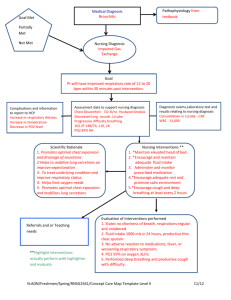
RELATED LEARNING EXPERIENCE REQUIREMENTS FOR MEDICAL AND SURGICAL WARD AREAS Name: APRIL L. BACALLA____________ Section: ___ _A5________ Area of Exposure: EMERGENCY ROOM____ Date of Exposure: 8/10/22___ Concept: Emergency Nursing: Nursing Case Management for Special Area Clinical Instructor: Miss Merra Marikit, RN I. GENERAL AND SPECIFIC OBJECTIVES A. General Objectives (Specify the concept of duty) The purpose of this is to acquire new knowledge about the health well-being of the patient, enhance the skills in improving and identifying the problems and show positive attitude to the patient as well as towards other people. B. Specific Objectives (Exact tasks written in order of priority) 1. To acquire an overview of demographic data such as the patient's name, age, date of birth, and others. 2. To be well informed on the patient’s history including the past and present hospitalization. 3. Explain the anatomy and physiology of the affected organ system according to the diagnosis of the patient and provide a brief discussion on its function. 4. To educate ourSelves about the pathophysiology and its clinical manifestation. 5. Interpret the laboratory results and indicated any abnormalities to the result. 6. To established appropriate nursing care plan that includes the independent and collaborative nursing. 7. To be acquainted with medications prescribed for the patient and there therapeutic effects and adverse reactions. 8. Have further readings about the news and updates related to the diagnosis or management of the patient. 9. To be knowledgeable on the different diagnostic procedure. 10. To formulate necessary discharge planning and health teaching essential for the patients fast recovery and prevention of possible complication. II. PATIENT’S DEMOGRAPHIC DATA Patient’s Initials: Elianna Victoria Tabar Dizon Sex: F Age: 3 years old Date of Birth: May 23, 2019 Marital Status: Address: Purok Sambag, Tisa Cebu City Occupation: NA Weight (kg): 145 kg Date and Time of Admission: 4:30 pm Chief Complaint: cough, fever and colds Admitting Diagnosis: T/C PCAP Admitting Physician: Dr. Gasendo Religion: Roman Catholic Height (m): 97 m III. PATIENTS MEDICAL HISTORY A. History of Present Illness ( A narrative detail of the current admission in chronological order) She ate an ice cream before getting the cough when they went outside. Before going to Jollibee, she had a non productive cough/dry cough for two days. They go to Manghihilot the next day, but nothing has changed. The next day, they go to the barangay doctor for guidance, and there is a crackling as the doctor auscultates the lungs. B. Past Health History Previous Hospitalizations/Surgery/Ilness (include date, hospital, diagnosis, procedure): NO previous hospitalization. Diagnosed Chronic Illness (specify): NA Immunizations (complete or incomplete, specify): Completed: Vitamin K, Hep. B, BCG and etc. Obstetric History (if applicable): NA Allergies (specify): NO allergies Other Important Information: NA C. Family Health History (Genogram with brief narrative explanation) D. Psychosocial History Brief Description of Lifestyle and Relationship with Family and Peers: She has a strong relationship with her parents, especially with her grandmother, who looks for her while her parents are away. When I interviewed her grandmother, she stated that her granddaughter ate healthy foods such as vegetables and fruits and enjoyed drinking dutchmill. She was breastfeeding before her mother went to travel overseas. From December till the present, she has been drinking Enfagrow milk. She is happy go lucky baby girl. Vices and Addictions (Provide a brief history, including smoking, alcohol, illegal drugs): No known vices and addiction. Employment History (all employment from beginning to the current): No employment history. Current Stage in Erickson’s Psychosocial Theory (discuss any positive or negative resolution): Autonomy vs. Shame and doubt. She enjoys playing with her cousins. She is always secure and confident in answering her notebook. She can already trace letters and numbers at the age of three. IV. PHYSICAL ASSESSMENT/EXAMINATION (Encircle and/or provide the information based from your assessment findings) Vital Signs Temperature: Pulse: Respiration: GENERAL SURVEY How does the Age: client look like? Sex: Male / Female Within Normal Limits Height: _________ Well groomed Facial Expression: Blood pressure: O2 Saturation: DOB: Body Build: Thin Pain Score: Cachectic Obese Weight: ______________ Poorly Groomed Anxious Happy Sad Angry NEUROLOGICAL (LOC) Level of Alert Awake Lethargic Obtunded Stuper Comatose Confused Consciousness Decerebrate Decorticate Oriented x 4: Person Place Time Event Response to touch/voice Eyes Unaided sight Glasses Contact lens Implants Prosthesis Snellen 20/ Blind Pupils Equal Round Reactive to light Accommodates Sluggish Brisk Nonreactive to light Consensual Pupil size before light ______mm Pupil size after light ______mm Ears Unaided hearing Hard of hearing Deaf Hearing aid Implant Cerumen Drainage Extremities Hand grips +1 +2 +3 +4 +5 equal unequal Foot pushes +1 +2 +3 +4 +5 equal unequal Cranial Nerves I (smell) II(vision) III+IV+VI (eye movement) V (sensation of face/oral) VII (facial movement/taste) VIII (hear/balance) IX (taste/swallow) X (chew/gag/speech) XI (shrug/turn head) XII (tongue movement) Pain (COLDSPA) Character Location Severity Associated Factors Onset Duration Pattern CARDIOVASCULAR Skin/Mucous Pink Pale Cyanotic Jaundiced Ruddy Membranes Flushed Diaphoretic Radial and Radial: Palpable (L/R) Absent (L/R) Pedal: (DP PT) Palpable (L/R) Pedal Pulses Absent (L/R) Apical R (2 people simultaneously) Apical and Radial Pulse Deficit adial Pulses Carotid Pulses (DO NOT TAKE AT SAME TIME) Right Left Thrill Bruit Capillary Refill Normal (<3 Sec) ______sec Jugular Neck Not visible Visible veins Edema Absent Present: location +1 +2 +3 +4 Anasarca Pitting Non Pitting Calf Tenderness Denies Positive Homan’s sign R L calf size R____ L_____ (team leader or charge nurse notified) Heart Regular Irregular Murmur Extra sounds Rhythm/Sounds Strong Faint Muffled -S12 IV Fluids RESPIRATORY Respirations Lung Sounds Cough Oxygen Respiratory Treatments Telemetry: rhythm ___________________ Pacemaker Defibrillator location Solution_______________ Rate __________ml/hr Infusion Pump Site location (be specific) ______________________________________ Site appearance: Clear Edema Erythema Tender Pallor Dialysis access: type __________ Thrill Bruit Location:___________ Appearance:____________ Regular Irregular Even Uneven Unlabored Labored Symmetrical Asymmetrical Clear LUL RUL LLL RLL RML Anterior Posterior Wheezes location__________ Rales/crackles location__________ Rhonchi location ________ Nasal flaring Sternal retraction Intercostal retraction Do lung sounds improve with cough and deep breath (y/n)? None Nonproductive Dry Moist Productive Sputum: amount _______________ color_______________ frequency___________ Room air Pulse ox ______ O2 at_____L/min Nasal Cannula Mask Tent CPAP BIPAP Incentive Spirometer (IS): ml______ frequency _______hold for ___ seconds # of times______ HHN medication Bipap Ventilator? TV rate 02% other GASTROINTESTINAL Oral Teeth Dentures Caries Dysphagia Mucous Membranes: intact moist dry pale leukoplakia Abdomen: Inspect Soft Round Flat Scaphoid Obese Auscultate Percuss Firm Hard Nondistended Distended Palpate Tender Non Tender Location: Bowel Sounds RLQ RUQ LUQ LLQ Normoactive Hypoactive Hyperactive Absent NGT/GT/JT None Type of tube _____ patent nonpatent Suction: low high Color of drainage ______________ Amount____________________ Bowel Movement Continent Incontinent last BM______________ Color _______________ Size_________________ Consistency_________________ Ostomy Stool Nutrition Diet___________ % eaten Breakfast____ Lunch_____ NPO? Why___________ Self feed Needs assistance Thickened liquids: honey nectar pudding Tube Feed_________________ GENITOURINARY Urine Continent Incontinent Catheter type _______________ Patent Nonpatent Color_________________ Clear Cloudy Sediment Burning Frequency Intake and Output PO/Oral/Tube Feed intake____________ IV intake____________ Urine output_________ Other output Fluid restriction Total I&O + /- ________________ Genitalia Male Female vaginal discharge LMP Post partum MUSCULOSKELETAL Mobility ADLs independent or assisted with _________________________________________________ Muscle Treatment None Cast Brace Splint Location Elevate Traction – type: _________________________ Traction weight: _________________________ CMST Circulation: color, pulses, cap refill Motion Sensation Temperature RA LA RL LL Antiembolitic Hose:knee/thigh Contractures Not present Present – which extremity? What % decreased? Amputation No Yes Location _______________________________ ROM AROM AAROM PROM CPM Limited location___________________ Mobility Turns self Sits independently Dangles Stands independently Walks independently Ambulatory assistance: Gait belt Cane Walker Crutches