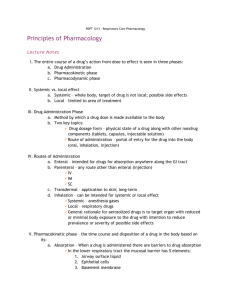
MODULE 2 PHARMACODYNAMICS PHARMACODYNAMIC PHASE “What the DRUG does to the body?” - Effects of drug in the body Drug response can cause a primary or secondary physiologic effect or both. - The primary effect is desirable. secondary effect may be desirable or undesirable. The primary effect of diphenhydramine is to treat the symptoms of allergy, and the secondary effect is a central nervous system depression that causes drowsiness. The secondary effect is undesirable when the patient drives a car, but at bedtime it could be desirable because it causes mild sedation. DOSE RESPONSE RELATIONSHIP - Is the body’s physiologic response to changes in drug concentration at the site of action. - Dose response is the relationship between the minimal versus the maximal amount of drug dose needed to produce the desired drug response. Some patients respond to a lower drug dose, whereas others need a high drug dose to elicit the desired response. The drug dose is usually adjusted to achieve the desired drug response. - For ex: Morphine and tramadol hydrochloride are prescribed to relieve pain. The maximum efficacy of morphine is > tramadol hydrochloride, regardless of how much tramadol hydrochloride is given. The pain relief with the use of tramadol hydrochloride is not as great as it is with morphine A. POTENCY – refers to the amount of drug needed to elicit a specific physiologic response to a drug. - The ability or capacity to achieve or bring about a particular result. B. MAXIMAL EFFICACY – The point at which increasing a drug’s dosage NO longer increases the desired therapeutic response. THERAPEUTIC INDEX AND THERAPEUTIC RANGE (THERAPEUTIC WINDOW) Therapeutic index (TI) – describes the relationship or ratio between therapeutic dose of a drug (ED50) and the toxic dose of a drug (TD50). The TI is the difference between these two points, ED and TD. Page 1 of 12 MODULE 2 PHARMACODYNAMICS Legend: ED – effective dose/therapeutic dose ED50 – Effective dose in 50% of people LD/TD50 – lethal dose, toxic dose in 50% of people. Drugs with low therapeutic index – have a narrow margin of safety, dosage might need adjustment and drug levels need to be monitored because of the small safety range between TD and ED Ex. Warfarin Digoxin Phenytoin Drugs with high therapeutic index – have a wide margin of safety and less danger of producing toxic effects. Plasma/serum drug levels DO NOT need to be monitored routinely for drugs with a high TI. Page 2 of 12 MODULE 2 PHARMACODYNAMICS ONSET, PEAK, DURATION OF ACTION ONSET – is the time it takes for a drug to reach the minimum effective concentration (MEC) after administration. MEC – minimum amount of drug required for drug effect. PEAK – occurs when it reaches its highest concentration in the blood. DURATION OF ACTION - is the length of time the drug exerts a therapeutic effect. *Some drugs produce effects in minutes, others may take hours or days. *If the drug plasma concentration decreases below the MEC, adequate drug dosing is not achieved, too high of a drug concentration can result in toxicity. Page 3 of 12 MODULE 2 PHARMACODYNAMICS Onset-Peak-Duration THERAPEUTIC DRUG MONITORING PEAK AND TROUGH DRUG LEVELS Peak and trough levels are drawn to determine a drug's concentration within the system They help determine if a drug is in a toxic range or if the dosage of the medication needs to be increased. PEAK - is the highest level of a medication in the blood at a specific time. It indicates the rate of drug ABSORPTION. If a peak drug level is ordered, a blood sample should be drawn at the proposed peak time, according to the route of administration. *Orally – peak time is usually 2-3 hours after drug administration. *IV – usually 30-60 minutes after infusion is complete. *IM – usually 2-4 hours after injection. TROUGH - Is the lowest plasma concentration of a drug. It measures the rate at which the drug is ELIMINATED. Trough levels are drawn immediately before the next dose of drug is given, regardless of route of administration. Page 4 of 12 MODULE 2 PHARMACODYNAMICS RECEPTOR THEORY RECEPTORS - - Mostly proteins that are found on cell surface membranes or within the cell itself. Receptor is where the binding of the drug may activate and produce a response. LIGAND - Any chemicals that bind to receptors are termed ligands (ex. Drugs) Page 5 of 12 MODULE 2 PHARMACODYNAMICS FOUR RECEPTOR FAMILIES: 1. Cell membrane-embedded enzymes - the ligand-binding domain for drug binding is on the cell surface. The drug activates the enzymes inside the cell and the response is initiated. 