u
Urology
Samir Bidnur, Yooah Krakowsky and Debonh Sasgea, chapter editors
Alaina Garbens and Modupe Oyeumt. associate editors
Adam Gladwish, EBM editor
Dr. Armando Lorenzo, Dr. Keith Jarvi and Dr. Sender Henchom, staff editors
Basic Anatomy Review ................... 2
Scrotal Mass........................... 27
Abdominal Wall
Anatomy of Scrotum
Genito-Urinary Tract Anatomy
Penis Anatomy
Varicocele
Spermatocele
Hydrocele
Testicular Torsion
Inguinal Hernia
Hematocele
Common Presenting Problems ............. 3
Hematuria
Scrotal Complaints
Urinary Retention
Dysuria
Voiding Dysfunction ..................... 5
Penile Complaints ...................... 29
Peyronie's Disease
Priapism
Paraphimosis
Phimosis
Erectile Dysfunction (ED)
Premature Ejaculation
Voiding
Failure to Store: Urinary Incontinence
Failure to Void: Urinary Retention
Benign Prostatic Hyperplasia (BPH)
Urethral Stricture
Neurogenic Bladder
Post Obstructive Diuresis (POD)
Trauma ............................... 32
Infectious and Inflammatory Diseases...... 10
Infertility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Urinary Tract Infections (UTI)
Recurrent/Chronic Cystitis
Interstitial Cystitis (Painful Bladder Syndrome)
Acute Pyelonephritis
Prostatitis/Prostatodynia
Epididymitis and Orchitis
Urethritis
Urethral Syndrome
Female Factors
Male Factors
Stone Disease ......................... 15
Approach to Renal Stones
Calcium Stones
Uric Acid Stones
Struvite Stones
Cystine Stones
Urological Neoplasms ................... 18
Approach to Renal Mass
Benign Renal Neoplasms
Malignant Renal Neoplasms
Carcinoma of the Renal Pelvis and Ureter
Bladder Carcinoma
Prostatic Carcinoma (CaP)
Prostate Specific Antigen (PSA)
Testicular Tumours
Penile Tumours
Toronto Notes 2011
Renal Trauma
Bladder Trauma
Urethral Injuries
Pediatric Urology ....................... 36
Congenital Abnormalities
Nephroblastoma (Wilm's Tumour)
Cryptorchidism/Ectopic Testes
Disorders of Sexual Differentiation
Circumcision
Enuresis
Selected Urological Procedures ........... 40
Bladder Catheterization
Cystoscopy
Radical Prostatectomy
Transurethral Resection of the Prostate (TURP)
Extracorporeal Shock Wave Lithotripsy (ESWL)
Common Medications ................... 43
Antibiotics
Erectile Dysfunction
Benign Prostatic Hyperplasia
Prostatic Carcinoma
Continence Agents
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Urology Ul
U2 Urology
Basic Anatomy Review
Toronto Notes 2011
Basic Anatomy Review
Above Arcuate Line
_
"!i¥='i'-
L-
,
.
Fascia
11!::.!2::! ,..-----External Oblique
r
'
.
}; '
Abdominus
Fascia
,..----- Extra peritoneal Fat
,..------ Peritoneum
Below Arcuate Lin e)--Inferior Epigastric Artery
--.._____Skin
\..__ Superficial Fascia
\..__ External Oblique
- ----"="="";._ '--Internal Oblique
--Transversus Abdominus
.._____Transversalis Fascia
'------ Extraperitoneal Fat
'------ Peritoneum
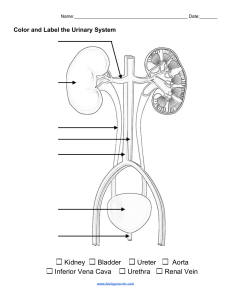
Figure 1. Midline Cross-Section of Abdominal Wall
External
spermatic fascia
Cremaster
muscle
Internal
spermatic fascia
Pampiniform
plexus
Tunica vaginalis
Dartos fascia
Figure 2. Anatomy of Scrotum
Minor
Major calyx
Pararenal fat
Renal sinus
Renal pelvis
Renal vein
Renal artery
Abdominal aorta
IVC
Ureter
Gonadal artery and vein
Renal papilla
Renal column
Renal pyramid
Renal capsule
(Gerota's fascia)
Ureter
Internal iliac artery and vein
External iliac artery and vein
Internal pudenal artery
Common penile artery
© Krista Shapton 2010
Male Pelvic Vasculature
Detrusor
Trigone
Base detrusor
Uretero-vesicular junction
Prostate
Prostatic urethra
Posterior urethra
Periurethral striated muscle-"2!rn.:.;...-Membranous urethra
Rhabdosphincter (external
Bulbar urethra : }
sphincter, striated muscle)
'
Anterior urethra
Spongy (penile) urethra
© Sandra Tavares 2007
Figure 3. Essential Genito-Urinary
Tract Anatomy
©June Li 2010
Figure 4. Cross Section of the Penis
Common Presenting Problems
Toronto Notes 2011
Urology U3
Common Presenting Problems
Hematuria
Classification (see Nephrology. NP6)
Tabla , . Etiology of Hematuria by Aga Group
B-20
Glomerulonephritis, llTI, cong..ital anomalies
2()..40
un, stones, bladder tumour
4[)..60
Male: bladder tumour, stones, UTI
Female: lJTI, stones, bladder tumour
>60
Male: BPH, bladder tumour, un
Female: bladder tumour, un
Etiology
Tabla 2. Etiology of Hamaturia by Typa
bleeding
Dyes (beets. rhodemine B in candy and juicesl
Hemoglobin (hemolytic anemial
Myoglobin (rhebdomyolysis)
Drugs (rifaiJ'1lin. phenazopyridine. pyridium. phenytoin)
Porphyria
Laxatives (phenolphthalein)
AnticoiiiJII!nts
Coagulation defects
Sickle cell dsease
Neoplasms
Leukemia
Ttmnboembolism
Stone
Trauma
Renal cell carcinoma
cell carcinoma
Wilm's tumour
Glomerulonephritis
Stone
Tumour
Uretlritis
Polyps
Foreign body
Uretlnl sbicture
Tuberculosis
Infarct
Polycystic kidneys
Arteriovenous malloiTIIiltion
History
• full history, inquire about timing of macroscopic hematuria in urinary stream
• initial: anterior urethra
• terminal: bladder neck and prostatic urethra
• total: bladder and/or above
Investigations
• gross hematuria and symptomatic hematuria require full workup
• CBC (rule out anemia, leukocytosis), electrolytes, creatinine, BUN
• urine studies:
• urinalysis (casts, crystals, cells)
• culture and sensitivity
• cytology
• imaging:
• CT/IVP to investigate upper tracts (ultrasound alone is not sufficient)
• cystoscopy to investigate lower tract (possible retrograde pyelogram)
• microscopic hematuria defined as more than two red blood cells (RBC) per high-power field
(HPF) (see Figure 5)
Acute Management of Severe Bladder HemoiThage
• manual irrigation via catheter with normal saline to remove clots
• continuous bladder irrigation (CBI) using large (22-26 Fr) 3-way Foley to help prevent clot
formation
• cystoscopy if bleeding quite active:
• identify resectable tumours
• coagulate obvious sites ofbleeding
• refractory bleeding:
• continuous intravesical irrigation with 1% alum (aluminum potassium sulfate) solution as
needed
• intravesical instillation of 1% silver nitrate solution
• intravesical instillation of 1-4% formalin (need general anesthesia)
• embolization or ligation ofiliac arteries
• cystectomy and diversion rarely
Cammon urologic CIIUUS of h111111lwi1
c., be grossly classified 115:
TIBUIIIII
Infection
Tumoun;
Ston11
U4 Urology
Common Presenting Problems
,, ,
The CUA guidelines advise: Repeat
initial urine microacopy if history of
llflllhral tnurna. IXlln:isa, or me11181.
lmmedim rllhi!Tal to nephrology if 1111y
of: proteinuria, -1' craatinine, rad cell
casts or clysmorphic RBCs
Toronto Notes 2011
I
>Z RBC,IHPF
I
I
Urinalysis and urine C&S
I
•
•
•
1. Rule out and treat benign causes {i.e. Ull)
2. If accompanied by d1J1111orphic RBC, or 1' Cr,
evalum for primary renal disease
,, ,
If neither 1 or 2, urologic evaluation required
•
Uppllf Tr-ct I-Fni Opt-
Urothtllial Cell Carcinoma {UCCI Riak Stratification
l'yela!Jam- Traditional
option and widely available, but use i$
decreasing. Reasollllble sensitivity for
UCC, but poor sensitivity for RCC.
+
+
HIGH RISK
Smoking hi&lory
Occupational chamictlllCPosura
Gross hematuria
>4Dyn old
Hx of &!Drage voiding &ymptoms
Hx of recurrent lJTI's
Ultrunnd - Superior to IVP for
8VIIIuation of renal piUllllChyma and
renal cysts. Urnillld sensitivity for UCC
and small renal masses. UIS alone is not
sullicilllt for uppar tract imaging.
•...
CT - Optimallllst for renal parenchyma,
calculi ll1d infections, but less
Complsta &valuation
and mora expentiv& thllll lltruound.
Involves elqiDIUre to l'lldiation and
inlnMIIIDUS CDIIII'IIl
1. Urine cytology
2. Upper tract imaging
LOW RISK
1. Urine cytology
2. Uppar tract imaging
+1
+ve
I
TreatUCC
+1111
i
3. Cysto.copy
3. Cysto.copy
I
I
.,.
.....
..
....
Follow up
Urinalysis, cytology, and BP at
6, 12, 24, 36 months
Figure 5. Workup of Asymptomatic Microscopic Hematuria Based on AUA Guidelines
Scrotal Complaints
• see Scrotal Mass, U27
Urinary Retention
------------------------------------------
• see Failure to Void, U6
Dysuria
Differential Diagnosis
Tabla 3. Differential Diagnosis of Dysuria
Infectious
urstllilis, 11'05f81itis, epididymitis,
vestibulitis
cervicitis, wlvovaginitis, perineal inllanmatiorilnfaelion, TB,
Naaplum
Renal cell, bladder, prostate, penis, vagiiiiWulva, BPH
C.lcul
Bladder stone, ureteral stone, kidney stone
lnlll11mltory
Seronegilliw arthropathie& (Riileliw arthritis: arthritis, uwitis, u181hritisl, drug &ide llf!ect&, autoimmune
disorders, chronic pelvic pain synctome (CPPSI. in1elslitial cystitis
Hormllllll
Endometriosis, hypoeslnlgenism
TraUIIII
Catheter insertion. post-coillll cyslitis (honaymoon cystitisI
Plychagenic
Somalimlion disorder, MOD, stress/anxiety disorder
Othar
Conteel sensitivity, foreign body
Approach
• focused history and physical to determine cause (fever, discharge, CVA tenderness,
conjunctivitis, back/joint pain)
• urine dip, C&S, R&M
• any discharge {urethral, vaginal, cervical) should be sent for gonococcus/chlamydia testing; wet
mount if vaginal discharge
• if suspect infection, may start empiric antibiotic treatment
• ±imaging of urinary tract (tumour, stones)
Urology US
Voiding Dysfunction
Toronto Notes 2011
Voiding Dysfunction
• see
GY36 for relevant female topics
Voiding
• two phases oflower urinary tract function:
1. Storage phase - bladder filling and urine storage
• accommodation and compliance
• no involuntary contraction
2. Voiding phase - bladder emptying
• coordinated detrusor contraction
• synchronous relaxation of outlet sphincters
• no anatomic obstruction
• voiding dysfunction can therefore be classified as:
• failure to store - due to bladder or outlet
• failure to void - due to bladder or outlet
• three types of symptoms: storage (formerly known as irritative), voiding (formerly known as
obstructive), post-void
Failure to Store: Urinary Incontinence
------
Definition
• involuntary leakage of urine
Etiology
• urgency incontinence:
• detrusor overactivity:
• CNS lesion, inflammation/infection (cystitis, stone, tumour), bladder neck obstruction
(tumour, stone), BPH
• decreased compliance of bladder wall:
• CNS lesion, fibrosis
• sphincter/urethral problem
• stress urinary incontinence (SUI):
• urethral hypermobility
• weakened pelvic floor allows bladder neck and urethra to descend with increased
intra-abdominal pressure
• urethra is pulled open by greater motion of posterior wall of outlet relative to anterior
wall
• associated with childbirth, pelvic surgery, aging, levator muscle weakness
• intrinsic sphincter deficiency (ISD)
• pelvic surgery, neurologic problem, aging and hypoestrogen state
• intrinsic sphincter deficiency and urethral hypennobility can co-exist
• F:M=2:1
• more frequent in the elderly, affecting 5-15% of those living in the community and 50% of
nursing home residents
Table 4. Urinary Incontinence: Types and Treatments
Type
Urga
Involuntary leakage of urile Involuntary leakage of IJ'ine
preceded by a strong,
suddan increases in
sudden Ullle to void
inlnHibdominal pressure
Etialagy
Bladder
{detrusor overactivity)
Dilgnollis
Hisloly
Urudynamics
Stress
Ovarllaw
Mixed
Involuntary leakage of
urine whan inti'IIV8Sical
pressure axceads
urethral pressure
Urinary leakage associated
with Ul'llencv and increased
inlnHibdominal pressure
Urethrs/Sphilcter weakness, Obslruction, neuropathy
post1)artum pelvic
{diabetes, MS.
musculature W8ilkn8Ss
antic:holinal'llic drugs)
Combination of bladder and
sphilcter issues
History
History
Urodynamics
Stras1 Test (hBw patient
bear downfcough)
•
• Urgancy
• Nocturia
• OV.uria
Thilit
Frequent Urgant Ni{#rtlime Di8Comfort
't'
C.usn of 11enn•1• Urinary
DIAPERS
Delirium
lnflammatiorVInfection
A1rophic
Phllllllllcautic:lllr,/Psyc:hologiclll
Epidemiology
• variable prevalence in women: 25-45%
Dalililio1
F•iluN to Store
Urinlry Tract Sr.-1111
(WTSJ (irritlltift)
History
Urodymmics
Stress Test
Excns uriu output
Resbicted mobiity/Retention
Stool impaction
U6 Urology
......
,
·}-----------------,
Voiding Dysfunction
Toronto Notes 2011
Table 4. Urinary Incontinence: Types and Treatments (continued)
Type
Urge
Sims
Owlflow
Traatmlllt
Lifestyle
Bladder habit training
Weight loss,
LWestyle
Clllheterillllion tD IIVDid
organ damage
Traat Wlderlying cause
Urge Incant!- Traidnnlnt
8ewanl of lllticholinerqic side effects
including delirium and urinary retention.
Batox
Medications:
Anticholin&rgics (1Diterodine
Kegel's exercises
Bulking agents
Surgary (slings, lVOT,
Miud
Combination of
management of urge and
stress incontinence
artificial sphinctn)
oxybutynin
(Ditropan"J. trospium
(Trosec1111. soiW&nacin
TCAs
Neuromodulation
Failure to Void: Urinary Retention
.._,,
,}-----------------,
Acute vs. Chronic llatlntlon
Acute retention is 1 medical emergency
chlllllllimd by pain and 11111ril with
nonnal bladder volume and
Acuta ovardillantion
lead Ill bllddar
rupture.
Chi'Oilic retention can be asymptomlllic
grwdy incnaud bladder voUnl
1nd detrusor hypertrophy foUowed by
atony (IIIII).
------------------
Etiology
• outflow obstruction:
• bladder neck or urethra - calculus, clot, foreign body, or neoplasm
• prostate - BPH, prostate cancer, prostatitis
• urethra - stricture. phimosis, traumatic disruption
• bladder innervation:
• spinal cord - injury, disc herniation, multiple sclerosis
• stroke
•DM
• post-pelvic surgery
• pharmacologic:
• anticholinergics
•narcotics
• antihypertensives (ganglionic blockers, methyldopa)
• over-the-counter cold medications containing ephedrine or pseudoephedrine (e.g. Sudafed•)
• antihistamines (e.g. Benadryl•, Nytol•, Sominex•)
• psychosomatic substances (e.g. ecstasy)
Clinical Features
•
•
•
•
palpable and/or percussible bladder (suprapubic)
possible purulent/bloody meatal discharge
DRE - size of prostate, anal sphincter tone
neurological- presence of abnormal deep tendon reflexes,
saddle sensation, etc.
Investigations
• CBC, electrolytes, Cr, BUN, urine R&M, C&S, ultrasound, cystoscopy, urodynamic studies, post
void residual (PVR) scan
Treatment
• guiding principles are to treat underlying cause of retention and use least invasive treatment
possible
• catheterization:
• contraindicated in trauma patient unless urethral disruption has been ruled out
• acute retention: immediate catheterization to relieve retention, leave Foley in to drain
bladder, follow up to determine cause
• chronic retention: intermittent catheterization by patient is commonly used; definitive
treatment depends on etiology
• suprapubic cystotomy
• for post-operative patients with retention:
• encourage ambulation
• alpha-blockers to relax bladder neck
• may need catheterization
• definitive treatment will depend on etiology
Toronto Nota 2011
Voicling Dyafunction
UroiOBf U7
Benign Prostatic Hyperplasia (BPH)
_ _ _ _ _ _ __ J
Definition
• hyperplasia ofstroma and epithelium in periurethral area ofprostate (transition zone) see Pigure6
• tone ofprolltlrtic smooth muscle cells plays a role in addltlon to hyperplasla.
Anterior 11r1111
lillll"'"""n
"'""
---=
/
ZIJfl8
Etiology
• etiology unknown
• androgen dihydrotestosteront: (DHT) required (converted from testosterone by
5-alpha reductase)
• possible role ofimpaired apoptosis, estrogens, ather growth factors
Epidemiology
• age-related. extremely common (SO% of50 year olds, 80% of80 year olds)
• 2596 of men will require treatment
Clinical Features
• result from outlet obstruction and compensatory changes In detrusor functl.on
• voiding symptoms:
• hesitancy, straining. weak/interrupted stres.m. incomplete bladder emptying
• decreased flow rates may be seen on uroflowmetry
• due to outflow obstruction and/or impaired detrusor contractility
• storage symptoms:
• urgency, frequency, nocturia, urgency incontinence
• thought to be due to detrusor overactivity and deaeased compliance
• prostate Is llllOOth, rubbery and symmetrically enlarged on DRE
• complications:
• retention
• overflow incontinence
• hydronephrosis and renal compromise
• infection
• gross hematuria
•bladderstones
Centnllzxn l'llripherlllzxn
EjiiCUIIIlny zona
C Meog'-' Brilllley
Figure I. Cr.....Saellon af
ProsbdB
lt'
AIIAPrDitllli Syqmn Scllre
FUIIIWJIE
Urgency
NDC!uria
WMkelrelm
lnterm-cy
llnlining
ineo.,.-811
._..g of
Each '"fll1piGm graded
out"' 5.
