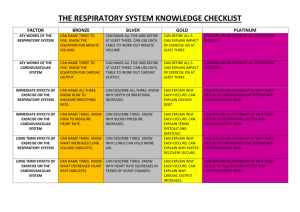
NORTH WALES CRITICAL CARE NETWORK LEVELS OF CRITICAL CARE FOR ADULT PATIENTS Throughout the work of the North Wales Critical Care Network reference to ‘Levels of Care’ for the critically ill are frequently required. Examples of such are, amongst others, when collecting data for the ‘patient flow’ studies or undertaking ‘unmet demand’ studies throughout the entire acute Trusts. Levels of Care are described in Designed for Life: Quality Requirements for Adult Critical Care in Wales (WHC 009 2006). However, the Network work groups have identified several difficulties with the interpretation of the definitions. This is partly because they are sometimes confused with English definitions and often because they are subjectively interpreted. Confusion is further compounded because the levels of care are précised in the Welsh Standards for Adult critical Care in Wales (2003) but additional definitive guidance is not provided. It is for these reasons therefore that the Network has enhanced the levels of care definitions by providing examples. Whilst it will be impossible to provide an example for all patient scenarios it is hoped that these will aid clinical practice and reduce the subjectivity in interpretations. The definitions for level of care in Wales are as follows (All Wales Critical Care Development Group 2003). Level 0 Suitable for patients whose needs can be met through normal ward care in an acute hospital. Level 1 Suitable for patients at risk of their condition deteriorating, those recently relocated from higher levels of care, and those whose needs can be met on an acute ward with additional advice and support from the critical care team. Level 2 Suitable for hospitalised patients requiring more detailed observation or intervention, including support for a single failing organ system, postoperative care and those stepping down from higher levels of care. Level 3 Suitable for hospitalised patients requiring advanced respiratory support in addition to the above, but the duration of multi-organ support or ability to manage multiple patients might be limited by staffing or equipment constraints. Level 3T Organ support and monitoring for most body systems should be available at Level 3T and these facilities would normally be available to multiple patients simultaneously. This level is suitable for critically ill patients requiring prolonged support for multi-organ failure. Such units would have a significant teaching and training role. Levels of Care Examples [Final] NWCCN Informatics Group Revised December ‘09 1 QUICK GUIDE TO LEVELS OF CRITICAL CARE FOR ADULT PATIENTS LEVEL 3 = (FOR MORE DETAIL & DEFINITION PLEASE REFER TO FOLLOWING PAGES) INCLUDE EXCLUDE 2 ORGAN SUPPORT (DUE TO ACUTE ILLNESS) ADVANCED RESPIRATORY SUPPORT GI SUPPORT 1 CHRONIC ORGAN SUPPORT + 1 ACUTE ORGAN SUPPORT: BASIC RESPIRATORY SUPPORT + BASIC RESPIRATORY SUPPORT + RENAL SUPPORT = LEVEL 3 BASIC CARDIOVASCULAR SUPPORT = BASIC RESPIRATORY SUPPORT + NEURO SUPPORT = LEVEL 3 LEVEL 2 BASIC RESPIRATORY SUPPORT + DERMATOLOGICAL SUPPORT = LEVEL 3 BASIC CARDIOVASCULAR SUPPORT + RENAL SUPPORT = LEVEL 3 BASIC CARDIOVASCULAR SUPPORT + NEURO SUPPORT = LEVEL 3 BASIC CARDIOVASCULAR SUPPORT + DERMATOLOGICAL SUPPORT = LEVEL 3 ADVANCED CARDIOVASCULAR SUPPORT + BASIC RESPIRATORY SUPPORT = LEVEL 3 ADVANCED CARDIOVASCULAR SUPPORT + RENAL SUPPORT = LEVEL 3 ADVANCED CARDIOVASCULAR SUPPORT + NEURO SUPPORT = LEVEL 3 ADVANCED CARDIOVASCULAR SUPPORT + DERMATOLOGICAL SUPPORT = LEVEL 3 NB BASIC RESPIRATORY SUPPORT + BASIC CARDIOVASCULAR SUPPORT = LEVEL 2 LEVEL 2 = 1 ORGAN SUPPORT (DUE TO ACUTE ILLNESS) BASIC RESPIRATORY SUPPORT + BASIC CARDIOVASCULAR SUPPORT = LEVEL 2 PRE-SURGICAL OPTIMISATION REQUIRING INVASIVE MONITORING EXTENDED POST-OP CARE PATIENTS REQUIRING HIGH DEGREE MONITORING OR OBSERVATION PATIENT RECENTLY LEVEL 3 BUT NOT WELL ENOUGH FOR LEVEL 1 PATIENT WITH UNCORRECTED ABNORMAL PHYSIOLOGICAL VARIABLES LEVEL 1= EPIDURAL ANALGESIA RECENTLY DISCHARGED FROM HIGHER LEVEL OF CARE OUTREACH SUPPORT REQUIRED LEVEL 0 NORMAL WARD CARE PRE-OP BED BLOCKING ROUTINE POST-OP PATIENTS DELAYED DISCHARGES (See Appendix 1 for description of basic, advanced respiratory and cardiovascular etc support) Levels of Care Examples [Final] 2 NWCCN Informatics Group Revised December ‘09 Level