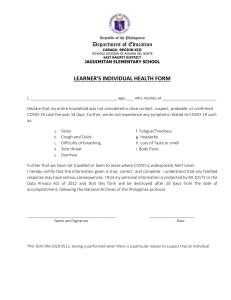
CLIENT/ VISITORS HEALTH DECLARATION FORM Name: Date of Visit: Address: Time of Visit: Phone #: Email Address: Purpose: School/ District: Temperature: YES NO Are you experiencing a. Fever b. Cough or colds c. Body pains d. Sore throat Have you had face to face contact with a probable or confirmed COVID-19 case within 1 meter for more than 15 minutes for the past 14 days? Have you provided direct care for a patient with probable or confirmed case COVID -19 care without proper protective equipment for the past 14 days? Have you travelled outside the Philippines in the last 14 days? ________________________ Have you travelled outside the current city, municipality where you reside? __________________ I declare that the information I gave are true and that I am liable to the laws of the land if information given are inaccurate. I hereby authorize DEPED SURIGAO DEL NORTE, to collect and process data indicated herein for the purpose of contact tracing effecting control of the COVID-19 transmission. I understand that my personal information is protected by RA 10173 or the Data Privacy Act of 2012 and that this form will be destroyed after 30 days from the data accomplishment, following the National Archives of the Philippine Protocol. _____________________________ Name and Signature CLIENT/ VISITORS HEALTH DECLARATION FORM Name: Date of Visit: Address: Time of Visit: Phone #: Email Address: Purpose: School/ District: Temperature: YES NO Are you experiencing a. Fever b. Cough or colds c. Body pains d. Sore throat Have you had face to face contact with a probable or confirmed COVID-19 case within 1 meter for more than 15 minutes for the past 14 days? Have you provided direct care for a patient with probable or confirmed case COVID -19 care without proper protective equipment for the past 14 days? Have you travelled outside the Philippines in the last 14 days? Have you travelled outside the current city, municipality where you reside? I declare that the information I gave are accurate and that I am liable to the laws of the land if information given are false. I hereby authorize DEPED SURIGAO DEL NORTE, to collect and process data indicated herein for the purpose of contact tracing effecting control of the COVID-19 transmission. I understand that my personal information is protected by RA 10173 or the Data Privacy Act of 2012 and that this form will be destroyed after 30 days from the data accomplishment, following the National Archives of the Philippine Protocol. _____________________________ Name and Signature