D-7 - Milcly wymp!DmllliG
B-19- Modlrmly aymp!CIIIIIIic
20.J5-SIIVIfllly
Nata; Dy.ril. nut ilcludad in 1100111 but
ia cammanly._illlcl with BPH
Investigations
• history
• a&&ess LUTS and effect on quality ofUfe, may include self-administered questionnaires (AUA
symptom and impact score)
• physical exam: DRE
• urinalysis to exclude UTI
• c.reatinine to assess renal function ± renal ultrasound to assess for hydronephrosis
• prostate-specific antigen (PSA) trJ rule out malignancy (iflife apectancy >10 years)
• umflowmetryto measure flow rate (optional)
• bladder ultrasowtd to determme post-void residual urine (optional)
• cystoscopy prior trJ potential surgical management
• biopsy ifsuspicious for malignancy
Treatment
• conservative for those with mild symptoms:
• watcltful waiting - 5096 of patients improve spontaneously
• includes Ufestyle changes (e.g. evening fluid restriction, planned voiding)
• medical treatment
• a-adrenergl.c antagunlsts - reduce stromal smooth muscle tone [e.g. terazosln (Hytrln-},
doxazosin (cardura•), tamsulosin (Plomax"), alfuzosin (Xatral-)1
• 5-a reductase inhibitor- blocks conversion of testosterone to DHT; acts on the epithelial
component of the prostate- reduces prostate size [e.g. finasteride (Proscar"), dutasteride
(Avodart")]
• combination shown to be synergistic (see sidebar)
• transurethral resection ofprostate (TURP):
• see Seleded UrolDgical Procedures, U40
• open prostatectomy:
• for large prostates or associated problems (e.g. bladder stones)
• suprapubic (transvesically to deal with bladder pathology)
• retropubic (through the prostatic capsule)
om.inimallylnvasivetherapy:
• prostatic stents, microwave therapy, laser ablation, water-induced thermotherapy,
cryotherapy, ¥ intensity focuaed ultrasound (HIFU) and transurethral neeclli: ablation
(TUNA)
..... ,
llpprmdllltlll'roltlta 1181
20 4:C - ct.ltnut
25t:e-pUn
50 t:e -lem111
75 t:e - oranga
I 00 cc - grapefnjt
.....
,,
Alllalm INIAiill11 fur IPH S...ry
• Rafnlctoty urilll'f rellntion
• Rac..,.n UTI1
• Rac....-.d hamaturlll Nfrll:lory111
mediDII trlltmlnt
• ._,..
!IIIIa out Cllhar
CIUIM)
•
8lu11M
US Urology
Voiding Dysfunction
Urethral Stricture
.
,.... ., .........,.....
• Lilt-Tim E1lld rlllmllmlil. hlllridl,
Definition
IIIIUPSI Trill}
• M>F
.. c.n-....n..., ...... aii:ll
,....... .,.,..,..s,.,...
NfJM2003; 349:2387-2398
lllwly:lllnlt:lnilld, daubla-bmdad, cantralllld trill
witllllll!l
of 4.5 YIIIJ.
Pllilnll: 3047 plliiiD Nth
BPH
IAignld Ill pil1:abo 7371. doxlzalin 7561
fillllllride (n • 768), « conDilali:ln 1lllrapy
(n= 786). Melli age 62.6.
CIII'IIIIMIM 11811mant-... dllllllllil
\15. finulaide Vi. cantinllillll111arapy.
Main D*-: Clnical J1R9111ion dainad 11:
fim ocamnce ol111 inl:niue IMI'bae lile of 111
IIIII fiu pcin1s in 1lla AUA sympiDm ara, ICUIII
LriiBy lllention.llllli
Toronto Notes 2011
nmrert
lrinlly111ct irluclim, ar llirwy imlli1R:a.
.... The &-¥r • • l!ldLEtion il CINTII81i¥e
incidence rlclinicll
1Dpllc:lllofar daomlin-
lft(P<0.001L fillllllride- 34!1
llld combinetioolMrlpy- &8'11IP<0.001).
Comnltion thenill¥- lillie IAIIiclive thui eitller
daaain [P<O.OOII artilllstwidl (P<O.OOII
IIane. 111111-na sV!bltdifnl:e
daaain llld fillllllridaalln.
l:.l:luiJn: long·term cantinlliJn 1herapywilh
daaain llld fillllllrida
ofll¥8111
clinicaiii'UQIIIIion othlrigl jRitllic h¥Perpln
&igniic:antlt ll1llll thui diltr811mint witb li1llar
• decrease in urethral calibre due to scar formation in urethra (may also involve corpus
spongiosum)
Etiology
• congenital- failure of normal canalization
• may cause bilateral hydronephrosis
• trauma:
• instrumentation (most common)
• external trauma (e.g. burns, straddle injury)
• other: foreign body, removal ofinflated Foley catheter, etc.
• infection:
• long-term indwelling catheter
• balanitis xerotica obliterans (lichen sclerosis or chronic progressive sclerosing dermatosis of
the male genitalia) causes meatal stenosis
Clinical Features
• voiding symptoms (obstructive symptoms)
• urinary retention
• related infections: recurrent UTI, secondary prostatitis/epididymitis
Investigations
• laboratory findings
• flow rates <10 ml/s (normal-20 ml/s) on uroflowmetry
• urine culture usually negative, but may show pyuria
• radiologic findings
• retrograde urethrogram, voiding cystourethrogram (VCUG) will demonstrate location
• urethroscopy
Treatment
• urethral dilatation:
• temporarily increases lumen size by breaking up scar tissue
• healing will often reform scar tissue and recreate stricture
• visual internal urethrotomy (VIU):
• endoscopically incise stricture without skin incision
• cure rate 50-8096 with single treatment, <50% with repeated courses
• open surgical reconstruction:
• complete stricture excision ± anastomosis, ± urethroplasty depending on location and size of
stricture
Neurogenic Bladder
Definition
• a malfunctioning urinary bladder due to a deficiency in some aspect of its innervation
4C. Gf Bllldder
Capacity (35()-500 cc;
J'ed$: (Agtj + 2) X 30)
Neurophysiology
ComplillnCI[minimal A Pmsur..tA
Table 5. Efferent Syrnpatlnmc, Parasympathetic, and Somatic Nerve Supply
Volume)
Conlraclility (vDiuniBry and &u&lllinad)
Cooperation of bladder and sphincter
Nam Fibrn
Sympathetic
Somlllic
Parasympathetic
Narve rucrt& in micluritiDII:
"12·3-4 Dlpe tile •inl orr t,.lloor.·
S1111ma11:
Nllll'lllrllllmittlr
T11111t
Kay Recaplara
T10-LZ
SZ-S4
SZ-S4
Noradrenuline
Acetylcholile
Acetylcholile
Trigone, internal sphincter, proximal LR!hra
Adrenergic {all
External s!ilincter
Nicotinic
Muscarinic (MZ. M31
Detrusor
• receptors in the bladder wall and mucosa relay information to pontine micturition centre
(PMC) and activate micturition reflex
• the PMC sends excitatory/inhibitory signals to regulate micturition reflex (normally inhibited
by cortical input)
• micturition: stimulation of sacral parasympathetic neurons (bladder contraction); inhibition
of sympathetic (IS relaxation) and sacral somatic neurons (ES relaxation)
• urine storage: inhibition of sacral parasympathetic neurons (bladder relaxation) aided by
sympathetic activation (bladder relaxation, IS contraction); stimulation of sacral somatic
neurons (ES contraction )
• voluntary action of external sphincter (pudendal n. S2-S4) can inhibit urge to urinate
• cerebellum, basal ganglia, thalamus, and hypothalamus all have input at PMC
Toronto Notes 2011
Urology U9
Voiding Dysfunction
Classification of Neurologic Voiding Dysfunction
• lesion above PMC [e.g. stroke, tumour, multiple sclerosis (MS)]: neurogenic detrusor over
activity (detrusor hyperreflexia)
• loss of voluntary inhibition of voiding
• intact pathway inferior to PMC maintains coordination ofvoiding episodes
• lesion of spinal cord [e.g. MS, arteriovenous malformation (AVM)]: detrusor sphincter
dyssynergia (DSD)
• loss of coordination between detrusor and sphincter (ie. detrusor contracts on closed
sphincter and vice versa)
• component of detrusor overactivity as well
• lesion of sacral cord or peripheral efferents (e.g. trauma, diabetes, disc herniation): detrusor
atony/areflexia
• flaccid bladder which fails to contract
• may progress to poorly compliant bladder with high pressures
• peripheral autonomic neuropathy: deficient bladder sensation -+ increasing residual urine -+
decompensation (e.g. DM, neurosyphilis, herpes zoster)
• muscular lesion: can involve detrusor, smooth/striated sphincter
Neuro-Urologic Evaluation
• history and physical exam (urologic and general neurologic)
• urinalysis, renal profile
• imaging: intravenous pyelogram (IVP), U/S to rule out hydronephrosis and stones
• cystoscopy
• urodynamic studies:
• uroflowmetry - assess flow rate, pattern
• filling cystometrogram (CMG) - assess capacity, compliance, detrusor overactivity
• voiding cystometrogram - pressure-flow study, assess bladder contractility and extent of
bladder outflow obstruction
• EMG - helps ascertain presence of coordinated or uncoordinated voiding, allows accurate
diagnosis of DSD
• video study- x-ray contrast to visualize bladder/bladder nec.k/urethra during CMG
Treatment
• goals of treatment:
• maintenance oflow pressure storage and emptying system with minimal tubes and collecting
devices is necessary to
• prevent renal failure
• prevent infections
• prevent incontinence or achieve social continence
• treatment options: depends on status of bladder and urethra
• bladder hyperactivity-+ medications to relax bladder (see Incontinence, US)
• if refractory:
- botulinum toxin injections into bladder wall
- occasionally augmentation cystoplasty
• flaccid bladder-+ clean intermittent catheterization (CIC)
Autonomic Dysreflexia
• exaggerated sympathetic nervous system response to visceral stimulation below the lesion in
spinal cord injury patients
• lesion is usually above T6/T7
• stimulation includes instrumentation, distention or stimulation of bladder, urethra or
rectum
• symptoms include: hypertension, headache, reflex bradycardia, sweating, anxiety, piloerection
• vasoconstriction below lesion, vasodilation above lesion
• treatment: remove noxious stimulus (e.g. insert catheter), parenteral ganglionic or a-blockers,
nifedipine (prophylaxis during cystoscopy)
Post Obstructive Diuresis (POD)
--------------------------
Definition
• polyuria resulting from relief of severe chronic obstruction
• >3 U24 hrs or >200 cclhr over each of two COlllleCutive hours
Pathophysiology
• ranges in severity: physiologic to pathologic process
• physiologic POD occurs secondary to excretion of retained urea, sodium, and water (high
osmotic load) after relief of obstruction
• self-limiting, usually resolves in 48 hrs with PO fluids but sometimes can continue even
after having reached euvolemic status (i.e. pathologic POD)
......
''
"Spillll •hack" earty phase foUowing
cord injury m111ilesl$ qlllonic bladder.
UIO Urology
Voiding Dysfunction/Infectious and In11ammatory Diaeaaes
Toronto Notes 2011
• pathologic POD is a sodium-wasting nephropathy that occurs secondary to an impaired
concentrating ability ofthe renal tubules due to:
• decreased reabsorption of sodium chloride in the thick ascending limb and urea in the
collecting tubule
• increased medullary blood flow (solute washout)
• increased flow and solute concentration in the distal nephron
Management
• admit patient and closely monitor hemodynamic status and electrolytes
• monitor urine output (U/0) q2h and ensure total fluid intake <U/0 by replacing every
1 cc U/0 with 0.5 cc 1/2 NS IV (PO fluids if physiologic POD)
• avoid glucose-containing fluid replacement (can cause iatrogenic diuresis)
• check Na and K q6-12h and replace prn
• follow creatinine and BUN to baseline
Infectious and Inflammatory Diseases
Urinary Tract Infections (UTI)
----------------------------
• for UTis during pregnancy, see Obstetrics, OB18
Definition
• greater than 100,000 bacterialml- midstream urine
• if symptomatic, 100 bacterialml may be significant
Classification
• uncomplicated: lower urinary tract infection in a setting of functionally and structurally
normal urinary tract
• complicated: pyelonephritis and/or structural/functional abnormality
• unresolved bacteriuria = urinary tract is not sterilized during therapy (most commonly due to
resistant organisms or noncompliance)
• recurrent UTI
• bacterial persistence = urine cultures become sterile during therapy but resultant reinfection
of the urine by the same organisms
• reinfection= new infection with new pathogen (80% of recurrent UTls)
Source
•
•
•
•
ascending (most common) - GI organisms
hematogenous (TB, perinephric abscess)
lymphatic
direct (inflammatory bowel disease, diverticulitis)
Risk Factors
• stasis and obstruction:
• residual urine in poorly flushing system, e.g. posterior urethral valves, reflux, medication
(anticholinergics), BPH, urethral stricture, cystocele
• foreign body:
• introduce pathogen or act as nidus of infection
• e.g. catheter, instrumentation
• decreased resistance to organisms:
• diabetes, malignancy, immunosuppression
• other factors:
• trauma, anatomic variance (congenital), female (short urethra)
Clinical Features
•
•
•
•
Cystitis: c....IEEPS
IIJeiJsrelle sp.
E. coli (90%), o1her G1111m-negalives
Enterococci
Proteus minlbilis.
aprophytiw.,
s.
s.
storage symptoms (frequency, urgency, dysuria)
voiding symptoms (hesitancy, post-void dribbling, dysuria)
hematuria
pyelonephritis: more severe symptoms (including constitutional symptoms, CVA tenderness)
Organisms
• routine cultures (see sidebar)
• non-routine cultures:
• tuberculosis (TB)
• Chlamydia trachomatis
• Mycoplasma (Ureaplasma urealyticum)
• fungi (Candida)
Toronto Notes 2011
Infectious anclln1lammatory Diaeaaes
Indications for Investigations
• persistence of pyuria/symptoms after adequate therapy
• severe infection with an increase in creatinine
• recurrent/persistent infections
• atypical pathogens (urea splitting organisms)
Investigations
• midstream urine R&M, C&S
• dipstick: leukocytes ± nitrites ± hematuria
• microscopy: >5 WBC/HPF in un-spun urine or >10 WBC/HPF in spun urine, bacteria,
±WBCcasts
• Gram stain: GN bacilli, GP cocci,> 1 bacterium/oil immersion field
• culture and sensitivity: midstream, catheterized or suprapubic aspirate
• hematuria workup - urine cytology; ultrasound, cystoscopy
• CT scan if indicated
Treatment
• confirm diagnosis
• identify organism and treat (TMP/SMX, fluoroquinolones, nitrofurantoin, cephalosporins)
• for mild infections 3 day course is sufficient (for treatment details see Common
Medications, U43)
• establish predisposing cause (if any) and correct
• if febrile, consider admission with IV therapy and rule out obstruction
Recurrent/Chronic Cystitis
• incidence of bacteriuria in females:
• pre-teens: 1 %; late teens: 4%; 30-50 years: 6%
• assess predisposing factors as described above
• possible relation to intercourse (postcoital antibiotics), perineal colonization
• investigations may include cystoscopy, ultrasound, CT
• antibiotic prophylaxis if >3 or 4 episodes per year in females
Etiology
• unknown:
• theories: increased epithelial permeability, autoimmune, neurogenic
• associations: severe allergies, irritable bowel syndrome (IBS), fibromyalgi.a
Treatment
• daily low-dose prophylaxis (nitrofurantoin, TMP/SMX)
• lifestyle changes (limit caffeine intake, increase fluid/water intake, smoking cessation)
• post-menopausal women: consider topical or systemic estrogen therapy
• no treatment for asymptomatic UTI except in pregnant women or patients undergoing urinary
tract instrumentation
Interstitial Cystitis (Painful Bladder Syndrome)
Definition
• chronic urgency, frequency± pain without other reasonable causation
Etiology
• unknown:
• theories: increased epithelial permeability, autoimmune, neurogenic, defective
glycosaminoglycan (GAG) layer overlying mucosa
• associations: severe allergies, irritable bowel syndrome (IBS), fibromyalgi.a
Epidemiology
• prevalence: -20/100,000
• 90% of cases are in females
• mean age at onset is 40 years
Classification
• non-ulcerative (more common) -younger to middle-aged
• ulcerative - middle-aged to older
Urology Ull
Ul2 Urology
Infedioua and ln1lammatory Diseases
Toronto Notes 2011
Diagnosis
• required criteria:
• glomerulations (submucosal petechiae) or Hunner's ulcers on C}'!l:oscopic examination
• pain associated with the bladder or urinary urgency
• negative urinalysis, C&S
Differential Diagnosis
• UTI, vaginitis, bladder tumour
• radiation/chemical cystitis
• eosin.ophilic:/TB cystitis
• bladder calculi
Treatment
• patient empowerment (diet, lifestyle)
• pentosan polysulfate (Elmiron•)
• low dose amitriptyline
• bladder hydrodistention (also diagnostic) under general anesthesia
• intravesical dimethylsulfoxide (DMSO) or Cystistat•
• surgery (augmentation cystoplasty and urinary diversion ± cystectomy)
Acute Pyelonephritis
------------------------------------
• see Infectious Diseases, ID21
Definition
• infection of the renal parenchyma with local and systemic manifestations
Etiology
• ascending (usually GN bacilli) or hematogenous route (usually GP cocci)
• causative microorganisms: E. coli (most common), Klebsiella, Proteus, Pseudomonas,
Enterococcus jaecalis, Enterobacter, S. Aureus, S. saphrophyticus
• common underlying causes of pyelonephritis: stones, strictures, prostatic obstruction,
vesicoureteric reflux, neurogenic bladder, catheters, DM, sickle-cell disease, PCKD,
immunosuppression, post-renal transplant, instrumentation, pregnancy
Clinical Features
• rapid onset (hours - day)
• LUTS including frequency, urgency, hematuria
• fever, chills, nausea, vomiting, myalgia, malaise
• CVA tenderness or exquisite flank pain
• dysuria is not a symptom of pyelonephritis without concurrent cystitis
,,
MacroBID has poor tissue penetration
and 1h818fm is not usad to treat
pyelonephritis (raquil'lll post-renal
Investigations
• urine R&:M, C&S (see Urinary Tract InfoctWns, UIO)
• blood
• CBC + differential: leukocytosis, left shift
• imaging - indicated if suspect complicated pyelonephritis or symptoms do not improve with
72 hours oftreatment
• Abdo/pelvic U/S
• IVP
• Cystoscopy
• CT
Treatment
• may treat as outpatient if hemodynamically stable, ciprofloxacin PO x 7-14 days or
cotrimoxazole (TMP/SMX) POx 14 days
• severe or non-resolving: admit, hydrate and treat with ampicillin IV and gentamycin IV
• emphysematous pyelonephritis: emergency nephrectomy
• stone obstruction: admit and emergency stenting or percutaneous nephrostomy tube
Toronto Notes 2011
Infectious anclln1lammatory Diaeaaes
Urology U13
Prostatitis/Prostatodynia
....