of Care Definitions (See Appendix 1 for description of basic, advanced respiratory and cardiovascular etc support) Level 3 Criteria Advanced respiratory support Monitoring and Support of two or more organs due to an acute illness (one of which may be basic or advanced respiratory support). Chronic dysfunction of one or more organs sufficient to restrict daily activities and who receive monitoring and support for one other organ due to an acute illness Levels of Care Examples [Final] Examples Respiratory failure from any cause that requires invasive, ventilatory support. Examples may include patients with: • Neurological depression o GCS <8 o Neuromuscular failure • Respiratory failure o Acute or chronic lung problems requiring ventilation e.g. COPD, ARDS, pneumonia, pulmonary oedema etc • Severe Cardiovascular instability o E.g. Shock – sepsis, cardiogenic etc Include Mechanical ventilatory support Acute dysfunction of two or more organs. Examples may include patients with: • Respiratory and cardiovascular failure o Invasive ventilation and intravenous vasoactive drugs • Respiratory and renal failure o Invasive ventilation and heamofiltration • Respiratory and neurological dysfunction1 o Airway protection for GCS< 8 • Major surgery who require advanced respiratory support (above) and monitoring / support of other organs • Continuous IV medication to control seizures and supplementary oxygen/airway monitoring Basic respiratory and renal, neurological or dermatological support Examples may include patients with: • Severe ischaemic heart disease and major perioperative haemorrhage • COPD requiring home oxygen presenting with sepsis related to immunosuppression Angina on mild exercise and pneumonia requiring CPAP 3 Exclude BIPAP / CPAP via ET tube Mask BIPAP Extracorporeal respiratory support CPAP via trache Non-invasive mask ventilation See page 6 for algorithm Basic cardiovascular and renal, neurological or dermatological support Gastrointestinal support Basic cardiovascular plus basic respiratory = Level 2 Advanced cardiovascular and basic respiratory or renal or neurological or dermatological support Gastrointestinal support Basic cardiovascular plus basic respiratory support = Level 2 NWCCN Informatics Group Revised December ‘09 (See Appendix 1 for description of basic, advanced respiratory and cardiovascular etc support) Level 2 Criteria Admissions receiving monitoring and support for one organ due to an acute illness Examples Examples may include patients with: • Respiratory supporto >50% inspired oxygen2 o A tracheostomy inserted in the last 24 hours o NIV or mask CPAP o The requirement for physiotherapy or suctioning at least every 2 hours • Cardiovascular supporto Cardiovascular instability requiring continuous ECG and invasive pressure monitoring o Haemodynamic instability due to hypovolaemia/haemorrhage/sepsis o Haemodynamic instability requiring balloon pump o A single infusion of vasoactive drug requiring appropriate monitoring4 • Central nervous system supporto CNS depression sufficient to compromise airway and protective reflexes • Acute impairment of renal, electrolyte or metabolic function o Renal replacement therapy o DKA o Profound hypothermia Include Basic cardiovascular support and basic respiratory support = one organ dysfunction = Level 2 Admissions receiving presurgical optimisation requiring invasive monitoring and treatment to improve organ function Examples may include patients requiring: Haemodynamic/respiratory resuscitation or optimisation. • Elective major surgery but pre-optimisation • Emergency surgery but resuscitation Insertion of invasive monitoring Admissions receiving extended post surgical Examples may include patients with: • Major elective surgery Levels of Care Examples [Final] Renal support Exclude Gastrointestinal support NIV- long standing or established care Neurological support Dermatological support Step down (relevant when no other support ticked – no longer needs ITU care but requires greater monitoring / observations than could be provided on a general ward) Invasive lines in for ‘convenience’ e.g. taking blood or IV access for drugs that could be given peripherally3 Pre-operative admissions to ‘reserve’ the critical care bed Routine post operative patients 4 NWCCN Informatics Group Revised December ‘09 care