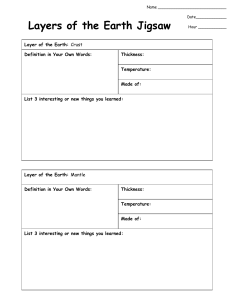
Alterations in Skin Integrity Dermatitis: Inflammation of the skin due to external stimuli Most common types in children Contact: an exposure to various irritants Diaper: irritation to infrequent diaper changes/hygiene products/Candida colonization Seborrheic: genetic/hormonal association Atopic: various triggers Contact Dermatitis: Inflammatory response to an irritant or allergen Findings: Pruritus- itchiness, Red bumps that can form moist, weeping blisters Skin warm and tender to touch, Scaly, raw or thickened skin What are some Nursing Interventions we would implement? Diaper Dermatitis caused by detergents, soaps, candida albicans Findings: Fiery red, scaly, Blisters, ulcers, Small red patches that blend together Nursing: Promptly remove soiled diaper, Non-irritating cleanser Expose to air, Apply skin barrier Parent education Seborrheic Dermatitis: Recurrent, inflammatory condition, overgrowth of yeast is a possible cause Cradle cap, blepharitis (chronic eyelid inflammation) Otitis externa (bacterial growth in ear canal causing infection) Pruritic Treatment: Gently scrub scalp to remove scales, Veg. oil, mineral oil, petroleum, Fine-tooth comb, Anti-seborrheic shampoo Dermatitis Treatment Medications: Antihistamines, If allergic or medication reaction Antibiotics Secondary bacterial infections (cellulitis), Antifungal, Candida albicans Complications: Bacterial infections Atopic Dermatitis (Eczema): Chronic inflammatory skin disorder, characterized by severe pruritus, associated with atopy Infants: Onset 2-6 months, resolve by 3 years of age Generalized distribution, Erythematous vesicles, papules Children: Onset 2-3 years of age Flexural areas, wrists, ankles, and feet Clusters of erythematous or flesh-colored papules Dry, lichenification- skin becomes thick and leathery. This is usually a result of constant scratching or rubbing. Symmetric Adolescents: Onset 12 years of age Atopic Dermatitis (Eczema) Nursing: Bathe with mild or no soap, emollient, Wash skin folds/genital area, Cotton clothing. Avoid excessive/ irritants Medications: Antihistamines, Topical steroids, immunomodulators, Antibiotics INFECTIOUS DISORDERS: Bacterial Viral Fungal Bacterial Infectious Disorders Impetigo: Staph, Highly contagious Preceded by break in skin that becomes infected, red macule →vesicular →erupts → secretions form crust Hands, neck, mouth, face, extremities, diaper area, skin folds Treatment: Topical antibiotic ointment, Oral or IV antibiotic Bacterial Infectious Disorders Pyoderma- any skin disease that is pyogenic (has pus) Staph or Strep Deeper infection into the dermisPossible systemic effects may cause fever/joint point Treatment: Cleanse with soap and water, Mupirocin, Antibiotics Folliculitis: Infection of a hair follicle, Caused by Staph (can be MRSA) Furuncle (boil): Large, swollen, red lesion of a hair follicle Carbuncle (multiple boils): More extensive Treatment: Warm compresses, Cleanse with soap and water, Incision and drainage (I&D), Antibiotics (topical or systemic) Cellulitis: Acute inflame. Of dermis, strep, staph, H. influenzae, Firm, red, swollen area of skin and subcutaneous tissue Possible systemic effects: Fever, malaise, Lymph node enlargement Treatment: Oral or parenteral antibiotics, Rest and immobilize, Acute care for systemic manifestations Viral Skin Infections Verruca (warts): Human Papillomavirus Rough, gray-brown firm papules, occur anywhere on skin Treated with salicylic acid (skin exfoliator) and duct tape, liquid nitrogen, surgical removal Verruca plantaris (plantar warts): Flat warts on plantar surface of feet caustic solution to wart Soak area, Decrease pressure Molloscum contagiosum: Poxvirus (a group of viruses in the same category- ex: chicken pox/smallpox/monkey pox/cow pox) Flesh-colored papules on extremities, face and trunk, Very contagious Resolves spontaneously in 18 months! For severe cases, remove chemically or w/ curettage (scraping