',
Prostlllic masuga may cMJse IIXIrllme
18ndem81Ri and incraaed risk af
inducing sepsis, abscess or apididymo-
• most common urologic diagnosis in men <50 years
• incidence 10-30%
• acute bacterial, chronic bacterial, abacterial subtypes
Tabla &. Comparison of tlla Thraa Types of Prostatilil
E1ialagy
Type 1: Acute Bill:tlriill Pramtitis
Type II: Chronic Bill:tBrill Prwliltitis
Type Ill: Chronic Pelvic Pail Syndrome {AHc:IBriil]
KEEPS (see U10 sidebar]: 811% E. coli
Ascending urethral infection and reiiUK into prostatic
ducts
01tan associated with autlst abmuctian {BPHJ,
recent cystascapy, prostatic biopsy
Most ilfections occur in 1he peripheral mne
(see Figure 61
Recurrent e.xacerblllions of acute
prostatitis signs and symptoms
Recurrent UTI with same organism
Divided into inflammlllory and non-inflammlllory
subtypes
lntraprostatic reflux of urine ± urethral hypertonia
Multilactorial (immunologicaL neuropathic,
neuroendocrine, psychosocial)
AcLIIe onset fiNer, chills, malaise
Rectal, lower back and perineal pain
Storagellld voiding WTS
Hematuria
asymptomlllic with normal
prostate on DRE
Pelvic pain, storage LUTS, ejaculatory pain, postejaculatory pain
lnmtigllions
RectaiiiDUIIl
Urine C&S: 4 specimens
Enlarged, tender, warm prostate
Colony counts in EPS and VB3
Urine C&S: 4specimens
should exceed those of initial and
VB1 [voided bladder urine): ilitial (urethra]
midstream by 10times (suggests
VB2: midstraern (bladder)
prostate as bacterial source]
EPS (eJC!li!!SSed prosta1ic secretions): {prostate] not
usually performed
VB3: post-massageiDRE (prostate)
UrineR&M
Blood CBC, C&S
Tl'1lltmllnt
Supportive measures (an!Viretics, analgesics,
stool softeners)
PO llllibiotics
1raat for
wks 1D prevent
Admission criteria: sepsis, urimry retention,
immunodeficiency
IV antibiotics {ampicillin and gentamicin) asevere
Mid-stream urine C&S at 1and 3 months post
antibiotic therapy
Avoid clllheterillllion due to risk of bacteremia llld
systemic infection
Small drainage calhBtar may be inserted a
obstruction suspected
Extended course of antibiotics
(3-4 months)
Ruoracp.linolones, TMP/SMX or
doxycydina; addition of an a-blockar
may reduce symptoms
DREwriabla
Urine C&S negative on serial specimens
Prostate biopsy (rarely performed) shows histological
inflammation
Trial of antibiotic therapy fluoroquinolone or doxycycline if
Chlamydia fnlchomtltis is suspected
a -blocker to relieve sphincter spasms, NSAIDs llld
supportive measuras for symptomatic llllillf
Epididymitis and Orchitis
Etiology
• infection:
• <35 years - gonorrhea or Chlamydia tradwmatis
• >35 years+ penetrative anal intercourse- GI organisms {esp. E. coli)
• mumps infection may involve orchitis after parotiditis
• other rare causes:
• TB
• syphilis
• granulomatous (autoimmune) in elderly men
• amiodarone (non-infectious cause, involves only head of epididymis)
• note: epididymitis is much more common than orchitis
Risk Factors
• UTI, unprotected sexual contact
• instrumentation/catheter
• reflux
• increased pressure in prostatic urethra (straining. voiding. heavy lifting) may cause reflux of
urine along vas deferens -+ sterile epididymitis
.... '
,I
If unsura b81w8an diagnosas of
epididymitis and torsion: vo to OR.
Ramambar: torsion >6 tn has poor
prognosil.
U14 Urology
......
,
•t-----------------,
Prehn'• 1ign: pain may be relieved with
elevation oftesticlel i1 epididymitis but
not in testicular 1Drsion. Poor sii1Sitivity,
e5p&ciaUy in children.
Infedioua and ln1lammatory Diseases
Toronto Notes 2011
Clinical Features
• sudden onset scrotal pain and swelling ± radiation along cord to flank
• scrotal erythema and tenderness
• fever
• storage symptoms, purulent discharge
• reactive hydrocele
Investigations
• urinalysis (pyuria), urine C&S
• ± urethral. discharge: Gialil stain/culture
• if diagnosis uncertain, must do:
• colour-flow Doppler ultrasound
• nuclear medicine scan
• examination under anesthesia
Treatment
• rule out toraion
• antibiotics:
• N. gono"heae or C. trachomatis - cefixime 400 mg PO once followed by azithromycin 1 g
single dose or doxycycline 100 mg bid x 10 days
• coliforms- broad spectrum antibiotics (Septra•, Cipro•) x 14 days
• scrotal support, ice, analgesia
Complications
• if severe -+ testicular atrophy
• 30% have persistent infertility problems
Urethritis
• common causes: infectious, inflammatory (e.g. reactive arthritis)
Tabla 7. lnfactious Urethritis: Gonococcal vs. Non-Gonococcal
Gunococc;al
Reactin Artllriti1 (furm•ly llnawn •
Clusatiw= DI'Qinillm Neisseria gononheae
Usually Chlamydia tr.Jchomatis
Diagn111il
History of sexual conlact, yellow purulent
discharge, irritcrtiva L.l1TS
Gram slain (GN diplococci}, urine PCR allll/or
culture from urethral specimen
Hirtory of sexual contact. mucoid whitish purulent
discharge, ± initaliva UJTS
Gram slain demonstrates >4 PMN/oil immersion field,
no evidence of N. gonon11eae, urine PCR ami/or culture
from urethral specimen
Cllfildme 400 mg PO DDCI orCeftrixune 125 mg
IM once AND treat for Chlamydia trachomatis
Azithrumydn 1 gPO DDCI or doxycycline 100 mg
PO bid x 7 days
Wer"• Synclrom•l
Urethritis, Uveitis ll1d Arthritis
(Cin"t pee,
188, clln"t climb a 1nlll}
Urethral Syndrome
• dysuria in females with consistently sterile urine cultures or low bacterial counts
• some have bacterial urethrocystitis (C. trachomatis or other organisms) and require
antimicrobial treatment
• treat: tetracycline or erythromycin
• rule out: vaginitis, cancer, interstitial cystitis, psychological etiologies
Toronto Notes 2011
Stone Disease
Urology U15
Stone Disease
Incidence
• prevalanceof2-3%
• male:female = 3:1, peak incidence 30-50 years of age
• recurrence rate: 10% at one year, 50% at 5 years, 60-80% lifetime
Clinical Features
• urinary obstruction -+ upstream distention -+ pain
• flank pain from renal capsular distention (non-colicky)
• severe waxing and waning pain radiating from flank to groin, testis, or tip of penis due to
stretching of collecting system or ureter (ureteral colic)
• writhing, never comfortable, nausea, vomiting, hematuria (90% microscopic), diaphoresis,
tachycardia, tachypnea
• occasionally symptoms oftrigonal irritation (frequency, urgency)
• bladder stones result in: storage and voiding LUTS, terminal hematuria, suprapubic pain
• ff fever, rule out concurrent pyelonephritis or obstruction
Differential Diagnosis of Renal Colic
• acute ureteral obstruction (other causes):
• UPJ obstruction
• sloughed papillae
• clot colic from gross hematuria
• acute abdominal crisis - biliary, bowel, pancreas, abdominal aortic aneurysm (AAA)
• gynecological- ectopic pregnancy, torsion/rupture of ovarian cyst, pelvic inflammatory disease
(PID)
• pyelonephritis (fever, chills, pyuria)
• radiculitis (Ll) -herpes zoster, nerve root compression
Location of Stones
• calyx
• may cause flank discomfort, recurrent infection or persistent hematuria
• may remain asymptomatic for years and not require treatment
• pelvis
• tend to cause obstruction at ureteropelvic junction (UPJ)
• staghom calculi (renal pelvis and one or more calyces)
• often associated with infection that will not resolve until stone is cleared
• ureter
• <5 mm diameter will pass spontaneously in 75% of patients
Stone Pathogenesis
• supersaturation of stone constituents (at appropriate temperature and pH)
• stasis, low flow and low volume of urine (dehydration)
• crystal formation and stone nidus
• loss of inhibitory factors:
• citrate (forms soluble complex with calcium)
• magnesium (forms soluble complex with oxalate)
• pyrophosphate
• Tamm-Horsfall glycoprotein
Risk Factors
• hereditary: RTA, G6PD, cystinuria, :xanthinuria, oxaluria, etc.
• dietary excess: Vitamin C, oxalate, purines, calcium
• dehydration (especially in summer months)
• sedentary lifestyle
• medications: thiazide
• UTI (with urea-splitting organisms)
• myeloproliferative disorders
• GI disorders: IBD
• hypercalcemia disorders: hyperparathyroidism, sarcoidosis, histoplasmosis, etc.
.....
,,
Ttle four narrowest passaae pointJ for
upper tract IIIDnn ara:
1. UPJ
z. Palvic brim
3. Under vas dafarantlbroad Hgamant
4.lNJ
Ul6 Urology
Stone Disease
Toronto Notes 2011
Approach to Renal Stone
--------------------------------
Urvent Intervention requirad if:
1. Solilllry kidney
2. Bilateral stones
3. lnllllctable pain or
4. Acuta renal faiure
Figura "1. Approach to Ranll Stone
,,_._, ________________
IWB
CT
Rdiollllllll
ladiolluclllt
Calcium
Uric Acid
lndinavir
Calcium
lndinavir
Struvita
Cystine
Struvita
Cystine
Uric Acid
....
.
,,
lndiemon• for •dndsahln bl huspibll:
l.lntractBIH pain
2.1nlrBctllble vomiting
3. Fever (sugglllll infection)
4. Compromised renal function
5. Singla kidney with UI&!Billl
obstructionlbilatellll obstructing
stones
....
,..,
If aptic, IJilllnl uramric mnt or
percutaneous neplns1Dmy should be
considerad.
..._,,
_._________________
lndicatiana far Pwcut.Moua
• Size >2.5 em
• Staghom
• UPJ obstruction
• Caiyl;1111l diverticulum
• Cystine stonas (poor1y friQIIIIIIlld
wilt1 ESWLJ
Investigations
• screening labs
• CBC -+ elevated WBC in presence of fever suggests infection
• electrolytes, Cr, BUN -+ to assess renal function
• urinalysis: R&M (WBCs, RBCs, crystals), C&S
• imaging
• kidneys, ureters, bladders (KUB) x-ray
• to differentiate opaque from non-opaque stones (e.g. uric acid, indinavir)
• 90% of stones are radiopaque
• crscan
• no contrast; good to distinguish radiolucent stone from soft tissue filling defect
• abdominal ultrasound
• may demonstrate stone (difficult in ureter)
• may demonstrate hydronephrosis
• IVP (not usually done)
• anatomy of urine collecting system, degree of obstruction, extravasation
• cystoscopy for suspected bladder stone
• strain all urine -+ stone analysis
• if recurrent stone formers, conduct metabolic studies
• serum electrolytes, Ca, P04> uric acid, creatinine and urea
• PTH ifhypercalcemic
• 24 hour urine x 2 for creatinine, Ca. P04> uric acid, Mg, oxalate, citrate
Treatment -Acute
• medical
• analgesic (Tylenol #3•,
DemeroJ•, morphine)± antiemetic
• NSAIDs help lower intra-ureteral pressure (e.g. Ketoralac)
• alpha-blockers: increase rate of spontaneous passage in distal ureteral stones
• ± antibiotics for UTI
• IV fluids if vomiting (note: IV fluids do NOT promote stone passage)
• interventional: if obstruction endangers patient (i.e. sepsis, renal failure)
• ureteric stent (via cystoscopy)
• percutaneous nephrostomy (image-guided)
• admit if necessary - see sidebar
Treatment - Elective
• medical
• conservative if stone <5 mm and no complications
• fluids to increase urine volume to >2 Uday (3-4 L if cystine)
• specific to stone type (Table 8)
Toronto Notes 2011
Stone Disease
Urology U17
• interventional
Bliclcyll o-IIDiian a till Tlllllnt II
UnllniS..
J. !im 2007; 1119:1183-117
•kidney
• stent if stone is 1.5-2.5 em
• extraoorporeal shockwave lithotripsy {ESWL} if stone <2.5 crn
• percutaneous nephrolithotomy if stone >2.5 em (see sidebar Ul6)
a-blockln
lilellpy.
liDs.- MBIJNE (JiruaJV 1966111 DctuiJer
• ureter
2005),111e C4clillll8 Carmi SMh lilnry, Er.tiASE
U1110
1111111u aladnlric diiiiJIIe of
llbllrldl pwmd 111111u Anrul Mallilu a1111u
An.Aaiacillliall (2002., 21Xl5)
Wife ..medfll'lillnm idlhlled in
l'llillll: 11 studin 11'1! llill:tian crD!i1
(n=l11). Ttatmllrt rqad from Bdlys ID 6Willis.
..... Giani: lnc:idlncl al dillll Lnlllll Rlnl
• ESWL is the primary modality oftreatment
• ureteroscopy (extraction or fragmentation) if
- failed ESWL
- ureteric stricture
- reasonable alternative for distall/3 of ureter
open ureterolithotomy (very rare)
• bladder
• transurethral cystolitholapaxy
• remove outflow obstruction (TURP or stricture dilatation}
1IIIUII: J.lminillrltian 11111 a-ilb:brwM!I
CGISIMiiw1llltmlli inmued incidence oftiDnl
- QIIIS8Miiw blltnwlt Ilana bv 4411
(M 1:11.31-1.51, p<0.001).
Cabiar. a-blac:lil!lhlnpr isiiDIICilled v.rith
igJilll:lnltf incmud lllH al clllll uretnl slllne
Prevention
• dietary modification:
• increase tluid (>2 L/day}, potassium intake
• reduce animal protein, oxalate, sodium, sucrose, and fructose intake
• avoid high-dose vitamin C supplements
• medications:
• thiazide diuretics for hypercalciuria
• allopurinol for hyperuricosuria
• potassium citrate for hypodtraturia
....
,'
Al1hough hypercalciuria i5 a risk fac!Dr
for stone formation. dacraasing diallry
calcium is NOT recommended 1o prevent
stone formlllion. Low dista!y calcium
IIIIIs 1o incnaasad lllCBID absorption and
higher Lilla levels of calcium OJIIIIII!I.
Table B. Stone Classification
Type of Slana
Cllci1111 [7§..15%)
Uric Acil [5-10%)
Efiolagy
Hypercalciuria
Hyparuricosuria [25% of pati8111s
with Ca stones)
Hyperoxaluria (<5% of patients)
Hypocitraturia [12% of patients)
Other causes:
• Hypomagn8S8111ia - associlll8d
with hyperoxama and
hypocitraturia
• High dietary sodium
• Decreased uril'lll'f proteins
Uric acid
in low volume, Infection with urea-splitting
acidi: urine with ahigh uric acid
organisms [Proteus, Pseudomonas.
concentnrtion:
Provid8nciB, KJebsialle.
o Hyperuricosuria alone
Mycoplasme, Satratia, S. autBUS)
o Low urimry pH, low ume volume
results in alkaline urinary pH and
(e.g. Gl water loss)
precipitation of struvit8
• Drugs (ASA, thiazides)
ammonium jhlsphata)
• Diet [pume rich red meats)
o Hyperuricosuria with hyperuricemia
o Gout
o High rate of cell tumover or cal daldh
gdemia, cytDtaxic drugs)
Autosomal recessive defect in small
bowel mucosal absorption and ranal
tubular absorption of dilasic amino
acids results in "COLA" in urine
[cystine, omithine,lysine, .-giline)
Kay faatulll
Radiopa!J!e on KUB
Rerllcing dietary calcium is NOT
an effective method of preventiol\"'
tr8irtrnent
Radiolucent on KUB
Radiopaque on CT
Acidic urine
Perpetuates UTI because stone
harbours organism
S1one and all forei!J1 bodies roost
be clecnd to avoid racurrenca
Associated with staghom calculi
Positive urine dip and cultures
Note: E. coli infection does nat
cause stnrvite stones
Aggressive stone disease seen in
children and young allllts
Recurrent stone formation, family
hi&tory
Often staghom calculi
Faintly radiopaque on KUB
Positive urine sodium nitroprusside
test. urine clr'Dnnatogrephy for
cystine
Trennent
Fluids to incn!llse urine volume
lncreesed fluid intake
Alkalinillltion of urine to pH 6.5 to 7
(bicarbonate. potassium drate)
± allopurinol
Shockwave lithotripsy not effective
Complete stone clearance
Antibiotics for 6weeks
Regular follow up urine
Increased fluid intake (3-4L of
urimt/davl
Alkalinize urine (bicarbonate,
pota&&ium citratu), Penicillaminl1/
a-MPG or Captopril (form compktx
with cystine)
Shockwave lithotripsy not effective
to >2Uday
stones: celulose
Matica/ if slons <5 mm For
pha&phate, orthoph05phate for
and no complications
absorptive causes
ProcadJrai/Sutg
For calcium oxalate stones: thiazides,
tTNtmant ifstons
± potassium citnlte, ± alopurinol
>5 mm orpresence of Calcium struvite- antibiotics (stone
complications (see U76) must be removed to treat infection)
StruYita [5-1 0%)
Cystine [1 %)
Ul8 Urology
Urological Neoplamu
Toronto Notes 2011
Urological Neoplasms
Approach to Renal Mass
..