2. Ligand-gated ion channels - the channel crosses the cell membrane. When the channel opens, ions flow in and out of the cells. This primarily affects sodium and calcium ions. 3. G Protein-coupled receptor Systems Three components: 1. The receptor 2. The G-protein that binds with guanosine triphosphate (GTP) 3. The effector – either an enzyme or an ion channel. DRUG Activates Receptors Activates G Protein Activates Effect Page 6 of 12 MODULE 2 PHARMACODYNAMICS 4. Transcription factors - found in the cell nucleus on DNA, not on the surface. Activation of receptors through transcription factors regulates protein synthesis and is prolonged. Unlike the first three which is rapid. *Ligand-binding domain – the site on the receptor at which drugs bind. AGONISTS, PARTIAL AGONISTS, AND ANTAGONISTS AGONISTS - drugs that activate receptors and produce desired response. Turn “ON” ANTAGONISTS - drugs that prevent receptor activation and block a response. Stop the reaction, turn “OFF.” PARTIAL AGONISTS - are drugs that elicit only moderate activity when binding to receptors also prevent receptor activation by other drugs. Page 7 of 12 MODULE 2 PHARMACODYNAMICS NONSPECIFIC AND NONSELECTIVE DRUG EFFECTS NONSPECIFIC DRUGS - Affect different sites of the same receptor. Example: Bethanecol – acts on cholinergic receptors located in the Bladder, Bronchus, Stomach, Blood vessels, Heart, Eyes NONSELECTIVE DRUGS - Drugs that affect different receptors. Example: Epinephrine – is used to treat anaphylaxis or severe asthma exacerbations (acts on Aplha1, Beta1, Beta2 receptors Page 8 of 12 MODULE 2 PHARMACODYNAMICS MECHANISMS OF DRUG ACTION 1. - Stimulation a drug that stimulates and enhances intrinsic activity Example: Adrenergic drugs – medications that stimulate certain nerves in your body. They do this my mimicking the action of the chemical messengers epinephrine and norepinephrine or by stimulating their release. - increase heart rate, sweating, and respiratory rate during fight or flight response. 2. Depression – decrease neural activity and bodily functions e.g. barbiturates and opiates Opiates - used to treat pain or cause sleep Ex. Fentanyl, Codein, Morphine Barbiturates – sedative-hypnotic medications used to stop or prevent convulsions and seizures. Ex. Phenobarbital, 3. Irritation – noxious effect such as astringents Page 9 of 12 MODULE 2 PHARMACODYNAMICS 4. Replacement – e.g. insulins, thyroid drugs, and hormones that replace essential body compounds Cytotoxic action – selectively kill invading parasites or cancers 5. - contain chemicals which are toxic to cells, prevents their replication or growth. - sometimes known as antineoplastics. Antimicrobial action – prevent, inhibit, or kill infectious organisms 6. 7. Modification of immune status – modify, enhance, or depress the immune system (e.g. interferons and methotrexate) Interferon – helps the immune system fight infection and other diseases. Methotrexate – immunosuppressant, slows down immune system and help reduce inflammation, ex. Rheumatoid arthritis SIDE EFFECTS, ADVERSE DRUG REACTIONS, AND DRUG TOXICITY SIDE EFFECT - - - Are secondary effect of a drug therapy. Side effects occur and can be predictable and may be desirable or undesirable. Range from inconvenient to severe or life threatening. Some are expected as part of drug therapy. Nurses must teach patients to report any side effects because side effects are the primary reason why patients stop taking the prescribed medication. The occurrence of side effects is NOT a reason to discontinue therapy, but can be managed with dosage adjustments, changing to a different drug in the same class of drugs, or implementing other interventions. Page 10 of 12 MODULE 2 PHARMACODYNAMICS ADVERSE DRUG REACTIONS (ADR) - Unintentional, unexpected reactions to drug therapy that occur at normal dosages. Reaction may be mild to severe and include anaphylaxis. Always undesirable and must be reported and documented. DRUG TOXICITY - When drug levels exceed the therapeutic range Results from overdose(intentional or unintentional) or drug accumulation. Factors that influence drug toxicity: - Disease Genetics Age TOLERANCE AND TACHYPHYLAXIS TOLERANCE - Decreased responsiveness to a drug over the course of therapy. An individual with drug tolerance requires higher dosage of drug to achieve the same therapeutic response. TACHYPHYLAXIS - Refers to an acute, rapid decrease in response to a drug, it may occur after the first dose or after several doses. Is considered, “acute tolerance.” PLACEBO EFFECT - Is a drug response not attributed to the chemical properties of the drug. - The response can be positive or negative. - May be influenced by the beliefs, attitudes, and expectations of the patient. - Although the placebo effect is psychological in origin, the response can be physiologic which results in changes in heart rate, BP, and pain sensation. Page 11 of 12 MODULE 2 PHARMACODYNAMICS Page 12 of 12