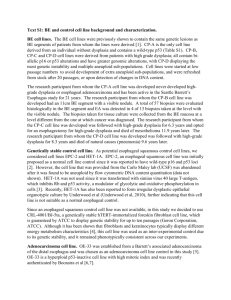
BARRETT ESOPHAGUS (BE) is a condition in which the lining of the esophageal mucosa is altered; the only known precursor to esophageal adenocarcinoma (EAC – one of the fastest rising cancers in Western populations with 5-year survival rate < 20%) Risk factor: White men age > 50; family history of BE or EAC; GERD; smoking; obesity CM: s/s of GERD (pyrosis - heartburn, regurgitation, dyspepsia - indigestion, dysphagia – difficulty swallowing, odynophagia – painful swallowing, hypersalivation, esophagitis), frequent heartburn; symptoms related to peptic ulcers or esophageal stricture, or both Assessment: esophagogastroduodenoscopy (EGD) -> abnormal: pink esophageal lining, normal: pale white; biopsy -> BE is diagnosed when the squamous mucosa of the esophagus is replaced by columnar epithelium (columnar metaplasia) at least 1 cm above the gastric folds, and that area resembles that of the stomach or intestines (intestinal metaplasia) a.e.b. the presence of goblet cells Management: individualized tx for each pt; no dysplasia – endoscopic ablation (minimally invasive procedure that allows the limited removal of a small nodule; preventing progression to dysplasia, which is an indicative of early EAC) & follow-up biopsies recommended no sooner than 3 to 5 years; progression of dysplasia – radiofrequency ablation (high-frequency heat/cold energy that kills surrounding cells and tissues); recommendations (surveillance with biopsies & the use of PPIs to control reflux symptoms) BARRETT ESOPHAGUS (BE) is a condition in which the lining of the esophageal mucosa is altered; the only known precursor to esophageal adenocarcinoma (EAC – one of the fastest rising cancers in Western populations with 5-year survival rate < 20%) Risk factor: White men age > 50; family history of BE or EAC; GERD; smoking; obesity CM: s/s of GERD (pyrosis - heartburn, regurgitation, dyspepsia - indigestion, dysphagia – difficulty swallowing, odynophagia – painful swallowing, hypersalivation, esophagitis), frequent heartburn; symptoms related to peptic ulcers or esophageal stricture, or both Assessment: esophagogastroduodenoscopy (EGD) -> abnormal: pink esophageal lining, normal: pale white; biopsy -> BE is diagnosed when the squamous mucosa of the esophagus is replaced by columnar epithelium (columnar metaplasia) at least 1 cm above the gastric folds, and that area resembles that of the stomach or intestines (intestinal metaplasia) a.e.b. the presence of goblet cells Management: individualized tx for each pt; no dysplasia – endoscopic ablation (minimally invasive procedure that allows the limited removal of a small nodule; preventing progression to dysplasia, which is an indicative of early EAC) & follow-up biopsies recommended no sooner than 3 to 5 years; progression of dysplasia – radiofrequency ablation (high-frequency heat/cold energy that kills surrounding cells and tissues); recommendations (surveillance with biopsies & the use of PPIs to control reflux symptoms) BARRETT ESOPHAGUS (BE) is a condition in which the lining of the esophageal mucosa is altered; the only known precursor to esophageal adenocarcinoma (EAC – one of the fastest rising cancers in Western populations with 5-year survival rate < 20%) Risk factor: White men age > 50; family history of BE or EAC; GERD; smoking; obesity CM: s/s of GERD (pyrosis - heartburn, regurgitation, dyspepsia - indigestion, dysphagia – difficulty swallowing, odynophagia – painful swallowing, hypersalivation, esophagitis), frequent heartburn; symptoms related to peptic ulcers or esophageal stricture, or both Assessment: esophagogastroduodenoscopy (EGD) -> abnormal: pink esophageal lining, normal: pale white; biopsy -> BE is diagnosed when the squamous mucosa of the esophagus is replaced by columnar epithelium (columnar metaplasia) at least 1 cm above the gastric folds, and that area resembles that of the stomach or intestines (intestinal metaplasia) a.e.b. the presence of goblet cells Management: individualized tx for each pt; no dysplasia – endoscopic ablation (minimally invasive procedure that allows the limited removal of a small nodule; preventing progression to dysplasia, which is an indicative of early EAC) & follow-up biopsies recommended no sooner than 3 to 5 years; progression of dysplasia – radiofrequency ablation (high-frequency heat/cold energy that kills surrounding cells and tissues); recommendations (surveillance with biopsies & the use of PPIs to control reflux symptoms) BARRETT ESOPHAGUS (BE) is a condition in which the lining of the esophageal mucosa is altered; the only known precursor to esophageal adenocarcinoma (EAC – one of the fastest rising cancers in Western populations with 5-year survival rate < 20%) Risk factor: White men age > 50; family history of BE or EAC; GERD; smoking; obesity CM: s/s of GERD (pyrosis - heartburn, regurgitation, dyspepsia - indigestion, dysphagia – difficulty swallowing, odynophagia – painful swallowing, hypersalivation, esophagitis), frequent heartburn; symptoms related to peptic ulcers or esophageal stricture, or both Assessment: esophagogastroduodenoscopy (EGD) -> abnormal: pink esophageal lining, normal: pale white; biopsy -> BE is diagnosed when the squamous mucosa of the esophagus is replaced by columnar epithelium (columnar metaplasia) at least 1 cm above the gastric folds, and that area resembles that of the stomach or intestines (intestinal metaplasia) a.e.b. the presence of goblet cells Management: individualized tx for each pt; no dysplasia – endoscopic ablation (minimally invasive procedure that allows the limited removal of a small nodule; preventing progression to dysplasia, which is an indicative of early EAC) & follow-up biopsies recommended no sooner than 3 to 5 years; progression of dysplasia – radiofrequency ablation (high-frequency heat/cold energy that kills surrounding cells and tissues); recommendations (surveillance with biopsies & the use of PPIs to control reflux symptoms)