Cystic
•
IUllnlso1.11d I
I
..
Hypoechoic
No calcification
Thin wall
Dense
Calcified
Septated
Sbip
CT*
CT
(exclude
angiomvolipoma)
Angiography
Possible
aspiration or biopJY
I
•
SUI'lllrf
..
Solid
I I
•
Surveillance
I
I
...
...
la!'llemass
(>1.5cm)
Small mass
(<1.5cm)
I
SUI'lllrf
I I
I I
Possible
surveillance
I
I
Figure I. Workup of a Renal Mass
•MRI DCCISionally pe!fonned I conlnlll corrnindit*d
Benign Renal Neoplasms
..._----------------,
Tabllra• Scl11n1U.
AuiD&omal dominant JYndrume
chnellrized by mantel retardation,
epilePJY, adenoma sebaceum •nd other
hllmar111111a.
ea- Gf Enlllrpd ICIIInep
SIIAPE
Sclerodanna
HIV nephropalhy
Amyloidosis
Polycvstic kidniiY diuas•
Endocrinopllthy' (diabeles)
RENAL CYSTS
• simple cysts
• very common - up to 50% at age 50
• usually incidental finding on abdominal imaging
• classification of cysts (i.e. simple and complex)
• Bosniak classification is used to stratify for risk of malignancy based on cyst features, see
Table 9
• polycystic kidney disease
• autosomal recessive - massive kidneys with early renal failure in children
• associated with hepatic disease
• autosomal dominant - progressive bilateral disease leading to hypertension and renal failure
• associated with hepatic cysts and cerebral aneurysms
• medullary sponge kidney
• dilatations of the collecting ducts
• usually benign course, but predispose to calcium phosphate stones
• von Hippel-Lindau syndrome
• renal cysts, cerebellar and retinal hemangioblastomas, pancreatic and epididymal cysts
• 30-40% incidence of renal cell carcinoma
Table 9. B01niak Classification of Renal Cysts
Features
Risk of Malig111ncy
Simple cyst
Round, no septalions, no calcifiCiltions,
no solid component
N99rzero
Minimally complex cyst
Thin septillion, calcifications, hyperdense on CT
Minimal
3
Con1llex cyst
ThickEr septatians, thicker and mere irregular
walls, measurable enhancement
Moderate. surgical intervention usually
necessaiY
4
Clearly malignanl
Class 3plus enhancing sllft-tissue components
Near certain
Cl11s
2
Toronto Notes 2011
Urological Neoplasms
Urology U19
Table 10. B•ign Renal Masses
Epidlllliolagy
Less than 1'!1. of alkllt renal tumours
Renal Oncocylllm1
llen1l Ad1110m1
3-7% of renal tumours. More common in males
Incidence increases with age
Found in 7-23% of all autopies
F>M
M:F=3:1
211% associill8d with tuberous sclerosis
(especially multiple, recurrent)
Dilgnasis
Clonal neoplasm consisting of fat. smooth
musde and blood vessels
May extend into 11!1181 vein and become
symptomatic
Spherical, capsLJIIllld with possible cenlnll scar
HistDiogically organized aggregates of
eosinophilic cells originating from intercalated
calls uf collecting diet
Small cortical lesions <1 em
Majority are solitary but can be multifocal
Histologically organized cells with no atypia which may
exhibit bisornv of chromosomes 7 and 11
R:idml diagnosis
Negative attenuation {-ZO HU) on CT is
pathognomonic
Rare presentation of hematuria, flank pain
and palpable mass (same as RCC)
lncidml finding on CT although difficult to
distinguish from RCC
Biopsy may be performed to rule out malignancy
lncidml finding on CT
Rarely syrl1llomatic
Controversy as tD whelher this represents benign or
preofllalignant neoplasm
Benign course although excision warranted if
inCillllsad risk uf rupture and retroperitoneal
bleed (large size, pregnancy, previous bleed)
Follow with serial UIS
PartiaVradical nephrectomy for large masses
High intensity focused ultrasound (HIFU) or
radiufrequency ablation (RFA) for smeller
masses
PartiaVradical nephrectornv if mass >3cm lkla tD
increased risk of mlll8stllsis
Malignant Renal Neoplasms
RENAL ADENOCARCINOMA [Renal Cell Carcinoma (RCC)]
Etiology
• cause unknown
• originates from proximal convoluted tubule epithelial cells
• risk factors: smoking (results in 2x increased relative risk), cadmium exposure, employment in
leather industry
• familial incidence seen with von Hippel-Lindau syndrome
Epidemiology
• eighth most common malignancy (accounts for 3% of all newly diagnosed cancers)
• 85% ofprimary malignant tumours in kidney
• male:female = 3:1
• peak incidence at 50-60 years of age
Pathology
• histological subtypes: clear, granular, spindle cell, papillary, chromophobe
Clinical Features
• usually asymptomatic- frequently diagnosed incidentally by U/S or CT
• poor prognostic indicators: weight loss, weakness, anemia, bone pain
• local effects: classic "too late triad" found in 10-15%:
• gross hematuria 50%
• flank pain <50%
• palpable mass <30%
• was called the "internist's tumour" because of paraneoplastic symptomatology, now called the
•radiologist's tumour· because of incidental diagnosis imaging
• systemic effects: paraneoplastic syndromes (10-40% ofpatients)
• hematopoietic disturbances: anemia, polycythemia, raised ESR
• endocrinopathies: hypercalcemia (increased vitamin D hydroxylation), erythrocytosis
(increased erythropoietin), hypertension (increased renin), production of other hormones
(prolactin, gonadotropins, TSH, insulin and cortisol)
• hepatic cell dysfunction - "Stauffer's syndrome": abnormal liver function tests, decreased
WBC count, fever, areas ofhepatic necrosis; no evidence of metastases; reversible following
removal ofprimary tumour
• hemodynamic alterations: systolic hypertension (due to AV shunting), peripheral edema
(due to caval obstruction)
• metastases: seen in 15% of new cases
• bone, brain, lung and liver most common sites
Investigations
• routine labs fur paraneoplastic syndromes (CBC, ESR, LFTs)
• urinalysis (60-75% have hematuria)
• renal ultrasound (solid vs. cystic lesion)
• CT scan (to distinguish solid vs. cystic lesion and to determine extent and operability)
• IVP (mass lesion): no longer routinely done
• angiography: no longer routinely done
... , ,
rumour may invade ranal vaint and
inferior vana
(may mull in
IICiiBI, hllpetic dysfunction, right lllrilll
tumour, and pulmonary .-nbolil.
U20 Urology
Urological Neoplamu
1'oroDio
2011
Methods of Spread
• direct. venous, lymphatic
Staging
• Involves cr, cheat .x-ray.liver euzymes and functions, bone &can
Table 11. 111M Clllllflcatlon of Renal Adellocarclnoma
T
N
M
Tl ; tllnOW' <1 em. cedined to P8l1ll pnnchyma
l1s; <4em
T1b: 4-7 em
NO: na regional nadas
Ml: na evidence af IIIBIIIIalis
TZ: limDUr >7 em. cadinad to ranal p111111chyma
T3: tllnOW' axl8nds no Dlljor vails or achnal.
but nat bawand GIJDilis fla:ia
T3a: itto arRI1fll cr sills fat
T3b: irto rellllll VIii or infnllillphlli!JIIIIic IVC
13c: illo supradillphl'llfllllic IVC
Figure 9. RCC Stegi1g
N1: IIIBIIIIalii1D 8
<Zem
node,
M1: pra8IIIC8 af liltlm 11181881111il
NZ: IIIBIIIIalii1D 8
node
bll\W8tll Zand 5em cr miAtipla
nadas <Zem
Nl: nada >5 em
T4: limDUr 8ld8ndl ba'jOIII Gllllla's fiiiCil
Treatment
• surgical:
• radical nephrectomy: en bloc removal of kidney, tumour, .ipsilateral adrenal gland (in upper
pole tumours) and intact Gerota's capsule md paraaortic lymphadenectomy
• partial nephrectomy: <4 em tumour or solitary kidney/bilateral tumours
• surgical removal ofsolitary metastasjs may be considered
• radiation for palliation - painful bony lesiona
• chemotherapy: NOT effi:ctive
• advanced stage:
• anti-angiogenesis (anti-VEGF)
• anti-tyrosine kinase: sunit:inib
• anti-ll.2: dacllzwnab (Zenapu-)
Prognosis
• stage at diagnosis is the most important predictor of survival:
• T 1 - 5-yeauurvival is 90-10096
• T2-T3 - 5-year survival is approximately 6096
• 5-year survival of patients presenting with metastasis is 0-2096
Carcinoma of the Renal Pelvis and Ureter
Epidemiology
• rare. a.ccounb for 496 ofall urothclial cancers
• frequently multifocal, 2-596 are bilateral
• M:F=3:1
• relative lncldence- bladder:renal:ureter = 100:10:1
RJ:CII-...-d
&rgery is 1ha only lllflctivl inlllwnti111
fur RCC; chllmDihlrapy i1 NOT uRIU.
.... ,
lliffllltlllilll DillgHIIIil of Aling Dafllct
• lkD1halial ctll cninal'lll (diffa1111i118
and CT an)
• Uric acid lllllnl (dlfallll'llilllll viii
cytology and CT sctn)
• Blaod clat
• l'lpll.., niCilllil
•
• GBJ Wlbl1 from 1111 pruduc;ing
orgllli11111
Pathology
• papillary urothelial cell carcinoma (UCC); 8596 (othen include squamous cell. adenocarcinoma)
• UCC of kidney md ureter are histologically similar to bladder UCC
Risk Factors
• smoking
• chemical exposure (industrial dyes and solvents)
• ll!lalgesic abuse (acetaminophen, ASA, and phenacetin)
• Balkan nephropathy (chronic interstitial nephropathy in countries such as Serbia, Montenegro.
Romania. Bulgaria)
Clinical Features
• gross pe.inle&s hemeturila (70-9096 of patients)
• microsoopic hematuria
• flank pain
• dysuria
• flank mass caused by tumour or associated hydronephrosis (10-2096 of patients)
Investigations
• cystoscopy and retrograde pyelogram: CT scan, radiolucent filling defect on IVP/CT urogram
Treatment
• radical ureteronephrectomy with cuff of bladder
• dlstal ureterectomy for dlstal ureteral tumours
Toronto Notes 2011
Urology U21
Urological Neoplasms
Bladder Carcinoma
Etiology
• unknown, but exposure to environmental and occupational carcinogens plays a role
• risk factors:
• smoking (main factor- implicated in 60% of new cases)
• chemicals: naphthylamines, benzidine, tryptophan, phenacetin metabolites
• cyclophosphamide
• prior history of radiation treatment to the pelvis
• Schistosoma hematobium infection (associated with SCC)
• chronic irritation: cystitis, chronic catheterization, bladder stones, (associated with SCC)
Epidemiology
• 2nd most common urological malignancy
• male:female = 3:1, white:black = 4:1
• mean age at diagnosis is 65 years
Pathology
• classification:
• urothelial cell carcinoma (UCC) >90%
• squamous cell carcinoma (SCC) 5-7%
• adenocarcinoma I%
• others <I%
• stages of urothelial cell carcinoma at diagnosis:
• superficial papillary (75%) -+ >80% overall survival
• 15% ofthese will progress to invasive UCC
• the majority of these patients will have recurrence
• invasive (25%} -+ 50-60% 5-year survival
• 85% have no prior history of superficial UCC (i.e. de novo)
• 15% have occult metastases at diagnosis -lymph nodes, lung, peritoneum, liver
• carcinoma in situ-+ flat, non-papillary erythematous lesion characterized by d)'liplasia confined
to urothelium
• more aggressive, poorer prognosis
• usually multifocal
• may progress to invasive UCC
Clinical Features
• hematuria (key symptom: 85-90% at the time of diagnosis)
• pain (50%)
• clot retention (17%)
• asymptomatic (20%)
• storage urinary symptoms - consider carcinoma in situ
• palpable mass on bimanual exam -+ likely muscle invasion
• obstruction of ureters -+ hydronephrosis and uremia (nausea, vomiting and diarrhea)
• metastases
• hepatomegaly, lymphadenopathy, bone lesions
• lower extremity lymphedema if local advancement or lymphatic spread
Investigations
• urinalysis, urine C&S, urine cytology
• ultrasound
• CT scan with contrast or intravenous pyelogram (IVP) -+ look for filling defect
• C}'litoscopy with bladder washings (gold standard)
• biopsy to establish diagnosis and to determine depth of penetration (although cold punch
biopsy can be transurethral. resection is standard)
• new advances with specific bladder tumour markers (e.g. NMP-22, BTA, Immunocyt, FDP)
Grading
• Grade 1: well-differentiated (10% invasive)
• Grade 2: moderately differentiated (50% invasive)
• Grade 3: poorly differentiated (80% invasive)
Staging
• for invasive disease: CT or MRI, chest x-ray, liver function tests (metastatic work-up)
',,
The "field d81act"tlleory helps to explain
why UCC has multiple lesions and
has I high rec1J111111Ce rata. The antira
uruthalium [ptlvis to bladder) il bath8d
in can:inogens.
U22 Urology
Urological Neoplamu
1'oroDio
2011
Tebl11112. DIM Clestificmun uf Bladd•
T
N
M
Tt: mnirrvasive papililwy Cll'tftlma
N slalus: as fllr 11!11111 cell carcdlma
M status: ulur renal eel carciloma
T11: caciloma ilsitu !CIS); flatlllnull'
Tl: 1111111111' iiMidas &Ubmucau,/IIIID prapria
'121: 111rncu iiMidas superficial mu&dll
T2b: 111mu inwdes deep IIIIIIZ
T3: 1111111111' iiMidBS ptrivesical fal
T41: q.cent 11g111 ilwlv1lnant; prasteta,
Ullnls arVIIIJinll
T4b: lldjlced argan invalvamant; pelvic Will
II' Bbdlri& wall
PalvicWIIIor
Abdominal Will
Fnltlat8
I
I
..
]§
0
F"1111•r• 10. Urutllaill Call Clln:inoma Gf Bladdar
Treatment
• superfida.l (non muscle invas1ve) disease: Tis, Ta, Tl
• transurethral resection ofbladder tumour (TURBT) ± &lDgle dose or maintenance
intnwesical chemo/immuno-therapy (e.g. BCG, mitomycin C) to decrease recurrence rate
• high grade disease - TURBT + lilllinlx:nance BCG OR cystectomy in select patients
• invasive disease: T2a, T2b, T3
• radical cystectomy + pelvic lymphadenectomy with urinary divezsion (e.g. lleoconduit
Figure II) or irradiation for small tumours
• advanced/metastatic disease: T4a, T4b, N+, M+
• initial combmatlon systemlc chemotherapy ± Irradiation ± surgery
Prognosis
• depends on
size, number oflesions, recurrence and presence of CIS:
• stage Tl- 90% at 5 years
• stage T2 - 55%
f"llglr& 11.1JeGCOndUit
• stage T3 - 2096
• stage T41N+IM+ - <5%
Prostatic Carcinoma (CaP)
Etiology
• notknown
• risk factors
• increased inddence in persons of African descent
• famlly history
• 1st degree relative = 2xrisk
• 1st and 2nd degree relatives = 9x risk
• high dietary fat increases risk by 2x
• cJgarette smoking
Epidemiology
• most prevalent cancer in males
• third leading cause of mole cancer deaths (following lung and colon)
• lifetime risk of a SO y.o. man for CaP is 5096, and risk of death from CaP is 3%
• 75% diagnosed between ages of 60 and 85 and mean age at diagnosis is 72
Toronto Notes 2011
Urological Neoplasms
',
Pathology
.... •t-----------------,
• adenocarcinoma
• >95%
• often multifocal
• urothelial cell carcinoma (4.5%)
• associated with UCC of bladder
• not hormone-responsive
• endometrial (rare)
• carcinoma of the utricle
DHJ.rentill DilgJMil of 1 Proltltic
Nodule
• l'nlstm cane• {30%)
• Benign prostatic hypurplaia
•
•
•
•
Anatomy (see Figure 6)
• 60-70% ofnodules arise in the peripheral zone
• 10-20% arise in the transition zone
• 5-10% arise in the central zone
Clinical Features
• usually asymptomatic
• most commonly detected by DRE, elevated PSA, or as an incidental finding on transurethral
resection of the prostate (TURP)
• DRE: hard irregular nodule or diffuse dense induration involving one or both lobes
• PSA: see Prostate Specific Antigl!n, U24
• locally advanced disease:
• storage and voiding LUTS (uncommon without spread)
• suspect with LUTS, incontinence ± back pain
• metastatic disease:
• bony metastasis to axial skeleton is very common (osteoblastic)
• visceral metastasis is less common with liver, lung and adrenal metastases occurring most
frequently
• leg pain and edema with nodal metastasis obstructing lymphatic and venous drainage
Methods of Spread
• local invasion
• lymphatic spread to regional nodes
• obturator > iliac > presacrallpara-aortic
• hematogenous dissemination occurs early
,.._I'IMience GIJNUSI* CA
blulll: Study MS cloeed emtv as olijectiues were
nwt. lb&ra-1 MAIIIIMI TldL£1ian (P<0.001)
in prM1111:1 rl pnllllll CA in 1111 filu1lrill gnllf
[18\ incidallctl COITptlld 1D pllcllllo p t [24ll.
inciclanca], but 1r1 ilcrnsa i11111 proporb al
lhose
Glide tuncus !Gleason score 1-101
N
M
M: distant metastasis
T2: palpable, confined ID prostate
T2a: tumour involving less than
alobe
T2b: tumour involving less than or equal to 1 lobe
T2c: tumour involving bath lobes
M1a: nonregionallymph nodes
M1b: bone(s]
M1c: lither site(sl with or
without bona disease
plecebol. The njorityal11mlurs in bath graups
118\lwera
bcdz8d di181M(T1 11 T2).
The firasleride group •lso lad a sigliicdy higher
inciclanca ai1111UII
swmpiDms 'dlll11111 pliabo graup.
Cancbioll: MIIIIIMII 55 who took filllllaride for
7\'IIIIW8nl 25\lals lblv1D dMop pniSIIt8
CA
1otbu plaeebotJQUP. h_.'dla
t:IIIC8IS ilthlfinllllridl grDUpWINaf I higi.Qlllll.
.....
