoalbuminemia. We also see casts in this pathology but the cylinduria are composed mainly of proteins ( no RBC’s). The severe loss of albumins leads to a major decrease in systemic blood Osmotic pressure and so this leads to severe systemic edema ( much worse than APSGN) and as a result of the fluid shift from blood to ISF there is a decrease in blood volume so we don’t see hypertension in spite of the renal response to decreased GFR. This low OP can also lead to severe ascites, pleural effusion and elelvated ICP. Another unusual finding is hyperlipidemia and lipiduria probably as a result of a generalized liver response to having to gear up to replace the albumins that have been lost. General manifestations then include oliguria, gross edema, significant weight gain (increased fluid retention in tisues), dyspnea (d/t pleural effusion), diarrhea (d/t GI edema) and CNS depression. Complications can include, among other things, a decrease in immunity and a resulting increased risk of infection d/t the immune suppressing effects of the corticosteroid treatment, the loss of complement and gamma globulins in proteinuria and the effects of edema in decreasing exchange and nutrient delivery to tissues. With aggressive treatment there is usually recovery within 7-21 days though there is a high risk of relapse in many (around 50% ) cases. Renal anatomy - The renal papilla is the location where the meduallary pyramids empty urine into cuplike structures called minor and major calyces The minor then major calyces receives urine from the papilla of one renal pyramid Once the filtrate centers the calyces, it becomes urine because no further reabsorption can occur In the kidney the renal papilla is the location where the medullary pyramid empty urine into the renal pelvis. Histologically it is marked by medullary collecting ducts converging to channel the fluid. Transitional epithelium begins to be seen Structures of the kidney Functions of the nephron - To produce urine, nephrons and collecting ducts perfrom three basic processes; glomerualr filtration, tubular reabsorption, and tubular secretion - Glomerualr filtration: is the first step of urine production -blood pressure forces water and most solutes in blood plasma across the wall of glomerualr capillaries - Tubular reabsorption: returning most of the filtered water and many of the filtered solutes to the blood, is the second basic fucntion of the nephrons and collecting ducts - Tubular secretion: the tubule and duct remove substance, such as wastes, drugs and excess ions, from blood in the perilubular capillaries and transport them into the fluid in the renal tubules. Cortical nephron Function of the nephron Filtration, reabsorption, and secretion in the nephron and collecting ducts Functions of the nephron - Epithelial cells all along the renal tubules and collecting ducts carry out tubular reabsorption and tubular secretion. Tubular reabsorption retains substances needed by the body, including water, glucose, amino acids, and ions. - Angiotensin II enhances reabsortion of Na+ and Cl-. angiotension II also stimulates the adrenal cortex to release aldostrone, which stimulates the collecting facts to reabsrob more Na and Cl and secrete more K. atrial natriuretic peptide ( ANP) inhibits reabsorption of Na ( and Cl and water) by the renal tubules, which reduces blood volume. - The major hromone that regualtes water revaorptin is antidiuretic hromen ( ADH), via negative feedback. Transportation, storage and elimination of urine - Urine produced by the nephrons drains into the minor calyces, which join to become major calyces that unite to form the renal pelvis From the renal pelvis, urine drains first into the ureters and then into the urinary bladder; urine is then dischraged from the body through the urethra The two ureters transport urine from the renal pelves of the right and left kidneys to the urinary bladder The wall of the ureters conistss of 3 layers; transitional epithelium on the inside ( mucosa), smooth muscle in the middle, and an outer layer of areolar connective tissue The urinary bladder is aholow muscualr organ in the pelvic cavity posterior to the pubic symphysis. Its fucntion is to store urine prior to micturition The mucosa of the urinary bladder contains transitional epithelium and rugae. The muscular layer of the wall consists of three layers of smooth muscle called the detrusor muscle. The outer coat is a fibrous covering. Urine produced by the nephrons drains into the monor calyces, which