of the abnormal tissue), cryotherapy Fungal Infections Most seen in Newborns - Immunocompromised Long term antibiotic use: White patches in mouth, Painful, Treatment Oral Candidiasis (Thrush) Dermatophytosis (Ringworm): Skin, hair, or nails Direct or indirect contact - Very contagious Tinea capitis (scalp): Scaly, circular lesion with alopecia, Treated with selenium sulfide shampoo Oral griseofulvin Tinea corporis (body): Round erythematous scaling patch, Central clearing Oral griseofulvin Treat infected pets Tinea cruris (jock itch):Caused by excessive sweating/tight clothing/overgrowth of a dermatophyte (type of fungus) Round, erythematous scaling patch, Pruritus, Medial thigh, and folds Topical antifungal Arthropod Bites and Stings Brown Recluse Vs Black Widow Brown recluse spiders: Mild sting that leads to erythema and blister Pain 2-8 hours after bite Necrotic ulceration 7-14 days Treatment: Cool compresses, Antibiotics, corticosteroids Brown Recluse Spider Bite (this is serious and can lead to amputation) Black widow spider: Mild sting-swollen, painful erythema, Dizziness, weakness, abdominal pain Clean with antiseptic, cool compresses, Treated with antivenom Scorpions: Intense pain, Erythema, burning, restlessness, vomiting Ascending paralysis Death for children <4 in first 24 hours Treated with antivenom, admit to ICU INFESTATIONS Pediculosis capitis: Scabies Pediculosis Capitis (Lice) Most common in pre-school to school age children Adult lice are hard to see Nits (white/tan tear-shaped specks) firmly attach to shaft Small, red bumps on the scalp, intense pruritus Treatment: 1% Permethrin shampoo, remove nits w. comb, repeat 7 days after shampoo, Wash clothing in hot water, Bag items Boil combs, brushes, and hair accessories x 10 minutes Scabies: Highly contagious, Mites burrow in epidermis Itchy, worse at night, Rash, especially between the fingers Treatment: 5% Permethrin Treat the entire family Calamine and cool compresses *Burns Infants Thermal (scalding liquid, house fires) Toddlers Thermal (hot liquids/grease) Electrical (biting cords) Chemical (ingestion) What do you think happened to this toddler in the image? How did he get burned? Pre-schoolers Thermal (liquids or hot appliances) School age & Adolescents Thermal (matches, fireworks) Electrical (climbing towers or trees with power lines) Chemical (combustion experiments) Burns: Degree Superficial/1st degree- painful Partial Thickness/2nd degree- more painful Full Thickness/3rd degree- painless as nerve endings are destroyed Based on Body Surface Area (BSA) Minor Partial thickness < 10% BSA Full thickness: Treated in outpatient setting`4 Moderate Partial thickness 10-20% BSA Full thickness: Admission to a hospital with expertise in burn care Major Partial thickness >20 % BSA Full thickness: Admission to a burn center Burns What are the nursing priorities when caring for a child with a burn? Minor burns Stop the burning- cool running water for 20 minutes Cleanse with mild soap Use antimicrobial ointment Apply dressing Provide pain medication Tetanus vaccine Major burns Maintain airway and ventilation Monitor VS, Provide O2 as necessary IV access Fluid replacement Treat with isotonic solutions in first 24 hours Maintain urine output Blood products Monitor for septic shock: Manage pain IV opioids Prevent infection Provide nutritional support Restore mobility Provide psychological support Burns: Treatment Medications: Topical antibiotic, Morphine, Sedation Wound care: Premedicate Remove previous dressing Assess for odors, drainage, Assist with debridement Skin coverings: Biologic dressings, Promote healing, Permanent skin coverings Treatment of choice for burns covering large areas of the body Autografts: child’s skin Maintain immobilization of graft site Elevate extremity, Wound care to donor site, Monitor for infection where covering/graft applied Complications Inhalation injury, Burns to face and lips Shock, Pulmonary problems Wound infection