,•t-----------------,
,
Co•idtntiona In lnt.rprdn1
Prostata Biopsy Renlts
• GI8QOn ISCOI'll6 for two moe!:
prN!minant patmms ar. l"'ported
{e.g. 3+4 = Gleason sum
Nota: 4+2 not equal to 3+3 despite
equivalent Gleason sum)
• Billlbnl "'·
...... itvolvement
• %of core and number of cores
involved
T3: tumour extEnds through prostate Cl!pSule
T31: IIX!nlcapsular IIXIIInsion (unilateral or bilatel'lll]
T3b: tumour invadng sami1111l vesicle(s]
T4: tumour invades adjacent structures (besides seminal vesicles]
Table 14. Prostate Cancer MDrtality Risk
GIBuon Score
S1llly: Alll'lllanimd,
plabo·
caolraled IM!dy designed Ill del2mine l'lllelber
tJultmart witli mllllarida Cldd IIIla lila
]R'IIIIence II prostm CA during 1711111 period.
,..._ 11.882lTII!Iv.illl . . . . rilkalpniSIItl
CA (55 YIIJIIIIIQI 11 oldlt AtriCIII-Anwican,
or 11st d'fBI relllive hlwi1Q pniSIIt8 CAl witli
11'1111TT111 ORE and 1 PSA IMI rl g 111tniWIN
17-,..r period.
N: spread ID 11!1jianal
T1: dinically undetectable
normal ORE and TilUS
T1a: tumour incidiiiTIBI histologic findilg in < 5% of tissue res!!Cted lymph nodes
T1 b: tumour incidental histologic findilg in > 5% of tissue resected
nc: tumour identified by neelle biopsy (because of elevated PSA
IMII; tumours found in 1or bath lobes by needle biopsy but nat
palpable or l'llliably visible by imaging
Stage
n.l'rlllllll c-l'nlnnllllll 1111 tiV1l
NUf 21103; 349:21&-224
Finllllrid1 (51TO"dly) vs. piiCiba
Tabla 13. Staging of PrDitate Cancer (TNM 2002)
PSA
Efllct rl Sllftun IIIII Villlllil E• lilt
all'lallllllc-ud .... c-n.
S.lnm IIIII Vlllmil ECa.-l'llldln Trill
(SB£CT)
lippnwl SM, Kltil EA et al..IA.WI2009;
301(1):39-51
llllllldr. Rlndomilld, pB:.bo canlrallid 1rillwitll
35,5331TIIII
\'Onin E.l8ilrliL111
+villmin E, or pllcebo.
c.t•ian: Sllaniln Dlvillmin E, IIana Ill in
combinltian lithe dalllllld f1lnriMDns lllld.
cill nat pmant pniSIIt8 elncl' in lllis pilldltion al
Nlltiwly haallhy 111811.
lhin
DRE
PSA elevated in the majority of patients with CaP
transrectal ultrasound (TRUS) -+ size and local staging
TRUS-guidedneedle biopsy
bone scan may be omitted in untreated CaP with PSA < 10 ng/ml
CT scanning to assess metastases
T
l'nlstatitis
l'nlstatic infarct
l'nllllllic: calculus
Tuben:ulous prostatitis
Qlled. t2'J.v.lli1e.
Investigations
•
•
•
•
•
•
Urology U23
Low Rilk
Madlll'lllt lhk
[if any of fallowing)
High Rilk
[if any of fuiiDWi1g)
<10
10-20
>20
<7
7
8-10
pT1-2a
pT2b-T2c
pT3/4
U24 Urology
Urological Neoplamu
Wi:ll ,......,_WIIr:WWiiliq
il Early,....... c..
NEJM m; 352:1 m-84.
.....: To dellnnina whether aut, lldical
praslllldDmy improved 1118 llniwl in lTIIII with
11011-invlliw pnllllta CIIICir II compnd ID
.
695 lllmWIIIPI1JIIIeeM.
111rolld iam 14 CIJ'ils lll1lllld Swldlll.linllad
bllwlln 1989ltld 199!.1ncmian
criteri• incUd8d being undlr lila of 75, n!JMt
......,....lliln:
diiQIIOMd
pn1111ta
CIIIC8t sllg8 T2 or lels.l'ltholagr hiiiiiD show
Ilk allllldnlltt or
llmlur.
l'ltialb W8A1 rlnllolriy lllignad 011811:1 bail ID
llillltr en iiiiiiMnlion grnup {TIIicll proslllaCIDmy)
or r:an1RA
Wliling). The PriniiV llllpoint
rl1he study was IMmll lTIGitJity u ID p!IJIIIts
C111C8t with IICDIIdlty 1ndpaia lllkln ID be local
prl9lllian and dilllnt 1111111111111. ADiiyliiWIS
perflmnld on 111 inllniiiHD-trllt belil.
The
lelltNe risk IRR) rllocll protpeSiion •nd dislllnl
llllllslllsll for 1118 inlllvmion
0.33
{p<O.OOllltld D.OO {p<O.DliiiiPiclivlly, II
compnd 1D 1118 COIIIJol Qroup. The Nlllivl risk II
derrtll d11111D poe11t1 CII1C8r in lila irrbrMnliorr
c:..:u-llrldicel ptOSIIIIcbrmy retb:el1he
risk rl dlltlr clJ11Dprillllll Cllll*' in 111111 with
11011-invlliw, WIIIID rnodllllaly dilllnrnlilfld
Ullourt, • compll8d ID Wlldrlul Wliq. The
lelltNe risk rl bodllocll iiiVISiorr 111d 1he spread
rldillld111111S1111s-dsolianificarrlti
decnued with lilly lldicll prostaiiCtDrTiy
Toronto Notes 2011
Treatment
• Tl (small well-differentiated CaP are associated with slow growth rate)
• if young consider radical prostatectomy, brachytherapy or radiation
• follow in older population {cancer death rate up to 10%)
·T2
• radical prostatectomy or radiation (70-85% survival at 10 years) or brachytherapy
• T3, T4
• staging lymphadenectomy and radiation or hormonal treatment
• N >0 or M >0 (see Common Medications, U43)
• requires hormonal therapy/palliative radiotherapy for metastases
• bilateral orchiectomy- removes 90% of testosterone
• GnRH agonists [e.g.leuprolide (Lupron• or Eligard•), goserelin (Zolada-)]
• estrogens [e.g. diethylstilbestrol (DES)]
• antiandrogens [bicalutamide (Casodcx•)]
• local irradiation of painful secondaries or half-body irradiation
• chemotherapy regimens that include docetaxel may improve survival in advanced prostate
cancer that is no longer responsive to hormone therapy
Table 15. Treatment Options for Localized Prostate Cancer
Wlll:hful Waiting
(Active Surveillance)
Low grade cisease or short life expecllllcy
( <5-10 y); good follow-(Jp
Disease pragression
81'1ChythM'IpJ
Low volume, low PSA (< 10), low grade
Erectile dyshr.ction (5D%),? long term effectiveness
ExtamaiB_.
Locally advanced disease, older patients
Radiation practitis (S'lf.), erectile dysfunction (51l%), risk
of rectal cancer
Young patients (<65 y), hilt! grade disease
Incontinence (11l%), erectile dysfunction (3D-51l%)
Tharapy
• Otlrar options includl
high irt1n1ity foms11 '*n!IOUnd {HIFll), hormonlllllllltion
Prognosis
• stage T 1-T2: excellent, comparable with normal life expectancy
• stage T3-T4: 40-70% survival at 10 years
• stage N+ and/or M+: 40% survival at 5 years
• prognostic factors: tumour stage, tumour grade, PSA value, PSA doubling time
Prostate Specific Antigen (PSA)
• enzyme produced by epithelial cells of prostate gland to liquify the ejaculate
• leaks into circulation and is present at <4 ng/mL
• measured total serum PSA is a combination of free (unbound) PSA ( 15%) and compl.exed PSA (85%)
It'
In PSA testing, tlink "free and auy":
increased free/total nrtio suggeslli
b111ign cauu of high PSA.
,,.,
c - ot lnt:r11uad PSA
BPH, pnnibditis,
i&ehsmirl/
infarction. acute urinary retention,
Pf1)5lllhl biopsy/allgflfY, prolllrtic;
masua-. urllh111l c:am...rimtion, TRUS,
111nal faiiU111,
bypass Ql1lft..
radia1ion therapy; a normal DRE does
NOT significantly llrnll1 PSA.
Screening Prostate Cancer: PSA and ORE
AUA Best Practice Statement, 2009 Update
• PSA may be elevated in prostate cancer and many other conditions; it is not specific to prostate
cancer
• currently mixed evidence concerning effect of PSA screening on mortality (ERSPC and PLCO
trials - see sidebar)
• population-based, routine screening not recommended
• must discuss risk factors, test characteristics, risk of over-detection and over-treatment,
treatment and active surveillance options
• well-informed patients can elect to undergo PSA test and DRE
• the decision to proceed to prostate biopsy should be based primarily on PSA and DRE results,
but should take into account multiple factors (free and total PSA, patient age, PSA velocity, PSA
density, family history, ethnicity, prior biopsy history and comorbidities)
Strategies to Increase Specificity of PSA
• age-related cut-off values
Table 16. Nonnal PSA Value by Aga Group
Serum PSA Concentndian {IIJ'l)
411-49
<2.5
50-59
<3.5
60-li9
<4.5
70-79
<6.5
JE st al..li1AM 1193; 270{71:86()..4.
Toronto Notes 2011
Urological Neoplasms
• free-to-total PSA ratio:
• complexed PSA increases in prostate cancer, decreasing the percentage of the free fraction
• <10% free PSA suggestive of cancer, >20% free suggests benign cause
• PSA velocity:
• change of>0.75 nglmUyear associated with increased risk of cancer
• PSA density:
• PSA divided by prostate volume as found on TRUS
• >0.15 nglmUg associated with increased risk of cancer
Other Uses for PSA (AUA Bast Practice Statement, 2009 Update)
• therapeutic decision making: patients with serum PSA levels <10.0 nglmL are most likely to
respond to local therapy
• work-up: bone scans are generally not necessary in patients with newly diagnosed prostate
cancer who have a PSA <20.0 nglmL unless the history or clinical examination suggests bony
involvement
• disease monitoring: serum PSA should fall to a low level following radiation therapy, high
intensity focused ultrasound and cryotherapy and should not rise on successive occasions. PSA
should remain undetectable following radical prostatectomy
• outcome prediction: in patients with metastatic disease receiving androgen suppression
therapy, failure to achieve a PSA nadir of <4.0 nglmL seven months after initiation of therapy is
associated with a very poor prognosis (median survival: one year)
Testicular Tumours
Etiology (Risk Facton)
• cryptorchidism, atrophy, sex hormones, HIV infection, infertility
• family history; personal history of testis cancer
Epidemiology
• rare, but most common in young adults (17-37 years of age)
• high cure rate
• any solid testicular mass in young patient - must rule out malignancy
• slightly more common in right testis (corresponds with slightly higher incidence of right-sided
cryptorchidism)
• 2-3% bilateral (simultaneously or successively)
Pathology
• primary:
• 1% of all malignancies in males
• most common solid malignancy in males aged 15-34 years
• undescended testicle has increased risk (10-40:x) of malignancy
• 95% are germ cell tumours (all are malignant)
• seminoma (35%) classic, anaplastic, spermatocytic
• nonseminomatous germ cell tumours (NSGCT)
embryonal cell carcinoma (20%),
teratoma (5%), choriocarcinoma (<1 %), yolk sac («1%), mixed cell type (40%)
• 5% are non-germ cell tumours (usually benign)
(testosterone, precocious
puberty), Sertoli (gynecomastia, decreased libido)
• secondary:
• male >50 years of age
• usually a lymphoma
• metastases (e.g. lung. prostate, GI)
Clinical Features
•
•
•
•
•
•
•
•
•
•
painless testicular enlargement (painful if intratesticular hemorrhage or infarction)
firm, non-tender mass
dull heavy ache in lower abdomen, anal area or scrotum
associated hydrocele in 10%
coincidental trauma in 10%
infertility (rarely presenting complaint)
gynecomastia due to secretory tumour effects
metastatic disease related back pain
supraclavicular and inguinal nodes
abdominal mass (retroperitoneal lymph node metastases)
Urology U25
.......
lullllllizlll bnpunlludy
NEJM2001; 3611:13211-8
.....: To detamina 1111 lfficlcy of prollllaspdic dg8n ll'SAiscraaq ill impi'Mig
Mllllllftivll in
........,..!dan:
1821611
IIQI!d SG-74
were remilldbltwelll1994- Z!l04 m
prDIIltS CIIICIIr.
patients
E!JropB counlrin 111d p!IIIIICtiwly mild and
IIIMimniltd llllilhlr 1
ar cantral group.
Scr.ning conlind of a PSA 1M talren MY 4
Y8ll1 {i
llld cut-dlfor bicl!liY was at
3ri;Pri TllliMnt rl conlimld i)RIIIIII
was laft1o the guidlines rlaldi courty. The
prin'llry anll-poirt was IMII1111101111ity. 11111(zad on
Ill iniiOOon-1o-SCRIIn IIIIis.
11116: Median fliiMo\QJ time WIS 9yem, and
1lle incidence rl prostate Clf1Cel ill the sa-eerilq
Pf was8.2\n. l8'l. in ill canlrDI
ThalliiiiM risk al dllth il
llfliUP
n. canlrDiwu 0.80 IP<D.15I. The lllltiiiD ria
IVClJclionwas0.71
group, trnslB; lila
needed to
sa.n r/1410 IIIII a rurlie! 11l8dld 1o 11111 r/48.
c:.I1111Dnl: T1'11111of PSAsa.ningwullill
1D !Xdarallillive riskllllb:tion aiM1ollllll
rl50 at 74 {MbthiiTlljority
rl benefit se111 in m111 aged SG-611.
1lle increaled rill ridilgllllil was spcdf
iiCflllld in
group, ltld clii1D the
ildolad CUll afmany prDIIltS Clnalll, !hill flct
nut be lliren irQ considlndion. Fur1her Wjy
is Wlll3llled 11 examine 1lle aptimll
llml ofPSA
Uldttnsholds
1D 1*11fon!ll1111 the optimall1llfllff 1D IHIICI
thlrisbri!MIIdilgnlllilandllllJCIIdprDIIltll
c:m:ur nutD!y.
.._n
', ,
On:ltiapoy
SurgiCIII dNC:unt (orchiopexy) of
undescended testis does nat reduce
the rill!: of mlllignlllncy. It can however,
r.duc1 the rilk of infertility lllld
physical axarn.
U26 Urology
.
..,., ,
.-----------------,
Testlll nl acroblm hlva
lymphlllic drain11Q8, lllenlfore
1rans-scrotalllppi'08ch for biopsy or
orchieciDmy shoolei be avoided.
..,., ,
..-----------------·
AorU is •11111 Left: Lsft testicle drains
iniD the pr. and pnaortic nodes.
IVC ie on thlllight: Right testicle
draits in to the IJII111CIMIII nod11.
..,., ,
.-----------------,
.
SUging
Clinical- CXR
metatases),
mllbrs for staging
AFP. LDH),
CT abdomenfpelvis
lymphadenoplllhy)
• Stage 1: disease limited to testis,
epididymis or lji&ITTIIIlic cord
• Stage II: diseasa limited to the
rvtroperitoneld nodn
• Stage Ill: diuase m.tutlltic to
supradiaptngmatic: nodal or visceral
Urological Neoplamu
Methods of Spread
• local spread follows lymphatics:
• right -+ medial, paracaval, anterior and lateral nodes
• left -+ left lateral and anterior paraaortic nodes
• "cross-over" metastases from right to left are fairly common, but they have not been reported
from left to right
• hematogenous most commonly to lung, liver, bones and kidney
Investigations
• diagnosis is established by railical inguinal orchidectomy
• tumour markers:
• beta-hCG and AFP are positive in 85% of non-seminomatous tumours
• pre-orchidectomy elevated marker levels return to normal post-operatively if no secondaries
• beta-hCG positive in 7% of seminomas, AFP never elevated with seminoma
• testicular ultrasound {hypoechok area within tunica albuginea =high suspicion oftesticular cancer)
• evidence of testicular microlithiasis is not a risk factor fur testicular cancer
• needle aspiration contraindicated
Management
• orchiectomy for all stages
• adjuvant therapies as per Figure 12
Tentoma
Embryonal CA
Germinal cell
.
.-----------------,
RPLIIIP can ba perform ad in a niiVI
sparing fashion, preserving niMII of
the hypogestric plaxus to maintain
antegl"lde ejaculation.
Mixed cell type
Yolk sac CA
l'lthologic {Ill orchiectomy)
• T1 :tumour confined to tosli$ and
epididymis, no vascui.-Jlymphl.tic:
illllll$ion
• T2: tumour extends beyond tunica
albuginea or vascular/lymphatic
illllll$ion
• T3: tumour involves spermatic cord
• T4: blmour invadll scrorum
• T4a: tumour invlldes spermatic cord
• T4b: tumour invedes acrollll WilD
... , ,
Toronto Notes 2011
Epithulium
Chorio CA
90%
Staga I
Surveillance
10%
40%
20%
20%
Staga 11+111
Staga I
Stage II
Staga II
./
./
./
Ralialion
RPI.JIID•
Chemothlnpy
±
?