join to become major calyces that unite to from the renal pelvis. - - Blood disorder From the renal pelvis, urine drains first into the ureters and then into the urinary bladder; urine is then discharged from the body through the urethra The two ureters transport urine from the renal pelves of the right and left kidney to the urinary bladder The urthera, the terminal portion of the urinary system, is a small tube leading from the floor of the urinary bladder to the exterior of the body. In females, it lies directly behind the pubic symphysis and is embeded in the front wall of the vagina, between the clitrois and vaginal opening. In males, the urethra passes vertically through the prostate, the deep perineal muscles, and finally the penis The micturtion reflex discharges urine from the urinary bladder by means of contraction of the detrusor muscle and relaxation of the internal urethral sphincter muscle, and by inhibtion of the external urethral pshincter Anemias - There are two general causes of anemias they are: - A. excess loss of RBC’s d/t excess bleeding losses or excess RBC destruction - B. insufficient production of RBC’s d/t factors such as nutritional deficiencies or bone marrow depression Increases hemopoiesis is generally insufficient to compensate for either of the two general causes. In the case of insufficient production there is no opportunity for erythropoiesis since the capacity to do so has been lost ( eg, nutritional deficiency). In the case of excess loss of RBC’s the rate of loss is much greater than the rate of replacement Basically: the main problem of anemia is that insufficient oxygen is being delivered to tissues. This will cause many effects including: ● An increase in heart rate and strength of contraction in an attempt at compensation. Chemoreceptors will detect low blood O2 concentration and stimulates the meduallryCVC centre to stimulate the heart. Over time this can lead to ventricular hypertrophy. ● Pallour ( pale color ) of the skin, mucosa and nail beds in part because of the reduction in hemoglobin pigment ( red pigment) and partly d/t SNS stimulated peripheral vasoconstriction in an attempt to increase BP in order to increase blood flow to tissues ● The rate and depth of breathing will be increased d/t the stimulation of the RCC in the medulla by chemoreceptors that have detected the low blood ( O2) ● CNS fucntion will decreased d/t the hypoxia. This will in dizziness and fainting and decreased neural activity generally ● Exercise intolerance will develop d/t the decreased delivery of o2 to muscle and neurons. The individual will fatigue easily and feel weak ● The rate of cell regeneration for healing /repair will decline d/t hypoxia ● The reproductive system will be affected in several ways. Decreased oxygen delivery will lead to decreased gametogenesis ( esp. In males) leading to decreased fertility. In females amenorrhea is a common outcome and in both genders the decreased in oxygen delivery to the brain can lead to loss of libido ➔ Anemia that develops rapidly to severe levels may show immediate s/s that result from: ➔ i) the effects of hypoxia eg. fatigue weakness, angina, headaches and dizziness ➔ ii) the effects of the compensation eg. tachycardia and pallour and increased resp rate Other s/s may arise depending on the cause of the anemia. For example excessive destruction of RBC’s may lead to jaundice ( yellowish coloration of the skin and sclera d/t accumulation of bilirubin produced by hemoglobin breakdown. If the anemia develops more slowly there may not initially be any obvious s/s because since the body is bale to gradually adapt through compensatory mechanism. Cardiac output may increase red bone marrow may be stimualte to try and increase RBC production and the hemoglobin may be altered to increase its ability to release more O2 to the tissues ( eg, hemoglobin affinity for O2 is reduced) Severe chronic anemia may lead to angina pain as the heart muscle works harder but receives less oxygen. Gradually to adapt to the increased workload the ventricles may hypertrophy which of course means that the cardiac muscles will need even more O2. this can lead to angina and ultimately to heart failure. Other problems could include a decreased growth of tissue ( especially epithelial tissue) Some of the common type of anemia, classified based on cause, include: IRON DEFICIENCY ANEMAIA. ESSENTAILLY this from of anemia is the result of there being inadequate iron available for the synthesis of hemoglobin