either because of the procedure and/or the condition of the admission. • • • Emergency surgery who are unstable or high risk An increased risk of post operative complications or interventions Intermediate surgery but who are >70 years or > ASA III (i.e. severe system disease with functional limitation or worse) Admissions receiving a greater degree of observation and monitoring than level 1 care Examples may include patients requiring: • Observation and monitoring that cannot be safely provided at level 1 or 0, judged on the basis of clinical circumstances and ward resources o Complex surgery, trauma requiring multiple blood transfusions o Treatment for severe DKA o Complex surgery requiring strict monitoring e.g. Free flap surgery, major vascular surgery, cardiac surgery, neuro surgery etc o Confused or fitting patients Admissions moving to stepdown care Examples are patients who were recently level 3 or 3T but are not well enough to be classed as level 1 or 0. Admissions with uncorrected physiological abnormalities receiving level 2 care as above Examples may include patients with: • Respiratory rate >40 breaths/min or >30 breaths/min for >6 hours • Heart rate >120 beats/min • Temperature <350C for >1 hour • Systolic BP <80 mmHg for >1 hour • Glasgow Coma Scale (GCS) <10 and at risk of deterioration Levels of Care Examples [Final] 5 Patients requiring significant nursing time e.g. Patients requiring ‘specialing’ Routine post operative patients Delayed discharges from critical care where the patient is now classed as level 1. NWCCN Informatics Group Revised December ‘09 (See Appendix 1 for description of basic, advanced respiratory and cardiovascular etc support) Level 1 Criteria Recently discharged from higher level of care Examples Examples are patients who were recently level 2 but are not well enough to be classed as level 0. Include All ITU/HDU discharges (unless classed level 2) Critical care outreach service support required Examples may include patients with: • Abnormal vital signs but not requiring a higher level of care Additional monitoring, clinical input or advice required Examples may include patients requiring: • >level 0 care • Observations at least 4 hourly • Physiotherapy or suctioning at least 6 hourly, but not more than 2 hourly (see level 2) Care from specialist staff / requiring additional facilities for one or more aspects of critical care on ward Examples may include patients requiring: • Renal replacement therapy (stable chronic renal failure) • Epidural analgesia • Tracheostomy care Patients requiring ‘specialing’ Level 0 Criteria Receiving normal ward care Examples Examples may include patients requiring: • Oral medication • Bolus IV medication • Patient controlled analgesia (PCA) • Observations less frequently than 4 hourly Include Exclude Exclude Additional Notes: Tracheosotomies per se do not contribute to levels of care. 1. If patients are intubated solely for airway protection then this triggers basic respiratory support only. It will generally also trigger neurological support as many of these patients will also have decreased level of consciousness due to brain dysfunction. See example in level 3 2. If patient are on 50% or less oxygen this does not trigger either advanced or basic respiratory care i.e. patients have to be on 51% or more. 3. Most patients will have their invasive monitoring in situ until just prior to leaving the unit, for patient comfort and our convenience. CVC or IA lines should only contribute to CVS level of care if you would replace or insert the line if it was not in situ at this point in time, and it would be beneficial to patient monitoring. 4. To trigger advanced CVS level of care then a patient must be on more than one inotropes or more than one rhythm control drugs. Being of one of each only triggers basic CVS. Levels of Care Examples [Final] 6 NWCCN Informatics Group Revised December ‘09 Appendix One (Reference CCMDS DSCN (2006) 14 pgs 15-17) 1. Basic Respiratory Support Indicated by one or more of the following: More than 50% oxygen delivered by face mask. Close observation due to the potential for acute deterioration to the point of needing advanced respiratory support (e.g. severely compromised airway or deteriorating respiratory muscle function). Physiotherapy or suction to clear secretions at least two hourly, whether via tracheostomy, minitracheostomy, or in the absence of an artificial airway. Patients recently extubated after a prolonged period of intubation and mechanical ventilation, via an endotracheal tube for more than 24 hours. Mask continuous positive airway pressure CPAP or non-invasive ventilation. Patients who are intubated to protect the airway but needing no ventilatory support and who are otherwise stable. 