Braces Wheelchair Gerichair Walks: distance frequency tolerance PT OT RNA Risk for falls Bed alarm Chair alarm 1 or 2 Person Transfer Floor pad Side Rails Mechanical Lift Slide Board INTEGUMENTARY Appearance Skin Wound Dressing Pressure Ulcers Intact Color___________ Pallor Rash Bruise Lesions Scar Location __________________ Turgor_____ seconds Site___________ Warm Hot Cool Cold Dry Moist None Surgical site – Location Well approximated Sutures Staples Steristrips Dressing: Dry/intact Non-intact Change: Yes No Drainage: Color Amount___________ Odor_________ Wound appearance: Drain type _________ Amount______ Stage Tunneling Stage Tunneling Stage Tunneling Location Eschar Location Eschar Location Eschar Size Slough Size Slough Size Slough ISOLATION (if applicable) Type Site PSYCHOSOCIAL Behavior Restraints Language Spoken Cooperative Uncooperative Other_______________ None Chemical location Culture Pleasant Withdrawn Physical: Combative type CMST of extremity RA LA RL LL Frequency Checked________________ _______________________ B. General Summary of Physical Assessment/Examination Findings (Provide a narrative summary of all the findings and correlate with the diagnosis of the patient) V. ANATOMY AND PHYSIOLOGY (Draw and label the affected organ/system and provide a brief discussion of its function/uses) The respiratory system is the network of organs and tissues that allows a person to breathe. Parts that are included in the lungs are the following airways, lungs, and blood vessels. The muscles that power your lungs are also part of the respiratory system. These parts work together to move oxygen throughout the body and clean out waste gases like carbon dioxide. Parts of The respiratory system: Mouth and nose: Openings that pull air from outside the body into the respiratory system. The starting point of air distribution. If exposure to irritants such as dust enter either the mouth or nose during breathing may result to rhinitis or asthma. Trachea: Passage connecting your throat and lungs. Since asthma affects the airways, the process occurs just below the throat in a single tube called the trachea (Weinberger). Lungs: Two organs that remove oxygen from the air and pass it into your blood. When a person breathes out, the blood carries carbon dioxide and other waste out of the body. Alveoli: Tiny air sacs in the lungs where the exchange of oxygen and carbon dioxide takes place. Bronchioles: Small branches of the bronchial tubes that lead to the alveoli. Physiology of breathing Inhalation, the external intercostal muscles contract, moving the ribcage up and out. The diaphragm moves down at the same time, creating negative pressure within the thorax. The lungs are held to the thoracic wall by the pleural membranes, and so expand outwards as well. This creates negative pressure within the lungs, and so air rushes in through the upper and lower airways. During the process of ventilation delivers air to the alveoli where gaseous exchange occurs by a simple process of diffusion. A gas will move from an area of high concentration to an area of low concentration. The partial pressure of O2 in the atmosphere is higher relative to that in the body and the bloodstream contains a higher partial pressure of CO2 than the atmosphere. For effective gas exchange to take place, air breathed into the lungs must travel to the alveolar membrane where the capillary walls are thin and there is an overall large surface area. VI. PATHOPHYSIOLOGY (Trace the disease process of the patient’s diagnosed condition. Provide a brief discussion after the tracing) Reference: VII. LABORATORY AND DIAGNOSTIC STUDY Date Type of Exam 8/10/22 Hematology Specific Examination: WBC RBC HEMOGLOBIN HEMATOCRIT PLATELET COUNT MCV MCH MCHC RDW-CV MPV PDW PCT P-LCC P-LCR Patient’s Results Normal Values Significance/ Interpretation 6.06 4. 64 13.0 37.7 249 5.00-17.00 4.0-5.20 10.20-15.20 36.00-46.00 150.00-450.00 NORMAL NORMAL NORMAL NORMAL NORMAL 81.4 28.0 34.4 13.1 7.2 8.4 0.18 23 9.3 78.00-94.00 23.00-31.00 32.00-36.00 11.50-14.50 6.00-11.00 8.10-25.00 0.15-0.40 44.00-140.00 18.00-50.00 NORMAL NORMAL NORMAL NORMAL NORMAL LESS THAN 8.10-25.00 NORMAL LESS THAN 44.0-140.00 LESS THAN 18.00-50.00 *Please use the back portion for additional laboratory and diagnostic study. VIII.DRUG STUDY Drug Classifica tion Mechanism of Action Indication Contraindic ation Generic Name: Budeson ide Corticostero ids Inhibits accumulati on of inflammato ry cells, decreases and prevents tissues from responding to inflammato ry process (reverses capillary permeabilit y and lysosomal stabilization at cellular level). Budesonide extended release capsules are indicated for the treatment and maintenance of mild to moderate Crohn’s disease. Various inhaled budesonide products are indicated for prophylactic therapy in asthma and to reduce exacerbations of COPD. Hypersensi tivity is a contraindic ation for albuterol. Also, if a patient is severely hypersensit ive to milk protein, it is advised to avoid the use of albuterol. Brand Name: Pulmicor t Dosage: 200 mg/2ml Route: Inhalatio n Frequen cy: Q12hrs Timing: 15 mins after salbuta mol Adverse Effects CNS: Restlessn ess, apprehens ion, anxiety, fear, insomnia, headache, drowsines s, weakness GI: Nausea, vomiting, heartburn, bad taste CV: Tachycardi a, palpitation s, anginal pain Resp: Respirator y difficulties, coughing, pulmonary edema Derma: Sweating, pallor, flushing Nursing Responsibilities Before: 1. Check physician’s order of medication 2. Check the patient’s allergy status. 3. Assess lung sounds, pulse, and blood pressure before administration. 4. Monitor vital signs. 5. Prepare drug on time. During: 1. Observe for paradoxical bronchospasm (wheezing). 2. Instruct mother to take missed dose as soon as remembered, spacing remaining doses at regular intervals. minister accurately because adverse reactions and tolerance might occur. 4. Observe any changes in heart rhythm, episodes of palpitations. Chest pain, shortness of breath. 5. Do not exceed recommended dosage After: 1. Inform the mother not to smoke near the child and to avoid respiratory irritants 2. Advise the mother to rinse the child’s mouth with water after each inhalation dose to minimize dry mouth. 3. Note: Albuterol can cause dizziness or vertigo; take necessary precautions. 4. Do not use OTC drugs without physician approval. Many medications (e.g., cold remedies) contain drugs that may intensify albuterol action. 5. Do not breast feed while taking this drug without consulting physician. * Please use the back portion for additional medications for drug study. Follow the prescribed format. IX. PROBLEM PRIORITIZATION (at least 5) Problem 1. Ineffective airway clearance 2. Ineffective breathing pattern 3. Ineffective Thermoregulation 4. Risk of hospital acquired infection 5. Powerlessness Justification X. NURSING CARE PLANS Problem 1: Ineffective Airway Clearance Defining Characteristics Subjective: “gahi kayo ang ubo sa akong apo unya saba kaayo iyang baga” as stated by the patient's grandmother Objective: Coughing Fever Colds Nursing Diagnosis Ineffective airway clearance Scientific Analysis Breathing is something that everyone does naturally and effortlessly. However, some people are unable to keep their airways open and their lungs healthy. A patent airway has always been essential to survival. Coughing, which is the key method for clearing the airway, arises anytime there is an issue in it. Coughing, however, can be difficult for certain patients, especially those with incisions, wounds, respiratory muscle fatigue, or neuromuscular weakness. Plan of Care Short Term: After 2-3 hours of nursing intervention, the patient will be able to: The guardian of the patient can describe the importance of proper medication. Demonstrate behavior or lifestyle changes to reduce pain. Long Term: After 8 hours of nursing intervention, the patient will be able to: Establish the use of appropriate activities and relaxation skills. Nursing Interventions Independent: 1. Assess airway for patency. 2. Auscultate lungs for presence of normal or adventitious breath sounds. 3. Assess hydration status: skin turgor, mucous membranes, tongue. 4. Check for peak airway pressures and airway resistance, if patient is on mechanical ventilation. 5. Review patient’s understanding of disease process. Collaborative: 1. Assist with procedure such as administering O2. 2. Administer medication such as bronchodilators. 3. Assist with monitor hypothermia therapy use respiratory device and treatment. 4. Prepare for assist with intubation, if indicated. Rationale Independent: 1. Maintaining patent airway is always the first priority, especially in cases like trauma, acute neurological decompensatio n, or cardiac arrest. 2. Abnormal breath sounds can be heard as fluid and mucus accumulate. This may indicate ineffective airway clearance. 3. Airway clearance is impaired with poor hydration and subsequent secretion thickening. 4. Increases in these parameters signal collection of secretions or fluid and likely for ineffective ventilation. 