./
./
./(residual mass)
./
./
Figura 12. Management of Tll'licular Cancer
1
APLND = retruperilmeai-IIXIe dillectiln Adapted from Dr. MAS Jewett
Prognosis
• 99% cured with stage I, stage ll disease
• 70-80% complete remission with advanced disease
Penile Tumours
• rare (<1% of cancer in males in U.S.), most common in 6th decade
Benign
• cyst, hemangioma, nevus, papilloma
Pre-malignant
• balanitis xerotica obliterans, leukoplakia, Buschke-Lowenstein tumour (large condyloma)
Pre-invasive Cancer
• carcinoma in situ (CIS):
• Bowen's disease -+ crusted, red plaques on the shaft
• erythroplasia of Queyrat -+ velvet red, ulcerated plaques on the glans
• treatment options: local excis.ion, laser, radiation, topical5-fluorouracil
Malignant
• risk factors:
• chronic inflammatory disease
• STI
• phimosis
• uncircumcised penis
• 2% of all urogenital cancers
• squamous cell (>95%), basal cell, melanoma, Paget's disease ofthe penis (extremely rare)
• definitive diagnosis requires full thickness biopsy oflesion
Toronto Notes 2011
Urological Neoplasms/Scrotal Mlllll
Urology U27
Table 17. TNM Staging for Penile Carcinoma
T
N
M
Tx: prinary 1ll1l0ur can nat be assessed
N1: metastasis in a single superficial,
node
M: presence {+I or absence (01 of
distant metastasis (lung. liver, bone,
brainI
TO: no evidence of primary tumour
T.: CIS
N2: melil&lil5is in
or bilahral
superficial lymph nodes
Ta: non-iiMISive carciloma
N3: metastasis in deep inguinal or pelvic
lymph noda(sl unilateral
T1: tumour invades subspithelial coniiiCiive
tissue (Buck's and lla1Ds fascial
T2: tumour invades carpus
cavemosurn (throu!ll tunica albugineaI
or
T3: tumour invades urethra or prostate
T4: tumour invades D1her adjacent structures
• lymphatic spread (superficial/deep inguinal nodes-+ iliac nodes) »hematogenous
Treatment
• wide surgical excision with tumour-free margins (dependent on extent and area of penile
involvement) ± lymphadenectomy
Scrotal Mass
• see Common Presenting Problems, U3
Tabla 1B. Differentiating batwaan Scrotal Mauas
Di&renti.. gf a Benign krvtal MIIR
Condition
Pain
Pllpalian
Tol'lion
+
Diffuse tenderness
+
+
+
Epididymal tenderness
Present cremaster reflex, positive Prehn's sign
Diffuse tenderness
PrasiJTI: cremaster reflex. positive Prehn's sign
Epididymitia
On:hitis
H1111atocllla
Additional Findnp
Absent cremaster reflex. negative Prehn's siiJI,
EMERGENCY!
Diffuse tenderness
No transillumillltion
HydiiiCIII
Testis not separable from
hydrocele, cord palpable
Transilumination
SparmlltDcela
Testis separable from
spermatocele, cord palpable
Transilumination
Bagofwonns
No transillumillltion
Testis separable from hernia, cord
nat palpable, cou!ll impulse may
transmit, may be reducible
No transillummon
lllricoclll
lndn=ct lnguilal
- (+ htnmgulatedl
Tumaur
- (+ hemorrhagicI Hard lump/nodule
HIS IllS
llydrucale
Infection
Sperm {spermatocele I
llaod {hlmlltacll•l
lnlllslirm (hamial
TDI'Iion
lome veins lvaricocelel
Idiopathic:
....
,·}-----------------,
,
Vuic:ec:ale Gl'lldilg
Grade 1: l'lllpeblti only with valsalva
manaevre
Grade 2: Palpable without VIIIIIIIVII
Grade 3: Visible through scrotal skin
....
,·}-----------------,
,
lndicllions for Tl'8ltnlent vf
Vuic:ec:ale
• Impaired sparm
or qullllity
• Pail or dulache llffectinv
of
life
• Affected testis fails to grow in
lldalascants
• Cosm.tic indications (especially in
lldalascantsl
U28 Urology
Scrotal Mass
Toronto Notes 2011
Table 19. Benign Scrotal Masses
Type
Vlricocele
Sp•IIIIIDc:lla
Hv*acell
Dllilitian
Diatatian and toltuosity
of
piiiXU&
A benign, sperm filled
epididymal rBtention cyst
Twisting of the testicle
Protrusion of abdominal
Collection of serous fluid
contenlli through the inguinal
that resulbi tom a dsf8ct or causilg wnous occlusion
irritation in the tunica vaginalis and engorgement as well as
canal into the scrotum
artaial ischemia and irllrction
Etiolagy
• 10%ofmen
• Due to incorJ1)elent valves
in the testicular vains
• 90% left sided
Wtiple theories, ncluding:
• Distal obstruction
• Aranysmal dilations of the
epididymis
• Agglutinal!d genn cells
• Usually idioplllhic
• Found in 5-111% testicular
tumOUIS
• Associated with traLIIII!/
infection
• Communicatilg: patent
processus vaginalis,
changas size during day
(peds)
• Non-communicating: nonpatent processus vaginal is
(adlltl
•
•
•
•
•
TlllUIIlll,
Cryptarchidism,
"Ball dapper dafonnity"
Many occur in sleep (50%)
Necrosis of
in 5-6
hoUIS
• Indirect (through internal
ring, oftEn into scrotum)congenillll
• Direct (through IIXtemal
ring. rarely into scrotum)abdominal muscle weakness
• Non-tender, cystic mJISS
• Transilluminates
• Non-tender, inlrascn!lal
mass
• Cystic
• Transilluminates
• Acute onset severe scrotsl
pail, swelling
• Gl upsets cases
• Retracted and transverse
testicle (horizontal lie)
• Negative Phren's sign
• Absent cramastaric reflex
• A small bulge in the groin
that may increase in size and
disappear when lying down
• Can present as aswollen or
enlarged scrotum
• Discomfurt or shlrp pain espacially when straining.
lilting. or exercising
• Physical exam
• U/S to r/o tumour
• U/S
• Conservative
• Needle drainage
• Surgical
• Emergency manual
detorsion (rotate outward)
with electiva bilateral
orchiopexy
• Falure of manual delllrsion:
surgical delllrsion with
orchiopexy
• Orchiectomy if poor
prognosis
• "Bag of wonns",
Phylical Eum • Oftan painless
• Pulsatas with valsalva
Hislllry/
IIYelligati- • Physical exam
• vasava
T1111tment
• U/S to r/o tumour
• CanseJVBtive
• Consentalive
• Surgical ligation of testicular • Avoid needle aspiration
as it Cllllead to infection,
wins
• Perculllleous vein occlusion reaccumulation and spilling
(balloon, sclerosing agents)
of irrilllting spenn within
• Repair may improve sperm
scrotum
count/motility 50·75%.
• Excisa symptomatic
TIISiicullr To11i1111
l1111uinll Hamil
• History 111d physical
colour ftow
Doppler probe over
• Invagination of the scrotum
testicular artery
• Valsalva
• Decrease uptake on 99m Tcpertechnetate scintillation
scan (doughnut sign)
• Surgical repair
TORSION OF TESTICULAR APPENDIX
• twisting of testicular/epididymal vestigial appendix
• often <16 years of age
Signs and Symptoms
• clinically similar to testicular torsion
• "blue dot sign· - blue infarcted appendage seen through scrotal skin (can usually be palpated as
small, tender lump)
• point tenderness over the superior-posterior portion of testicle
Treatment
• analgesia - most will subside over 5-7 days
• surgical exploration and excision if diagnosis uncertain or refractory pain
HEMATOCELE
• trauma with bleed into tunica vaginalis
• ultrasound helpful to exclude fracture of testis which requires surgical repair
Treatment
• ice packs, analgesics, surgical repair
'IbroDlo Nota 2011
Peaile Com.plainb
Urology U29
Penile Complaints
Payronia's Disease
Definition
• benign curvature of penile shaft secondary to fibrous thickening of tumca albuginea
• commonly on donal surface resulting in upward curvature of erect penis - may occur at any site
Etiology
• exact etiology unknown
• trauma/repeated mk:rotrauma -+ inflammation -+ fibrosis
• familial predisposition
• relllted to diabetes mellitus, vascular disease, autoimmunity, Dupuytren's contracture
• role of vitamin E deficiency. beta-blockade, elevated serotonin
Clinical Features
• penile curvature andlor pain with erection
• penile shortening and poor erection distal to plaque
Tralltment
• depends on pain and interference with intercourse
• watchful waiting (spontaneous resolution in up to SO%)
• vitamin E, potassium paraaminabenzoate (potaba) -limited efficacy
• intralesional verapamll
• surgery if stable disease, slgnlftcant deformity AND failed medl.cal. therapy
• exdsion ofplaque ± prosthesis
Priapism
UROLOGICAL EMERGENCY
Definition
• prolonged unwanted erection lasting >4 hours
• tumescence (swelling) of corpora cavernosa (often painful) with flaccid glans penis (no corpora
spongioswn involvement)
Classlnc:atlon
• low-flow (most common): reducedlabsent cavemosal blood flow-+ hypoxia. acidosis
-+ischemia
• high-How: unregulated a.rtJ:rial flow with normal tissue oxygenation
Etiology
• primary - 60% idiopathic
• secondary:
• thromboembolic - including sickle cell, thalassemia, total parenteral nutrition, dlalf!lll,
leukemia, solid tumours
• neurogenic- spinal cord injury, autonomic neuropathy
• traumatic - cavemosal artery laceration, arterio-venous fistula
• medication- intracavernosal drug injection (e.g. triple lllix), alpha-blockers, anticoagulants.
antidepressant&. antipsychotics, anxiolytia,
• reaeational drugs - cocaine, marijuana. alcohol
Treatment
• treat reversible causes (e.g.leukophorms ifleukemia, treat sickle cell crisis)
• high flow often self-limited - observation vs. a.rtJ:rial embolization
• lowflow:
1. urgent
via needle aspiration of blood
2. phenylephrine injection into the corpora cavernosa ql0-15min
3. ahunt creation between cavemosum and spongiosum ifno response within I hour
Complications
• erect:lle dysfunction due to corporal fibrosis iftreatment delayed (50%)
• 9096 risk if>24 hours
1. Fillraus plaqua
Z. Tmic:a lllbuailel
3. CG!pus I:IW8I'IIOIUm
4.Budt'•fQc;ia
5. CGfpus _,.angiost.m
&. Uralhr1
c J ... Li 201 a
Figura 13. Payronia'a
..
U30 Urology
Penile Complaints
Toronto Notes 2011
Paraphimosis
UROWGICAL EMERGENCY
Definition
• foreskin caught behind glans leading to edema -+ unable to reduce foreskin
Treatment
• squeeze edema out ofthe glans with manual pressure (analgesia required)
• pull on foreskin with fingers while pushing on glans with thumbs
• if fails, perform dorsal slit or circumcision
• elective circumcision for definitive treatment (paraphimosis tends to recur)
Complications
• infection, glans ischemia, gangrene
Phimosis
Definition
• inability to retract foreskin over glans penis
• may be caused by balanitis (infection of glans), often due to poor hygeine or congenital
• normal congenital adhesions separate naturally by 1-2 years of age
Treatment
• circumcision, dorsal slit, proper hygiene (trial of topical corticosteroids in children)
Complications
• balanoposthitis (inflammation of prepuce), paraphimosis, penile cancer
Erectile Dysfunction (ED)
-------------------------------------
Definition
• consistent (>3 months duration) or recurrent inability to obtain or maintain an adequate
erection for sexual performance
Physiology
• erection involves the coordination of psychologic, neurologic, hemodynamic, mechanical and
endocrine components
• nerves: sympathetic (Tll-12), parasympathetic (52-4), somatic [dorsal penile/pudendal nerves
(S2-4)]
Erections POINT AND SHOOT
parasympa1hetics = point; and
sympathlllict/lomatiCI = sboat
• erection ("POINT")
• parasympathetics -+ release ofnitric oxide (NO) -+ increased cGMP levels within corpora
cavernosa leading to:
1. arteriolar dilatation
2. sinusoidal smooth muscle relaxation -+ increased arterial inflow and compression of
penile venous drainage (decreased venous outflow)
• emission ("SHOOT")
• sensory afferents from glans
• secretions from prostate, seminal vesicles, and ejaculatory ducts enter prostatic urethra
(sympathetics)
• ejaculation ("SHOOT")
• bladder neck closure (sympathetic)
• spasmodic contraction of bulbo-cavernosus and pelvic floor musculature (somatic)
• detumescence
• sympathetic nerves, norepinephrine, endothelin-1 -+ arteriolar and sinusoidal constriction
-+ penile flaccidity
Classification
Table 28. Classification of Erectile Dysfunction
Fsyt:hoganic:
Proportion
011141t
Fn=quenc:y
Variation
Age
Organic Risk Fac:tDrs
fHTN, DM, Dyslipidemia]
Nocbi'111VAM aractian
Organic:
111%
90%
Sudden
Gradual
Sporadic
'IIIith partner 111d circumstance
Younger
All circumstances
No
No organic risk fac!Drs
Old•
Risk fac!Drs present
Present
Absent
Toronto Notes 2011
Penile Complaints
Urology U31
Etiology (.. IMPOTENCE'")
•
•
•
•
•
•
•
•
•
Iatrogenic: pelvic surgery/pelvic radiation
Mechanical: Peyronie's, post-priapism
Psychological: depression, stress, anxiety, PTSD, widower syndrome
Occlusive vascular: arterial (hypertension, diabetes, smoking, hyperlipidemia, peripheral
vascular disease, smoking), venous (impaired vena-occlusion)
Trauma: penile/pelvic
Extra factors: renal failure, cirrhosis, COPD, sleep apnea, malnutrition
Neurogenic: CNS (e.g. Parkinson's, multiple sclerosis, spinal cord injury,
spina
bifida, stroke), PNS (e.g. diabetes, peripheral neuropathy)
Chemical: antihypertensives, sedatives, antidepressants, antipsychotics, anxiolytics,
anti-androgens (including 5-alpha reductase inhibitors), statins, GnRH agonists, illicit drugs
Endocrine: diabetes, hypogonadism, hyperprolactinemi.a, hypo/hyperthyroid
Diagnosis
• complete history (sexual, medical, and psychosocial)
• self-administered questionnaires (International Index of Erectile Function, Sexual Health
Inventory for Men Questionnaire, ED Intensity Scale, ED Impact Scale)
• focused physical exam, including vascular and neurologic examinations
• lab investigations - based on clinical picture
• risk factor evaluation: fasting blood glucose or HbAlc, cholesterol profile
• other: TSH, CBC, urinalysis
• hypothalamic-pituitary-gonadal axis evaluation: testosterone (free and total), prolactin, lli,
FSH
• usually unnecessary to do further testing except in certain situations
• specialized testing
• non-invasive:
• nocturnal penile tumescence monitor
• invasive (rarely done):
• intracavemous injection of papaverine or PGE1 - rule out significant arterial or venous
impairment
• Doppler studies pre- and post-papaverine injection - cavernosal anatomy and arterial
flow evaluation (penile-brachial index <0.6 suggestive ofvascular cause}
• angiography of pudendal artery post papaverine injection -post-traumatic ED
evaluation only fur possible vascular reconstruction
• dynamic cavernosometry and cavemosography- to evaluate leakage from penile veins
Treatment
• must fully inform patient/partner of options, benefits and complications
• non-invasive:
• lifestyle changes (alcohol, smoking), psychological (sexual counseling and education)
• change precipitating medications
• minimally invasive:
• oral medication (see Common Medications, U43)
• sildenafil (V!agra•), tadalafil (Cialis•), vardenafil (Levitra•): inhibits phosphodiesterase
type 5
• rarely used
- yohimbine: a-blocker that is best fur psychogenic ED
- trazodone: serotonin antagonist and reuptake inhibitor
• androgen replacement therapy: if hypogonadism
• vacuum devices: draw blood into penis via negative pressure, then put ring at base of penis
once erect
• MUSE: Male Urethral Suppository for Erection - vasoactive substance (PGE1) capsule into
urethra
• invasive:
• intracorporal vasodilator injection/self-injection
• triple therapy (papaverine, phentolamine, PGE1) or PGE1 alone
• complications include priapism (overdose}, thickening of tunica albuginea at site of
repeated injections (Peyronie's plaque) and hematoma
• implants (last resort): malleable or inflatable
• vascular surgery: microvascular arterial bypass and venous ligation (investigational}
... , ,
THiolilanme deficiem:y ia an
uncommon cause of ED.
PDE-5 inhibitoR are contn.indica1ed in
patienlli on nitnrtllf/nitravlyl;erin due to
savere hypotension.
U32 Urology
Penile Complaint:a!I'rauma
Toronto Notes 2011
Premature Ejaculation
----------------------------------
Definition
• occurrence of ejaculation prior to when one or both partners desire it
• primary premature ejaculation
• never experienced sexual activity without the presence of premature ejaculation
• secondary premature ejaculation
• the individual once had acceptable ejaculatory control, but now experiences premature
ejaculation, not associated with a general medical condition
Epidemiology
• 30-70% prevalence
• most common sexual dysfunction reported in men 18-30 years old, associated with secondary
impotence in men 45-65 years old
Investigations
• indicated by history and physical
• testosterone levels if in conjunction with impotence
Treatment
•
•
•
•
•
must rule out and treat any associated general medical conditions (ie. fear of angina)
often thought to be due to psychological factors; identify and address specific stressors
referral to psychiatry, couples counseling or sex therapy
SSRis have been found to be effective in some cases
clomipramine (daily or PRN 4-6 hours before intercourse)
Trauma
• see Emergency Medicine. ER14
Renal Trauma
Etiology
• blunt (80%, motor vehicle collision (MVC), assaults, falls) vs. penetrating (20%, stab wounds
and gunshots)
History
• mechanism of injury
Physical Exam
• ABCs, renal vascular injury -+ shock mandating resuscitation
• upper abdominal/flank tenderness, flank contusions, lower rib/vertebral transverse process
fracture suggests blunt trauma
Investigations
• urinalysis: hematuria- requires workup but degree does not correlate with the severity of injury
• imaging: cr (contrast triphasic) if patient stable -look for renal laceration, extravasation of
contrast, retroperitoneal hematoma. and associated intra-abdominal organ injury
Staging
•
•
•
•
•
I: contusion/hematoma
II: <1 em laceration without urinary extravasation
III: >1 em laceration without urinary extravasation
IV: urinary extravasation
V: shattered kidney or avulsion of pedicle
Classification According to Severity
• minor: contusions and superficial lacerations/hematomas - 90% of all blunt traumas, surgical
exploration seldom necessary
• major: laceration that extends into medulla and collecting system, major renal vascular injury,
shattered kidney
Management
• microscopic hematuria + isolated well-staged minor injuries -+ no hospitalization
• gross hematuria + contusion/minor lacerations -+ hospitalize, bedrest, repeat CT ifbleeding
persists
Toronto Notes 2011
Urology U33
Trauma
• surgical intervention:
• absolute indications: hemorrhage and hemodynamic instability
• relative indications
• non-viable tissue and major laceration
• urinary extravasation
• vascular injury
• expanding or pulsating peri-renal mass
• laparotomy for associated injury
Outcome
• follow up with ultrasound or CT before discharge, and at 6 weeks
• hypertension in 5% of renal trauma
Bladder Trauma
• blunt (MVC, falls, and crush injury) vs. penetrating trauma to lower abdomen, pelvis, or perineum
• blunt trauma is associated with pelvic fracture in 97% of cases
Clinical Features
• abdominal tenderness, distention, and inability to void
• may be peritoneal signs or symptoms
• associated injuries including pelvic and long bone fractures are common
• hemodynamic instability due to extensive blood loss in the pelvis
• suprapubic discomfort and/or tenderness
Investigations
• urinalysis - gross hematuria in 90%
• imaging
• cystogram and post-drainage film for extravasation
Claulflcatlon
• contusions: no urinary extravasation, damage to mucosa or muscularis
• intraperitoneal ruptures: often involve the bladder dome
• extraperitoneal ruptures: involve anterior or lateral bladder wall in full bladder
Treatment
• penetrating trauma: surgical exploration
• contusion: urethral catheter until hematuria completely resolves
• extraperitoneal bladder perforations: typically non-operative with foley insertion
• surgery if. infected urine, rectallvaginal perforation, bony spike into bladder or iflaparatomy
for concurrent injury
• intraperitoneal rupture usually requires surgical repair and suprapubic catheteri2ation
Complications
• complications of bladder injury itself are rare
• mortality is around 20%, and is usually due to associated injuries rather than bladder rupture
Urethral InJuries
Etiology
• posterior urethra: common site of injury is junction ofmembranous and prostatic urethra due
to blunt trauma, MVCs, peMc fracture
• shearing force on fixed membranous and mobile prostatic urethra
• anterior urethra: straddle injury can crush bulbar urethra against pubic rami
• other causes: iatrogenic (instrumentation, prosthesis insertion), penile fracture, masturbation
with urethral manipulation
• always look for associated bladder rupture
Clinical Features
• blood at urethral meatus
• high riding prostate on digital exam
• sensation of voiding without urine output
• swelling and butterfly perineal hematoma
• distended bladder
• penil and/or scrotal hematoma
Investigations
• do not perform cystoscopy or catheteri2ation before retrograde urethrography if urethral
trauma suspected
• retrograde urethrography- demonstrates extravasation and location of injury
',.._---------------,
,
AUpatients with suspected urethral
injury should undergo retrograde
Ul'llhragram {RUG).