2. Advanced Respiratory Support Indicated by: Invasive mechanical ventilatory support (excluding mask / hood continuous positive airway pressure (CPAP) or mask pressure support ventilation (BiPAP) or CPAP applied via a tracheal tube). Summary algorithm that explains the differences between basic (BRS) and advanced respiratory support (ARS). Ventilation ARS Trans-laryngeal BiPAP or CPAP INTUBATION? Tracheostomy No ventilation BRS Ventilation ARS BiPAP CPAP No ventilation, long term airway access only BRS No ARS or BRS 3. Basic Cardiovascular Support Indicated by one or more of the following: Treatment of circulatory instability due to hypovolaemia from any cause. Use of a central venous pressure CVP line for basic monitoring of central venous pressure and / or the provision of central venous access to deliver titrated fluids to treat hypovolaemia. Use of an arterial line for basic monitoring of arterial pressure or sampling of arterial blood. Single intravenous vasoactive drug used to support arterial pressure, cardiac output or organ perfusion. Intravenous drugs to control cardiac arrhythmias. Non-invasive measurement of cardiac output (e.g. echocardiography, thoracic impedance). 4. Advanced Cardiovascular Support Indicated by one or more of the following: Levels of Care Examples [Final] NWCCN Informatics Group Revised December ‘09 7 Multiple intravenous vasoactive and/or rhythm controlling drugs. When used simultaneously to support or control arterial pressure, cardiac output or organ perfusion (e.g. inotropes, amiodarone, nitrates) Patients resuscitated after cardiac arrest where critical care is considered clinically appropriate. Observation of cardiac output and derived indices (e.g. pulmonary artery catheter, lithium dilution, pulse contour analyses, oesophageal doppler). Intra aortic balloon pumping and other assist devices. Insertion of a temporary cardiac pacemaker (criteria valid for each day of connection to a functioning external pacemaker unit). Placement of a gastrointestinal tonometer. 5. Renal Support Indicated by: Acute renal replacement therapy (e.g. haemodialysis, haemofiltration etc.) or the provision of renal replacement therapy to a chronic renal failure patient who is requiring other acute organ support in a critical care situation. 6. Neurological Support Indicated by one or more of the following: Central nervous system depression sufficient to prejudice the airway and protective reflexes, excepting that caused by sedation prescribed to facilitate mechanical ventilation or poisoning (e.g. self administered overdose, alcohol, drugs etc). Invasive neurological monitoring e.g. Intracranial pressure ICP, jugular bulb sampling. external ventricular drain. Severely agitated or epileptic patients requiring constant nursing attention and/or heavy sedation. Continuous intravenous medication to control seizure and/or continuous cerebral monitoring. Therapeutic hypothermia using cooling protocols or devices. 7. Gastrotintestinal Support Indicated by: Feeding with parenteral or enteral nutrition. 8. Dermatological Support Indicated by one or more of the following: Patients with major skin rashes, exfoliation or burns (e.g. greater than 30% body surface area affected). Use of multiple trauma dressings (e.g. multiple limb or limb and head dressings). Use of complex dressings (e.g. large skin area greater than 30% body surface area, open abdomen, vacuum dressings or large trauma such as multiple limb or limb and head dressings). 9. Liver Support Indicated by: Extracorporeal liver replacement device bioartificial liver or charcoal haemoperfusion. Acknowledgments Much of this document is based on the Intensive Care Society Levels of Care for adult patients standards and guidelines (2002) and work from the Critical Care team in Ysbyty Gwynedd ICU. Levels of Care Examples [Final] NWCCN Informatics Group Revised December ‘09 8