5. Patient teaching will vary depending on the acute or chronic disease condition as well as the patient’s cognitive level. Collaborative: 1. To maintain clear open airway. 2. To promote pharmacologic regimen. 3. A various therapies may acquire/maintain adequate airways improve respiratory function and gas exchange. 4. Presence of prolonged apnea postictally may require ventilatory support. Problem 2: Ineffective Breathing Pattern Related to Retain Mucus Secretion Defining Characteristics Subjective: “Mag lisud man og ginhawa akong apo tungod aning ubo niya unya murag gi sip on” as stated by the patient's grandmother Objective: Coughing Fever Colds Nursing Diagnosis Ineffective breathing pattern related to retain mucus secretion. Scientific Analysis When the abdominal wall excursion during inspiration, expiration or both do not maintain optimum ventilation for the individual, the nursing diagnosis Ineffective Breathing Pattern is one of the issues nurses need to focus on. It is considered the state in which the rate, depth, timing, rhythm, or pattern of breathing is altered. When the breathing pattern is ineffective, the body will likely not get enough oxygen to the cells. Respiratory failure may be correlated with variations in respiratory rate, abdominal and thoracic patterns. Plan of Care Short Term: After 2-3 hours of nursing intervention, the patient will be able to: Demonstrate a measurable increase intolerance in activity with absence of dyspnea and excessive fatigue. Nursing Interventions Independent: 1.Advise increase fluid intake. 2. Administer medication as ordered. 3. Evaluate patient’s response to activity. 4. Encourage adequate rest balanced with moderate activity. Promote adequate nutritional intake. 5. Force fluids to at least 3000 ml per day and offer warm, rather than cold fluids. Collaborative: 1. Administer medications as prescribe: mucolytics or expectorants. Rationale Independent: 1.To liquefy secretion. 2. To facilitate fast recovery. 3. Establishes patient’s capabilities or needs and facilitates choice of intervention. 4. Facilitates healing process and enhances natural resistance. 5. Fluids especially warm liquid said in mobilization and expectoration of secretions. Collaborative: 1. Aids in reduction of bronchospasm and mobilization of secretions. Problem 3: Risk for altered body temperature related to Thermoregulation System Damage Defining Characteristics Subjective: “Taas kayo iyang hilanat” as stated by the patient's grandmother Objective: Coughing High Fever Colds Nursing Diagnosis Risk for altered body temperatur e related to thermoregu lation system damage Scientific Analysis Hyperthermia is defined as elevated body temperature due to a break in thermoregulation that arises when a body produces or absorbs more heat than it dissipates. It is a sustained core temperature beyond the normal variance. Hyperthermia is characterized by an uncontrolled increase in body temperature that exceeds the body’s ability to lose heat with failure in hypothalamic thermoregulation. Plan of Care Short Term: After 2-3 hours of nursing intervention, the patient will be able to: Demonstrate a measurable increase intolerance in activity with absence of dyspnea and excessive fatigue. Long Term: After 8 hours of nursing intervention, the patient will be able to: Nursing Interventions Independent: 1.Monitor core temperature. 2. Increase oral fluid intake. 3. Promote bed rest, encourage relaxation skills and diversional activities. 4. Discuss importance of adequate fluid intake and protein diet. 5. Promote surface cooling, loosen clothing and cool environment. Collaborative: 1.Administer medications as indicated to treat underlying cause. 2.Administer replacement fluids and electrolytes to support circulating volume and tissue perfusion. Rationale Independent: 1. Temperature of 38.9-41.1°Csugges t acute infectious disease process. 2. To support circulating volume and tissue perfusion. 3. To reduce metabolic demands/oxygen consumption. 4. To prevented hydration. 5. Heat is loss by convection, radiation and conduction. Collaborative: 1. To treat underlying causes. 2. To support circulating volume and tissue perfusion. XI. DISCHARGE PLANNING General Case of the Patient: Subjective Data Objective Data Assessment/Nursing Diagnosis Planning Intervention Activity Medication Environment Treatment Health Teachings Outpatient Referral Diet Evaluation XII. Further Readings (News and recent updates related to the diagnosis or management of the patient)