U34 Urology
..,., ,
•t----------------.
Do not csthmrim if IIISPIC! umh111l
injury.
Trauma/Infertility
Toronto Notes 2011
Treatment
• simple contusions - no treatment
• partial urethral disruption:
• very gentle attempt at catheterization by urology staff or urology resident
• with no resistance to catheterization- Foley x 2-3 weeks
• with resistance to cathetemation - suprapubic cystostomy or urethral catheter alignment in OR
• periodic flow rates/urethrograms to evaluate fur stricture formation
• complete disruption:
• immediate repair if patient stable, delayed repair if unstable (suprapubic tube in interim)
Infertility
Definition
• failure to conceive after one year of unprotected, properly timed intercourse
• incidence:
• 15% of all couples - investigate both partners
• 1/3 female, 1/3 male, 1/3 combined problem
• primary (has never conceived before) vs. secondary (has conceived before)
Female Factors
• see Gptecology, GY21
Male Factors
Male Reproduction
• hypothalamic-pituitary-testicular axis (HPTA): GnRH from hypothalamus acts on anterior
pituitary stimulating release of LH and FSH
• LH acts on Leydig (interstitial) cells -+ testosterone synthesis/secretion
• FSH acts on Sertoli cells -+ structural and metabolic support to developing spermatogenic
cells
• FSH and testosterone support germ cells (responsible for spermatogenesis)
• sperm route: epididymis -+ vas deferens -+ ejaculatory ducts -+ prostatic urethra
Etiology
• idiopathic (25% infertile males)
• endocrine (see Endocrinology, E48)
• hypothalamic-pituitary-testicular axis (2-3%)
• e.g. Kallmann's syndrome, excess prolactin, excess androgens, excess estrogens
• testicular
• varicocele (35-40% infertile males)
• tumour
• congenital (Klinefelter's triad: small, firm testes, gynecomastia and azoospermia)
• post-infectious (epididymo-orchitis, STis, mumps)
• uncorrected torsion
• cryptorchidism ( <5% of cases)
• obstructive
• iatrogenic (vasectomy, hernia repair, hydrocelectomy, orchidopexy)
• infectious (gonorrhea, chlamydia)
• trauma
• congenital (absence of vas deferens, cystic fibrosis)
• bilateral ejaculatory duct obstruction, epididymal obstructions
• Kartagener's syndrome
• retrograde ejaculation secondary to bladder/prostate surgery
• medications (chemotherepeutics, GnRH agonists, anabolic steroids)
• drugs (marijuana. cocaine, tobacco, alcohol}
• increased testicular temperature (sauna. hot baths, tight pants or underwear)
• chronic disease: liver, renal
History
• medical history (past illness, diabetes, trauma, CF, genetic syndromes)
• surgical history (orchidopexy, cryptorchidism, prostate)
• fertility history (pubertal onset, previous pregnancies, duration of infertility, treatments)
• sexual history (erection/ejaculation, timing, frequency, STis)
• family history
• medications (e.g. nitrofurantoin, cimetidine, sulfasalazine, spironolactone, alpha-blockers)
• social history (alcohol, tobacco, cocaine, anabolic steroids)
• occupational exposures
Toronto Notes 2011
Infertility
Urology U35
Physical Exam
• general appearance (sexual development. gynecomastia)
• scrotal exam (size, consistency and nodularity of testicles; palpation of cord; DRE)
Investigations
• semen analysis (SA) at least 2 specimens over several weeks
• hormonal evaluation - indicated with abnormal semen analysis (rare to be abnormal with
normal SA)
• testosterone for evaluation ofHPA
• FSH measures state of sperm production
• serum LH and prolactin are measured iftestosterone or FSH are abnormal
• genetic evaluation
• chromosomal studies (Klinefelter's Syndrome - XXY)
• genetic studies (Y-chromosome microdeletion, CF gene mutation)
• immunologic studies (antisperm antibodies in ejaculate and blood)
• testicular biopsy
• scrotal U/S (varicocele, testicular size)
• vasography (assess patency of vas deferens)
Treatment
• lifestyle
• regular exercise, healthy diet
• eliminate lifestyle habits described above
• medical
• endocrine therapy (see
E48)
• treat retrograde ejaculation
• discontinue anti-sympathomimetic agents, may start a-adrenergic stimulation
(phenylpropanolamine, pseudoephedrine, or ephedrine)
• treat underlying infections
• surgical
• varicocelectomy (if indicated)
• vasovasostomy (vasectomy reversal)
• epididymovasostomy
• transurethral resection of blocked ejaculatory ducts
• assisted reproductive technologies (ART) - refer to infertility spectalist
• sperm washing + intrauterine insemination (niT)
• in vitro fertilization (IVF)
• intracytoplasmic sperm injection (ICSI)
Figure 14. Infertility Workup
..... , !
WHO GuidlliNarmll 11111111 V.I• Volum1: 2·5 ml
• Concenlnltion: > 20 million sperm/ml
• Morphology: 30'lla nonmlll forms
• Motility: >SO'lla adeqlll!e forward
J11V11111$$ion
•
complltl in 20 minutn
• pH: 7.2·7.8
• WBC: < 1oper high p - field or
<10' WBCfml. semen
.
..... , !
Mutation of Cystic Fibrosis
Transmembrane Conductance Regulator
{CFTR) gene associated with congenilll
bilabnllabunc1 of vas dlf1r1ns
{CBAVD)Ind epididymal cysts, aven if
patient manif8sts no symptoms of CF.
..... , !
Common Ter.....lour on Sem1111lylil:
• Teratospemnia: Abnormal morphology
• AsthlnDSpiiTTlil: Abnormal motility
• Oligospermia: Demased sperm count
• Amospermia: Ablant Jpann in wman
• Mixed types, i.e. oligoiSihenospermill
U36 Urology
Pediatric Urology
Toronto Notes 2011
Pediatric Urology
Congenital Abnormalities
,, ,
Majority of antenatal hydronaphrosas
resolve during pregnancy or wilhin the
first yaar of lifa.
•
•
•
•
not uncommon; 1/200 have congenital abnormalities of the GU tract
UTI is the most common presentation postnatally
hydronephrosis is the most common finding antenatally
six common presentations of congenital urological abnormalities:
1. ANTENATAL HYDRONEPHROSIS
• 1 in 500 fetal U/S -detectable on U/S as early as :first trimester
• most common urological consultation in perinatal period
• can be unilateral or bilateral
• important to examine the rest of the GU system for anomalies
• differential diagnosis
• UPJ or UVJ obstruction
• multi-cystic kidney
• reflux
• posterior urethral valves
• duplication anomalies
• antenatal in utero intervention rarely indicated unless posterior urethral valves
2. POSTERIOR URETHRAL VALVES (PUV)
• the most common obstructive urethral lesion in male infants
• abnormal mucosal folds at the distal prostatic urethra causing varying degrees of obstruction
• most commonly recognized on prenatal ultrasound examination -+ bilateral hydronephrosis,
thickened bladder, oligohydramnios
Clinical Presentation -depends on age and severity
• antenatal: bilateral hydronephrosis, distended bladder, oligohydramnios
• neonatal (recognized at birth): palpable abdominal mass (distended bladder, hydronephrosis),
ascites (transudation of retroperitoneal urine), respiratory distress (pulmonary hypoplasia
resulting from oligohydramnios) and features of oligohydramnios
• neonatal (not recognized at birth): within weeks present with urosepsis, dehydration, electrolyte
abnormalities, failure to thrive
• toddlers: presents with urinary infections or voiding dysfunction
• school-aged boys: voiding dysfunction -+ urinary incontinence
Associated Findings
• oligohydramnios - due to low intrauterine production of urine
• renal dysplasia - due to high pressure reflux
• pulmonary hypoplasia secondary to oligohydramnios
Diagnosis
• VCUG -+ dilated and elongated posterior urethra, reflux
Treatment
• immediate catheterization to relieve obstruction, followed by cystoscopic resection of PUV
3. UPJ OBSTRUCTION
• the most common congenital defect of the ureter (but can be secondary to tumour, stone, etc.)
• M:F=2:1
• 40% bilateral
• unclear etiology: adynamic segment of ureter, stenosis, strictures, aberrant blood vessels -+
extrinsic compression
Clinical Presentation
• symptoms depend on severity and age at diagnosis (mostly asymptomatic :finding on antenatal
UIS)
• infants: abdominal mass, urinary infection
• children: pain, vomiting. failure to thrive
• some cases are diagnosed after puberty and into adulthood
Diagnosis
• antenatal U/S most common, Doppler U/S, IVP, and renal scan± furosemide
Urology U37
'IbroDlo Nota 2011
Treatment
• surgical correction (pyeloplasty), consider nephrectomy if< 1596 renal function
Prognosis
• good since usually unilateral di&ease
4. VESICOURETERAL RER.UX (WR)
• common condition wherein urine p111111es retrograde from the bladder through the UVJ into the
ureter
• incidence ranges from 1-18.5% in normal children
• present in up to 70% ofchildren with UTI
• 85% ofVUR occurs in females but a male presenting with UTI has a hlgher lilaillhood ofhavmg
VUR
• common cause ofantenatal hydronephrosis
• 30-5096 of children with reflux will have renal scarring
• common causes: trigonal weakness, lateral insertion ofthe uretErs, short submucosal segment
(all part of"primary refluxj
• many other causes including secondary reflux, infravesical obstruction, iatrogenic, secondary to
ureteric abnormalities (e.g. ureterocele, ectopic ureter. or duplication), and secondary to cystitis
Presentation
• UTI, urosepsl.s
• pyelonephritis
• pain on voiding
• symptoms ofrenal fiillure (uremia, hypertension)
• diagnosis and staging lB done wing VCUG ± U/S
Complications
• pyelonephritis
• hydroureter/hydronephrosis
Treatment (sea sidebar for grading)
• many cbildren •outgrow" reflux (60% of primary reflux)
• annual renal UIS and VCUGIRNC to monitor; renal scan ifswspect new renal scar (episode of
pyelonephritis)
• treatment Is dependent on the grade:
• medical (grade I-III) - goal is to keep urine free ofinfection to prevent renal damage wbile
waiting for cbild to ·outgrow" their reflux
• long term antibiotic propbylms at half the treatment dose for half the treatment time (TMP/
SMX, amoxicillin, or nitrofurantoin)
• surgical (ureteroneocystostomy± ureteroplasty) or subureteral injection of Dc:Hux- or
.....
'.'
VUR Gredlna IMted an C\'lflllnlll
lirwul: ureters GDv fil
lirwull: unrbn and pt11vislil
lraulll: uratJn and pcilvis fill with
SGIIII dilltatian
Gm.. IV: lnblrs, Pllvil and
with S. .cant dllllldiDII
lrau V: Inters, Pllvis and cllycas Iii
with major dilatalion and 1Qr1uosily
Gla!Ur
Coronal"
Sl.koronal
Macroplastique•
• indications:
- failure of medical management
- new renal scars
- breakthrough infections
- high grade reflux (grade IV or V - not an absolute indication)
• prognosis depends on degree of damage at the time of diagnosis
Dilllll Penile
5. HYPOSPADIAS
• a condition in which the urethral meatus opens on the ventral side ofthe penis. promnal. to the
glans penis
• very common; 1/300 live male births
• multifa.ctorial genetic mode ofinheritance
• white »black
• may be associated with chordee, intersex states, undescended t2sticles or inguinal hernia
• depending on the severity, there may be difficulty directing the urinary stream or infertility
Oong-term)
• treatment Is surgical correction - optimal repair before 2 years old
• circumcision should be deferred because the foreskin may be utllized in the correction
•·
J --..- '
- .·
•
. .. ·.
SQ'IJIII
Perileal
Figura 15. Clluilicetio• af
(*•ccam far 75%)
.....
''
r::l-cRIJ-m_cisa_pdl
_ _ nm_with_.- - - - ,
U38 Urology
Pediatric Urology
Toronto Notes 2011
6. EPISPADIAS-EXSTROPHY COMPLEX
• rare: incidence 1/30,000, 3:1 male to female predominance
• epispadias-exstrophy complex: a spectrum of defects - depends on the timing of the rupture of
the cloacal membrane
• bladder exstrophy (congenital absence of a portion oflower abdominal and anterior vesical
wall, with eversion of bladder)
• several variants
• cloacal exstrophy (vesicointestinal fissure)
• most severe
• exposed bladder, bowel and colon with imperforate anus
• associated with spina bifida in >50%
• epispadias
• least severe
• urethra opens on dorsal penis
• high morbidity -+ incontinence, infertility, reflux
Etiology
• represents failure of closure of the cloacal membrane, resulting in the bladder and urethra
opening directly through the abdominal wall
Treatment
• surgical correction at birth, later corrections for incontinence, increasing bladder capacity and
vesicoureteral reflux may be needed
Naphroblastoma (Wilm's Tumour)
---------------------
• arises from abnormal proliferation of metanephric blastoma
• 5% of all childhood cancers, 5% bilateral
• average age of incidence is 3 years
• 1/3 hereditary (autosomal dominant) and 2/3 sporadic
• familial form associated with other congenital abnormalities and gene defects
Clinical Features
• abdominal mass: large, firm, unilateral (most common presentation- 80%)
• hypertension (60%)
• flank tenderness
• microscopic hematuria
• nausea/vomiting
Treatment
• always investigate contralateral kidney
• treatment of choice is radical nephrectomy ± radiation ± chemotherapy
Prognosis
• generally good; overallS-year survival about 80%
• metastatic disease may respond well
Cryptorchidism/Ectopic Tastes
..._,,
Normal Tntlcullr Develop..lllt ond
Deeclllt in Uloro
Znd Mlllllb- Tnticle begins to form
4th Month - Begins to take Dl1 its
normal
and mi{J'It86 from
its origin at the kidney to the internal
inguinal ring
7th Month - The tntis, surroundld in
peritoneal caverinv. begins to descend
through the intimal ring, inguinal conal
and external ring to terminate in the
scrotum
• definition: testes located abnormally somewhere along the normal path of descent
(prepubic > external inguinal ring > inguinal canal > abdominal)
• ectopic testis (testis found outside its normal path of descent} is rare
• incidence:
• 2.7% of full term newborns
• 0.7%-0.8% at 1 year old
• differential diagnosis:
• retractile testes
• atrophic testes
• intersex state (bilateral impalpable testes)
Treatment
• undescended testes should be brought down to monitor for malignancy and preserve
fertility (better in less than 1 year of age)
• hormonal therapy (hCG or LH may facilitate their descent -+ not proven)
• surgical -+ orchiopexy
Toronto Notes 2011
Pediatric Urology
Urology U39
Prognosis
•
•
•
•
untreated bilateral cryptorchidism -100% infertility
treated bilateral: 60-70% fertility rate (dependent on the age at the time of surgery)
treated/untreated unilateral: fertility is still less than the general population
risk of malignancy is 10-40x increased in undescended testes; this risk does not decrease with
surgical descent, but monitoring is made easier
• increased risk of testicular torsion (always perfonn bilateral orchiopexy for prevention if doing
orchiopexy for torsion)
Disorders of Sexual Differentiation
Definition and Classification
• genitalia that do not have a normal appearance based on the chromosomal sex ofthe child due
to the undermasculinization of genetic males or the virilization ofgenetic females
• considered a social emergency
• four major categories
1. 46XY DSD
• defect in testicular synthesis of androgens
• androgen resistance in target tissues
• palpable gonad
2.46XXDSD
• most due to congenital adrenal hyperplasia (21-hydroxylase deficiency most common
enzymatic defect) -+ shunt in steroid biosynthetic pathway leading to excess androgens
3. ovotesticular DSD
4. mixed gonadal dysgenesis (46 XY/45 XO most common karyotype)
• presence ofY chromosome -+ partial testis determination to varying degrees
Diagnosis and Treatment
• thorough maternal and family history needed
• other fonns of abnormal sexual development:
• maternal medication or drug use in pregnancy -+ maternal hyperandrogenemia
• parental consanguinity
• physical exam: palpable gonad(= chromosomal male), hyperpigmentation, evidence of
dehydration, hypertension, stretched phallus length, position of urethral meatus
• chromosomal evaluation - sex karyotype
• laboratory test:s:
• plasma 17-OH-progesterone (after 36 hours of life) -+ increased in 21-hydroxylase
deficiency (CAH)
• plasma 11-d.eoxycortisol-+ increased in
deficiency
• basal adrenal steroid levels
• serum testosterone and DHT pre- and post-hCG stimulation (2,000 IU/day for 4 days)
• serum electrolytes
• ultrasound of adrenals, gonads, uterus, and fallopian tubes
• endoscopy and genitography of urogenital sinus
• sex assignment (with extensive family consultation)
• must consider capacity for sexually functioning genitalia in adulthood and psychologic
impact
• reconstruction of external genitalia - between 6-12 months
• long term psychological guidance and support for both patient and family
Circumcision
Definition
• removal of some or all of the foreskin from the penis
Epidemiology
• 30% worldwide
• frequency varies depending on geographic location, religious affiliation, socioeconomic
classification
Medical Indications
• phimosis
• definitive treatment of paraphimosis
Contraindication&
• unstable or sick infant
• congenital genital anomalies (hypospadias)
• family history of bleeding disorders warrants laboratory investigation prior to circumcision
. . Chailillflll' l'mdllll
!Willi...
Codnne lhllllllse .\)sf /lev 21m; {21:!m336Z
lie.._.: 11Msl'8'.iiaw llVIUIIalllle
llac:tiwllla ll'lllllflly 11'111 cirann:ililn
fur p!IIVIOOng aapitian llf HN in h..._.
nwl. Th••lylld dill ilfllllnlfnllllldomilld
canllaled trBls ID assess tile elicacy rJ 1111le
citlm:ilion far
HIV aaPiition in IMI1
in Alric:a \Wiich begin il2002.
Clncbinl: Thill'lllli&w lwld lti'Dng INidance
tt11t ITIIIIIcll mae circlm:iliill rab:ls 111e
ICqUilililn ti HN by
mllllblllwlen
m 11'111
24
11111-.tof HIVIIII
.......
whl h111 So with 1111: AMIINIIIpill
JW4 21108; 300(141:1674-84.
lie.._.: TIMslnlllll-nlylis mminad 15
IU!ia (u= 53 561) tt1lt qiJIIItitDI\' ..rinld
the 1110eiltion bllval1111le liluncilion lll1d
HNJS11111101111 men who hive ret willl men
(MSMI.
llulll: n. Dddll ti baing HlV-plllitM Will IIIII
lignificlntlv 1owar
in c:irwmcilad MSM.
Thl•ocidion
HN
ciMicliollll'lll
but notllllistic:att sigriCIIII.
Mill ciriJlmcilion hid I paiiClivl UlllCillion
l'liGI HN in lllldes II MSM Clllllucfld before 1he
ti hijllf IICtiva lnliulrMII1falpy.
Clncbinl: This lllliylis fOII'Id insl&ient
INid..:elllll male ciMiclioll
llglinst HN inllctiDn or Dtlm Slll. llcMMt the
pndlctiwellwct ti ll'lle circn:iiorl
in MSM Wli11 aJnduclld Wore 11!1 n of
lil#t active antirelnMnlllhen!rt supports
f1llfw imllqltion rl male cin:oou:ilian fur HlV
preverOin III'DIIg MSM.
U40 Urology
Pediatric Urology/Selected Urological Procedures
Toronto Notes 2011
Complications
• bleeding
• infection
• phimosis, skin bridges
• fistula
• glans injury
• penile sensation deficits
Enuresis
• see Pediatrics. Pl2
Selected Urological Procedures
Bladder Catheterization
SbipiiiiMIIIiq 11111r in IIIII Sldl
•111111r CaiMIIrialion (-... VIII• in Cb:ll
lledcilts.i•l
1. Ellpllin pnx:adura 1D lhll pllilnt and on1.111
na cantnilllicltianl (blood IIIIIWIU,
ICIOIII hlmltDml, pelvic frlcbn, !Mgll-ridng
proelatll
2. Ensur8 you hlv8 cdllltr •nd tit, idoclile jllly
tllll:1111811r 1Dpa wilhiiiiiiiCh Ill till bldlill
3. wpatiant
don 11011-s!Brile
glowlllld fiiiiCt foralkil
4. Insert 10·15ml of ldocU!e ielll' iiiD LRIInl
meQJI tnd Pnc:fl
p8lils for • •
mindls
5. Open kllnd piiQJ
patilllt'&legl
6. lbi . . giMs
7.
coHua ball in IIQeplic
B. Open lubricllltand dispel ontol:llilllllr1nly
9.
ofwllar lnd callacling ..,nm
!Dcttflltlr
10. l'lllc:efenestJDd dnipe Mr pubic regiorund
pro*lll11iQ111
11.1imp]JIIIile lllllftv.ntlumdominlnl hind.
hold
llld purpaticUir to IIIII
pltielts body (this bind is now nan-lleriel
12. C.• glms ponil in ciwlurrl)lion
13. LJJbriCIII tip of clllllltr, irlllrl iiiD lllllnl
meQis tnd IIMrlce to 1lle IMI of111e IIIIIIDIIII
inllltion port
14. Wd fGI rebln of llile ido colecling
w
Ab:ll.,..
• catheter size measured by the French {Fr) scale- circumference in mm
• each 1 mm increase in diameter = approximately 3 Fr increase {standard size 16-18 Fr)
Continuous Catheterization
• indications:
• accurate monitoring of urine output
• relief of urinary retention due to medication, neurogenic bladder or intravesical obstruction
• temporary therapy for urinary incontinence
• perineal wounds
• clot removal {24-28 Fr) for continuous bladder irrigation {CBI)
• post-operative
Intermittent Catheterization
• indications:
• post-void residual volume measurement
• to obtain sterile diagnostic specimens for urinalysis/cultures
• management of neurogenic bladder or chronic urinary retention
Causes of Difficult Catheterizations and Treatment
• patient discomfort - use sufficient lubrication {± xylocaine)
• collapsing catheter -lubrication as above ± firmer catheter (silastic catheter)
• meatal/urethral stricture - dilate with progressively larger catheters/balloon catheter
• BPH - use
catheter as angled tip can help navigate around prostate
• urethral disruption/obstruction -filiform catheter or suprapubic catheterization
• anxious patient - anxiolytic medication
praalll w
15. !Moe urine is bling, ilftllle llllllaan l'litiiCIUt
•lowilu Cl1ilullrlrnulrlel
16.
pul Clllletlll bac:t lnd llpe ID patient's
111igh f1lpG the cltfllter, not 1ht callacling
$'jSIImUing)
17.11aduceforllkintop!MIIIplla;Mmolis
Complications of Catheterization
• infection - UTI
• meatal/urethral trauma
Contraindications
• urethral trauma: blood at the meatus of the urethra, scrotal hematoma, pelvic fracture, and/or
high riding prostate
Cystoscopy
Objective
• endoscopic inspection of the lower urinary tract {urethra, prostate, bladder neck, walls and
dome, and ureteral orifices) using irrigation, illumination, and optics
• scopes can be flexible or rigid
Indications
• hematuria
• LUTS (irritative or obstructive)
• urethral and bladder neck strictures
• stones
• bladder tumour surveillance
• evaluation of upper tracts with retrograde pyelography (ureteric:: stents, catheters)
Toronto Notes 2011
Selected Urological Procedures
Complications
• during procedure
• infection, bleeding, anesthetic-related
• perforation (rare)
• post-procedure (short-tenn)
• epididymo-orchitis (rare)
• urinary retention
• post-procedure (long-term)
• stricture
Radical Prostatectomy
Objective
• the removal of the entire prostate and prostatic capsule via a lower midline abdominal incision,
laparoscopically or robotically
• internal iliac and obturator vessel lymph nodes may also be dissected and sent for pathology
(dependent on risk: clinical stage, grade, PSA)
• seminal vesicle vessels are also ligated
Indications
• treatment for localized prostate cancer
Complications
• immediate (intraoperative)
• blood loss
• rectal injury
• ureteral injury (extremely rare}
• perioperative
• lymphocele fonnation
• late
• moderate to severe urinary incontinence (3-10%)
• mild urinary incontinence (20%)
• erectile dysfunction (-50%, depending on whether one, both, or neither of the neurovascular
bundles are involved in extracapsular extension of tumour)
Transurethral Resection of the Prostate (TURP)
Objective
• to partially resect the periurethral area ofthe prostate (transition zone) to decrease symptoms of
urinary tract obstruction
• accomplished via a cystoscopic approach using an electrocautery loop, irrigation (glycine}, and
illumination
Indications
•
•
•
•
•
•
obstructive uropathy (large bladder diverticula, renal insufficiency)
refractory urinary retention
recurrent UTis
recurrent gross hematuria
bladder stones
intolerance/failure of medical therapy
Complications
• acute:
• intra- or ext:raperitoneal rupture ofthe bladder
• rectal perforation
• incontinence
• incision of the ureteral orifice (with subsequent reflux or ureteral stricture)
• hemorrhage
• epididymitis
• sepsis
• transurethral resection syndrome (also called "post-TURP syndrome·)
• caused by absorption of a large volume of the hypotonic irrigation solution used, usually
through perforated venous sinusoids, leading to a hypervolemic hyponatremic state
• characterized by dilutional hyponatremia, confusion, nausea, vomiting, hypertension,
bradycardia, visual disturbances, CHF, and pulmonary edema
• treat with diuresis and (if severe) hypertonic saline administration
Urology U41
U42 Urology
Selected Urological Procedures
Toronto Notes 2011
• chronic:
• retrograde
(>75%}
• erectile dysfunction (5-1 0% risk increases with increasing use of cautery)
• incontinence (<1%)
• urethral stricture
• bladder neck contracture
Extracorporeal Shock Wave Lithotripsy (ESWL)
Objective
• to treat renal calculi, proximal calculi, and midureteral calculi which cannot pass through the
urinary tract naturally
• shockwaves are generated and focused onto stone -+ fragmentation, allowing stone fragments to
pass spontaneously and less painfully
Indications
• potential first-line therapy for renal and ureteral calculi less than 2.5 em in size
• individuals with calculi in solitary kidney
• individuals with hypertension, diabetes or renal insufficiency
Contraindication&
• acute urinary tract infection or urosepsis
• bleeding disorder or coagulopathy
• pregnancy
• obstruction clistal to stone
Complications
• bacteriuria
• bacteremia
• post-procedure hematuria
• ureteric obstruction (by stone fragments)
• peri-nephric hematoma
Toronto Notes 2011
Urology U43
Common Medications
Common Medications
Tabla 21. Antibiotics
Duration of TNIIImant
Umililti-ID Uu
Simple uncomplicated cystitis
Recunent cystitis
Pyelonephritis
Prostatitis
Epididynitiil/architis (Gremilegative organism)
3 days
Stevens.Jolrlson syndrome
?Salety in last 2 weeks of pregnancy
Resistalce 20% in the community
nilrufunrrtoin
Simple uncomplicated cystitis
Recunent cystitis
7 days
Contnindicated in nmal failure
Pulmonary toxicity/fibrosis
ciproflox.acin
Cystitis
Pyelonephritis
3 days
7-14 days
?Safety in pregnancy
Achilles tendon rupture
genlllmicin
Severely ill patients with pyelaneplritis, prostatitis
Dnlg
TMP/SMX
LDI'(lll!rm as prophylaxis
14 days
4-awusb
Zweeks
Only IV
Nephllllllxic
Ototoxic
Tabla 22. Erectile Dysfunction Medications
Dnlg
Cia•
Machlnilm
sildenalil (V'IIgraat)
tadalafil (Cialisllt)
vardenalil (l..evitra"l
Phosphodiastarase 5
inhibiiDr
Selectiva irtlibition of PDE5
(enzyme which degrades cGMP)
Leads to sinusoidal smooth muscle
relaxation and erection
alprostadi (MUSE:
Male Unrtlnl Suppository
fur Erection)
Prostaglandin E1
Activation of cAMP. relaxing
sinusoidlll smooth muscle
Local release (capsule inserted
intD urethra)
ED
Penile
Presyncope
alprostadi
(intracavemosal iljection)
triple therapy also used:
papaverine, phentolamine,
See above
See above
ED
Thickening of tunica albuginea at site of
repeated injections (Peyronie's plaque)
Painful erection
Hematoma
Contrainrlcated if Hx of priapism, or in conditions
predisposing to priapism
lndi:ltion
ED when some erection
present
Sevara hypotansion
Contraindicated if Hx of priapism. or in
conditions predisposing to priapism (leukemia,
myelofibrosis, polycythemia, sickle cell disease)
Contlllindicatad with nilllltas
pan
PGE1
Tabla 23. B•ign Prostatic Hyperplasia Medications
Dnlg
Clus
Machanism
lndiCition
tei8ZOSin (llytrin"l
dDXIIZOSin (Callba"l
tamsulosin (Aornax®)
Alpha 1blockers
Alpha-adrenergic anlllgonists reduce stromlll
smooth muscle tone
Reduce dynamic component of bladder outlat obstruction
BPH
finasteride
dutasteride (Avodartilt)
5 alpha-reductase
inhibiiDr
Blocks convarsion of tastosterone to DHT
Reduces static corqlOilent of bladder outlet obstruction
Reduces prostatic volume
BPH
Alpha 1a selactiva
Alpha 1a selactiva
Presyncope
Leg edema
Ratrograde ejaculation
Headache
Asthenia
Nasal congestion
Saxual dysfunction
PSA decreases
Naill: AI alpt.-IIIDCbrs diMllopad far 81'11 hiVIlsimillr afli:lcy. '-a(.llph•1sala:IMI11Q811!1 hM 111 impnMld sida lllact pmfila.
Tabla 24. Prostatic Carcinoma Medications
Drug
Class
Machanilm
lldic:ation
Advasa Elfacts
leuprolide (Luprnnllt, 8igard"),
goserelin (Zolad!lt8 )
GnRH agonist
ntially stimulates LH. increasing testosterone and
causing "flare" {clinically: i'lcreased bone pain),
later causes low testosterone
CaP (N>D, M>D)
Hot flashes
*diethylstilbestrol (DES)
Estrogens
Hlibit LH and cytotoxic effect on tumour cells
As above
*cyproterone acetate
Steroidel antiandrogen
with DHT for iltracellular receptors:
1. Prevent flare produced by GnRH agonist
2. Use for compiBIB androgen blockade
3. May preserve patency
As above
ftutamide
bicalutamide (Caso£Ex®)
Nort-steroidal antiandrogen
As above
As above
Hepatotoxic: AST/ALT monitoring
*ketoconazole, spironolactone
Steroidogenesis inhibiiDrs
Blocks multiple enzymes in steroid pathway,
including adrenal androgens
As above
Gl syrl1IIDrns
Hyperkalemia
Gynecomastia
Headache
Decreased libido
Increased risk of cardiovascular events
U44 Urology
Toronto Notes 2011
Common MedicationsJR.eferenc:es
Tabla 25. Continanca Agents
Drug
Clus
oxybutynin
AntispiiSIIlDiic
lndl:lllion
lmibillactian Df ACh an
smaD1h muscle
oxybutynin {Ditropan<»)
tolterodine {Detro18 )
trospium [Trosec18)
Anticholilergic
(Vesicaraa)
lkge incontinence +
urgency + frequency
llecreeses frequency of
unirllibited detrusor
contraction
lliminishes initial urge to void
Muscarinic receptor antagonist lkge incontinence +
Selective for bladder
urgency + frequency
Increases bladder vo.,me
llecraases detrusor pressure
Dry mouth
Blurred visim
Canstipatian
Supraventricular
tachycardia
As above
dlllilenacin {Enablat')
imipramine
Tricyclic
llllidelftSSBnt
Sympathomimetic sff8cts:
urinary sphincter conlnlction
Stress and urge
incontinence
As abDW
Weight gain
Anticholinergic elfects:
Orthostatic hypotension
detrusor relaxation
Prolonged PR interval
Nlllt: AIIIIIIH:IMJiilwgics 11111J11ily lfllctiw and liq acting fmmulllilns (llllrollA1 111d Ditropln XL8)111 balblr IDiarrllld. Nln IIIISCII'inic t.l3 rapiDr spaciic
IHJIIIIIy Efficacious iiS older drugs, hllwever, ACTs bued 111 helcl-111·/nml compuisan to lang acting furmulllilns n
llglds lsallenlcin.
References
G.... lnfllrnlti111
AnuriCillllrulogical Allocillli1111. http;'/wwau111111..D19'guidainlrl
Amll'iC111 Aao1:i1ticr1 of Ftmily Phy$icia11$. hllp;'/wtow.Mfp.tqiafpl2002041 W158UIIm
Ferri F. Practical Glide ID tt. Clll oftt.lllldical plliant (&thad.) ZW6. St Lllil: Mosby.
Galdmln I, Ausialo D. Cecil Tlldbook of Medicine (22nd ad.] 2004.
Salnlars (EIIaviar).
MIICflrlme MI House lllicer Series: Uralogy. 13rd ad.] ZWI.
UAJincotl Ylfllllllli &
TaiiiQIIo EA. McAnilch JN. Srrith's Glmllll Uralogy.(l&th ad.)2004. McGraw-Hill Companies,
Uralogy Clilnnal
Wein AJ, Kavoussi Ul, Novick AC, l'lrlin AW rnd Cl'eteTs CA. Campbelrs Urology. 19th ed.]
PhilldeliJ!il: WB Saunders Co.
c-llll'rlllllllingl'n6ll•
Colirn RA 111d llrailn RS. Micrascapic hamablia. Naw Englrnd Joumal II Mldicine.2003;348:2330-2338
MoriDnAR,IIilsm EAand Wil11111 JWI.. Nephrology: l.lnwlligltion lndtnlllrrWit!IIICIUIIIII kilhlyiiDIIBL CMAJ 166(2):213-218,Jan 2002
Teichnan JMH. Acute -.nal colic ln1m
c•lcuiJs. New England Joumalcl Madicile. 2004;350:684·693
Uralagi:ll Ern.Jn:ia
Galejs LE. Dilgnolis and treatmrnt ol the IICUII scra11rn. Americ:lln Ftmily l'hyan. 1991;51(41:817-24
Medialions
Bii-Axelson A, Holmberg I, llwtu M, et. al. Radical Proslnc:tomyversus
Waiting il Early l'rosllte Cancer. NEJM. ZW5; 352: 1977·84.
Common Medications: Gray J (Edi1mj. Therapeutic Choicas (4th ld). Canadiln Phlrmacirls Allocilltion, Dttawa. 2003.
Micramadax heellh catlll8rias. v.ww.micnlmedax.com
Rini B. HIIIIIi S.llale*l!l J. et.al Bevaciarmab Pl.ile
Cornplllll with Interferon Alta MDII!Ihmpy in l'ltientJ with Metn111ic Renal Cell Can:incml:
CALGB !11206. J. Cln. One. 2008; 26: 5422-28.